
Comparison of Tongue Characteristics Classified According to Ultrasonographic Features Using a K-Means Clustering Algorithm

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size
2.2. Participation
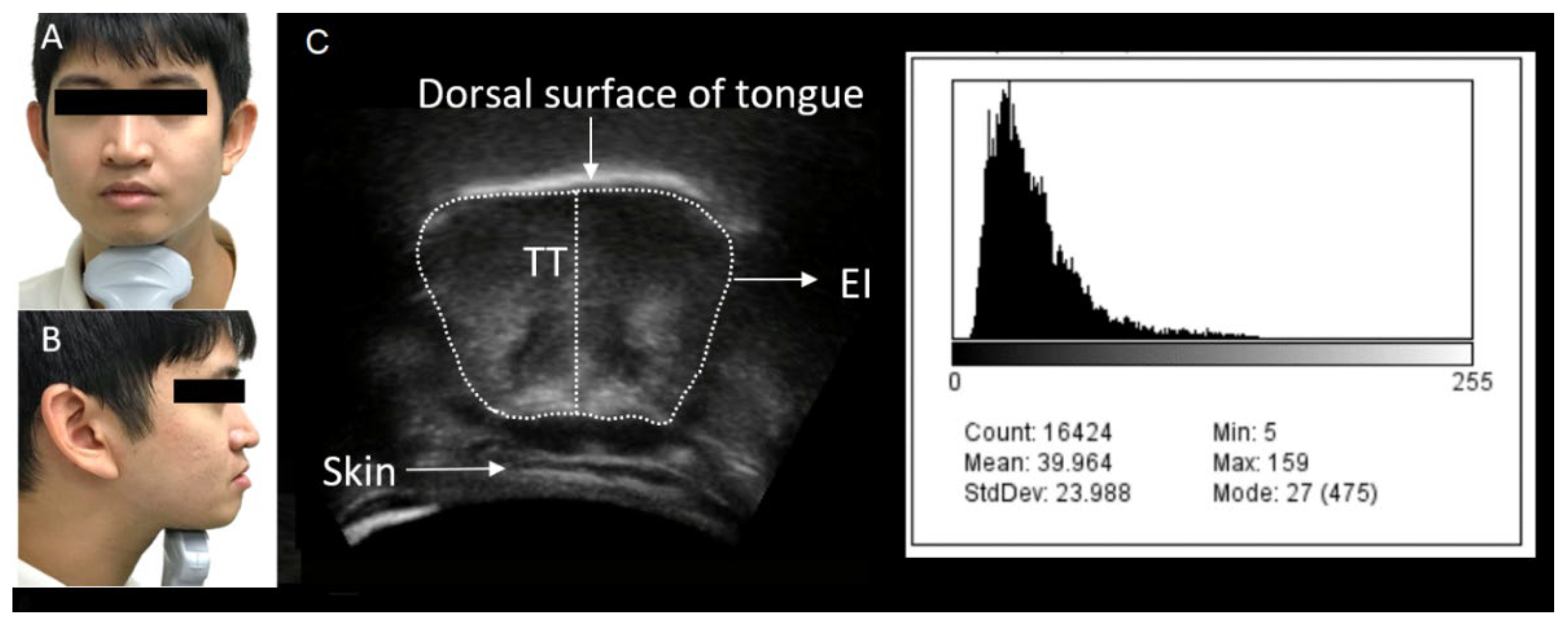
2.3. Assessment of Tongue Characteristics
2.4. Assessment of Tongue Function
2.5. Statistical Analysis
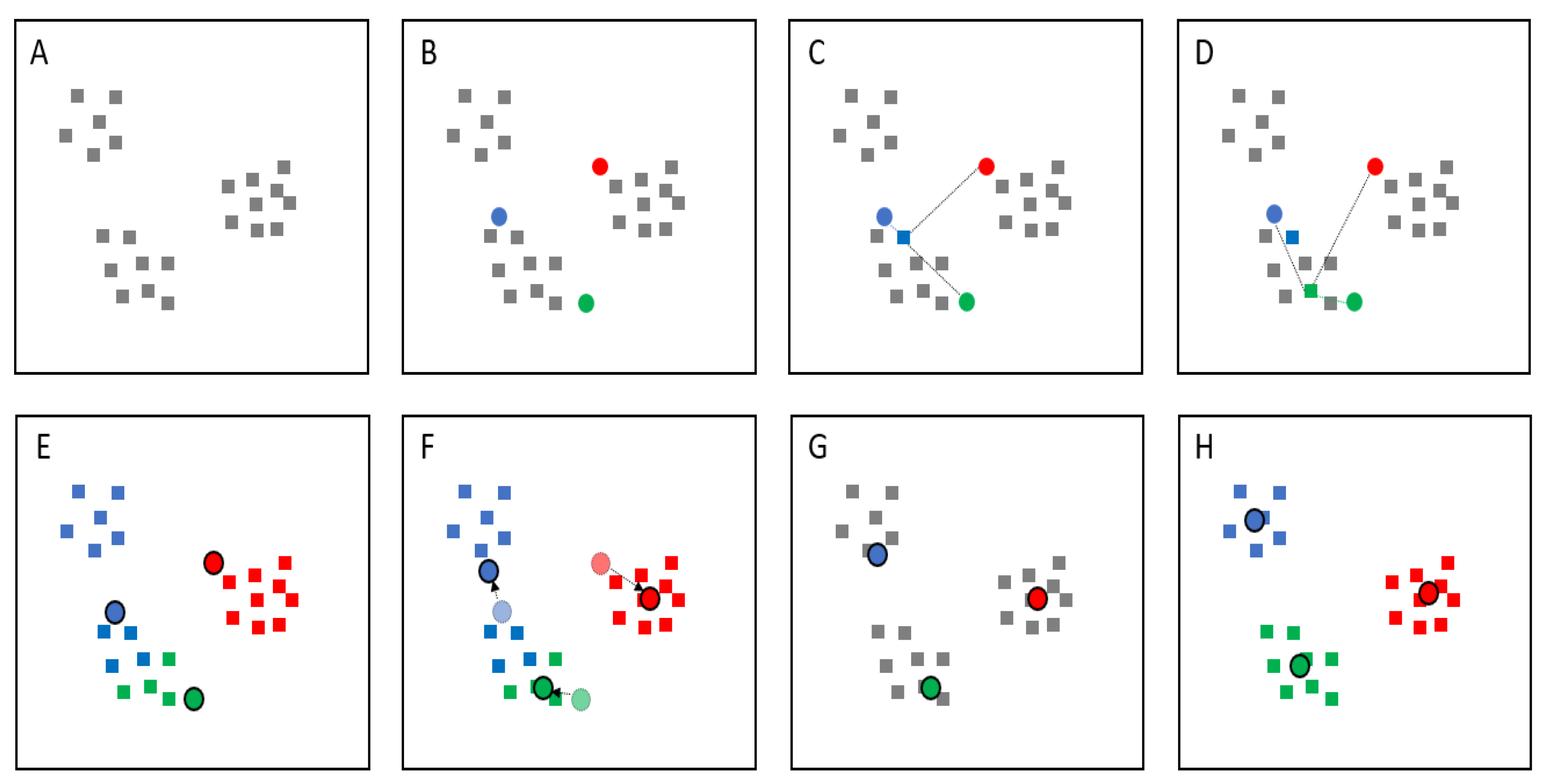
2.6. Classification Using K-Means Clustering Algorithms
3. Results
3.1. Determining Optimal Clusters
3.2. Tongue Characteristics
3.3. Tongue Function
4. Discussion
4.1. Relationship between Tongue Group and TP
4.2. Relationship between Tongue Groups and OD
4.3. Categorizing Tongue Characteristics Using K-Means Clustering Algorithms
4.4. Clinical Implications
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Watanabe, Y.; Yamada, Y.; Fukumoto, Y.; Ishihara, T.; Yokoyama, K.; Yoshida, T.; Miyake, M.; Yamagata, E.; Kimura, M. Echo Intensity Obtained from Ultrasonography Images Reflecting Muscle Strength in Elderly Men. Clin. Interv. Aging 2013, 8, 993–998. [Google Scholar] [CrossRef] [Green Version]
- Robbins, J.; Humpal, N.S.; Banaszynski, K.; Hind, J.; Rogus-Pulia, N. Age-Related Differences in Pressures Generated During Isometric Presses and Swallows by Healthy Adults. Dysphagia 2016, 31, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Sanders, I.; Mu, L. A Three-Dimensional Atlas of Human Tongue Muscles. Anat. Rec. 2013, 296, 1102–1114. [Google Scholar] [CrossRef] [Green Version]
- Sakamoto, Y. Structural Arrangement of the Intrinsic Muscles of the Tongue and Their Relationships with the Extrinsic Muscles. Surg. Radiol. Anat. 2018, 40, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Fukumoto, Y.; Ikezoe, T.; Yamada, Y.; Tsukagoshi, R.; Nakamura, M.; Mori, N.; Kimura, M.; Ichihashi, N. Skeletal Muscle Quality Assessed from Echo Intensity Is Associated with Muscle Strength of Middle-Aged and Elderly Persons. Eur. J. Appl. Physiol. 2012, 112, 1519–1525. [Google Scholar] [CrossRef] [Green Version]
- Fukumoto, Y.; Ikezoe, T.; Yamada, Y.; Tsukagoshi, R.; Nakamura, M.; Takagi, Y.; Kimura, M.; Ichihashi, N. Age-Related Ultrasound Changes in Muscle Quantity and Quality in Women. Ultrasound Med. Biol. 2015, 41, 3013–3017. [Google Scholar] [CrossRef] [Green Version]
