
Look beyond the Mirror: Laparoscopic Cholecystectomy in Situs Inversus Totalis—A Systematic Review and Meta-Analysis (and Report of New Technique)

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Definition of Situs Inversus Totalis
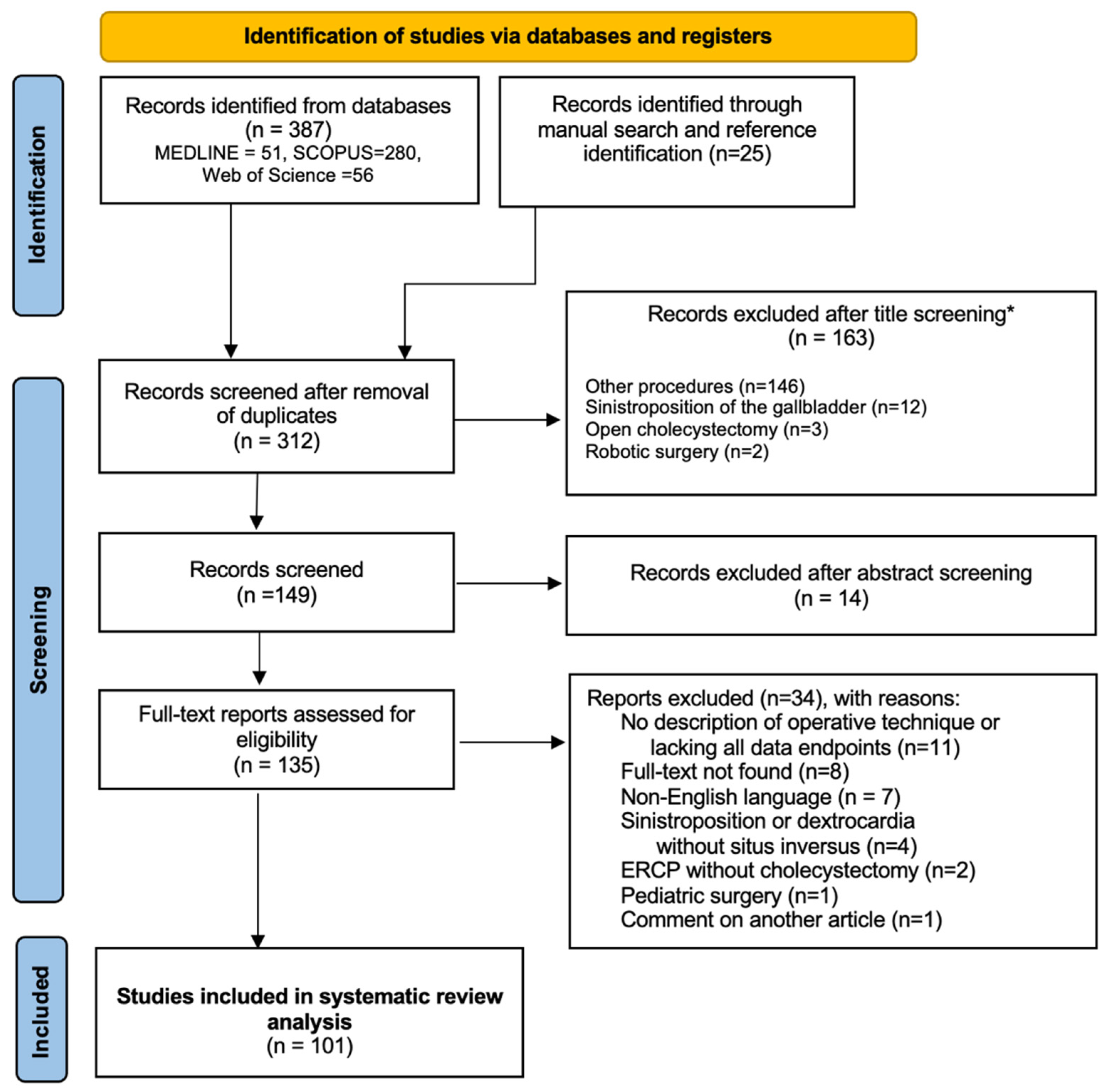
2.2. Research Strategy and Articles Inclusion
2.3. Bias Risk Assessment in Results of Included Studies and Results of Meta-Analysis
