2. Case Report
A 63-year-old man presented to the emergency department (ED) with fever (T 38 °C), cough, and asthenia for a few days. His medical history was notable for coronary heart disease and atrial fibrillation, which required an implantable cardioverter defibrillator, chronic obstructive pulmonary disease, a smoking habit, previous splenectomy for immune thrombocytopenia (ITP), and chronic myelomonocytic leukemia in treatment with hydroxycarbamide.
In the ED his vital signs quickly deteriorated, revealing a drowsiness, tachycardia with 140 bpm, blood pressure of 50/30 mmHg, temperature of 37 °C, and hypoxia (pO2 of 50 mmHg to blood gas analysis). Blood samples showed C-reactive protein 14.57 mg/dL, white blood count (WBC) 28.440 103/mm3 (93% neutrophils), procalcitonin (PCT) 151 ng/mL, creatinine 2.72 mg/dL, and total bilirubin 1.9 mg/dL.
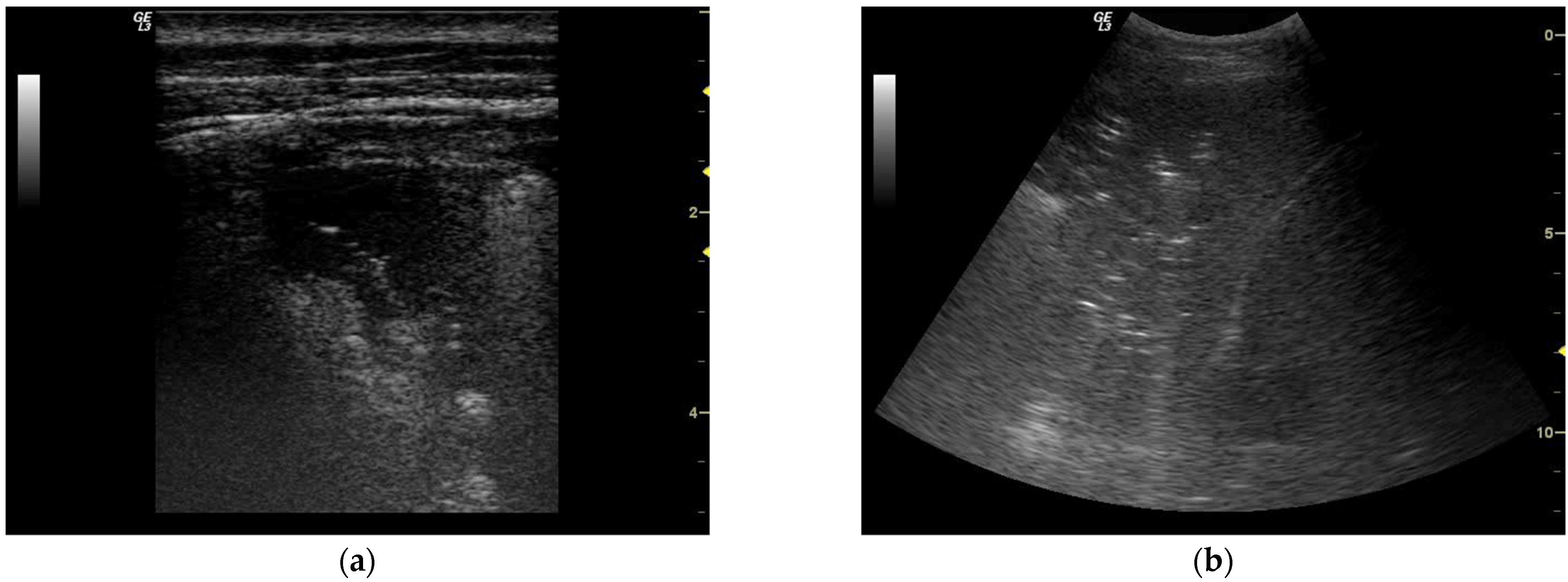
A total-body ultrasound (US) assessment was performed. Lung US revealed bilateral basal consolidations (
Figure 1) and moderate pleural effusions. Abdominal US was negative for effusions of free fluids, whilst scans performed on the left hypochondrium raised doubts concerning reliability since the spleen was not clearly visible. Thus, a CT scan was required.
A non-contrast chest CT scan confirmed bilateral basal consolidations, CT scans of brain, abdomen, and pelvis were negative for infective findings, and an abdominal CT scan confirmed splenectomy. Due to hypoxia and respiratory failure, 3 h after his arrival in the ED the patient was intubated and mechanically ventilated; then, he was transferred to intensive care for the treatment of septic shock.
