
General Roadmap and Core Steps for the Development of AI Tools in Digital Pathology

 ,
,  , and
, and 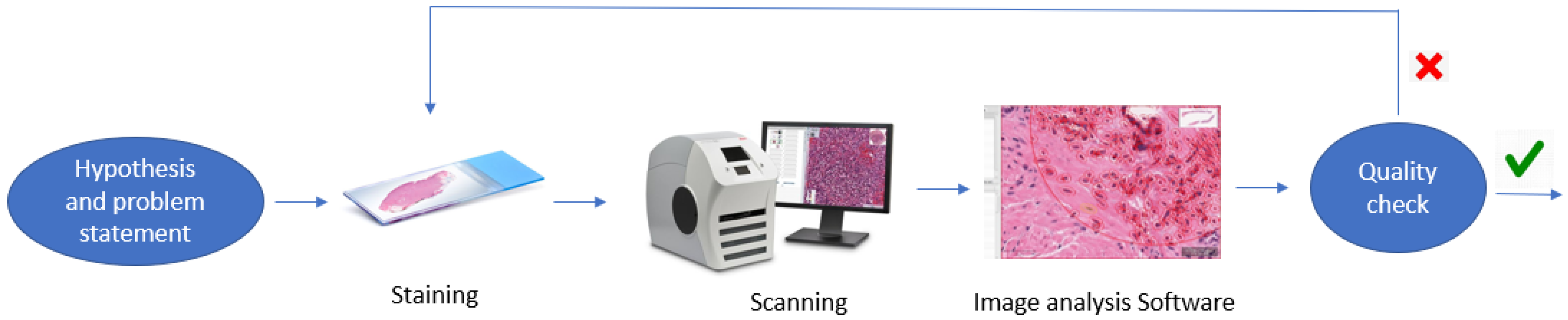{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- Hypothesis formulation.
- Data preparation in the wet-lab and digital annotations and pre-processing.
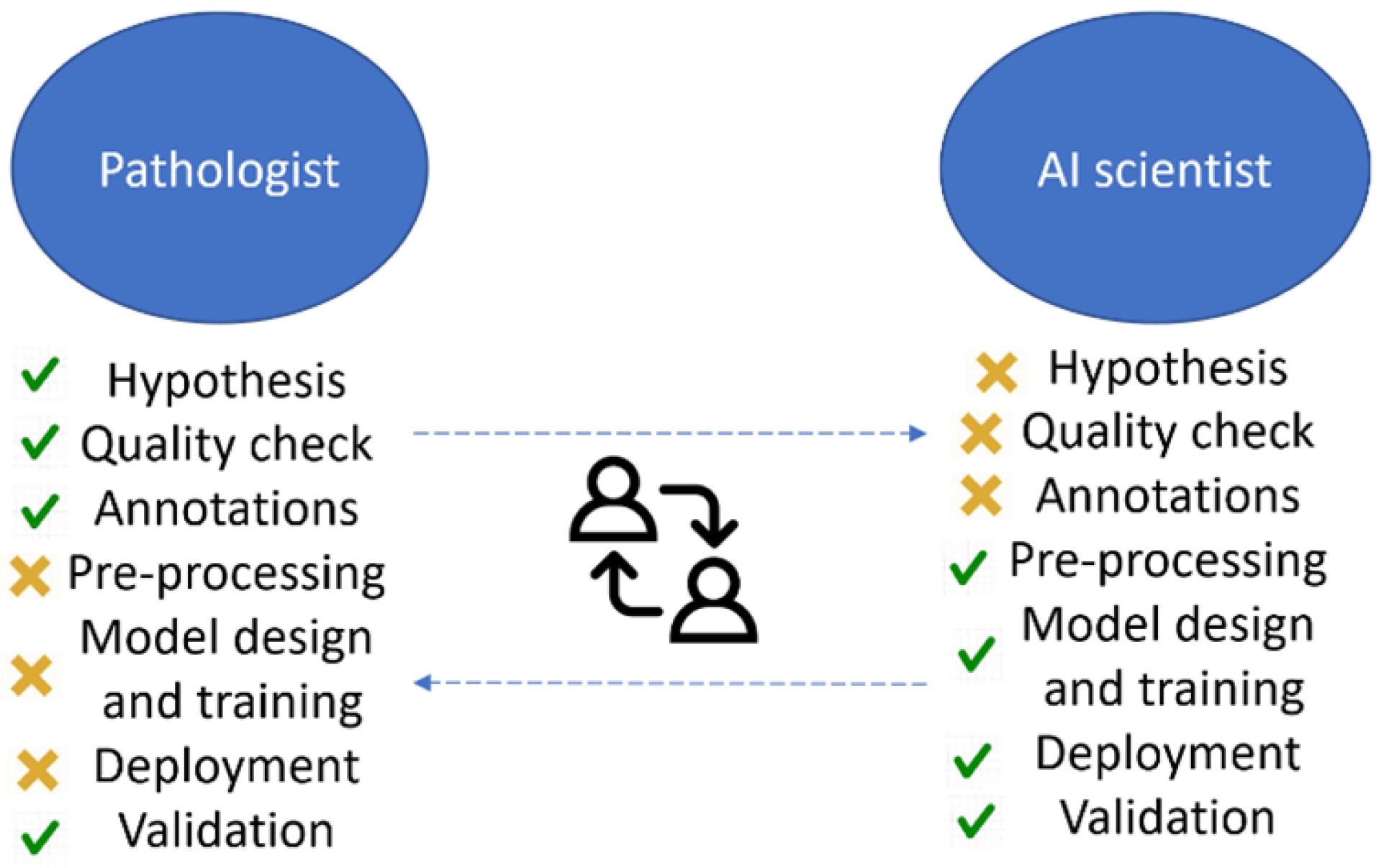
- AI models design, training, and clinical validation.
- Deployment.
2. Workflow and Methods
2.1. Hypothesis Formulation
2.2. Wet-Lab Work
2.3. Data Preparation
2.3.1. Quality Check
2.3.2. Descriptive Region
2.3.3. Annotations
2.3.4. Preprocessing
2.3.5. Data Augmentation
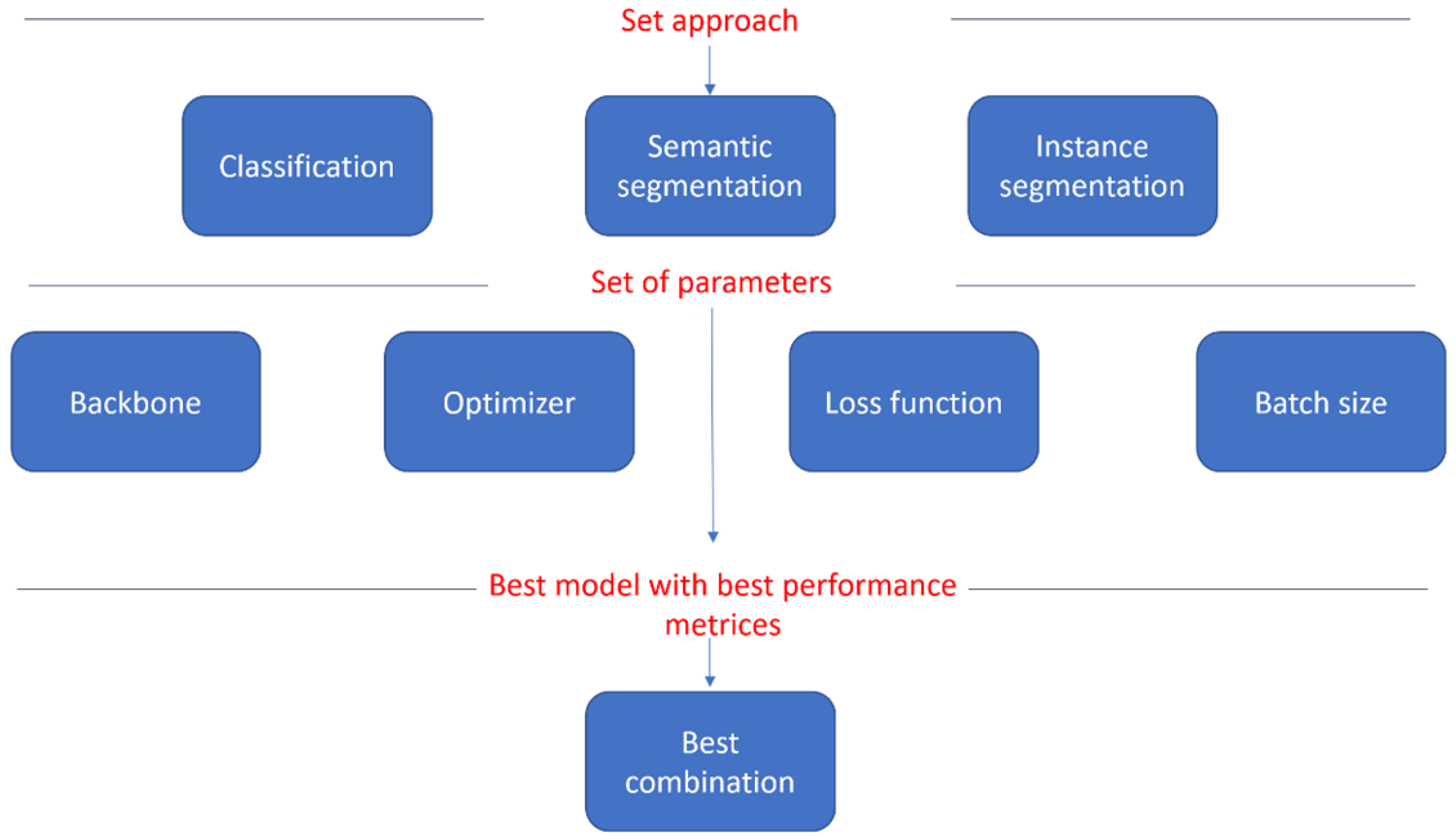
2.4. Model Design and Training
2.5. Clinical Utility and Hypothesis Validation
3. Deployment
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koteluk, O.; Wartecki, A.; Mazurek, S.; Kołodziejczak, I.; Mackiewicz, A. How do machines learn? Artificial intelligence as a new era in medicine. J. Pers. Med. 2021, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Salto-Tellez, M.; Maxwell, P.; Hamilton, P. Artificial intelligence-the third revolution in pathology. Histopathology 2019, 74, 372–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, R.; Bajgiran, A.M.; Mirak, S.A.; Shakeri, S.; Zhong, X.; Enzmann, D.; Raman, S.; Sung, K. Joint prostate cancer detection and gleason score prediction in mp-MRI via FocalNet. IEEE Trans. Med. Imaging 2019, 38, 2496–2506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irvin, J.; Rajpurkar, P.; Ko, M.; Yu, Y.; Ciurea-Ilcus, S.; Chute, C.; Marklund, H.; Haghgoo, B.; Ball, R.; Shpanskaya, K.; et al. Chexpert: A large chest radiograph dataset with uncertainty labels and expert comparison. Proc. AAAI Conf. Artif. Intell. 2019, 33, 590–597. [Google Scholar] [CrossRef]
