
A Case of Multinucleate Cell Angiohistiocytoma with New Reflectance Confocal Microscopy Findings



Abstract
:1. Introduction
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smith, N.P.; Jones, E.W. Multinucleate cell angiohistiocytoma—A new entity. Br. J. Dermatol. 1985, 113, 15. [Google Scholar] [CrossRef]
- Jones, E.W.; Cerio, R.; Smith, N.P. Multinucleate cell angiohistiocytoma: An acquired vascular anomaly to be distinguished from Kaposi’s sarcoma. Br. J. Dermatol. 1990, 122, 651–663. [Google Scholar] [CrossRef] [PubMed]
- Rawal, Y.B.; Anderson, K.M.; Rawal, S.Y. Multinucleate cell angiohistiocytoma: An uncommon mucosal tumour. Clin. Exp. Dermatol. 2009, 34, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Calderaro, J.; Rethers, L.; Ortonne, N. Multinucleated Cells Angiohistiocytoma: A Reactive Lesion? Am. J. Dermatopathol. 2010, 32, 415–417. [Google Scholar] [CrossRef] [PubMed]
- Valerón-Almazán, P.; Dehesa, L.; Santana, N.; Vilar, J.; Carretero, G. Hallazgos dermatoscópicos del angiohistiocitoma de células multinucleadas: ¿una variante de dermatofibroma? Actas Dermosifiliogr. 2011, 102, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.F.; Dong, D.; Myung, P.; McNiff, J.M. Multinucleate cell angiohistiocytoma: A clinicopathologic study of 62 cases and proposed diagnostic criteria. J. Cutan. Pathol. 2019, 46, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Pogorzelska-Antkowiak, A.; Wcisło-Dziadecka, D.; Brzezińska-Wcisło, L.; Pawlicki, K.; Antkowiak, R.; Corneli, P. Features of dermatofibroma in reflectance confocal microscopy. Int. J. Dermatol. 2020, 59, 951–954. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.M.; Singh, R.; Udager, A.M.; Billings, S.D. Benign Fibrous, Fibrohistiocytic, and Myofibroblastic Lesions. In Soft Tissue Tumors of the Skin; Springer: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Millán-Cayetano, J.-F.; Yelamos, O.; Rossi, A.M.; Marchetti, M.A.; Jain, M. Reflectance confocal microscopy features of facial angiofibromas. Derm. Pract. Concept 2017, 7, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Frew, J.W. Multinucleate Cell Angiohistiocytoma. Am. J. Dermatopathol. 