
C-Reactive Protein for the Early Assessment of Non-Malarial Febrile Patients: A Retrospective Diagnostic Study

 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Setting
- -
- Patients who did not fulfil the diagnostic criteria.
- -
- Records with incomplete demographic data.
- -
- Records with no CRP value available within 48 h of the initiation of specific treatment.
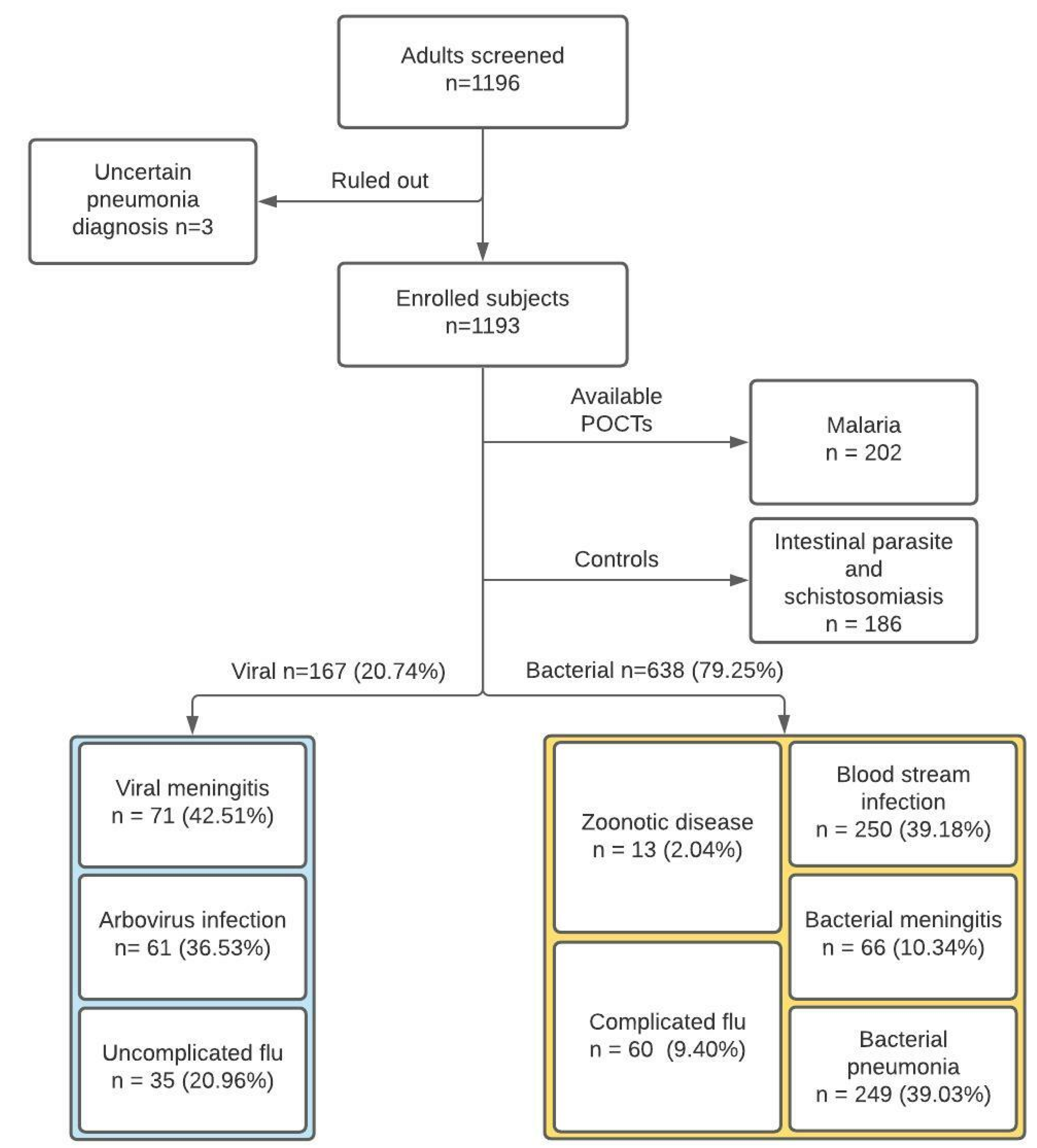
2.2. Disease Group Classification
- Viral infections (including viral meningitis, arbovirus infections and flu);
- Bacterial infections, including blood stream infections, bacterial meningitis, bacterial pneumonia, zoonotic infections (Brucella, Leptospira), and complicated flu with secondary bacterial infections likely requiring antibiotic treatment;
- Malaria;
- Intestinal parasites and schistosomiasis.
