
Image-Guided Percutaneous Ablation for Primary and Metastatic Tumors

 , ,
, ,
Abstract
:1. Introduction
2. Imaging Modalities for Guiding Percutaneous Ablation Devices
2.1. Ultrasound
2.2. Fluoroscopy
2.3. Computed Tomography, Cone-Beam CT, and CT Fluoroscopy
2.4. MRI
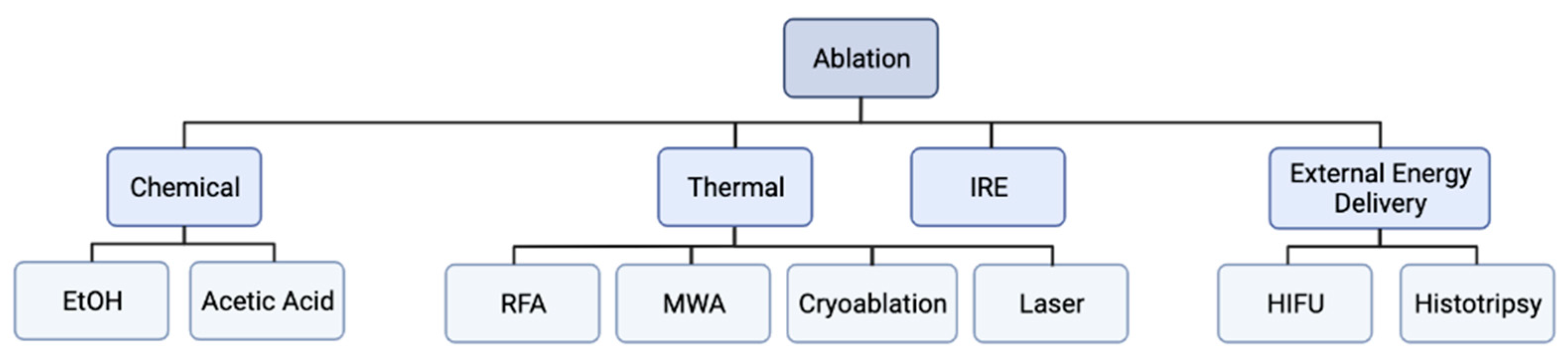
3. Physics and Mechanism of Action of Percutaneous Ablation Devices
3.1. Radiofrequeny Ablation
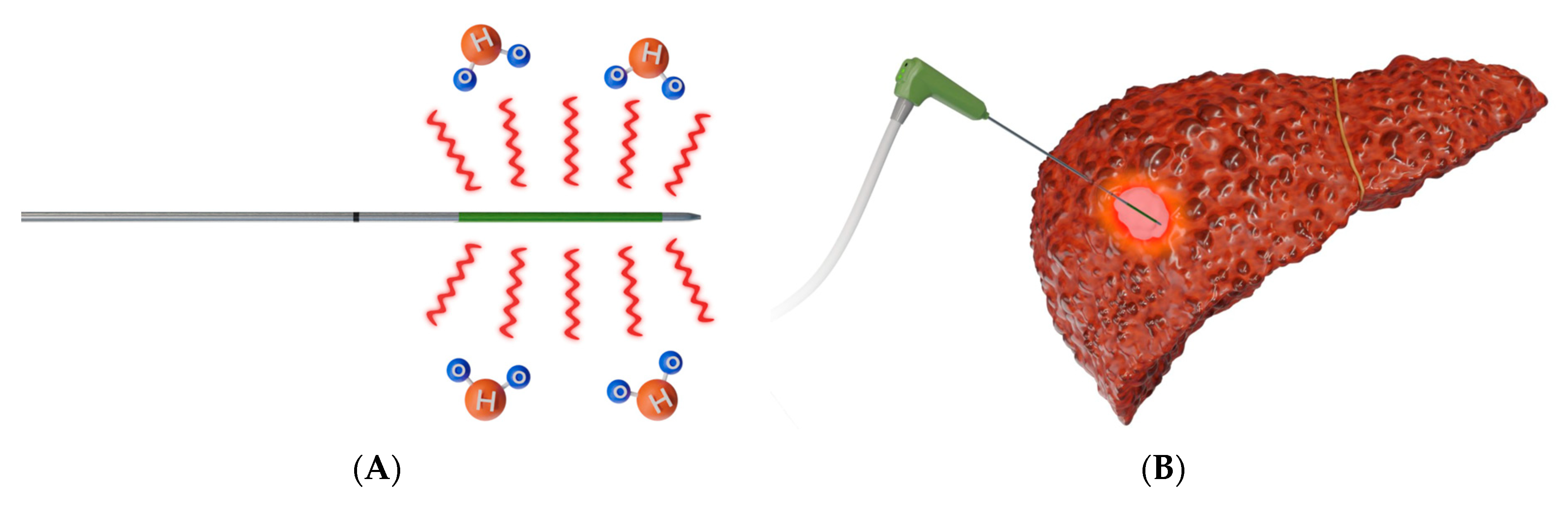
3.2. Microwave Ablation
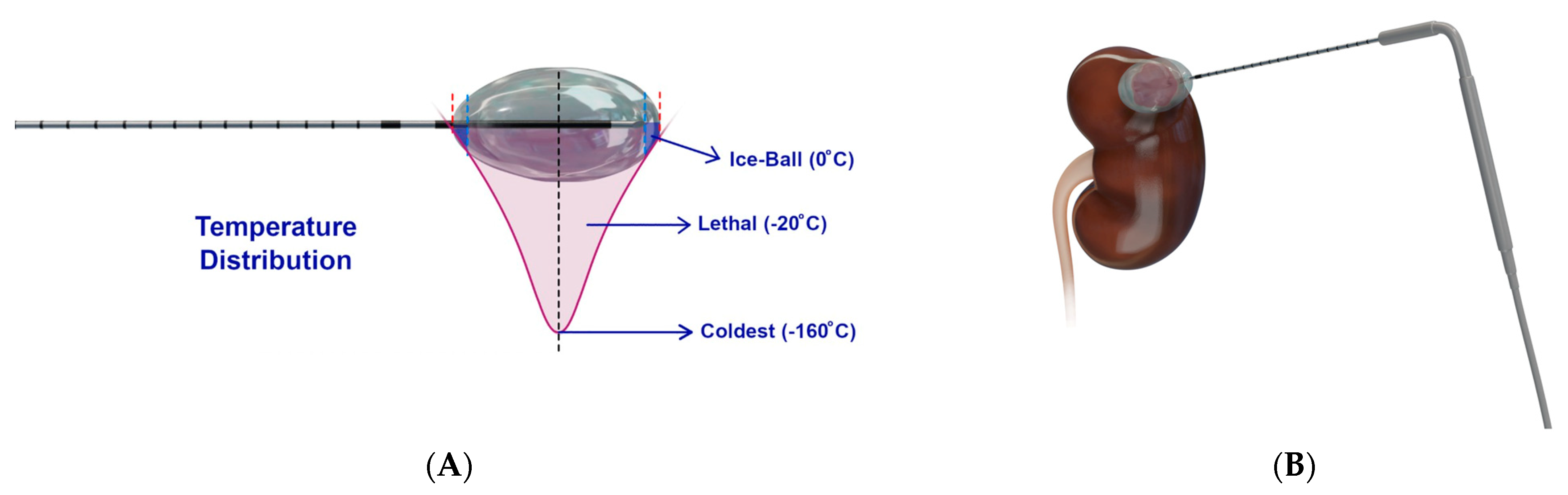
3.3. Cryoablation
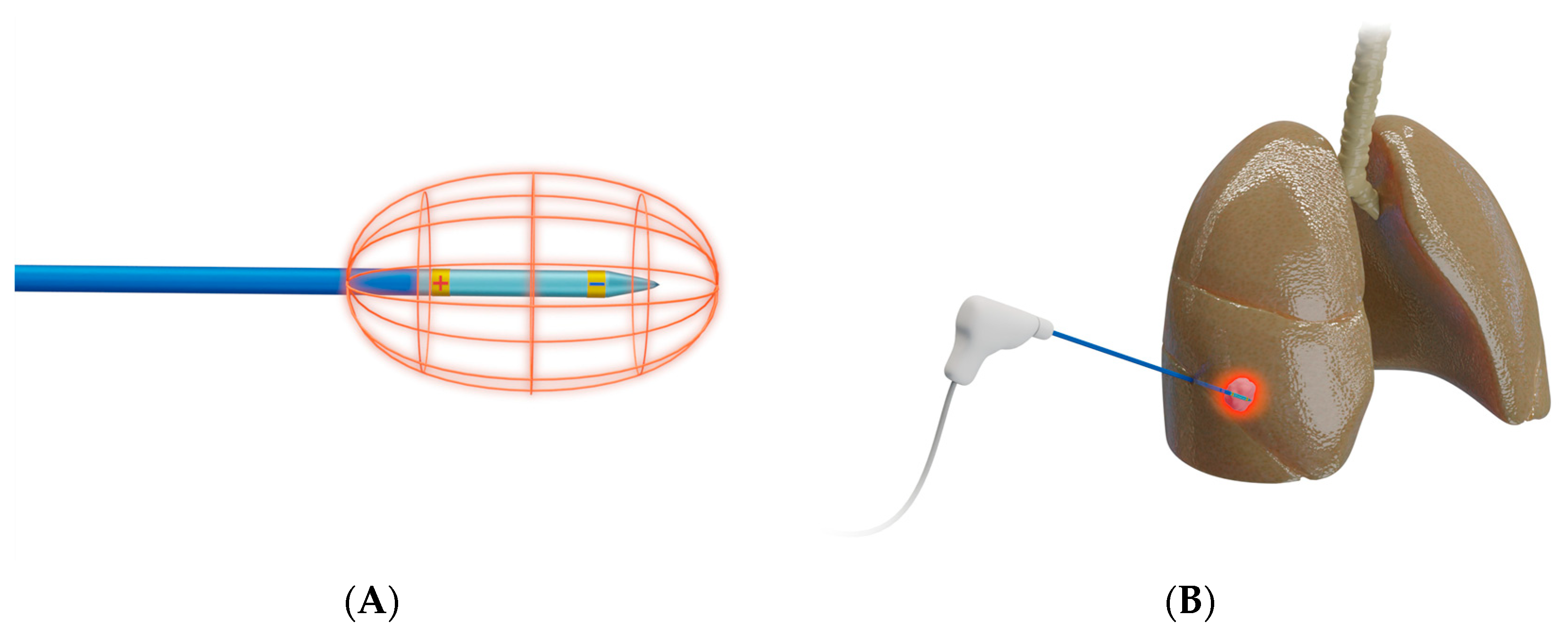
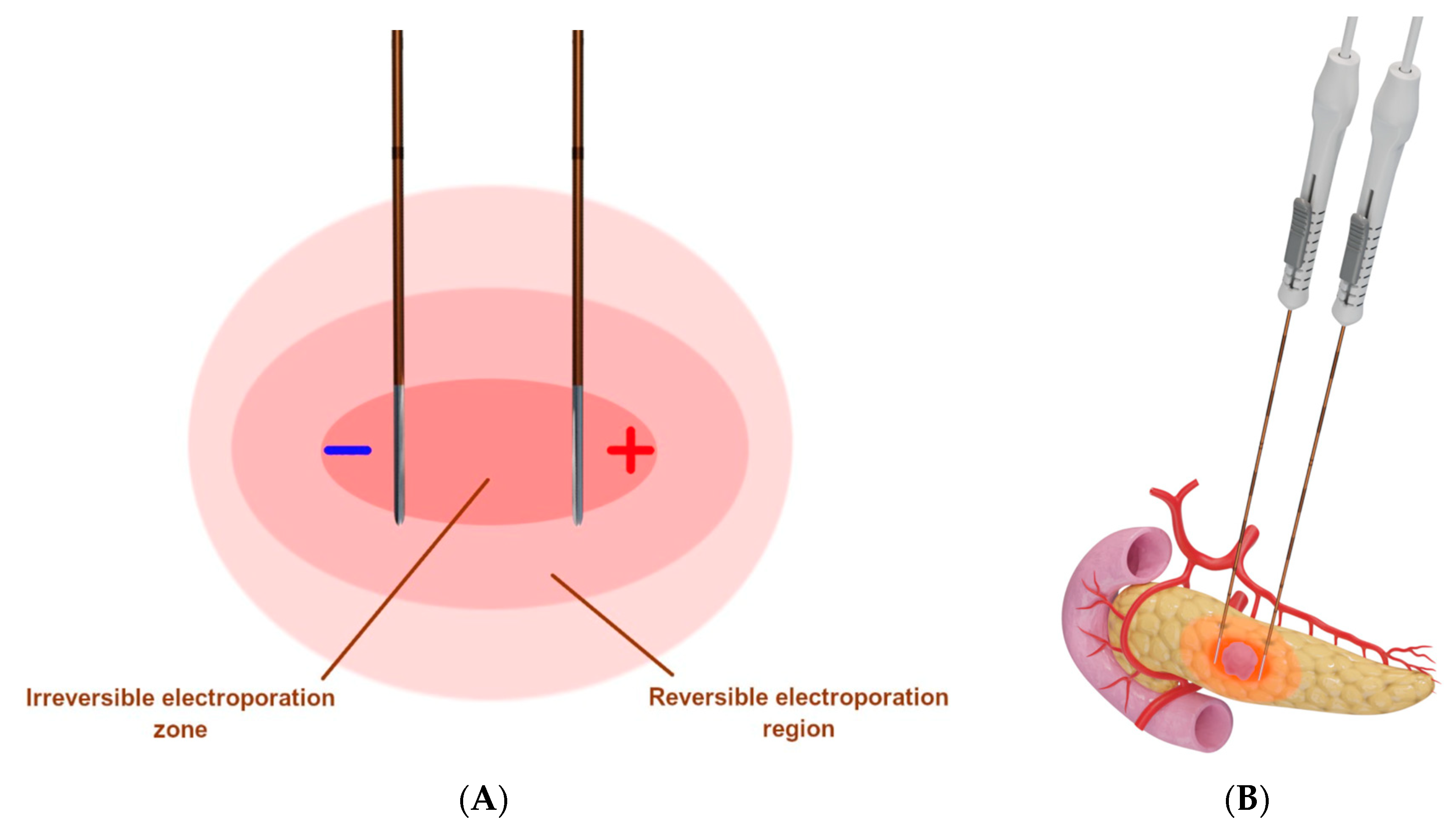
3.4. Irreversible Electroporation
3.5. Laser Ablation
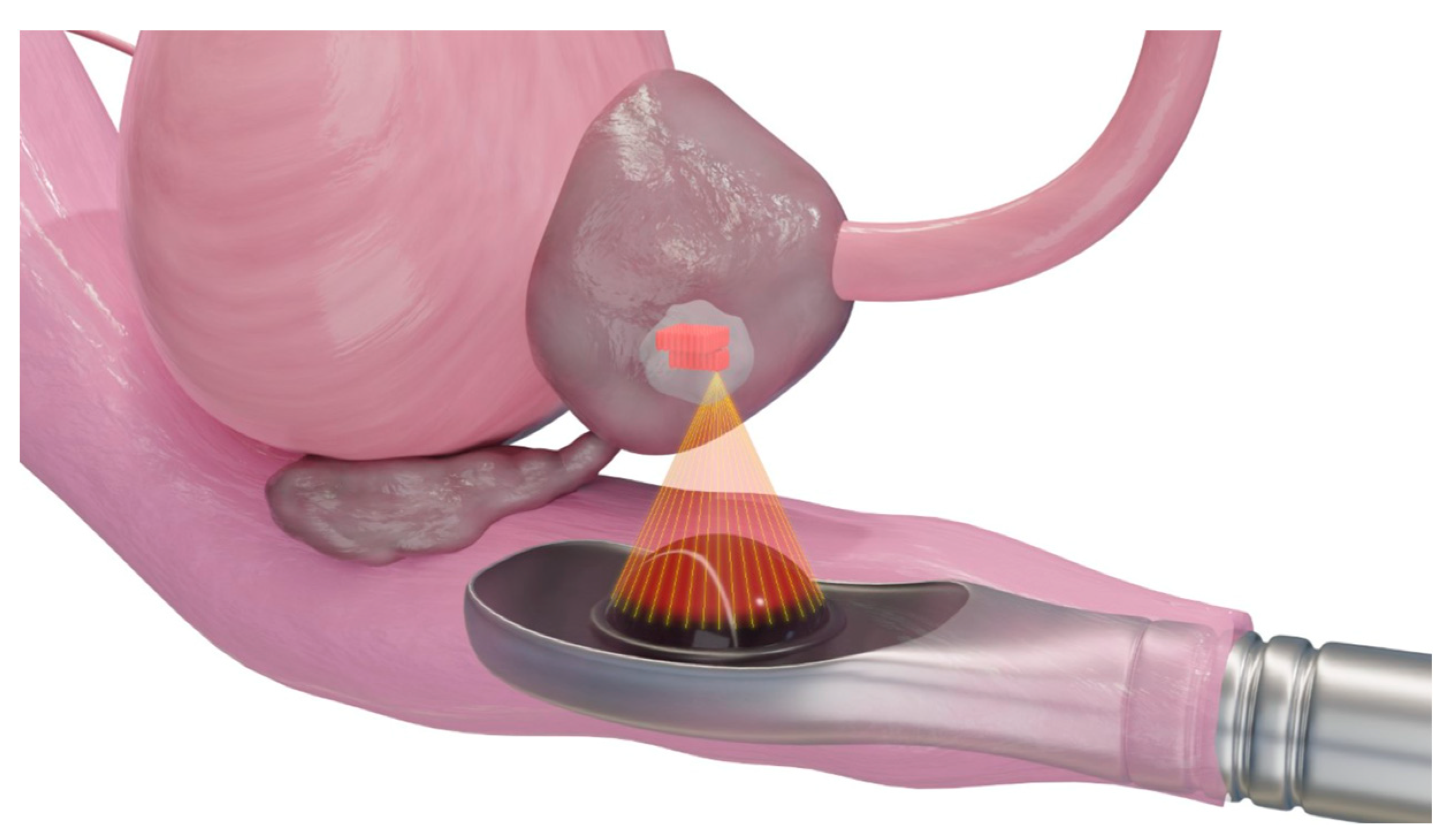
3.6. High-Intensity Frequency Ultrasound
3.7. Histotripsy
4. Primary and Metastatic Liver Tumors

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Study Design | Recruitment Years | Country | Sample Size | Comparison | Cancer | Residual Disease | LTR | OS | PFS | Complications | Mean Ablation Time |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kamal et al. [13] | RCT | 2017 | Egypt | 56 | MWA vs. RFA | ≤5 cm HCC | 5.9% vs. 11.2% (p = 0.673) | 9.1% vs. 9.1% (1 year, p = 1.000) | 82.1% vs. 78.6% (1-year, p = 1.0) | 92.3% vs. 90.9% (p = 0.932) | 7.1% vs. 0% (NSD) | 4.41 vs. 14.21 min (p < 0.001) |
| Shibata et al. [58] | RCT | 1999–2000 | Japan | 72 | MWA vs. RFA | ≤4 cm HCC | 11% vs. 4% (p = 0.26) | 17.4% vs. 8.3% (27 months, p = 0.20) | 100% vs. 100% (27 months, p = 1.00) | N/A | 11.1% vs. 2.8% (p = 0.36 | 33 vs. 52 min (p < 0.001) |
| Vietti et al. [55] | RCT | 2011–2015 | Switzerland | 144 | MWA vs. RFA | ≤4 cm HCC | 5% vs. 4% at 1 month (p = 0.93) | 6% vs. 12% (48 months, p = 0.27) | 86% vs. 84% (2-year p = 0.87) | NSD, p = 0.80 | 2 grade 4 in MWA vs. 3 grade 3 in RFA | 4–6 vs. 12 min |
| Abdelaziz et al. [53] | RCT | 2009–2014 | Egypt | 111 | MWA vs. RFA | ≤5 cm HCC | Complete ablations: 96.1% vs. 94.2% (p = 0.60) | 3.9% vs. 13.5% (48. months, p = 0.49) | 62% vs. 47.4% (2-year, p = 0.49) | N/A | 3.2% vs. 11.1% (minor, p = 0.09) | N/A |
