
The TVGH-NYCU Thal-Classifier: Development of a Machine-Learning Classifier for Differentiating Thalassemia and Non-Thalassemia Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Baseline Demographics and Genomic Technique
2.2. General Concept of SVM
2.3. Detail Process of Two-Stage SVM Procedure
2.3.1. Step 1. SVM for the Data with Three Classes, αTT, βTT, and Non-Thalassemia
- Randomly select two-thirds of the cohort as training data.
- Apply the “svm” and “tune” R package e1071 and use 10-fold cross validation to determine the best parameters of SVM and build the best classifier.
- Apply the principle of one-versus-one classification to classify each patient into one of αTT, βTT, and non-thalassemia.
2.3.2. Step 2. Merge the Prediction Result of Being αTT or βTT into One Class, Named “Thalassemia”. The Classifier Performing Binary Classification, Thalassemia and Non-Thalassemia, Is Then Completed
3. Results
3.1. Baseline Demographics
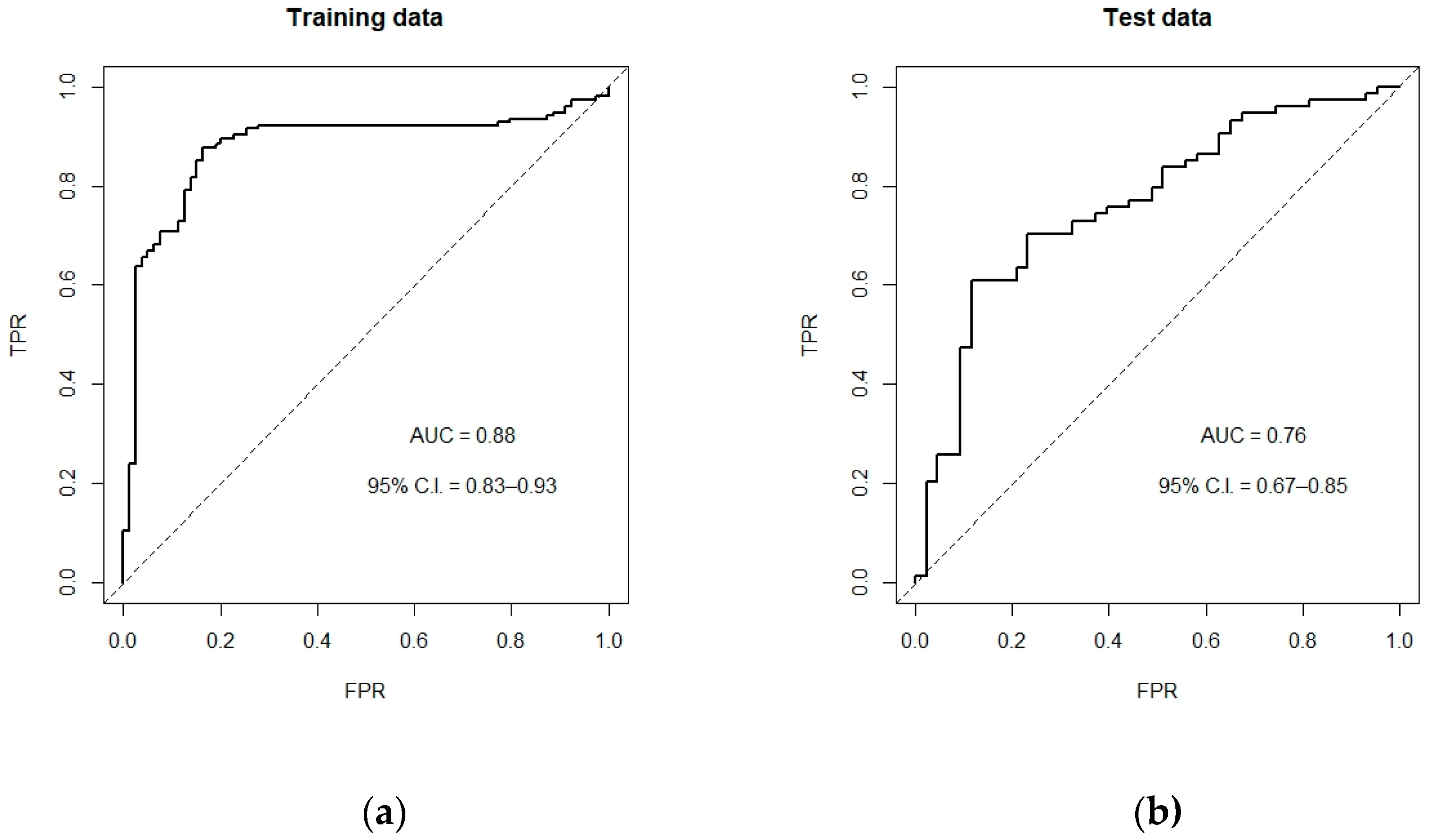
3.2. SVM Prediction Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Munkongdee, T.; Chen, P.; Winichagoon, P.; Fucharoen, S.; Paiboonsukwong, K. Update in Laboratory Diagnosis of Thalassemia. Front. Mol. Biosci. 2020, 7, 74. [Google Scholar] [CrossRef] [PubMed]
- Clegg, J.B.; Weatherall, D.J. Thalassemia and malaria: New insights into an old problem. Proc. Assoc. Am. Physicians 1999, 111, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Modell, B.; Darlison, M. Global epidemiology of haemoglobin disorders and derived service indicators. Bull. World Health Organ. 2008, 86, 480–487. [Google Scholar] [CrossRef]
- Kattamis, A.; Forni, G.L.; Aydinok, Y.; Viprakasit, V. Changing patterns in the epidemiology of beta-thalassemia. Eur. J. Haematol. 2020, 105, 692–703. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.T.; Old, J.M.; Miles, K.; Fisher, C.A.; Weatherall, D.J.; Clegg, J.B. Rapid detection of alpha-thalassaemia deletions and alpha-globin gene triplication by multiplex polymerase chain reactions. Br. J. Haematol. 2000, 108, 295–299. [Google Scholar] [CrossRef]
- Shaw, N.S.; Yeh, W.T.; Pan, W.H. Prevalence of Iron Deficiency in the General Population in Taiwan. Nutr. Sci. J. 1999, 24, 119–138. [Google Scholar]
- DeLoughery, T.G. Microcytic Anemia. N. Engl. J. Med. 2014, 371, 1324–1331. [Google Scholar] [CrossRef]
- Weiss, G.; Ganz, T.; Goodnough, L.T. Anemia of inflammation. Blood 2019, 133, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Killip, S.; Bennett, J.M.; Chambers, M.D. Iron deficiency anemia. Am. Fam. Physician 2007, 75, 671–678. [Google Scholar]