2.3. Data Management and Confidentiality
2.4. Sampling and Sample Size
2.5. Statistical Analysis
2.6. Ethical Approval
3. Results
3.1. Demographic, Clinical, and Laboratory Characteristics (Viral vs. Bacterial)
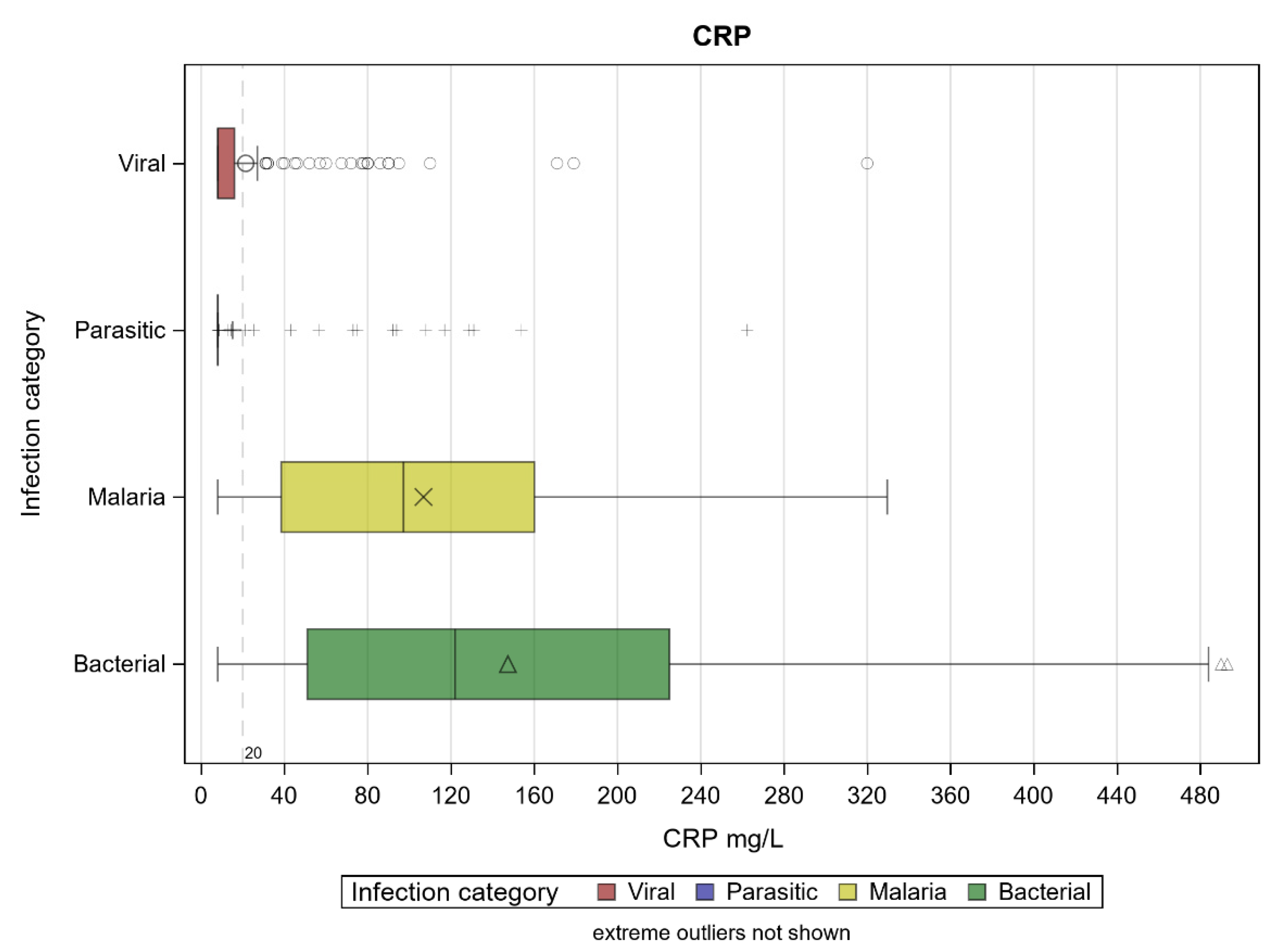
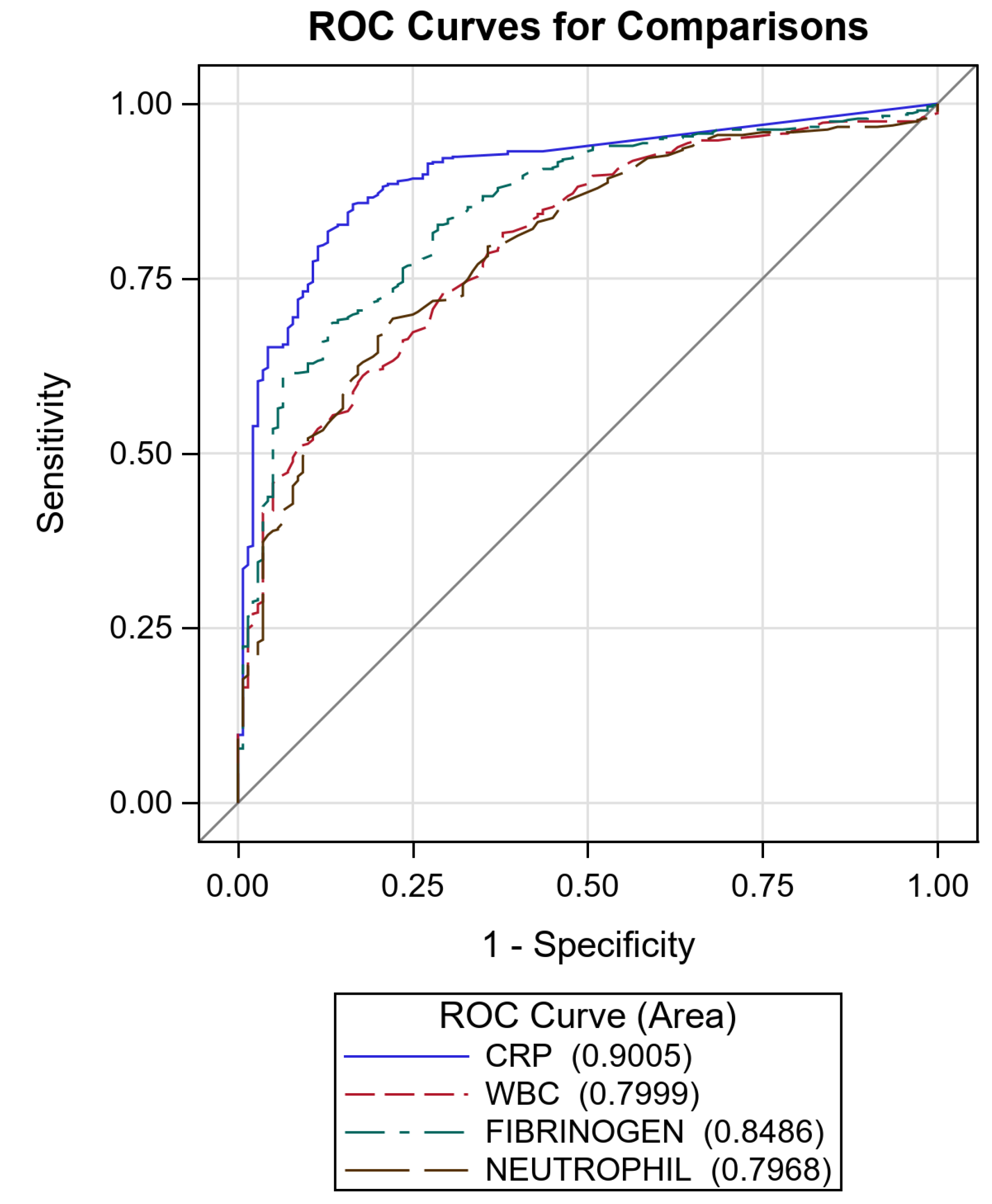
3.2. Biomarkers (Viral vs. Bacterial)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance 2014; WHO Press: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. WHO Informal Consultation on Fever Management in Peripheral Health Care Settings: A global Review of Evidence and Practice; WHO Press: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. Guidelines for the Treatment of Malaria; WHO Press: Geneva, Switzerland, 2015. [Google Scholar]
- Bisoffi, Z.; Sirima, S.B.; Menten, J.; Pattaro, C.; Angheben, A.; Gobbi, F.; Tinto, H.; Lodesani, C.; Neya, B.; Gobbo, M.; et al. Accuracy of a rapid diagnostic test on the diagnosis of malaria infection and of malaria-attributable fever during low and high transmission season in Burkina Faso. Malar. J. 2010, 9, 19. [Google Scholar] [CrossRef] [Green Version]
- Keitel, K.; Kagoro, F.; Samaka, J.; Masimba, J.; Said, Z.; Temba, H.; Mlaganile, T.; Sangu, W.; Rambaud-Althaus, C.; Gervaix, A.; et al. A novel electronic algorithm using host biomarker point-of-care tests for the management of febrile illnesses in Tanzanian children (e-POCT): A randomized, controlled non-inferiority trial. PLoS Med. 2017, 14, e1002411. [Google Scholar] [CrossRef]
- Hildenwall, H.; Muro, F.; Jansson, J.; Mtove, G.; Reyburn, H.; Amos, B. Point-of-care assessment of C-reactive protein and white blood cell count to identify bacterial aetiologies in malaria-negative paediatric fevers in Tanzania. Trop. Med. Int. Health TM IH 2017, 22, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Lubell, Y.; Blacksell, S.D.; Dunachie, S.; Tanganuchitcharnchai, A.; Althaus, T.; Watthanaworawit, W.; Paris, D.H.; Mayxay, M.; Peto, T.J.; Dondorp, A.M.; et al. Performance of C-reactive protein and procalcitonin to