| Yu et al. [54] | RCT | 2008–2015 | China | 203 | MWA vs. RFA | ≤5 cm HCC | Effectiveness: 99.6% vs. 98.8% (p = 0.95) | N/A | 81.9% vs. 81.4% (3-year, p = 0.91) | N/A | 3.4% vs. 2.5% (major, p = 0.59) | 9 vs. 24.4 min (p < 0.001) |
| Chong et al. [56] | RCT | 2011–2017 | China | 93 | MWA vs. RFA | ≤5 cm HCC | 4.3% vs. 2.2% (1 month, p > 0.999) | N/A | 72.7% vs. 67.1% (3-year, p = 0.899) | DFS: 24.1% vs. 22.7% (3-year, p = 0.912) | 2.1% vs. 2.2% (overall, p > 0.999) | 12 vs. 24 min (p < 0.001) |
| Wang et al. [66] | RCT | 2008–2013 | China | 360 | Cryoablation vs. RFA | ≤4 cm HCC | Effectiveness: 98.5% vs. 95.8% (p = 0.106) | 5.6% vs. 10% (p = 0.115) | 67% vs. 66% (3-year, NSD) | DFS: 54% vs. 50% (3-year, NSD) | 3.9% vs. 3.3% (major, p = 0.776) | N/A |
| Chen et al. [82] | Retrospective population-based | 2004–2015 | United States | 3614 | Cryoablation vs. RFA | HCC | N/A | N/A | NSD | NSD in CSS | N/A | N/A |