- Chantaramanee, A.; Tohara, H.; Nakagawa, K.; Hara, K.; Nakane, A.; Yamaguchi, K.; Yoshimi, K.; Junichi, F.; Minakuchi, S. Association Between Echo Intensity of the Tongue and Its Thickness and Function in Elderly Subjects. J. Oral Rehabil. 2019, 46, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, N.; Mori, T.; Fujishima, I.; Wakabayashi, H.; Itoda, M.; Kunieda, K.; Shigematsu, T.; Nishioka, S.; Tohara, H.; Yamada, M.; et al. Ultrasonography to Measure Swallowing Muscle Mass and Quality in Older Patients with Sarcopenic Dysphagia. J. Am. Med. Dir. Assoc. 2018, 19, 516–522. [Google Scholar] [CrossRef]
- Tamura, F.; Kikutani, T.; Tohara, T.; Yoshida, M.; Yaegaki, K. Tongue Thickness Relates to Nutritional Status in the Elderly. Dysphagia 2012, 27, 556–561. [Google Scholar] [CrossRef] [Green Version]
- Shalev-Shwartz, S.; Ben-David, S. Understanding Machine Learning: From Theory to Algorithms; Cambridge University Press: Cambridge, UK, 2014. [Google Scholar]
- Kambatla, K.; Kollias, G.; Kumar, V.; Grama, A. Trends in Big Data Analytics. J. Parallel Distrib. Comput. 2014, 74, 2561–2573. [Google Scholar] [CrossRef]
- Al-Naami, B.; Bashir, A.; Amasha, H.; Al-Nabulsi, J.; Almalty, A.M. Statistical Approach for Brain Cancer Classification Using a Region Growing Threshold. J. Med. Syst. 2011, 35, 463–471. [Google Scholar] [CrossRef]
- Ding, J.; Cheng, H.D.; Huang, J.; Liu, J.; Zhang, Y. Breast Ultrasound Image Classification Based on Multiple-Instance Learning. J. Digit. Imaging 2012, 25, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Übeyli, E.D.; Doğdu, E. Automatic Detection of Erythemato-Squamous Diseases Using k-Means Clustering. J. Med. Syst. 2010, 34, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Estivill-Castro, V. Why So Many Clustering Algorithms: A Position Paper. SIGKDD Explor. Newsl. 2002, 4, 65–75. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Science, 2nd ed.; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Dupont, W.D.; Plummer, W.D. Power and Sample Size Calculations for Studies Involving Linear Regression. Control. Clin. Trials 1998, 19, 589–601. [Google Scholar] [CrossRef]
- Utanohara, Y.; Hayashi, R.; Yoshikawa, M.; Yoshida, M.; Tsuga, K.; Akagawa, Y. Standard Values of Maximum Tongue Pressure Taken Using Newly Developed Disposable Tongue Pressure Measurement Device. Dysphagia 2008, 23, 286–290. [Google Scholar] [CrossRef]