distinguish viral from bacterial and malarial causes of fever in Southeast Asia. BMC Infect. Dis. 2015, 15, 511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aabenhus, R.; Jensen, J.; Jørgensen, K.; Hróbjartsson, A.; Bjerrum, L. Biomarkers as point-of-care tests to guide prescription of antibiotics in patients with acute respiratory infections in primary care. Cochrane Database Syst. Rev. 2014, 11, CD010130. [Google Scholar] [CrossRef] [PubMed]
- Escadafal, C.; Nsanzabana, C.; Archer, J.; Chihota, V.; Rodriguez, W.; Dittrich, S. New Biomarkers and Diagnostic Tools for the Management of Fever in Low- and Middle-Income Countries: An Overview of the Challenges. Diagnostics 2017, 7, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertoli, G.; Ronzoni, N.; Silva, R.; Spinicci, M.; Perlini, C.; Omega, L.; Ursini, T.; Bartoloni, A.; Olliaro, P.; Bisoffi, Z.; et al. Usefulness of C-Reactive Protein and Other Host BioMarker Point-of-Care Tests in the Assessment of Non-Malarial Acute Febrile Illnesses: A Systematic Review with Meta-Analysis. Am. J. Trop. Med. Hyg. 2020, 103, 1797–1802. [Google Scholar] [CrossRef] [PubMed]
- Vashist, S.K.; Venkatesh, A.G.; Schneider, E.M.; Beaudoin, C.; Luppa, P.B.; Luong, J.H.T. Bioanalytical advances in assays for C- reactive protein. Biotechnol. Adv. 2016, 34, 272–290. [Google Scholar] [CrossRef] [PubMed]
- Kortz, T.B.; Nyirenda, J.; Tembo, D.; Elfving, K.; Baltzell, K.; Bandawe, G.; Rosenthal, P.J.; Macfarlane, S.B.; Mandala, W.; Nyirenda, T.S. Distinct Biomarker Profiles Distinguish Malawian Children with Malarial and Non-malarial Sepsis. Am. J. Trop. Med. Hyg. 2019, 101, 1424–1433. [Google Scholar] [CrossRef] [PubMed]
- Otten, T.; de Mast, Q.; Koeneman, B.; Althaus, T.; Lubell, Y.; van der Ven, A. Value of C-reactive protein in differentiating viral from bacterial aetiologies in patients with non-malaria acute undifferentiated fever in tropical areas: A meta-analysis and individual patient data study. Trans. R. Soc. Trop. Med. Hyg. 2021, 101, 276–282. [Google Scholar] [CrossRef]
