
Utility of Next-Generation Sequencing in the Reconstruction of Clonal Architecture in a Patient with an EGFR Mutated Advanced Non-Small Cell Lung Cancer: A Case Report

 , and
, and
Abstract
:1. Introduction
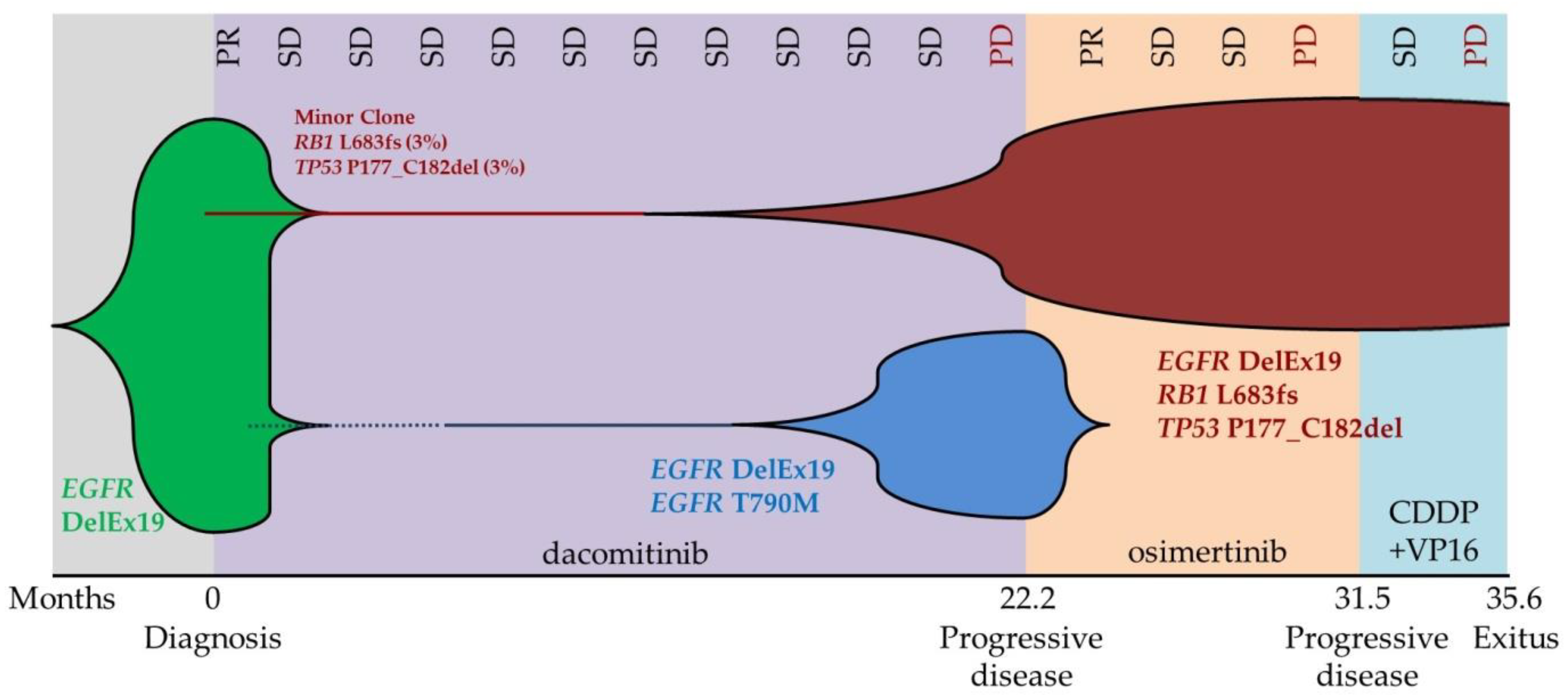
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Yang, C.Y.; Yang, J.C.H.; Yang, P.C. Precision Management of Advanced Non-Small Cell Lung Cancer. Annu. Rev. Med. 2020, 71, 117–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeda, M.; Nakagawa, K. First-and Second-Generation EGFR-TKIs Are All Replaced to Osimertinib in Chemo-Naive EGFR Mutation-Positive Non-Small Cell Lung Cancer? Int. J. Mol. Sci. 2019, 20, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marino, F.Z.; Bianco, R.; Accardo, M.; Ronchi, A.; Cozzolino, I.; Morgillo, F.; Rossi, G.; Franco, R. Molecular Heterogeneity in Lung Cancer: From Mechanisms of Origin to Clinical Implications. Int. J. Med. Sci. 2019, 16, 981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camidge, D.R.; Pao, W.; Sequist, L.V. Acquired Resistance to TKIs in Solid Tumours: Learning from Lung Cancer. Nat. Rev. Clin. Oncol. 2014, 11, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.L.; Ahn, M.J.; Garassino, M.C.; Kim, H.R.; Ramalingam, S.S.; Shepherd, F.A.; He, Y.; Akamatsu, H.; Theelen, W.S.M.E.; et al. Osimertinib or Platinum-Pemetrexed in EGFR T790M-Positive Lung Cancer. N. Engl. J. Med. 2017, 376, 629–640. [Google Scholar] [CrossRef] [Green Version]
- Schmid, S.; Li, J.J.N.; Leighl, N.B. Mechanisms of Osimertinib Resistance and Emerging Treatment Options. Lung Cancer 2020, 147, 123–129. [Google Scholar] [CrossRef]
- Mehlman, C.; Cadranel, J.; Rousseau-Bussac, G.; Lacave, R.; Pujals, A.; Girard, N.; Callens, C.; Gounant, V.; Théou-Anton, N.; Friard, S.; et al. Resistance Mechanisms to Osimertinib in EGFR-Mutated Advanced Non-Small-Cell Lung Cancer: A Multicentric Retrospective French Study. Lung Cancer 2019, 137, 149–156. [Google Scholar] [CrossRef]
- Leonetti, A.; Sharma, S.; Minari, R.; Perego, P.; Giovannetti, E.; Tiseo, M. Resistance Mechanisms to Osimertinib in EGFR-Mutated Non-Small Cell Lung Cancer. Br. J. Cancer 2019, 121, 725–737. [Google Scholar] [CrossRef]
- Jamal-Hanjani, M.; Wilson, G.A.; McGranahan, N.; Birkbak, N.J.; Watkins, T.B.K.; Veeriah, S.; Shafi, S.; Johnson, D.H.; Mitter, R.; Rosenthal, R.; et al. Tracking the Evolution of Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 376, 2109–2121. [Google Scholar] [CrossRef] [Green Version]
- Amirouchene-Angelozzi, N.; Swanton, C.; Bardelli, A. Tumor Evolution as a Therapeutic Target. Cancer Discov. 2017, 7, 805–817. [Google Scholar] [CrossRef] [Green Version]
- Merker, J.D.; Oxnard, G.R.; Compton, C.; Diehn, M.; Hurley, P.; Lazar, A.J.; Lindeman, N.; Lockwood, C.M.; Rai, A.J.; Schilsky, R.L.; et al. Circulating Tumor DNA Analysis in Patients with Cancer: American Society of Clinical Oncology and College of American Pathologists Joint Review. J. Clin. Oncol. 2018, 36, 1631–1641. [Google Scholar] [CrossRef] [PubMed]