- Campanella, G.; Hanna, M.G.; Geneslaw, L.; Miraflor, A.; Silva, V.W.K.; Busam, K.J.; Brogi, E.; Reuter, V.E.; Klimstra, D.S.; Fuchs, T.J. Clinical-grade computational pathology using weakly supervised deep learning on whole slide images. Nat. Med. 2019, 25, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Nalisnik, M.; Amgad, M.; Lee, S.; Halani, S.H.; Vega, J.E.V.; Brat, D.J.; Gutman, D.A.; Cooper, L.A. Interactive phenotyping of large-scale histology imaging data with HistomicsML. Sci. Rep. 2017, 7, 14588. [Google Scholar] [CrossRef] [Green Version]
- Bejnordi, B.E.; Veta, M.; Van Diest, P.J.; Van Ginneken, B.; Karssemeijer, N.; Litjens, G.; Van Der Laak, J.A.; Hermsen, M.; Manson, Q.F.; Balkenhol, M.; et al. Diagnostic assessment of deep learning algorithms for detection of lymph node metastases in women with breast cancer. JAMA 2017, 318, 2199–2210. [Google Scholar] [CrossRef]
- Holzinger, A.; Malle, B.; Kieseberg, P.; Roth, P.M.; Müller, H.; Reihs, R.; Zatloukal, K. Towards the augmented pathologist: Challenges of explainable-ai in digital pathology. arXiv 2017, arXiv:1712.06657. [Google Scholar]
- Carpenter, A.E.; Jones, T.R.; Lamprecht, M.R.; Clarke, C.; Kang, I.H.; Friman, O.; Guertin, D.A.; Chang, J.H.; Lindquist, R.A.; Moffat, J.; et al. CellProfiler: Image analysis software for identifying and quantifying cell phenotypes. Genome Biol. 2006, 7, R100. [Google Scholar] [CrossRef] [Green Version]
- Saltz, J.; Sharma, A.; Iyer, G.; Bremer, E.; Wang, F.; Jasniewski, A.; DiPrima, T.; Almeida, J.S.; Gao, Y.; Zhao, T.; et al. A containerized software system for generation, management, and exploration of features from whole slide tissue images. Cancer Res. 2017, 77, e79–e82. [Google Scholar] [CrossRef] [Green Version]