- Sarukawa, S.; Noguchi, T.; Miyazaki, K.; Itoh, H.; Nishino, H.; Kusama, M.; Sugawara, Y.; Kawada, K. Development of a Tool for Speech Intelligibility Evaluation After Glossectomy: The TKR Speech Test. Jpn. J. Head Neck Cancer 2013, 39, 374–378. [Google Scholar]
- Alpaydin, E. Introduction to Machine Learning, 3rd ed; MIT Press: Cambridge, MA, USA, 2014. [Google Scholar]
- Thinsungnoena, T.; Kaoungkub, N.; Durongdumronchaib, P.; Kerdprasopb, K.; Kerdprasop, N. (Eds.) The Clustering Validity with Silhouette and Sum of Squared Errors. In Proceedings of the 3rd International Conference on Industrial Application Engineering (ICIAE2015), Tokyo, Japan, 14–16 March 2015. [Google Scholar]
- Bholowalia, P.; Kumar, A. EBK-Means: A Clustering Technique Based on Elbow Method and k-Means in WSN. Int. J. Comput. Appl. 2014, 105, 17–24. [Google Scholar]
- Charrad, M.; Ghazzali, N.; Boiteau, V.; Niknafs, A. NbClust: An R Package for Determining the Relevant Number of Clusters in a Data Set. J. Stat. Soft. 2014, 61, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Hamahata, A.; Beppu, T.; Shirakura, S.; Hatanaka, A.; Yamaki, T.; Saitou, T.; Sakurai, H. Tongue Pressure in Patients with Tongue Cancer Resection and Reconstruction. Auris Nasus Larynx 2014, 41, 563–567. [Google Scholar] [CrossRef]
- Shaker, R.; Cook, I.J.; Dodds, W.J.; Hogan, W.J. Pressure-Flow Dynamics of the Oral Phase of Swallowing. Dysphagia 1988, 3, 79–84. [Google Scholar] [CrossRef]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef] [PubMed]
- Umemoto, G.; Furuya, H.; Arahata, H.; Sugahara, M.; Sakai, M.; Tsuboi, Y. Relationship Between Tongue Thickness and Tongue Pressure in Neuromuscular Disorders. Neurol. Clin. Neurosci. 2016, 4, 142–145. [Google Scholar] [CrossRef] [Green Version]
- Akima, H.; Yoshiko, A.; Hioki, M.; Kanehira, N.; Shimaoka, K.; Koike, T.; Sakakibara, H.; Oshida, Y. Skeletal Muscle Size Is a Major Predictor of Intramuscular Fat Content Regardless of Age. Eur. J. Appl. Physiol. 2015, 115, 1627–1635. [Google Scholar] [CrossRef] [PubMed]
- Akima, H.; Yoshiko, A.; Tomita, A.; Ando, R.; Saito, A.; Ogawa, M.; Kondo, S.; Tanaka, N.I. Relationship Between Quadriceps Echo Intensity and Functional and Morphological Characteristics in Older Men and Women. Arch. Gerontol. Geriatr. 2017, 70, 105–111. [Google Scholar] [CrossRef]