| Meijerink et al. [67] | RCT | 2014–2018 | Netherlands | 51 | IRE | CRLM ≤ 5 cm | 74% achieved local tumor control after repeat procedures | 32% after 1 year | Median 2.7 years (95% CI: 1.6, 3.8) | 68% (95% CI: 59, 84) | 40% adverse effects | Median procedure time 2.43 h w/o anesthesia |
| Frühling et al. [68] | Nonrandomized clinical trial | 2011–2014 | Sweden | 30 | IRE | HCC and liver metastasis | 21.1% at 3 months and 34.2% at 6 months | 28.6% after both 3 and 6 months | 56.7% | N/A | 3.3% major, 20% minor, | - |
| Glassberg et al. [83] | Meta-analysis | 2009–2017 | N/A | 28 studies | MWA vs. RFA | HCC and liver metastasis | N/A | LTP: RR = 0.70; p = 0.02 | NSD in 1-, 3-, and 5-year OS | NSD in 1-, 3-, and 5-year DFS | RR = 1.05; p = 0.75 | N/A |
5. Renal Tumors
| Authors | Study Type | Inclusion Years | Sample Size | Comparison | Cancer | Findings |
|---|---|---|---|---|---|---|
| Thompson et al. [98] | Retrospective cohort | 2000–2011 | 1803 | Partial nephrectomy (PN) vs. RFA vs. cryoablation | T1N0M0 RCC | No significant difference in local recurrence-free survival. Metastases-free survival better in PN and cryoablation relative to RFA. |