- Martel, A.L.; Hosseinzadeh, D.; Senaras, C.; Zhou, Y.; Yazdanpanah, A.; Shojaii, R.; Patterson, E.S.; Madabhushi, A.; Gurcan, M.N. An image analysis resource for cancer research: PIIP—Pathology image informatics platform for visualization, analysis, and management. Cancer Res. 2017, 77, e83–e86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, Y.; Chen, M.; Kao, D.; Gao, G.; Chen, X. CheXplain: Enabling Physicians to Explore and Understand Data-Driven, AI-Enabled Medical Imaging Analysis. In Proceedings of the 2020 CHI Conference on Human Factors in Computing Systems, Honolulu, HI, USA, 25–30 April 2020; pp. 1–13. [Google Scholar]
- Xie, Y.; Gao, G.; Chen, X. Outlining the design space of explainable intelligent systems for medical diagnosis. arXiv 2019, arXiv:1902.06019. [Google Scholar]
- Yang, Q.; Steinfeld, A.; Zimmerman, J. Unremarkable ai: Fitting intelligent decision support into critical, clinical decision-making processes. In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems, Glasgow, UK, 4–9 May 2019; pp. 1–11. [Google Scholar]
- Yang, Q.; Zimmerman, J.; Steinfeld, A.; Carey, L.; Antaki, J.F. Investigating the heart pump implant decision process: Opportunities for decision support tools to help. In Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems, San Jose, CA, USA, 7–12 May 2016; pp. 4477–4488. [Google Scholar]
- Brezočnik, L.; Fister, I.; Podgorelec, V. Swarm Intelligence Algorithms for Feature Selection: A Review. Appl. Sci. 2018, 8, 1521. [Google Scholar] [CrossRef] [Green Version]
- Diaz-Garelli, J.F.; Wells, B.J.; Yelton, C.; Strowd, R.; Topaloglu, U. Biopsy records do not reduce diagnosis variability in cancer patient EHRs: Are we more uncertain after knowing? AMIA Summits Transl. Sci. Proc. 2018, 2018, 72–80. [Google Scholar]
- Allison, K.H.; Reisch, L.M.; Carney, P.A.; Weaver, D.L.; Schnitt, S.J.; O’Malley, F.P.; Geller, B.M.; Elmore, J.G. Understanding diagnostic variability in breast pathology: Lessons learned from an expert consensus review panel. Histopathology 2014, 65, 240–251. [Google Scholar] [CrossRef] [Green Version]