- Kapasi, A.J.; Dittrich, S.; Gonzalez, I.J.; Rodwell, T.C. Host Biomarkers for Distinguishing Bacterial from Non-Bacterial Causes of Acute Febrile Illness: A Comprehensive Review. PLoS ONE 2016, 11, e0160278. [Google Scholar]
- Salami, O.; Horgan, P.; Moore, C.E.; Giri, A.; Sserwanga, A.; Pathak, A.; Basnyat, B.; Kiemde, F.; Smithuis, F.; Kitutu, F.; et al. Impact of a package of diagnostic tools, clinical algorithm, and training and communication on outpatient acute fever case management in low- and middle-income countries: Protocol for a randomized controlled trial. Trials 2020, 21, 974. [Google Scholar] [CrossRef] [PubMed]
- Althaus, T.; Lubell, Y.; Maro, V.P.; Mmbaga, B.T.; Lwezaula, B.; Halleux, C.; Biggs, H.M.; Galloway, R.L.; Stoddard, R.A.; Perniciaro, J.L.; et al. Sensitivity of C-reactive protein for the identification of patients with laboratory-confirmed bacterial infections in northern Tanzania. Trop. Med. Int. Health 2020, 25, 291–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Infectious Disease | Diagnostic Criteria | Type of Infection |
|---|---|---|
| MALARIA | Parasitological identification, PCR | Not viral |
| BLOOD STREAM INFECTION | Microbiological identification | Not viral |
| BACTERIAL PNEUMONIA | Radiological signs, microbiological identification, urinary antigens | Not viral |
| BACTERIAL MENINGITIS (S. pneumoniae, N. meningitidis, H. influenzae) | Microbiological identification, PCR | Not viral |
| ZOONOTIC DISEASES (brucellosis, leptospirosis, rickettsiosis) | Serology, PCR | Not viral |
| UNCOMPLICATED FLU | Serology, PCR | Viral |
| COMPLICATED FLU (OVER INFECTION) | Serology, PCR | Not viral |
| ARBOVIRUS INFECTION (dengue, chikungunya, zika) | Serology, PCR | Viral |
| VIRAL MENINGITIS | Serology, PCR | Viral |
| INTESTINAL PARASITE INFECTION AND SCHISTOSOMIASIS | Serology, parasitological identification, PCR | Controls |
| Center | Viral N (%) | Bacterial N (%) | Parasitic N (%) | Malaria N (%) | Overall N (%) |
|---|---|---|---|---|---|