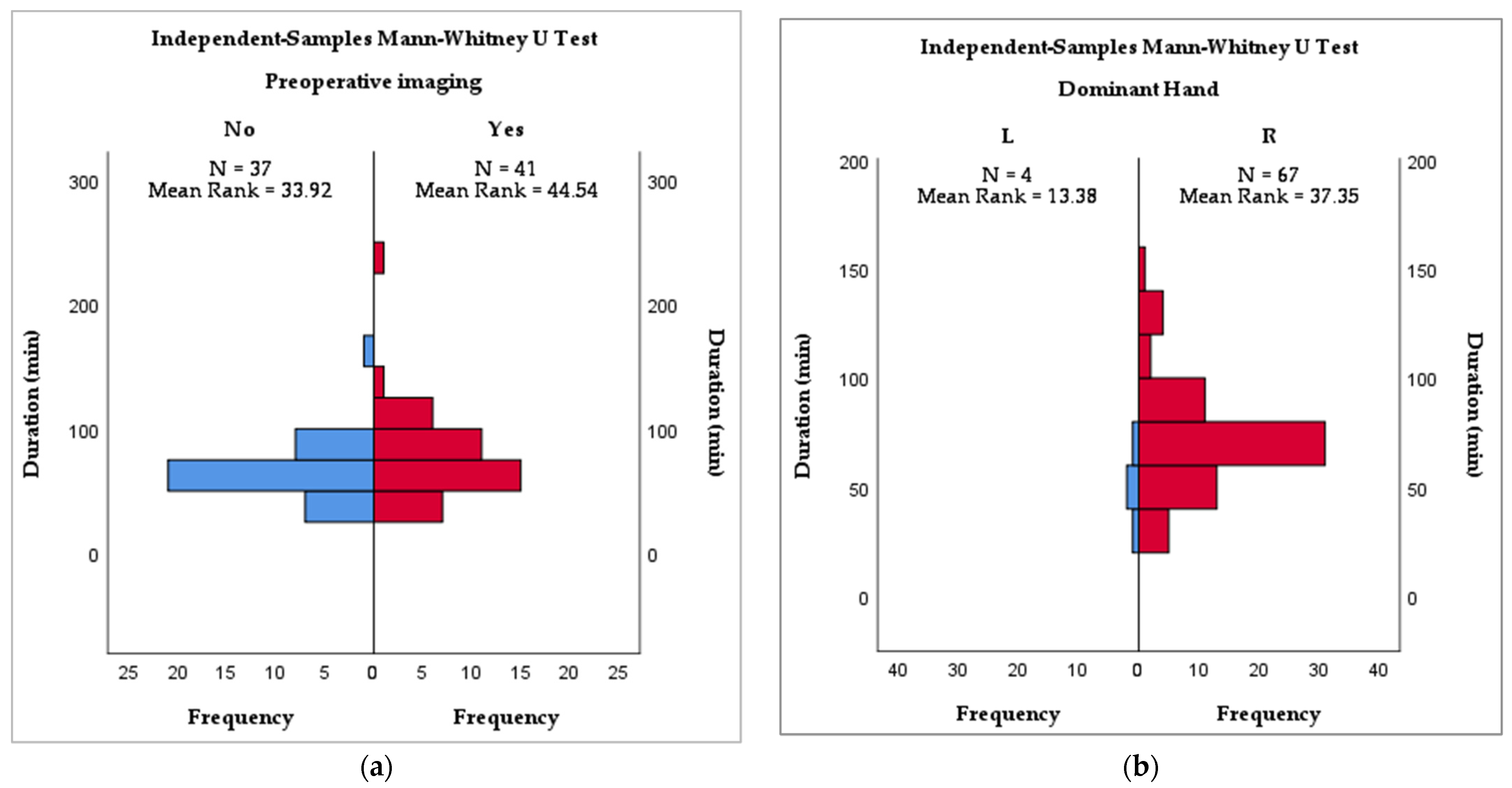
2.4. Data Extraction and Statistical Analysis
3. Results
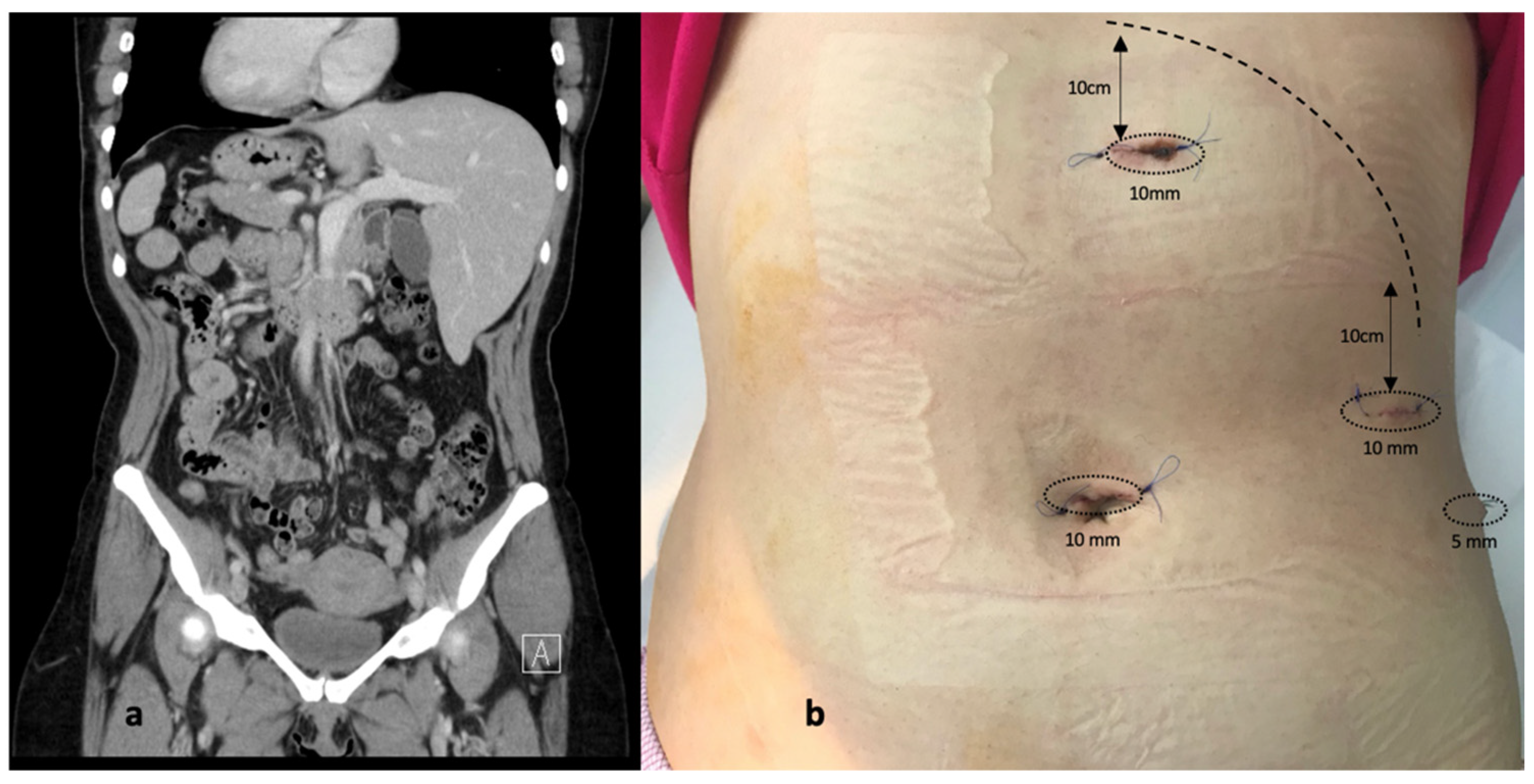
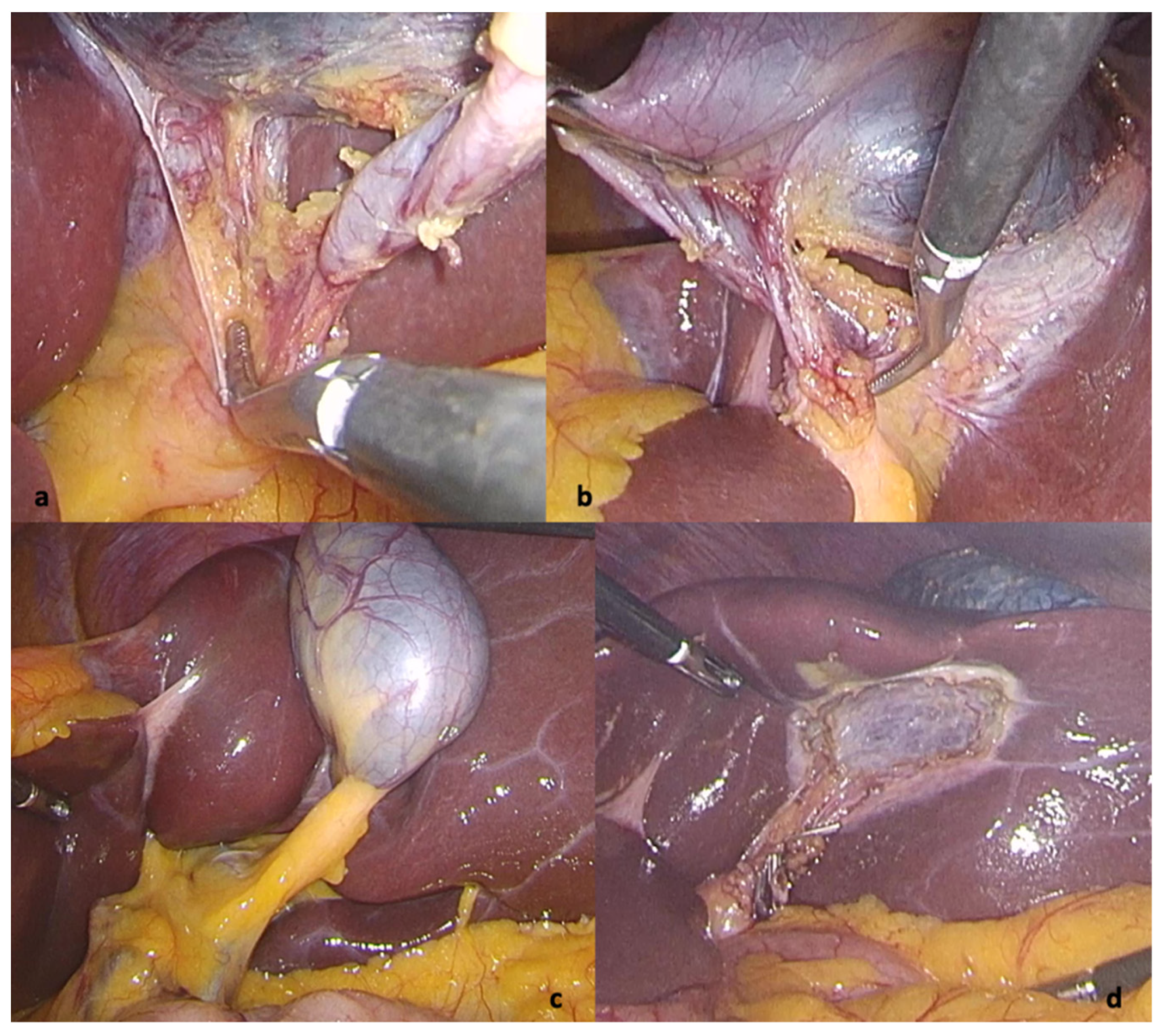
3.1. Case Report
3.2. Literature Review
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mayo, C.W.; Rice, R.G. SITUS INVERSUS TOTALIS: A Statistical Review of Data on Seventy-Six Cases with Special Reference To Disease of the Biliary Tract. Arch. Surg. 1949, 58, 724–730. [Google Scholar] [CrossRef]
- Campos, L.; Sipes, E. Laparoscopic Cholecystectomy in a 39-Year-Old Female with Situs Inversus. J. Laparoendosc. Surg. 1991, 1, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Chaouch, M.A.; Jerraya, H.; Dougaz, M.W.; Nouira, R.; Dziri, C. A Systematic Review of Laparoscopic Cholecystectomy in Situs Inversus. J. Investig. Surg. 2019, 34, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Declaration of Helsinki—WMA—The World Medical Association. Available online: https://www.wma.net/what-we-do/medical-ethics/declaration-of-helsinki/ (accessed on 14 February 2022).
- Situs Ambiguus—An Overview|ScienceDirect Topics. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/topics/medicine-and-dentistry/situs-ambiguus (accessed on 13 February 2022).