- Saarenheimo, J.; Eigeliene, N.; Andersen, H.; Tiirola, M.; Jekunen, A. The Value of Liquid Biopsies for Guiding Therapy Decisions in Non-Small Cell Lung Cancer. Front. Oncol. 2019, 9, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of Circulating Tumor DNA in Early- and Late-Stage Human Malignancies. Sci. Transl. Med. 2014, 6, 224ra24. [Google Scholar] [CrossRef] [Green Version]
- Cecchini, M.J.; Yi, E.S. Liquid Biopsy Is a Valuable Tool in the Diagnosis and Management of Lung Cancer. J. Thorac. Dis. 2020, 12, 7048. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; Wilcox, W.R. Changing Paradigm of Cancer Therapy: Precision Medicine by next-Generation Sequencing. Cancer Biol. Med. 2016, 13, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Zhong, Y.; Xu, F.; Wu, J.; Schubert, J.; Li, M.M. Application of Next Generation Sequencing in Laboratory Medicine. Ann. Lab. Med. 2021, 41, 25–43. [Google Scholar] [CrossRef]
- Mosele, F.; Remon, J.; Mateo, J.; Westphalen, C.B.; Barlesi, F.; Lolkema, M.P.; Normanno, N.; Scarpa, A.; Robson, M.; Meric-Bernstam, F.; et al. Recommendations for the Use of Next-Generation Sequencing (NGS) for Patients with Metastatic Cancers: A Report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2020, 31, 1491–1505. [Google Scholar] [CrossRef]
- Papadopoulou, E.; Tsoulos, N.; Tsantikidi, K.; Metaxa-Mariatou, V.; Stamou, P.E.; Kladi-Skandali, A.; Kapeni, E.; Tsaousis, G.; Pentheroudakis, G.; Petrakis, D.; et al. Clinical Feasibility of NGS Liquid Biopsy Analysis in NSCLC Patients. PLoS ONE 2019, 14, e0226853. [Google Scholar] [CrossRef] [Green Version]
- George, J.; Lim, J.S.; Jang, S.J.; Cun, Y.; Ozretia, L.; Kong, G.; Leenders, F.; Lu, X.; Fernández-Cuesta, L.; Bosco, G.; et al. Comprehensive Genomic Profiles of Small Cell Lung Cancer. Nature 2015, 524, 47–53. [Google Scholar] [CrossRef]
- Vargas, A.J.; Harris, C.C. Biomarker Development in the Precision Medicine Era: Lung Cancer as a Case Study. Nat. Rev. Cancer 2016, 16, 525–537. [Google Scholar] [CrossRef]
- Tsimberidou, A.M.; Fountzilas, E.; Nikanjam, M.; Kurzrock, R. Review of Precision Cancer Medicine: Evolution of the Treatment Paradigm. Cancer Treat. Rev. 2020, 86, 102019. [Google Scholar] [CrossRef] [PubMed]
- Kohsaka, S.; Petronczki, M.; Solca, F.; Maemondo, M. Tumor Clonality and Resistance Mechanisms in EGFR Mutation-Positive Non-Small-Cell Lung Cancer: Implications for Therapeutic Sequencing. Future Oncol. 2019, 15, 637–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.K.; Lee, J.; Kim, S.; Kim, S.; Youk, J.; Park, S.; An, Y.; Keam, B.; Kim, D.W.; Heo, D.S.; et al. Clonal History and Genetic Predictors of Transformation into Small-Cell Carcinomas from Lung Adenocarcinomas. J. Clin. Oncol. 2017, 35, 3065–3074. [Google Scholar] [CrossRef] [PubMed]