- Strasser, E.M.; Draskovits, T.; Praschak, M.; Quittan, M.; Graf, A. Association Between Ultrasound Measurements of Muscle Thickness, Pennation Angle, Echogenicity and Skeletal Muscle Strength in the Elderly. Age 2013, 35, 2377–2388. [Google Scholar] [CrossRef] [Green Version]
- Neel, A.T.; Palmer, P.M. Is Tongue Strength an Important Influence on Rate of Articulation in Diadochokinetic and Reading Tasks? J. Speech Lang. Hear. Res. 2012, 55, 235–246. [Google Scholar] [CrossRef]
- Hiramatsu, T.; Kataoka, H.; Osaki, M.; Hagino, H. Effect of Aging on Oral and Swallowing Function After Meal Consumption. Clin. Interv. Aging 2015, 10, 229–235. [Google Scholar] [PubMed] [Green Version]
- Zhang, J.; Jiang, W.; Wang, R.; Wang, L. Brain MR Image Segmentation with Spatial Constrained k-Mean Algorithm and Dual-Tree Complex Wavelet Transform. J. Med. Syst. 2014, 38, 93. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Nakagawa, K.; Yoshimi, K.; Chantaramanee, A.; Nakane, A.; Furuya, J.; Tohara, H. Age-related changes in swallowing muscle intramuscular adipose tissue deposition and related factors. Exp. Gerontol. 2021, 1, 111505. [Google Scholar] [CrossRef]
- McIlduff, C.E.; Martucci, M.G.; Shin, C.; Qi, K.; Pacheck, A.K.; Gutierrez, H.; Mortreux, M.; Rutkove, S.B. Quantitative ultrasound of the tongue: Echo intensity is a potential biomarker of bulbar dysfunction in amyotrophic lateral sclerosis. Clin. Neurophysiol. 2020, 131, 2423–2428. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in Elderly People. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Namiki, C.; Hara, K.; Tohara, H.; Kobayashi, K.; Chantaramanee, A.; Nakagawa, K.; Saitou, T.; Yamaguchi, K.; Yoshimi, K.; Nakane, A.; et al. Tongue-Pressure Resistance Training Improves Tongue and Suprahyoid Muscle Functions Simultaneously. Clin. Interv. Aging 2019, 14, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, K.; Tohara, H.; Hara, K.; Nakane, A.; Kajisa, E.; Yoshimi, K.; Minakuchi, S. Relationship of Aging, Skeletal Muscle Mass, and Tooth Loss with Masseter Muscle Thickness. BMC Geriatr. 2018, 18, 67. [Google Scholar] [CrossRef] [PubMed]
- Sakayori, T.; Maki, Y.; Hirata, S.; Okada, M.; Ishii, T. Evaluation of a Japanese “Prevention of Long-Term Care” Project for the Improvement in Oral Function in the High-Risk Elderly. Geriatr. Gerontol. Int. 2013, 13, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Umemori, N.; Kakinoki, Y.; Karaki, J.; Kakigawa, H. New method for determining surface roughness of tongue. Gerodontology. 2012, 29, 90–95. [Google Scholar] [CrossRef]
