
Image-Quality Assessment of Polyenergetic and Virtual Monoenergetic Reconstructions of Unenhanced CT Scans of the Head: Initial Experiences with the First Photon-Counting CT Approved for Clinical Use

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. CT Protocols and Image Acquisition
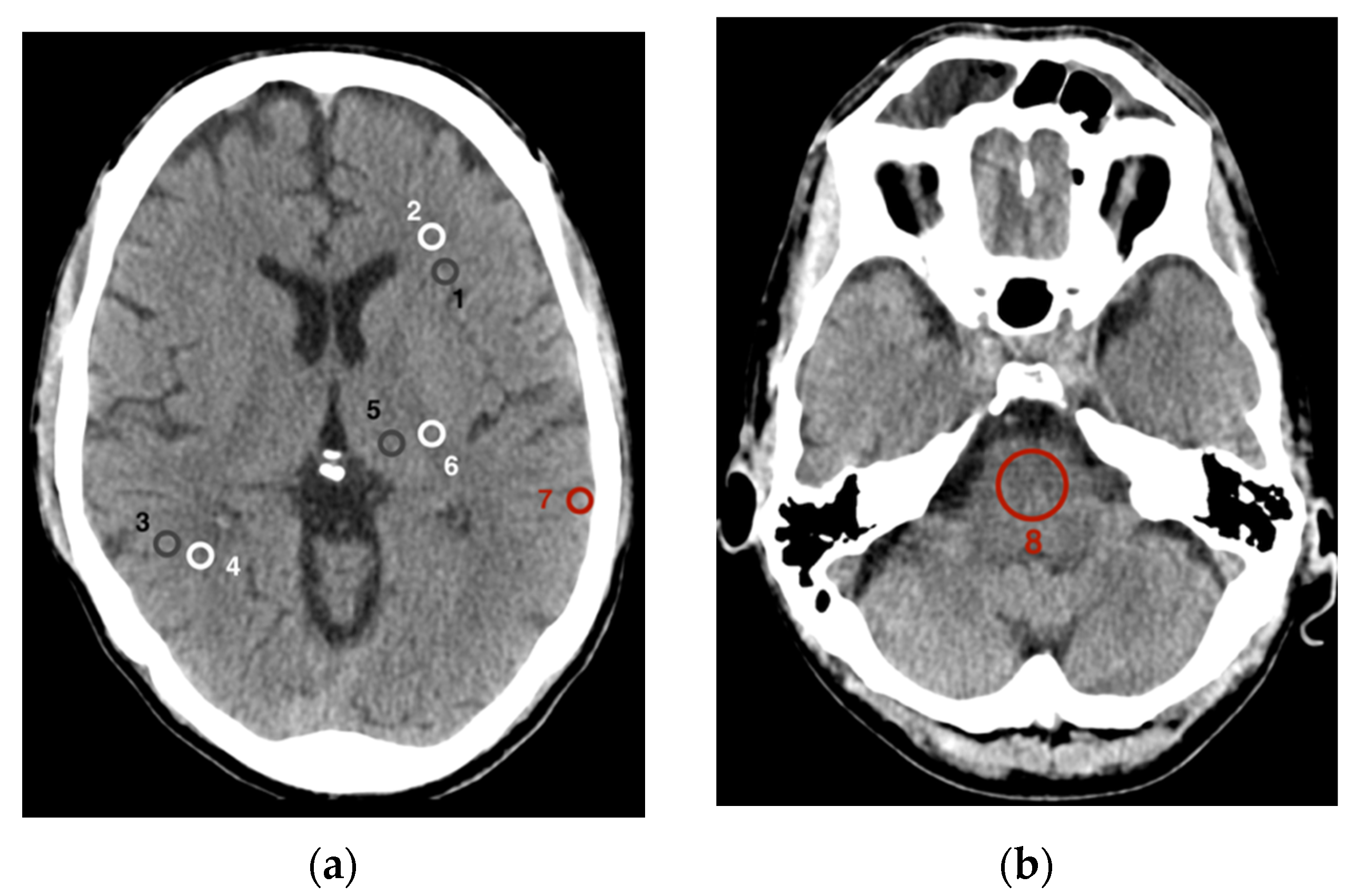
2.3. Quantitative Image Analysis
2.4. Statistical Analysis
3. Results
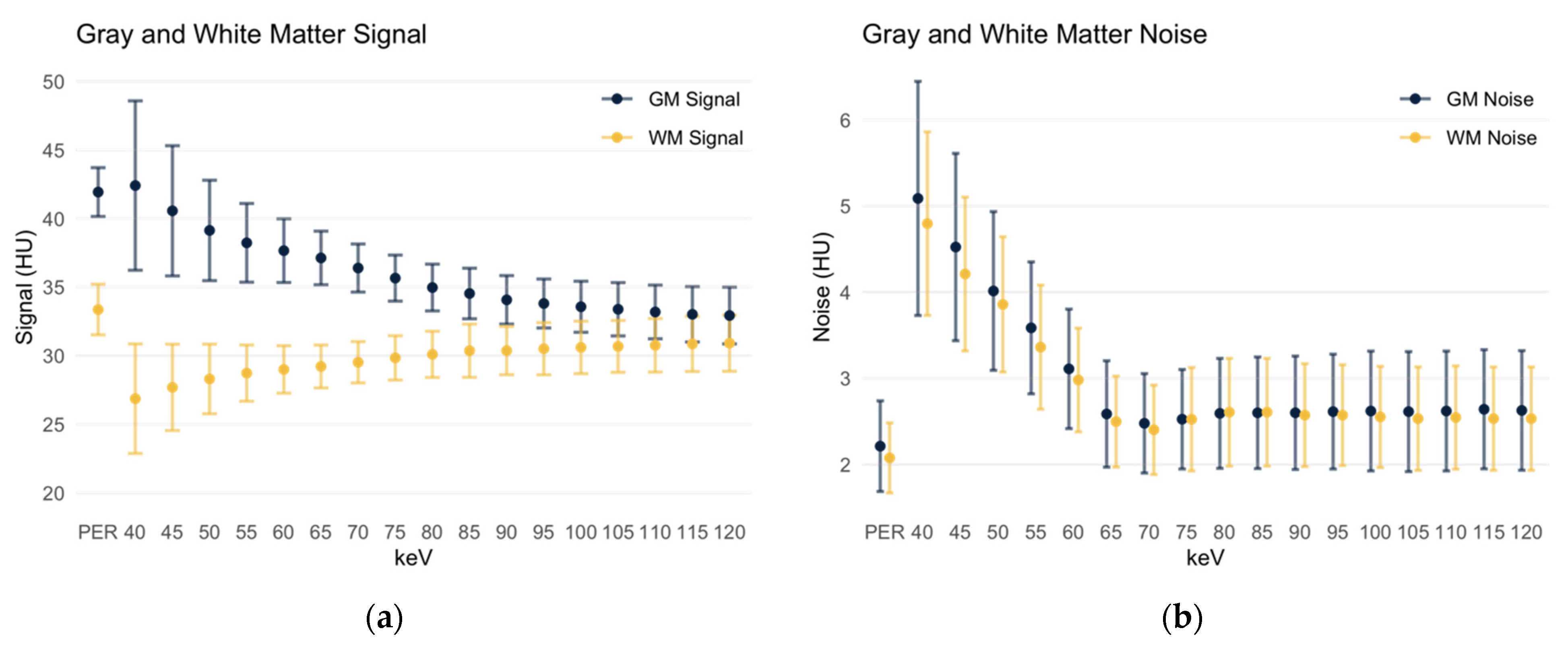
3.1. Signal and Noise in Gray and White Matter
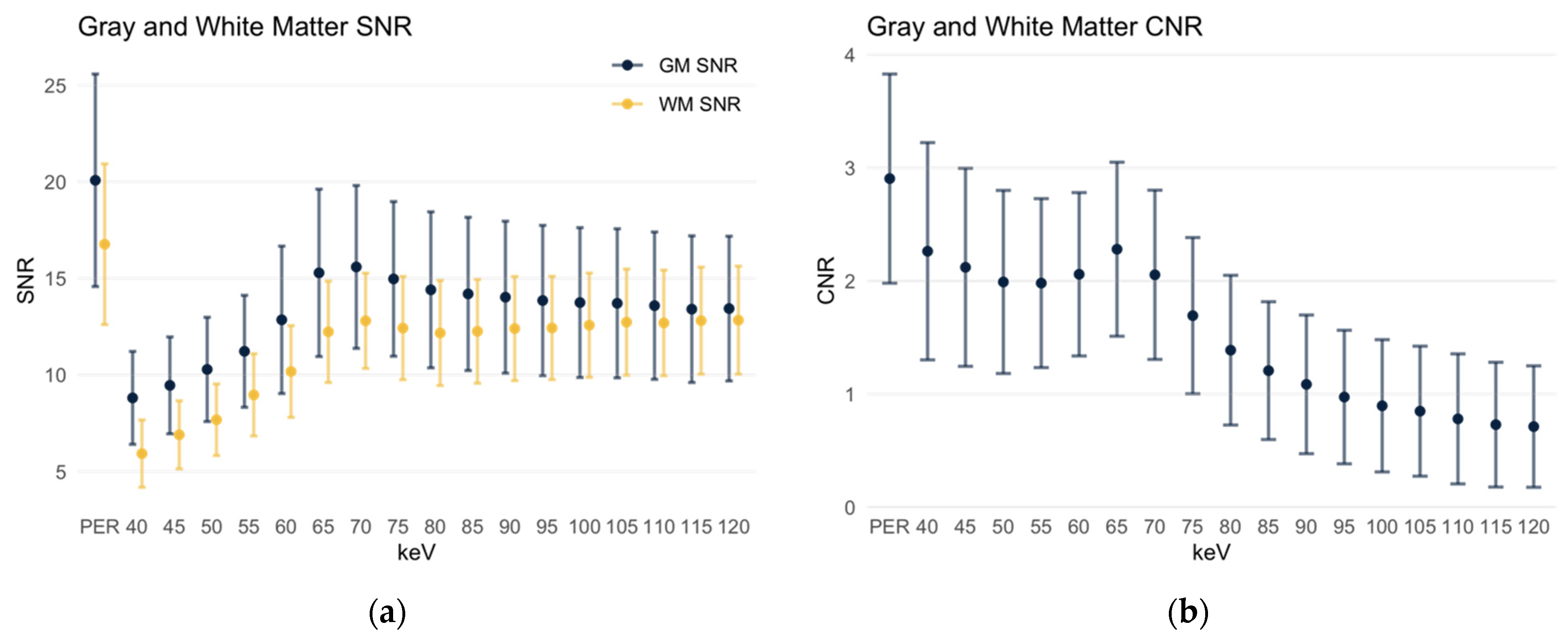
3.2. Signal-to-Noise-Ratio of Gray and White Matter
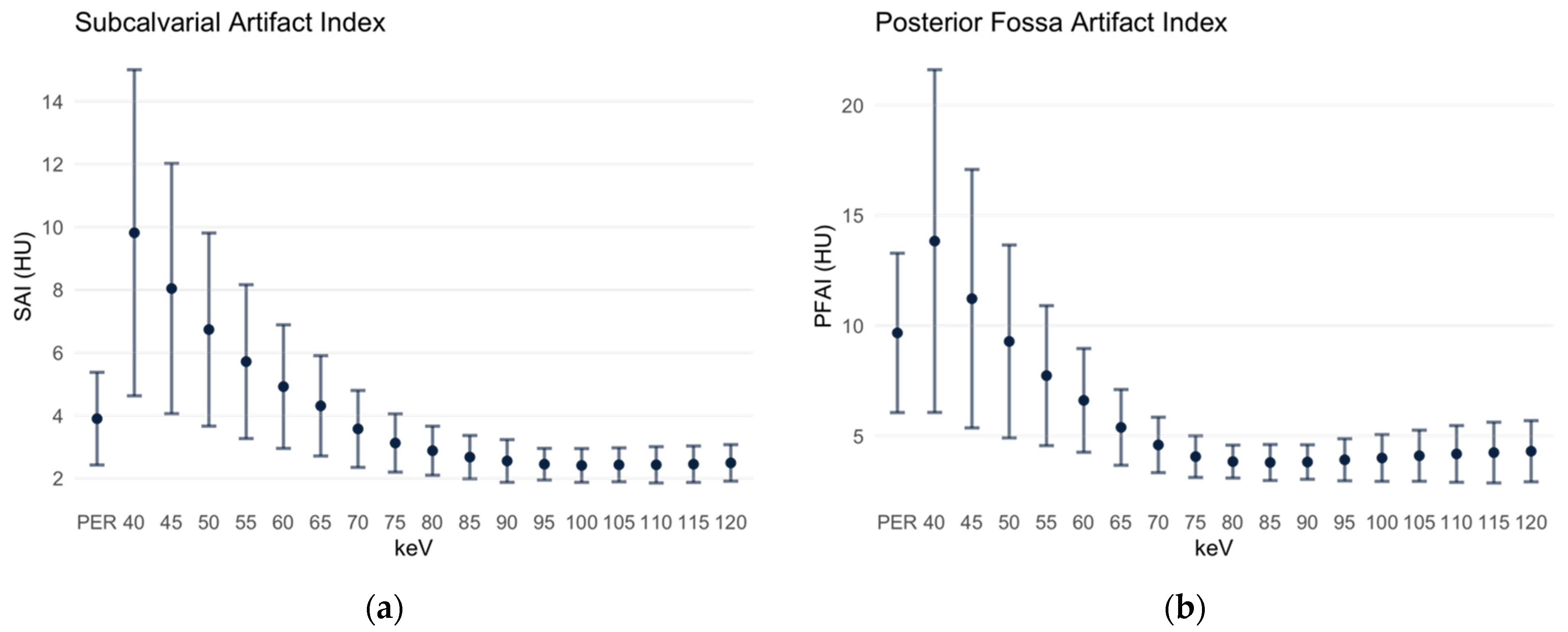
3.3. Subcalvarial and Posterior Fossa Artifact Indices
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lell, M.M.; Kachelrieß, M. Recent and Upcoming Technological Developments in Computed Tomography: High Speed, Low Dose, Deep Learning, Multienergy. Investig. Radiol. 2020, 55, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.H.; Burke, C.J.; Howlett, D. Cranial computed tomography 2: Use in clinical practice. Br. J. Hosp. Med. 2010, 71, 514–519. [Google Scholar] [CrossRef]
- Odle, T. Emergency Computed Tomography. Radiol. Technol. 2020, 91, 267ct–287ct. [Google Scholar]
- Garcia-Esperon, C.; Bivard, A.; Levi, C.; Parsons, M. Use of computed tomography perfusion for acute stroke in routine clinical practice: Complex scenarios, mimics, and artifacts. Int. J. Stroke 2018, 13, 469–472. [Google Scholar] [CrossRef] [PubMed]
- News Release. Siemens Launches World’s First Photon-Counting CT Scanner. Appl. Radiol. 2021. Available online: https://appliedradiology.com/communities/CT-Imaging/siemens-launches-world-s-first-photon-counting-ct-scanner (accessed on 3 December 2021).