| FIRENZE | 131 (78.4) | 405 (63.5) | 32 (17.2) | 57 (28.2) | 625 (52.4) |
| NEGRAR | 36 (21.6) | 233 (36.5) | 154 (82.8) | 145 (71.8) | 568 (47.6) |
| Overall | 167 | 638 | 186 | 202 | 1193 |
| Demographical Data | N | Overall | Diagnoses | |||
|---|---|---|---|---|---|---|
| Viral | Bacterial | Parasitic | Malaria | |||
| FEMALE, N (%) | 1193 | 434 (36.4) | 77 (46.1) | 269 (42.1) | 30 (16.1) | 58 (28.7) |
| AGE (YEARS), MEDIAN (IQR) | 1193 | 46 (32–63) | 37 (30–50) | 57 (42–69) | 25 (21–34) | 41 (33–52) |
| PATIENTS’ ORIGIN, N (%) | 1193 | |||||
| ITALY | 709 (59.4) | 125 (74.9) | 561 (65.8) | 15 (8.1) | 60 (29.7) | |
| AFRICA | 343 (28.8) | 7 (4.2) | 140 (16.4) | 157 (84.4) | 128 (63.4) | |
| SOUTHEAST ASIA | 27 (2.3) | 6 (3.6) | 42 (4.9) | 6 (3.2) | 3 (1.5) | |
| OTHER | 114 (9.6) | 29 (17.4) | 110 (12.9) | 8 (4.3) | 11 (5. 4) | |
| CLINICAL DATA | ||||||
| HIV, N (%) | 1193 | 40 (4.2) | 7 (3.8) | 24 (4.4) | 1 (0.5) | 8 (4.0) |
| FEVER ON ADMISSION, N (%) TEMPERATURE ON ADMISSION, MEDIAN (IQR) | 1171 478 | 485 (41.4) 38.30 °C (37.90–38.90) | 90 (53.9) 38.00 °C (37.80–38.50) | 301 (47.6) 38.40 °C (38.00–39.00) | 4 (2.3) 37.75 °C (37.65–38.15) | 90 (46.0) 38.40 °C (38.00–39.00) |
| FEVER IN THE LAST 24 HOURS, N (%) TEMPERATURE IN THE LAST 24 HOURS, MEDIAN (IQR) | 1190 391 | 677 (56.0) 39.00 °C (38.30–39.30) | 110 (65.9) 39.00 °C (38.05–39.00) | 419 (65.7) 39.00 °C (38.50–39.50) | 3 (1.6) 40.00 °C (40.00–40.00) | 145 (71.8) 39.00 °C (38.00–39.10) |
| MAXIMUM OBSERVED TEMPERATURE DURING HOSPITALIZATION, MEDIAN (IQR) | 1108 | 38.00 °C (37.00–39.00) | 38.00 °C (37.50–38.70) | 38.40 °C (37.50–39.00) | 36.50 °C (36.20–36.70) | 38.30 °C (37.00–39.20) |
| FEVER DURATION (DAYS), MEDIAN (IQR) | 1113 | 2.00 (0.00–5.00) | 3.00 (1.00–5.00) | 3.00 (1.00–5.00) | 0.00 (0.00–0.00) | 1.00 (0.00–2.00) |
| CARDIAC FREQUENCY (BPM), MEDIAN (IQR) | 1090 | 82.00 (72.00–95.00) | 80.00 (70.00–89.00) | 87.00 (76.00–100.00) | 70.00 (60.00–80.00) | 83.5 (72.00–98.00) |
| DIED, N (%) | 1193 | 13 (2.0) | 0 (0.0) | 13 (2.0) | 0 (0.0) | 0 (0.0) |