2015, 37, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Zaballos, P.; Puig, S.; Llambrich, A.; Malvehy, J. Dermoscopy of dermatofibromas: A prospective morphological study of 412 cases. Arch. Dermatol. 2008, 144, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Draghici, C.; Vajaitu, C.; Solomon, I.; Voiculescu, V.M.; Popa, I.M.; Lupu, M. The dermoscopic rainbow pattern-a review of the literature. Acta Derm. Croat 2019, 27, 111. [Google Scholar]
- Vázquez-López, F.; Alvarez-Cuesta, C.; Hidalgo-García, Y.; Pérez-Oliva, N. The handheld dermatoscope improves the recognition of Wickham striae and capillaries in Lichen planus lesions. Arch. Dermatol. 2001, 137, 1376. [Google Scholar]
- Kopera, D.; Smolle, J.; Kerl, H. Multinucleate cell angiohistiocytoma: Treatment with argon laser. Br. J. Dermatol. 1995, 133, 308–310. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Jorge, B.; del Pozo, J.; García-Silva, J.; Barja, J.M.; Yebra-Pimentel, M.T.; Fonseca, E. Multinucleate cell angiohistiocytoma: Treatment using intense pulsed light. Dermatol. Surg. 2009, 35, 1141–1143. [Google Scholar] [CrossRef]
- Richer, V.; Lui, H. Facial multinucleate cell angiohistiocytoma: Long-term remission with 585 nm pulsed dye laser. Clin. Exp. Dermatol. 2015, 41, 312–313. [Google Scholar] [CrossRef] [PubMed]
- Scope, A.; Ardigo, M.; Marghoob, A.A. Correlation of Dermoscopic Globule-Like Structures of Dermatofibroma Using Reflectance Confocal Microscopy. Dermatology 2007, 216, 81–82. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Lesion Type | RCM | Histopathology |
|---|---|---|
| Dermatofibroma | Typical honeycomb pattern, with occasional epidermal streaming. Numerous dilated hypo-reflective spaces (vessels) at the dermal–epidermal junction. Hyper-reflective “rings” composed of monomorphic cells surrounding dark dermal papillae [7]. | Circumscribed but unencapsulated tumor predominantly dermal-based. Variable amounts of epidermal hyperplasia, basal layer hyperpigmentation, and follicular induction. Lightly eosinophilic spindle cells present in a focally storiform growth pattern. Secondary elements including Touton-type giant cells, hemosiderin and foam-laden cells, and a lymphohistiocytic inflammatory infiltrate. Collagen trapping at the periphery [8]. |