- Danielsson, M.; Persson, M.; Sjölin, M. Photon-counting X-ray detectors for CT. Phys. Med. Biol. 2021, 66, 03tr01. [Google Scholar] [CrossRef]
- Willemink, M.J.; Persson, M.; Pourmorteza, A.; Pelc, N.J.; Fleischmann, D. Photon-counting CT: Technical Principles and Clinical Prospects. Radiology 2018, 289, 293–312. [Google Scholar] [CrossRef]
- Flohr, T.; Petersilka, M.; Henning, A.; Ulzheimer, S.; Ferda, J.; Schmidt, B. Photon-counting CT review. Phys. Med. 2020, 79, 126–136. [Google Scholar] [CrossRef]
- Flohr, T.G.; McCollough, C.H.; Bruder, H.; Petersilka, M.; Gruber, K.; Süss, C.; Grasruck, M.; Stierstorfer, K.; Krauss, B.; Raupach, R.; et al. First performance evaluation of a dual-source CT (DSCT) system. European Radiol. 2006, 16, 256–268. [Google Scholar] [CrossRef]
- D’Angelo, T.; Cicero, G.; Mazziotti, S.; Ascenti, G.; Albrecht, M.H.; Martin, S.S.; Othman, A.E.; Vogl, T.J.; Wichmann, J.L. Dual energy computed tomography virtual monoenergetic imaging: Technique and clinical applications. Br. J. Radiol. 2019, 92, 20180546. [Google Scholar] [CrossRef]
- Alvarez, R.E.; Macovski, A. Energy-selective reconstructions in X-ray computerized tomography. Phys. Med. Biol. 1976, 21, 733–744. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Leng, S.; McCollough, C.H. Dual-energy CT-based monochromatic imaging. AJR Am. J. Roentgenol. 2012, 199, S9–S15. [Google Scholar] [CrossRef] [PubMed]
- Meinel, F.G.; Bischoff, B.; Zhang, Q.; Bamberg, F.; Reiser, M.F.; Johnson, T.R. Metal artifact reduction by dual-energy computed tomography using energetic extrapolation: A systematically optimized protocol. Investig. Radiol. 2012, 47, 406–414. [Google Scholar] [CrossRef]