- Caron, M.; Misra, I.; Mairal, J.; Goyal, P.; Bojanowski, P.; Joulin, A. Unsupervised Learning of Visual Features by Contrasting Cluster Assignments. In Advances in Neural Information Processing Systems; Larochelle, H., Ranzato, M., Hadsell, R., Balcan, M.F., Lin, H., Eds.; Curran Associates, Inc.: Red Hook, NY, USA, 2020; Volume 33, pp. 9912–9924. [Google Scholar]
- Steiner, D.F.; Chen, P.H.C.; Mermel, C.H. Closing the translation gap: AI applications in digital pathology. Biochim. Biophys. Acta (BBA)-Rev. Cancer 2021, 1875, 188452. [Google Scholar] [CrossRef]
- Cruz Rivera, S.; Liu, X.; Chan, A.; Denniston, A.; Calvert, M.; SPIRIT-AI and CONSORT-AI Working Group; SPIRIT-AI and CONSORT-AI Steering Group; SPIRIT-AI and CONSORT-AI Consensus Group. Guidelines for clinical trial protocols for interventions involving artificial intelligence: The SPIRIT-AI extension. Nat. Med. 2020, 26, 1351–1363. [Google Scholar] [CrossRef]
- Lara, H.; Li, Z.; Abels, E.; Aeffner, F.; Bui, M.M.; ElGabry, E.A.; Kozlowski, C.; Montalto, M.C.; Parwani, A.V.; Zarella, M.D.; et al. Quantitative image analysis for tissue biomarker use: A white paper from the digital pathology association. Appl. Immunohistochem. Mol. Morphol. 2021, 29, 479–493. [Google Scholar] [CrossRef]
- Sarker, M.M.K.; Makhlouf, Y.; Craig, S.G.; Humphries, M.P.; Loughrey, M.; James, J.A.; Salto-Tellez, M.; O’Reilly, P.; Maxwell, P. A Means of Assessing Deep Learning-Based Detection of ICOS Protein Expression in Colon Cancer. Cancers 2021, 13, 3825. [Google Scholar] [CrossRef]
- Wahab, N.; Miligy, I.M.; Dodd, K.; Sahota, H.; Toss, M.; Lu, W.; Jahanifar, M.; Bilal, M.; Graham, S.; Park, Y.; et al. Semantic annotation for computational pathology: Multidisciplinary experience and best practice recommendations. arXiv 2021, arXiv:2106.13689. [Google Scholar] [CrossRef]
- Pei, S.C.; Lin, C.N. Image normalization for pattern recognition. Image Vis. Comput. 1995, 13, 711–723. [Google Scholar] [CrossRef]