- Higgins, J.P.; Savović, J.; Page, M.J.; Sterne, J.A.C. Revised Cochrane Risk-of-Bias Tool for Randomized Trials (RoB 2) Full Guidance Document. Br. Med. J. 2019, 366, l4898. [Google Scholar]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F.; Mohammad, D.; Murad, H. Methodological Quality and Synthesis of Case Series and Case Reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Mohammed, A.A.; Arif, S.H. Laparoscopic Cholecystectomy for Left-Sided Gall Bladder in Situs Inversus Totalis Patient, a Technically Demanding Procedure. Ann. Med. Surg. 2019, 47, 1–4. [Google Scholar] [CrossRef]
- Takalkar, Y.P.; Koranne, M.S.; Vashist, K.S.; Khedekar, P.G.; Garale, M.N.; Rege, S.A.; Dalvi, A.N. Laparoscopic Cholecystectomy with Choledochoduodenostomy in a Patient with Situs Inversus Totalis. J. Minimal Access Surg. 2018, 14, 241–243. [Google Scholar] [CrossRef]
- Reitano, E.; de’Angelis, N.; Schembari, E.; Carrà, M.C.; Francone, E.; Gentilli, S.; La Greca, G. Learning Curve for Laparoscopic Cholecystectomy Has Not Been Defined: A Systematic Review. ANZ J. Surg. 2021, 91, E554–E560. [Google Scholar] [CrossRef]
- Schott, G.D. Mirror Writing: Neurological Reflections on an Unusual Phenomenon. J. Neurol. Neurosurg. Psychiatry 2007, 78, 5–13. [Google Scholar] [CrossRef]
- Hamdorf, J.M.; Hall, J.C. Acquiring Surgical Skills. Br. J Surg 1999, 87, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Abboudi, H.; Khan, M.S.; Dasgupta, P.; Ahmed, K. Measuring the Surgical “Learning Curve”: Methods, Variables and Competency. BJU Int. 2014, 113, 504–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strasberg, S.M.; Brunt, L.M. The Critical View of Safety. Ann. Surg. 2017, 265, 464–465. [Google Scholar] [CrossRef] [PubMed]
- Yaghan, R.J.; Gharaibeh, K.I.; Hammori, S. Feasibility of Laparoscopic Cholecystectomy in Situs Inversus. J. Laparoendosc. Adv. Surg. Tech. 2001, 11, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Fanshawe, A.E.E.; Qurashi, K. Laparoscopic Cholecystectomy for Gallstone Pancreatitis in a Patient with Situs Inversus Totalis. J. Surg. Case Rep. 2017, 2017, rjx003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, Z.; Khan, S.A.; Chhabra, S.; Yadav, R.; Kumar, N.; Vij, V.; Saxena, D.; Talera, D.; Kankaria, J.; Gupta, S.; et al. Our Experience with Surgery in Situs Inversus: Open Peptic Perforation Repair and Laparoscopic Cholecystectomy in 1 Patient and 3 Patients Respectively. Int. J. Surg. Case Rep. 2016, 29, 34–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oms, L.M.; Badia, J.M. Laparoscopic Cholecystectomy in Situs Inversus Totalis: The Importance of Being Left-Handed. Surg. Endosc. Other Interv. Tech. 2003, 17, 1859–1861. [Google Scholar] [CrossRef]
- Peters, M.; Reimers, S.; Manning, J.T. Hand Preference for Writing and Associations with Selected Demographic and Behavioral Variables in 255,100 Subjects: The BBC Internet Study. Brain Cogn. 2006, 62, 177–189. [Google Scholar] [CrossRef]
- Anderson, M.; Carballo, E.; Hughes, D.; Behrer, C.; Reddy, R.M. Challenges Training Left-Handed Surgeons. Am. J. Surg. 2017, 214, 554–557. [Google Scholar] [CrossRef]