- Neuhaus, V.; Abdullayev, N.; Große Hokamp, N.; Pahn, G.; Kabbasch, C.; Mpotsaris, A.; Maintz, D.; Borggrefe, J. Improvement of Image Quality in Unenhanced Dual-Layer CT of the Head Using Virtual Monoenergetic Images Compared With Polyenergetic Single-Energy CT. Investig. Radiol. 2017, 52, 470–476. [Google Scholar] [CrossRef]
- Pourmorteza, A.; Symons, R.; Reich, D.S.; Bagheri, M.; Cork, T.E.; Kappler, S.; Ulzheimer, S.; Bluemke, D.A. Photon-Counting CT of the Brain: In Vivo Human Results and Image-Quality Assessment. AJNR Am. J. Neuroradiol. 2017, 38, 2257–2263. [Google Scholar] [CrossRef] [Green Version]
- Pomerantz, S.R.; Kamalian, S.; Zhang, D.; Gupta, R.; Rapalino, O.; Sahani, D.V.; Lev, M.H. Virtual monochromatic reconstruction of dual-energy unenhanced head CT at 65–75 keV maximizes image quality compared with conventional polychromatic CT. Radiology 2013, 266, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Rozeik, C.; Kotterer, O.; Preiss, J.; Schütz, M.; Dingler, W.; Deininger, H.K. Cranial CT artifacts and gantry angulation. J. Comput. Assist. Tomogr. 1991, 15, 381–386. [Google Scholar] [CrossRef]
- Zhao, X.M.; Wang, M.; Wu, R.Z.; Dharaiya, E.; Feng, F.; Li, M.L.; You, H.; Wang, Y.; Wang, Y.N.; Jin, Z.Y. Dual-layer spectral detector CT monoenergetic reconstruction improves image quality of non-contrast cerebral CT as compared with conventional single energy CT. Eur. J. Radiol. 2018, 103, 131–138. [Google Scholar] [CrossRef]
- Kursun-Cakmak, E.; Demirturk Kocasarac, H.; Bayrak, S.; Ustaoğlu, G.; Noujeim, M. Estimation of contrast-to-noise ratio in CT and CBCT images with varying scan settings in presence of different implant materials. Dentomaxillofac. Radiol. 2019, 48, 20190139. [Google Scholar] [CrossRef]