- Offin, M.; Chan, J.M.; Tenet, M.; Rizvi, H.A.; Shen, R.; Riely, G.J.; Rekhtman, N.; Daneshbod, Y.; Quintanal-Villalonga, A.; Penson, A.; et al. Concurrent RB1 and TP53 Alterations Define a Subset of EGFR-Mutant Lung Cancers at Risk for Histologic Transformation and Inferior Clinical Outcomes. J. Thorac. Oncol. 2019, 14, 1784–1793. [Google Scholar] [CrossRef]
- Nguyen, K.S.H.; Kobayashi, S.; Costa, D.B. Acquired Resistance to Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors in Non-Small-Cell Lung Cancers Dependent on the Epidermal Growth Factor Receptor Pathway. Clin. Lung Cancer 2009, 10, 281–289. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Yu, J.; Zhang, H.; Liu, J. TP53 Co-Mutations in Advanced EGFR-Mutated Non-Small Cell Lung Cancer: Prognosis and Therapeutic Strategy for Cancer Therapy. Front. Oncol. 2022, 12, 860563. [Google Scholar] [CrossRef]
- Nakagawa, K.; Nadal, E.; Garon, E.B.; Nishio, M.; Seto, T.; Yamamoto, N.; Park, K.; Shih, J.Y.; Paz-Ares, L.; Frimodt-Moller, B.; et al. RELAY Subgroup Analyses by EGFR Ex19del and Ex21L858R Mutations for Ramucirumab Plus Erlotinib in Metastatic Non-Small Cell Lung Cancer. Clin. Cancer Res. 2021, 27, 5258–5271. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, Z.; Chen, R.; Fang, C.; Zhang, C.; Ji, M.; Yang, X. Immunotherapy-Based Combination Strategies for Treatment of EGFR-TKI-Resistant Non-Small-Cell Lung Cancer. Future Oncol. 2022, 18, 1757–1775. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Moment | EGFR Exon 19 | EGFR p.(Thr790) | TP53 Exon 5 | RB1 p.(Leu683) |
|---|---|---|---|---|
| NSCLC FFPE sample | p.(Glu746_Ala750del) 20% | NMD | p.(Pro177_Cys182del) 2.5% | p.(Leu683Phefs*13) 3% |
| Disease progression on dacomitinib (LB) | p.(Glu746_Ala750del) 7.9% | p.(Thr790Met) 3% | p.(Pro177_Cys182del) 2.5% | NI |
| Disease progression on osimertinib (LB) | p.(Glu746_Ala750del) 58% | NMD | p.(Pro177_Cys182del) 68% | NI |
| SCLC FFPE sample | p.(Glu746_Ala750del) 73% | NMD | p.(Pro177_Cys182del) 90% | p.(Leu683Phefs*13) 96% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simarro, J.; Pérez-Simó, G.; Mancheño, N.; Muñoz-Núñez, C.F.; Cases, E.; Juan, Ó.; Palanca, S. Utility of Next-Generation Sequencing in the Reconstruction of Clonal Architecture in a Patient with an EGFR Mutated Advanced Non-Small Cell Lung Cancer: A Case Report. Diagnostics 2022, 12, 1266. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051266
Simarro J, Pérez-Simó G, Mancheño N, Muñoz-Núñez CF, Cases E, Juan Ó, Palanca S. Utility of Next-Generation Sequencing in the Reconstruction of Clonal Architecture in a Patient with an EGFR Mutated Advanced Non-Small Cell Lung Cancer: A Case Report. Diagnostics. 2022; 12(5):1266. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051266
Chicago/Turabian StyleSimarro, Javier, Gema Pérez-Simó, Nuria Mancheño, Carlos Francisco Muñoz-Núñez, Enrique Cases, Óscar Juan, and Sarai Palanca. 2022. "Utility of Next-Generation Sequencing in the Reconstruction of Clonal Architecture in a Patient with an EGFR Mutated Advanced Non-Small Cell Lung Cancer: A Case Report" Diagnostics 12, no. 5: 1266. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051266