- Camaschella, C. Iron-deficiency anemia. N. Engl. J. Med. 2015, 372, 1832–1843. [Google Scholar] [CrossRef] [Green Version]
- Matos, J.F.; Dusse, L.M.S.; Borges, K.B.G.; de Castro, R.L.V.; Coura-Vital, W.; Carvalho, M.d.G. A new index to discriminate between iron deficiency anemia and thalassemia trait. Rev. Bras. Hematol. Hemoter. 2016, 38, 214–219. [Google Scholar] [CrossRef] [Green Version]
- Brancaleoni, V.; Di Pierro, E.; Motta, I.; Cappellini, M.D. Laboratory diagnosis of thalassemia. Int. J. Lab. Hematol. 2016, 38 (Suppl. 1), 32–40. [Google Scholar] [CrossRef] [Green Version]
- Goddard, A.F.; James, M.W.; McIntyre, A.S.; Scott, B.B. Guidelines for the management of iron deficiency anaemia. Gut 2011, 60, 1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, J.J.M.L.; Urrechaga, E.; Aguirre, U. Discriminant indices for distinguishing thalassemia and iron deficiency in patients with microcytic anemia: A meta-analysis. Clin. Chem. Lab. Med. 2015, 53, 1883–1894. [Google Scholar] [CrossRef]
- Jayabose, S.; Giamelli, J.; LevondogluTugal, O.; Sandoval, C.; Ozkaynak, F.; Visintainer, P. #262 Differentiating iron deficiency anemia from thalassemia minor by using an RDW-based index. J. Pediatric Hematol./Oncol. 1999, 21, 314. [Google Scholar]
- Mentzer, W.C., Jr. Differentiation of iron deficiency from thalassaemia trait. Lancet 1973, 1, 882. [Google Scholar] [CrossRef]
- England, J.M.; Fraser, P.M. Differentiation of iron deficiency from thalassaemia trait by routine blood-count. Lancet 1973, 1, 449–452. [Google Scholar] [CrossRef]
- Ricerca, B.M.; Storti, S.; d’Onofrio, G.; Mancini, S.; Vittori, M.; Campisi, S.; Mango, G.; Bizzi, B. Differentiation of iron deficiency from thalassaemia trait: A new approach. Haematologica 1987, 72, 409–413. [Google Scholar] [PubMed]
- Sirdah, M.; Tarazi, I.; Al Najjar, E.; Al Haddad, R. Evaluation of the diagnostic reliability of different RBC indices and formulas in the differentiation of the beta-thalassaemia minor from iron deficiency in Palestinian population. Int. J. Lab. Hematol. 2008, 30, 324–330. [Google Scholar] [CrossRef]
- Srivastava, P.C.; Bevington, J.M. Iron deficiency and-or thalassaemia trait. Lancet 1973, 1, 832. [Google Scholar] [CrossRef]
- Telmissani, O.A.; Khalil, S.; Roberts, G.T. Mean density of hemoglobin per liter of blood: A new hematologic parameter with an inherent discriminant function. Lab. Haematol. 1999, 5, 149–152. [Google Scholar]