| Fibrous papule (angiofibroma) | Regular honeycomb pattern. Nodules with increased cellular density and occasional clefting (BCC-like features). Small, round to linear and canalicular hypo-reflective dark spaces. Hyper-reflective, thickened collagen bundles surrounding hair follicles and BCC-like structures. Small bright round cells [9]. | Normal epidermis with epidermal invagination in the papillary dermis or superficial portion of external sheath of the hair follicle. Increased vascularization with variably sized, ectatic blood vessels. Thickened collagen bundles arranged around hair follicles. Occasionally multinucleated cells. Lymphocytes [9]. |
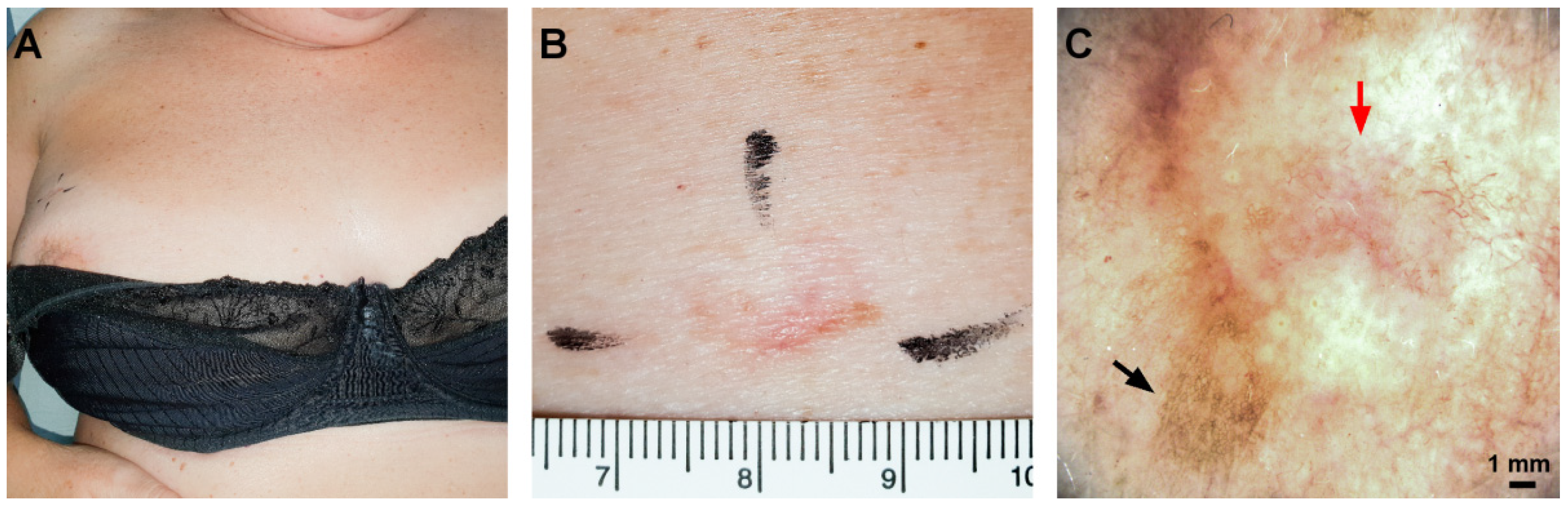
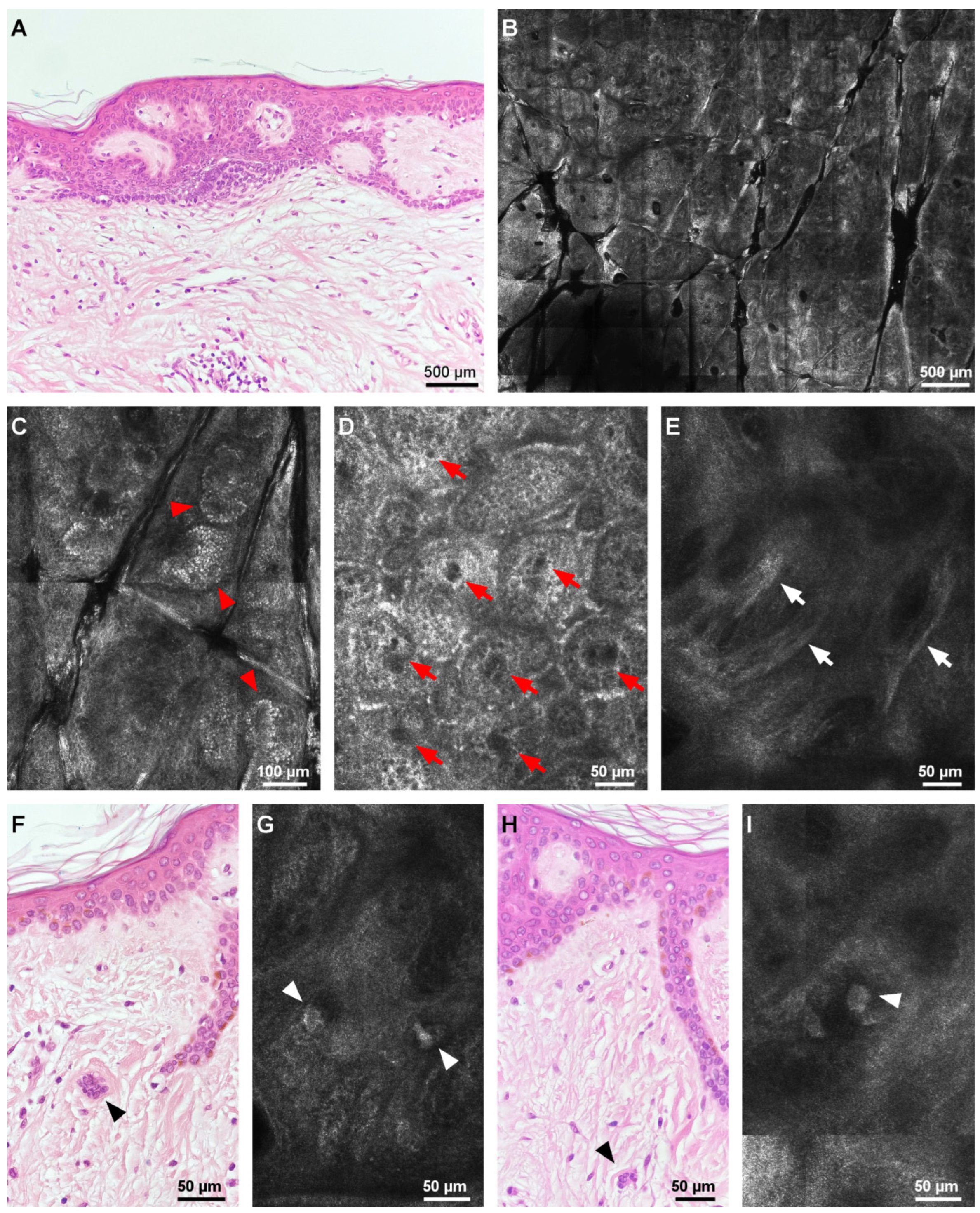
| Multinucleate cell angiohistiocytoma | Epidermis with a regular honeycomb pattern and clusters of hyper-reflective cells at the periphery. Numerous round, hypo-reflective spaces (vessels) at the dermal–epidermal junction. Hyper-reflective, dense strand-like structures. Isolated, large, mildly reflective, bizarre structures with angulated edges at the level of the superficial dermis. | Varying epidermal hyperplasia. Proliferation of dilated capillary dermal vessels. Thickened, dense collagen fibers in the upper dermis. Bizarre multinucleated cells with scalloped, angulated cytoplasm. Scattered lymphohistiocytic infiltrate [8]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lupu, M.; Tebeica, T.; Malciu, A.M.; Voiculescu, V.M. A Case of Multinucleate Cell Angiohistiocytoma with New Reflectance Confocal Microscopy Findings. Diagnostics 2022, 12, 1276. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051276
Lupu M, Tebeica T, Malciu AM, Voiculescu VM. A Case of Multinucleate Cell Angiohistiocytoma with New Reflectance Confocal Microscopy Findings. Diagnostics. 2022; 12(5):1276. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051276
Chicago/Turabian StyleLupu, Mihai, Tiberiu Tebeica, Ana Maria Malciu, and Vlad Mihai Voiculescu. 2022. "A Case of Multinucleate Cell Angiohistiocytoma with New Reflectance Confocal Microscopy Findings" Diagnostics 12, no. 5: 1276. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051276