- Hanna, G.B.; Drew, T.; Clinch, P.; Shimi, S.; Dunkley, P.; Hau, C.; Cuschieri, A. Psychomotor Skills for Endoscopic Manipulations: Differing Abilities Between Right and Left-Handed Individuals. Ann. Surg. 1997, 225, 333–338. [Google Scholar] [CrossRef]
- Barbara, L.; Sama, C.; Labate, A.M.M.; Taroni, F.; Rusticali, A.G.; Festi, D.; Sapio, C.; Roda, E.; Banterle, C.; Puci, A.; et al. A Population Study on the Prevalence of Gallstone Disease: The Sirmione Study. Hepatology 1987, 7, 913–917. [Google Scholar] [CrossRef] [PubMed]
- Rojas, C.L.; Aguayo, W.G.; Molina, G.A.; Ochoa, C.; Neira, A.; Vinueza, M.E. Acute Cholecystitis and Residual Choledocholithiasis in a Situs Inversus Patient, Successful Laparoscopic Approach and ERCP a Case Report from Ecuador. Ann. Med. Surg. 2020, 54, 101–105. [Google Scholar] [CrossRef]
- Cociorvei, A.; Calu, V. Laparoscopic Ultrasound in Billiary Diseases. Chirurgia 2011, 106, 353–358. [Google Scholar]
- Calu, V.; Dumitrescu, I.; Miron, A. The Place of Laparoscopy in the Surgical Treatment of Scleroatrophic Cholecystitis. Chirurgia 2010, 105, 653–656. [Google Scholar] [PubMed]
- Patle, N.M.; Tantia, O.; Sasmal, P.K.; Khanna, S.; Sen, B. Laparoscopic Cholecystectomy In Situs Inversus-Our Experience of 6 Cases. Indian J. Surg. 2010, 72, 391–394. [Google Scholar] [CrossRef] [Green Version]
- Ren, J.J.; Li, S.D.; Geng, Y.J.; Xiao, R. Modified Laparoscopic Cholecystectomy Technique for Treatment of Situs Inversus Totalis: A Case Report. J. Int. Med. Res. 2017, 45, 1261–1267. [Google Scholar] [CrossRef] [Green Version]
- Al-Jumaily, M.; Achab, M.; Hoche, F. Laparoscopic Cholecystectomy in Situs Inversus Totalis: Is It Safe? J. Laparoendosc. Adv. Surg. Tech. 2001, 11, 229–231. [Google Scholar] [CrossRef]
- Aydin, U. Laparoscopic Cholecystectomy in a Patient with Situs Inversus Totalis. World J. Gastroenterol. 2006, 12, 7717. [Google Scholar] [CrossRef]
- Tavassoli, A.; Zandbaf, T.; Rezapanah, A. Laparoscopic Cholecystectomy In Situs Inversus, a Novel Port Placement Technique, Two Case Reports, and Review of Literature. Iran. Red Crescent Med. J. 2021, 23. [Google Scholar] [CrossRef]
- Tirelli, F.; Grieco, M.; Biondi, A.; Belia, F.; Persiani, R. Laparoscopic Cholecystectomy with Indocyanine Green Fluorescence in Patient with Situs Inversus Totalis. Mini-Invasive Surg. 2021, 5, 15. [Google Scholar] [CrossRef]
- Ali, M.S.; Attash, S.M. Laparoscopic Cholecystectomy in a Patient with Situs Inversus Totalis: Case Report with Review of Literature. BMJ Case Rep. 2013, 2013, bcr2013201231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akbulut, S.; Ulku, A.; Senol, A.; Tas, M.; Yagmur, Y. Left-Sided Appendicitis: Review of 95 Published Cases and a Case Report. World J. Gastroenterol. 2010, 16, 5598–5602. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, Y.; Fukunaga, Y.; Higashino, M.; Tanimura, S.; Takemura, M.; Tanaka, Y.; Laparoscopic, O.H. Laparoscopic Hemicolectomy in a Patient with Situs Inversus Totalis CASE REPORT. World J. Gastroenterol. 2007, 13, 5035–5037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaegashi, M.; Kimura, T.; Sakamoto, T.; Sato, T.; Kawasaki, Y.; Otsuka, K.; Wakabayashi, G. Laparoscopic Sigmoidectomy for a Patient With Situs Inversus Totalis: Effect of Changing Operator Position. Int. Surg. 2015, 100, 638–642. [Google Scholar] [CrossRef] [Green Version]