- Shikhaliev, P.M. Beam hardening artefacts in computed tomography with photon counting, charge integrating and energy weighting detectors: A simulation study. Phys. Med. Biol. 2005, 50, 5813–5827. [Google Scholar] [CrossRef]
- Hwang, W.D.; Mossa-Basha, M.; Andre, J.B.; Hippe, D.S.; Culbertson, S.; Anzai, Y. Qualitative Comparison of Noncontrast Head Dual-Energy Computed Tomography Using Rapid Voltage Switching Technique and Conventional Computed Tomography. J. Comput. Assist. Tomogr. 2016, 40, 320–325. [Google Scholar] [CrossRef]
- Hixson, H.R.; Leiva-Salinas, C.; Sumer, S.; Patrie, J.; Xin, W.; Wintermark, M. Utilizing dual energy CT to improve CT diagnosis of posterior fossa ischemia. J. Neuroradiol. 2016, 43, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.Z.; Miao, F.; Li, J.Y.; Dong, H.P.; Shen, Y.; Chen, K.M. High-definition CT Gemstone spectral imaging of the brain: Initial results of selecting optimal monochromatic image for beam-hardening artifacts and image noise reduction. J. Comput. Assist. Tomogr. 2011, 35, 294–297. [Google Scholar] [CrossRef]
- Lennartz, S.; Laukamp, K.R.; Neuhaus, V.; Große Hokamp, N.; Le Blanc, M.; Maus, V.; Kabbasch, C.; Mpotsaris, A.; Maintz, D.; Borggrefe, J. Dual-layer detector CT of the head: Initial experience in visualization of intracranial hemorrhage and hypodense brain lesions using virtual monoenergetic images. Eur. J. Radiol. 2018, 108, 177–183. [Google Scholar] [CrossRef]
- Goldman, L.W. Principles of CT: Radiation dose and image quality. J. Nucl. Med. Technol. 2007, 35, 213–225. [Google Scholar] [CrossRef] [Green Version]