- Isaksson, L.J.; Raimondi, S.; Botta, F.; Pepa, M.; Gugliandolo, S.G.; De Angelis, S.P.; Marvaso, G.; Petralia, G.; De Cobelli, O.; Gandini, S.; et al. Effects of MRI image normalization techniques in prostate cancer radiomics. Phys. Medica 2020, 71, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Janowczyk, A.; Zuo, R.; Gilmore, H.; Feldman, M.; Madabhushi, A. HistoQC: An open-source quality control tool for digital pathology slides. JCO Clin. Cancer Inform. 2019, 3, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tellez, D.; Litjens, G.; Bándi, P.; Bulten, W.; Bokhorst, J.M.; Ciompi, F.; Van Der Laak, J. Quantifying the effects of data augmentation and stain color normalization in convolutional neural networks for computational pathology. Med. Image Anal. 2019, 58, 101544. [Google Scholar] [CrossRef] [Green Version]
- Hynes, S.O.; Pang, B.; James, J.A.; Maxwell, P.; Salto-Tellez, M. Tissue-based next generation sequencing: Application in a universal healthcare system. Br. J. Cancer 2017, 116, 553–560. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makhlouf, Y.; Salto-Tellez, M.; James, J.; O’Reilly, P.; Maxwell, P. General Roadmap and Core Steps for the Development of AI Tools in Digital Pathology. Diagnostics 2022, 12, 1272. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051272
Makhlouf Y, Salto-Tellez M, James J, O’Reilly P, Maxwell P. General Roadmap and Core Steps for the Development of AI Tools in Digital Pathology. Diagnostics. 2022; 12(5):1272. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051272
Chicago/Turabian StyleMakhlouf, Yasmine, Manuel Salto-Tellez, Jacqueline James, Paul O’Reilly, and Perry Maxwell. 2022. "General Roadmap and Core Steps for the Development of AI Tools in Digital Pathology" Diagnostics 12, no. 5: 1272. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051272