- Kikutani, T.; Tamura, F.; Nishiwaki, K.; Suda, M.; Kayanaka, H.; Machida, R.; Yoshida, M.; Akagawa, Y. The degree of tongue-coating reflects lingual motor function in the elderly. Gerodontology 2009, 26, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Pillen, S.; Arts, I.M.P.; Zwarts, M.J. Muscle ultrasound in neuromuscular disorders. Muscle Nerve. 2008, 37, 679–693. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Group 1 (Mean ± Standard Deviation) | Group 2 (Mean ± Standard Deviation) | Group 3 (Mean ± Standard Deviation) | Range | p-Value (ANOVA †) |
|---|---|---|---|---|---|
| Physical data | |||||
| Number | 54 | 109 | 73 | - | - |
| Sex (female, %) | 71.6 | 74.1 | 64.4 | - | - |
| Age (years) | 72.6 ± 5.0 | 69.8 ± 5.6 | 71.0 ± 5.2 | 65.0–86.0 | 0.007 |
| BMI ‡ (kg/m2) | 23.4 ± 2.9 | 22.7 ± 2.9 | 22.4 ± 2.7 | 14.0–32.4 | 0.154 |
| Ultrasonographic data | |||||
| Tongue thickness (mm) | 37.6 ± 3.7 | 40.5 ± 3.5 | 44.0 ± 4.2 | 29.2–54.3 | <0.001 |
| Echo intensity | 55.1 ± 4.7 | 42.8 ± 3.5 | 32.2 ± 4.1 | 21.1–66.8 | <0.001 |
| Tongue function data | |||||
| Tongue pressure (kPa) | 28.7 ± 9.9 | 32.3 ± 7.1 | 31.4 ± 8.2 | 4.9–53.3 | 0.030 |
| /ta/ | 5.6 ± 1.1 | 6.1 ± 1.2 | 6.2 ± 0.8 | 3.2–9.2 | 0.005 |
| /ka/ | 5.4 ± 1.1 | 5.8 ± 1.1 | 5.7 ± 0.8 | 2.4–10.2 | 0.040 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chantaramanee, A.; Nakagawa, K.; Yoshimi, K.; Nakane, A.; Yamaguchi, K.; Tohara, H. Comparison of Tongue Characteristics Classified According to Ultrasonographic Features Using a K-Means Clustering Algorithm. Diagnostics 2022, 12, 264. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020264
Chantaramanee A, Nakagawa K, Yoshimi K, Nakane A, Yamaguchi K, Tohara H. Comparison of Tongue Characteristics Classified According to Ultrasonographic Features Using a K-Means Clustering Algorithm. Diagnostics. 2022; 12(2):264. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020264
Chicago/Turabian StyleChantaramanee, Ariya, Kazuharu Nakagawa, Kanako Yoshimi, Ayako Nakane, Kohei Yamaguchi, and Haruka Tohara. 2022. "Comparison of Tongue Characteristics Classified According to Ultrasonographic Features Using a K-Means Clustering Algorithm" Diagnostics 12, no. 2: 264. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020264