- Ehsani, M.A.; Shahgholi, E.; Rahiminejad, M.S.; Seighali, F.; Rashidi, A. A new index for discrimination between iron deficiency anemia and beta-thalassemia minor: Results in 284 patients. Pak. J. Biol. Sci. 2009, 12, 473–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, R.; King, R. A new red cell discriminant incorporating volume dispersion for differentiating iron deficiency anemia from thalassemia minor. Blood Cells 1989, 15, 481–491; discussion 492–485. [Google Scholar] [PubMed]
- Shine, I.; Lal, S. A strategy to detect beta-thalassaemia minor. Lancet 1977, 1, 692–694. [Google Scholar] [CrossRef]
- Huber, A.; Ottiger, C.; Risch, L.; Regenass, S.; Hergersberg, M.; Herklotz, R. Thalassämie-Syndrome: Klinik und Diagnose Syndromes thalassémiques: Clinique et diagnostic. Swiss Med. Forum 2004, 4, 947–952. [Google Scholar]
- Ullah, Z.; Khattak, A.A.; Ali, S.A.; Hussain, J.; Noor, B.; Bano, R.; Mahsud, M.A.J. Evaluation of five discriminating indexes to distinguish Beta-Thalassemia Trait from Iron Deficiency Anaemia. J. Pak. Med. Assoc. 2016, 66, 1627–1631. [Google Scholar] [PubMed]
- Urrechaga, E.; Aguirre, U.; Izquierdo, S. Multivariable discriminant analysis for the differential diagnosis of microcytic anemia. Anemia 2013, 2013, 457834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janel, A.; Roszyk, L.; Rapatel, C.; Mareynat, G.; Berger, M.G.; Serre-Sapin, A.F. Proposal of a score combining red blood cell indices for early differentiation of beta-thalassemia minor from iron deficiency anemia. Hematology 2011, 16, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.S.; Quah, T.C.; Low, P.S.; Chong, S.S. A rapid and reliable 7-deletion multiplex polymerase chain reaction assay for alpha-thalassemia. Blood 2001, 98, 250–251. [Google Scholar] [CrossRef] [Green Version]
- Yu, W.; Liu, T.; Valdez, R.; Gwinn, M.; Khoury, M.J. Application of support vector machine modeling for prediction of common diseases: The case of diabetes and pre-diabetes. BMC Med. Inform. Decis. Mak. 2010, 10, 16. [Google Scholar] [CrossRef] [Green Version]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. An Introduction to Statistical Learning: With Applications in R; Spinger: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Keogh, R.H.; Seaman, S.R.; Barrett, J.K.; Taylor-Robinson, D.; Szczesniak, R. Dynamic Prediction of Survival in Cystic Fibrosis: A Landmarking Analysis Using UK Patient Registry Data. Epidemiology 2019, 30, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Vehapoglu, A.; Ozgurhan, G.; Demir, A.D.; Uzuner, S.; Nursoy, M.A.; Turkmen, S.; Kacan, A. Hematological