| Biomarkers Median (IQR) | N | Overall | Diagnoses | |||
|---|---|---|---|---|---|---|
| Viral | Bacterial | Parasitic | Malaria | |||
| WBC (N/µL) | 1190 | 6.80 (4.50–11.00) | 4.70 (3.10–7.20) | 8.60 (6.00–13.50) | 5.30 (4.10–6.40) | 4.90 (4.00–6.10) |
| Neutrophils (N/µL) | 1131 | 4.10 (2.20–7.80) | 2.80 (1.40–4.80) | 7.10 (4.30–11.80) | 2.05 (1.5–2.80) | 2.90 (1.80–4.00) |
| Fibrinogen (mg/dL) | 1044 | 4.79 (3.51–6.19) | 3.88 (3.22–4.78) | 5.82 (4.83–7.90) | 2.49 (2.25–3.01) | 4.17 (3.51–4.98) |
| ESR (mm/h) | 734 | 30.00 (12.00–54.00) | 14.00 (8.00–24.50) | 52.00 (35.00–67.00) | 9.00 (6.00–16.00) | 30.00 (15.00–52.00) |
| Biomarkers | Cut-Off | Sensitivity (95% CI) | Specificity (95% CI) |
|---|---|---|---|
| CRP | 11.00 | 92.8 (90.8–94.8) | 69.3 (62.3–76.3) |
| WBC | 3.60 | 93.7 (91.8–95.6) | 32.3 (25.2–39.4) |
| FIBRINOGEN | 3.85 | 93.5 (91.4–95.5) | 48.3 (40.1–56.4) |
| NEUTROPHILS | 1.60 | 95.1 (93.3–96.8) | 29.2 (22.2–36.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertoli, G.; Mazzi, C.; Ronzoni, N.; Silva, R.; Spinicci, M.; Pozzi, M.; Sponga, P.; Aiello, A.; Ursini, T.; Bartoloni, A.; et al. C-Reactive Protein for the Early Assessment of Non-Malarial Febrile Patients: A Retrospective Diagnostic Study. Diagnostics 2021, 11, 1728. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091728
Bertoli G, Mazzi C, Ronzoni N, Silva R, Spinicci M, Pozzi M, Sponga P, Aiello A, Ursini T, Bartoloni A, et al. C-Reactive Protein for the Early Assessment of Non-Malarial Febrile Patients: A Retrospective Diagnostic Study. Diagnostics. 2021; 11(9):1728. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091728
Chicago/Turabian StyleBertoli, Giulia, Cristina Mazzi, Niccolò Ronzoni, Ronaldo Silva, Michele Spinicci, Marco Pozzi, Pietro Sponga, Andrea Aiello, Tamara Ursini, Alessandro Bartoloni, and et al. 2021. "C-Reactive Protein for the Early Assessment of Non-Malarial Febrile Patients: A Retrospective Diagnostic Study" Diagnostics 11, no. 9: 1728. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091728