Persistent hypotension required fluids and hemodynamic support with noradrenaline (peak dosage 0.8 mcg kg−1 min−1). Cultures were obtained in the ED and empiric antibiotic therapy with piperacillin/tazobactam was started, aiming at infection control. As for source identification, common infectious etiologies (Cytomegalovirus, Mycoplasma pneumoniae, Epstein–Barr virus, Chlamydia pneumoniae, and Legionella pneumophila) were excluded. A SARS-CoV-2 test was repeated and confirmed to be negative. Bronchoalveolar lavage and urine cultures were negative. Meanwhile, after 11 h of incubation, two aerobic blood cultures isolated a Gram-negative rod. After 24–36 h, small colonies grew in a chocolate agar under an enriched 5% CO2 environment. Using a matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF) Vitek MS® (bioMérieux, Vila Nova de Gaia, Portugal), C. canimorsus was identified on blood culture on day 4. Further history analysis revealed that the patient lived with his two dogs, although no wound or scar was found after re-examination of the skin.
During the patient’s ICU stay, clinical conditions gradually improved, and source control proved to be effective since C. canimorsus was sensitive to the empiric antibiotic therapy. Lung US confirmed the resolution of respiratory impairment. On day 7 the patient was weaned from respiratory support, and discharge from the internal medicine ward was possible on day 15. Blood cultures repeated 20 days after admission were negative, and the patient was discharged alive from the hospital. After discharge from the ICU, written informed consent and ethical approval were obtained for clinical case publication.
3. Discussion
Capnocytophaga canimorsus is a commensal bacterium in the oral flora of dogs and cats; the bacterium is a zoonotic agent and has been isolated from humans infected by dog or cat bites, scratches, licks or simply exposure to dogs or cats. Classified as a facultative anaerobic, it is a Gram-negative rod (1–4 mm long), fusiform or filamentous, gliding bacteria closely related to Fusobacterium and Bacteroides species; it grows slowly on blood, incubated for at least 5 days, up to 14 days [
2].
C. canimorsus is able to avoid the immune system in the early stages of infection by means of the downregulation of TLR4 and the proinflammatory signaling cascade; it is also resistant against phagocytosis and killing. Considered to be less virulent in healthy people,
C. canimorsus could be seriously harmful in immunocompromised subjects such as patients with asplenia, a long history of alcohol abuse, cirrhosis, immunosuppressive therapy, hemochromatosis, beta-talassemia major and a cigarette-smoking habit. Our patient presented some of these risk factors. Nevertheless, cases among immunocompetent persons have been described [
3].
Initially, patients may show local lesions related to animal bites, without significant signs of inflammation, or localized cellulitis, pain at the site of injury, lymphangitis and regional lymphadenopathy. The initial symptoms of septicemia are fever, chills, myalgia, vomiting, diarrhea, abdominal pain, dyspnea and mental confusion. A fulminant and severe course of the infection in immunocompromised persons is characterized by sepsis, meningitis, osteomyelitis, peritonitis, endocarditis, pneumonia, disseminated intravascular coagulation (DIC), and fulminant purpura; they also been observed in healthy patients. The median time from exposure to sepsis is 3 days, and 7 days for meningitis [
4].
Due to unspecific presentation and slow growth on cultures, the diagnosis and treatment of
C canimorsus bacteremia are often challenging, unless the history of a dog bite is clear. Other studies have reported similar cases; however, in these cases, a dog bite was visible on presentation, unlike in the present case. Indeed, although specific bacteremia after an animal bite such as
C. canimorsus or
Pasteurella multocida could be suspected, the lack of any skin lesion as a route of infection should not be employed as a rule-out criteria. Currently, the MALDI-TOF MS method is the gold standard for detecting bacteria in blood samples. Nevertheless, Gram-stain exam under the microscope may reveal multiple Gram-negative, extracellular, fusiform rods and several intracellular copies of the pathogen in neutrophils even before MALDI-TOF, thus leading clinicians to suspect the presence of
C. canimorsus thanks to the observation of toxic granulation in the cytoplasm of neutrophils in peripheral blood smear. Indeed, matching examination of peripheral blood smears with patient history and clinical examination might certainly assist diagnosis, and guide prompt empiric treatment in patients with septicemia following close animal contact [
5].
C. canimorsus is generally sensitive to penicillin, third-generation cephalosporins, carbapenems, clindamycin, doxycycline, chloramphenicol, macrolides, rifampin, and fluorochinolones, whilst it is considered to be resistant to aztreonam, trimethoprim, Fosfomycin, and aminoglycozides. The length of treatment varies between reports, from 14 to 21 days. The literature presents a few cases of patients infected by
C. canimorsus who died due to complications caused by the septic state, often due to misunderstood diagnosis or late treatment. According to the literature, mortality from
C. canimorsus ranges from 10% to 30% [
6], with the mortality rate of severe sepsis being as high as 26%. Early culture sample collection, pertinent and timely-administered antibiotic therapy, and intensive support treatment, as in this case, decrease the risk of complications and increase survival, especially in patients with coexisting risk factors or comorbidities [
7].


 ,
, 
{kind=link}