- Huh, J.W.; Kim, H.R.; Cho, S.H.; Kim, C.Y.; Kim, H.J.; Joo, J.K.; Kim, Y.J. Laparoscopic Total Mesorectal Excision in a Rectal Cancer Patient with Situs Inversus Totalis. J. Korean Med. Sci. 2010, 25, 790–793. [Google Scholar] [CrossRef] [Green Version]
- Gündeş, E.; Çetin, A.; Aday, U.; Çiyiltepe, H.; Bozdağ, E.; Senger, A.S.; Gülmez, S.; Değer, K.C.; Uzun, O.; Polat, E. Gastric Cancer with Situs Inversus Totalis: Does It Really Create Difficulties for Surgeons? Gastroenterol. Rev. 2018, 13, 47–51. [Google Scholar] [CrossRef]
- Catheline, J.M.; Rosales, C.; Cohen, R.; Bihan, H.; Luc Fournier, J.; Roussel, J.; Bénichou, J. Laparoscopic Sleeve Gastrectomy for a Super-Super-Obese Patient with Situs Inversus Totalis. Obes. Surg. 2006, 16, 1092–1095. [Google Scholar] [CrossRef]
- O’Connor, N.; Sugrue, M.; Melly, C.; McGeehan, G.; Bucholc, M.; Crawford, A.; O’Connor, P.; Abu-Zidan, F.; Wani, I.; Balogh, Z.J.; et al. It’s Time for a Minimum Synoptic Operation Template in Patients Undergoing Laparoscopic Cholecystectomy: A Systematic Review. World J. Emerg. Surg. 2022, 17, 15. [Google Scholar] [CrossRef]
- Griffiths, E.A.; Hodson, J.; Vohra, R.S.; Marriott, P.; Katbeh, T.; Zino, S.; Nassar, A.H.M. Utilisation of an Operative Difficulty Grading Scale for Laparoscopic Cholecystectomy. Surg. Endosc. 2019, 33, 110–121. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Sex | N | Mean | Minimum | Maximum |
|---|---|---|---|---|---|
| Age | F | 85 | 45.68 | 16 | 79 |
| M | 36 | 51.86 | 21 | 88 | |
| Total | 121 | 47.52 | 16 | 88 |
| Disease | N | Mean | Std. Dev. | |
|---|---|---|---|---|
| N/A | Duration (min) | 2 | 100.00 | 70.711 |
| (N = 2) | Postop Stay (days) | 2 | 4.50 | 3.536 |
| Morbidity | 0 | |||
| AC | Duration (min) | 16 | 67.06 | 23.510 |
| (N = 32) | Postop Stay (days) | 28 | 2.82 | 2.127 |
| Morbidity | 31 | |||
| CC | Duration (min) | 50 | 68.14 | 21.089 |
| (N = 73) | Postop Stay (days) | 63 | 1.52 | 0.981 |
| Morbidity | 73 | |||
| CHL | Duration (min) | 6 | 112.33 | 67.331 |
| (N = 9) | Postop Stay (days) | 8 | 2.88 | 2.475 |
| Morbidity | 9 | |||
| CHO | Duration (min) | 0 | ||
| (N = 1) | Postop Stay (days) | 1 | 2.00 | |
| Morbidity | 1 | |||
| AP | Duration (min) | 4 | 50.00 | 18.257 |
| (N = 4) | Postop Stay (days) | 3 | 2.00 | 1.732 |
| Morbidity | 4 | |||
| Variable | N | Min | Median | Max | Spearman’s r |
|---|---|---|---|---|---|
| Duration (min) | 78 | 30 | 68 | 240 | r = 0.032 p = 0.786 |
| PO Stay (days) | 105 | 1 | 1 | 11 |
| Operative Technique | Duration (min) | Morbidity | Postop Stay (Days) | ||
|---|---|---|---|---|---|
| Other Techniques | N = 6 | Valid | 4 | 6 | 6 |
| Missing | 2 | 0 | 0 | ||
| Median | 72.00 | 0.00 | 1.00 | ||
| Percentiles | 25 | 40.00 | 0.00 | 1.00 | |
| 50 | 72.00 | 0.00 | 1.00 | ||
| 75 | 74.75 | 0.00 | 3.50 | ||
| MirA | N = 94 | Valid | 60 | 93 | 82 |