- Kalender, W.; Bautz, W.; Felsenberg, D.; Süss, C.; Klotz, E. Material-selective imaging and density measurement using the dual-energy method. I. Principles and methodology. Digit. Bilddiagn. 1987, 7, 66–72. [Google Scholar]
- Albrecht, M.H.; Vogl, T.J.; Martin, S.S.; Nance, J.W.; Duguay, T.M.; Wichmann, J.L.; Cecco, C.N.D.; Varga-Szemes, A.; Assen, M.V.; Tesche, C.; et al. Review of Clinical Applications for Virtual Monoenergetic Dual-Energy CT. Radiology 2019, 293, 260–271. [Google Scholar] [CrossRef]
- Grant, K.L.; Flohr, T.G.; Krauss, B.; Sedlmair, M.; Thomas, C.; Schmidt, B. Assessment of an advanced image-based technique to calculate virtual monoenergetic computed tomographic images from a dual-energy examination to improve contrast-to-noise ratio in examinations using iodinated contrast media. Investig. Radiol. 2014, 49, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.K.; Huang, H.M. Noise reduction in dual-energy computed tomography virtual monoenergetic imaging. J. Appl. Clin. Med. Phys. 2019, 20, 104–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Image-Quality Parameter | Polyenergetic Reconstruction | Monoenergetic Reconstruction | p Value |
|---|---|---|---|
| GM Signal | 41.93 ± 1.78 | 40 keV: 42.41 ± 6.17 120 keV: 32.93 ± 2.07 | p = 0.540 p < 0.001 |
| WM Signal | 33.37 ± 1.84 | 40 keV: 26.87 ± 3.99 120 keV: 30.92 ± 2.05 | p < 0.001 p < 0.001 |
| GM Noise | 2.21 ± 0.53 | 40 keV: 5.09 ± 1.36 120 keV: 2.63 ± 0.69 | p < 0.001 p < 0.001 |
| WM Noise | 2.07 ± 0.41 | 40 keV: 4.8 ± 1.07 120 keV: 2.53 ± 0.6 | p < 0.001 p < 0.001 |
| GM SNR | 20.08 ± 5.5 | 70 keV: 15.59 ± 4.22 | p < 0.001 |
| WM SNR | 16.77 ± 4.16 | 70 keV: 12.8 ± 2.47 | p < 0.001 |