indices for differential diagnosis of Beta thalassemia trait and iron deficiency anemia. Anemia 2014, 2014, 576738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.K.; Chen, L.P.; Chang, H.L.; Sung, Y.C. Underestimation of the coexistence of iron deficiencies and thalassemia minors: A single institution experience in Taiwan. Kaohsiung J. Med. Sci. 2014, 30, 409–414. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Non-Thalassemia | αT | βT | p-Value | |
|---|---|---|---|---|
| Sample size | 122 (34.9%) | 179 (51.1%) | 49 (14%) | --- |
| Age | 44.5 (33, 56) | 40 (23, 55) | 43 (28, 68) | 0.118 |
| Sex (female, male) | 88, 34 | 98, 81 | 28, 21 | <0.01 |
| WBC (103/μL) | 6055 (4500, 7660) | 6020 (5100, 7200) | 6200 (4820, 7900) | 0.554 |
| RBC (106/μL) | 4.58 (4.01, 5.07) | 5.43 (4.93, 5.89) | 5.1 (4.42, 5.72) | <0.001 |
| Hb (g/dL) | 10.85 (8.8, 12.2) | 11.8 (10.5, 12.5) | 10.9 (9.6, 12) | <0.001 |
| HCT (%) | 34.15 (28.3, 38.1) | 37.3 (33.7, 40) | 33.8 (30.2, 37.4) | <0.001 |
| MCV (fL) | 73.8 (65.2, 81.9) | 68.5 (65.7, 72) | 65.4 (62.6, 75.4) | <0.001 |
| MCH (pg) | 23.15 (19.6, 27.1) | 21.4 (20.6, 22.4) | 21 (20, 24.8) | 0.002 |
| MCHC (g/dL) | 31.9 (30.3, 33) | 31.4 (30.9, 32) | 32 (31.4, 32.5) | 0.001 |
| RDW (%) | 18.35 (15.1, 20.9) | 15.6 (14.8, 16.9) | 16.3 (15.5, 18.1) | <0.001 |
| Platelet (103/μL) | 291 (225,350) | 239 (192, 303) | 235 (195.5, 281) | <0.001 |
| Mentzer | 16.2 (13.3, 19.0) | 12.7(11.5, 14.3) | 13.7 (10.8, 16.6) | <0.001 |
| RDWI | 290.9 (238.9, 353.8) | 197.8 (177.1, 239.1) | 232.5 (180.3, 305.9) | <0.001 |
| CRUISE | 43.62 (42.59, 45.12) | 43.1 (42.4, 43.73) | 44 (42.94, 44.53) | <0.001 |
| S&L | 1241.5 (827.2, 1796.2) | 1009.3 (886.9, 1158.6) | 895.5 (787.7, 1409.9) | <0.001 |
| Srivastava | 5.05 (4.06, 6.3) | 3.94 (3.56, 4.47) | 4.48 (3.35, 5.18) | <0.001 |
| G&K | 97.1 (72.9, 112.1) | 63.4 (56.4, 75.4) | 70.8 (56.7, 96.3) | <0.001 |
| Sirdah | 36.9 (31.1, 42.9) | 28.11 (24.2, 33.3) | 29.52 (23.0, 37.3) | <0.001 |
| Ehsani | 27 (15.5, 39) | 14 (8.6, 21.1) | 18.3 (4.8, 28.3) | <0.001 |
| E&F | 12.3 (6.1, 19.5) | 1.4 (−4.1, 8.5) | 4.46 (−3.7, 13.9) | <0.001 |
| Ricerca | 4.2 (3.0, 4.9) | 2.9 (2.6, 3.3) | 3.4 (2.8, 4.2) | <0.001 |
| MDHL | 1.43 (1.24, 1.6) | 1.71 (1.53, 1.84) | 1.57 (1.4, 1.83) | <0.001 |
| MCHD | 0.32 (0.3, 0.33) | 0.31 (0.31, 0.32) | 0.32 (0.31, 0.33) | 0.001 |
| HH | 27.2 (22.7, 32.1) | 22.0 (20.7, 24.1) | 23.7 (21.4, 28.6) | <0.001 |
| Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|
| Mentzer index | 58.41% | 79.51% | 84.08% | 50.79% |
| RDWI | 62.83% | 85.25% | 88.75% * | 55.32% |
| CRUISE index | 72.12% | 27.05% | 64.68% | 34.38% |
| Shine and Lal (S&L) | 90.27% | 37.70% | 72.86% | 67.65% |
| Srivastava | 41.59% | 83.61% | 82.46% | 43.59% |
| Green and King (G&K) | 55.31% | 86.07% | 88.03% | 50.97% |
| Sirdah | 44.69% | 89.34% | 88.60% | 46.58% |
| Ehsani | 54.87% | 77.05% | 81.58% | 47.96% |
| England and Fraser (E&F) | 42.92% | 86.07% | 85.09% | 44.87% |
| Ricerca | 85.84% | 40.16% | 72.66% | 60.49% |
| Telmissani- MDHL | 40.09% | 88.52% | 86.67% | 44.26% |
| Telmissani- MCHD | 99.12% * | 7.38% | 66.47% | 81.82% * |
| Huber Herklotz | 9.73% | 96.72% * | 84.62% | 36.65% |
| Model/Indices | CER (SD) | AUC (95% C.I.) |
|---|---|---|
| SVM model | 0.26 (0.04) | 0.76 (0.69–0.86) |
| Ricerca | 0.68 (0.04) | 0.51 (0.40–0.62) |
| Mentzer | 0.44 (0.04) | 0.52 (0.39 0.66) |
| RDWI | 0.46 (0.04) | 0.51 (0.38 0.64) |
| CRUISE | 0.62 (0.04) | 0.57 (0.47 0.67) |
| MDHL | 0.36 (0.04) | 0.5 (0.38 0.62) |
| S & L | 0.73 (0.03) | 0.48 (0.36 0.59) |
| Srivastava | 0.36 (0.04) | 0.52 (0.39 0.65) |
| G & K | 0.41 (0.04) | 0.52 (0.39 0.66) |
| Sirdah | 0.36 (0.04) | 0.51 (0.39 0.64) |
| Ehsani | 0.43 (0.04) | 0.53 (0.40–0.66) |
| E & F | 0.38 (0.04) | 0.48 (0.36–0.60) |
| MCHD | 0.82 (0.10) | 0.50 (0.47–0.54) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, Y.-K.; Liu, H.-M.; Lee, L.-H.; Chen, Y.-J.; Chien, S.-H.; Lin, J.-S.; Chen, W.-C.; Cheng, M.-H.; Lin, P.-H.; Lai, J.-Y.; et al. The TVGH-NYCU Thal-Classifier: Development of a Machine-Learning Classifier for Differentiating Thalassemia and Non-Thalassemia Patients. Diagnostics 2021, 11, 1725. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091725
Fu Y-K, Liu H-M, Lee L-H, Chen Y-J, Chien S-H, Lin J-S, Chen W-C, Cheng M-H, Lin P-H, Lai J-Y, et al. The TVGH-NYCU Thal-Classifier: Development of a Machine-Learning Classifier for Differentiating Thalassemia and Non-Thalassemia Patients. Diagnostics. 2021; 11(9):1725. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091725
Chicago/Turabian StyleFu, Yi-Kai, Hsueng-Mei Liu, Li-Hsuan Lee, Ying-Ju Chen, Sheng-Hsuan Chien, Jeong-Shi Lin, Wen-Chun Chen, Ming-Hsuan Cheng, Po-Heng Lin, Jheng-You Lai, and et al. 2021. "The TVGH-NYCU Thal-Classifier: Development of a Machine-Learning Classifier for Differentiating Thalassemia and Non-Thalassemia Patients" Diagnostics 11, no. 9: 1725. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091725