| Missing | 34 | 1 | 12 | ||
| Median | 65.00 | 0.00 | 1.00 | ||
| Percentiles | 25 | 50.00 | 0.00 | 1.00 | |
| 50 | 65.00 | 0.00 | 1.00 | ||
| 75 | 80.00 | 0.00 | 3.00 | ||
| MirF | N = 12 | Valid | 7 | 10 | 8 |
| Missing | 5 | 2 | 4 | ||
| Median | 60.00 | 0.00 | 2.50 | ||
| Percentiles | 25 | 55.00 | 0.00 | 2.00 | |
| 50 | 60.00 | 0.00 | 2.50 | ||
| 75 | 88.00 | 0.00 | 4.50 | ||
| SP | N = 9 | Valid | 7 | 9 | 9 |
| Missing | 2 | 0 | 0 | ||
| Median | 75.00 | 0.00 | 2.00 | ||
| Percentiles | 25 | 54.00 | 0.00 | 1.00 | |
| 50 | 75.00 | 0.00 | 2.00 | ||
| 75 | 90.00 | 0.00 | 2.00 | ||
| Dominant Hand | Duration (Min) | Morbidity | Postop Stay (Days) | |||
|---|---|---|---|---|---|---|
| N/A (N = 18) | N | Valid | 6 | 18 | 15 | |
| Missing | 12 | 0 | 3 | |||
| Median | 67.50 | 0.00 | 2.00 | |||
| Percentiles | 25 | 45.00 | 0.00 | 1.00 | ||
| 50 | 67.50 | 0.00 | 2.00 | |||
| 75 | 127.50 | 0.00 | 3.00 | |||
| AMBI (N = 3) | N | Valid | 1 | 3 | 2 | |
| Missing | 2 | 0 | 1 | |||
| Median | 106.00 | 0.00 | 1.00 | |||
| Percentiles | 25 | 106.00 | 0.00 | 1.00 | ||
| 50 | 106.00 | 0.00 | 1.00 | |||
| 75 | 106.00 | 0.00 | 1.00 | |||
| L (N = 7) | N | Valid | 4 | 7 | 5 | |
| Missing | 3 | 0 | 2 | |||
| Median | 47.50 | 0.00 | 1.00 | |||
| Percentiles | 25 | 33.75 | 0.00 | 1.00 | ||
| 50 | 47.50 | 0.00 | 1.00 | |||
| 75 | 57.50 | 0.00 | 7.00 | |||
| R (N = 93) | N | Valid | 67 | 90 | 83 | |
| Missing | 26 | 3 | 10 | |||
| Median | 70.00 | 0.00 | 1.00 | |||
| Percentiles | 25 | 55.00 | 0.00 | 1.00 | ||
| 50 | 70.00 | 0.00 | 1.00 | |||
| 75 | 80.00 | 0.00 | 2.00 | |||
| Variable | 95% CI for ρ | p-Value | |
|---|---|---|---|
| Duration of surgery (min) | Disease | (−0.311, 0.136) | 0.068 |
| Preoperative imaging | (0.007, 0.430) | 0.038 | |
| Dominant Hand | (−0.000, 0.442) | 0.024 | |
| Operating Technique | (−0.190, 0.267) | 0.731 | |
| IOC | (−0.045, 0.394) | 0.114 | |
| Postop Stay (days) | Disease | (−0.525, −0.189) | 0.001 |
| Preoperative imaging | (−0.164, 0.219) | 0.771 | |
| Dominant Hand | (−0.268, 0.144) | 0.543 | |
| Operating Technique | (−0.175, 0.219) | 0.079 | |
| IOC | (−0.325, 0.061) | 0.174 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Enciu, O.; Toma, E.A.; Tulin, A.; Georgescu, D.E.; Miron, A. Look beyond the Mirror: Laparoscopic Cholecystectomy in Situs Inversus Totalis—A Systematic Review and Meta-Analysis (and Report of New Technique). Diagnostics 2022, 12, 1265. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051265
Enciu O, Toma EA, Tulin A, Georgescu DE, Miron A. Look beyond the Mirror: Laparoscopic Cholecystectomy in Situs Inversus Totalis—A Systematic Review and Meta-Analysis (and Report of New Technique). Diagnostics. 2022; 12(5):1265. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051265
Chicago/Turabian StyleEnciu, Octavian, Elena Adelina Toma, Adrian Tulin, Dragos Eugen Georgescu, and Adrian Miron. 2022. "Look beyond the Mirror: Laparoscopic Cholecystectomy in Situs Inversus Totalis—A Systematic Review and Meta-Analysis (and Report of New Technique)" Diagnostics 12, no. 5: 1265. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051265