| GM-WM CNR | 2.90 ± 0.92 | 65 keV: 2.28 ± 0.77 | p < 0.001 |
| SAI | 3.90 ± 1.48 | 40 keV: 9.82 ± 5.19 70 keV: 3.57 ± 1.22 120 keV: 2.49 ± 0.58 | p < 0.001 p = 0.324 p < 0.001 |
| PFAI | 9.67 ± 3.61 | 40 keV: 13.84 ± 7.77 85 keV: 3.8 ± 0.82 120 keV: 4.31 ± 1.39 | p < 0.001 p < 0.001 p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michael, A.E.; Boriesosdick, J.; Schoenbeck, D.; Woeltjen, M.M.; Saeed, S.; Kroeger, J.R.; Horstmeier, S.; Lennartz, S.; Borggrefe, J.; Niehoff, J.H. Image-Quality Assessment of Polyenergetic and Virtual Monoenergetic Reconstructions of Unenhanced CT Scans of the Head: Initial Experiences with the First Photon-Counting CT Approved for Clinical Use. Diagnostics 2022, 12, 265. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020265
Michael AE, Boriesosdick J, Schoenbeck D, Woeltjen MM, Saeed S, Kroeger JR, Horstmeier S, Lennartz S, Borggrefe J, Niehoff JH. Image-Quality Assessment of Polyenergetic and Virtual Monoenergetic Reconstructions of Unenhanced CT Scans of the Head: Initial Experiences with the First Photon-Counting CT Approved for Clinical Use. Diagnostics. 2022; 12(2):265. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020265
Chicago/Turabian StyleMichael, Arwed Elias, Jan Boriesosdick, Denise Schoenbeck, Matthias Michael Woeltjen, Saher Saeed, Jan Robert Kroeger, Sebastian Horstmeier, Simon Lennartz, Jan Borggrefe, and Julius Henning Niehoff. 2022. "Image-Quality Assessment of Polyenergetic and Virtual Monoenergetic Reconstructions of Unenhanced CT Scans of the Head: Initial Experiences with the First Photon-Counting CT Approved for Clinical Use" Diagnostics 12, no. 2: 265. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020265