| Atwell et al. [99] | Retrospective review | 2000–2010 | 385 | Cryoablation vs. RFA | RCC ≤ 3 cm | No significant difference in complications, local tumor recurrence, and local recurrence-free survival. |
| El Dib et al. [100] | Meta-analysis | 2000–2008 | 883 | Cryoablation vs. RFA | RCC | No significant difference in complications and pooled proportion of clinical efficacy |
| Atwell et al. [101] | Retrospective cohort | 2000–2010 | 533 | Cryoablation vs. RFA | RCC | No significant difference in major complication rates. |
| Andrews et al. [102] | Retrospective cohort | 2000–2011 | 1798 | PN vs. cryoablation vs. RFA | T1N0M0 | No significant difference in survival and local recurrence, and metastases. |
| Zhou & Arellano [107] | Retrospective cohort | 2006–2016 | 384 | MWA vs. RFA vs. cryoablation | T1cN0M0 RCC | Similar complication rates and immediate renal function changes. MWA had lowest ablation time, procedural time, and dosage of sedative. |
| Martin & Athreya [108] | Meta-analysis | 2003–2012 | 3153 | Cryoablation vs. MWA | Small renal masses | No significant difference in primary effectiveness, cancer-specific survival, local tumor progression, and progression to metastatic disease. |
| Zhou et al. [109] | Retrospective cohort | 2006–2016 | 297 | MWA vs. RFA vs. cryoablation | T1aN0M0 RCC | At 2 years follow-up, no significant difference in local recurrence, metastatic progression, stability of renal function, and adverse event rate. |
6. Pancreatic Tumors
7. Primary and Metastatic Adrenal Tumors
8. Thyroid and Parathyroid Tumors
| Authors | Study Type | Inclusion Years | Sample Size | Comparison | Cancer | Findings |
|---|---|---|---|---|---|---|
| Guo et al. [146] | Meta-analysis | 2016–2019 | 1768 patients | RFA vs. MWA | Benign thyroid nodules | Similar pooled 3- and 6-month volume reduction rate (VRR), symptom improvement, cosmetic scores, and complications. RFA showed superior 12-month VRR. |
| He et al. [147] | Meta-analysis | 1998–2015 | 873 patients | RFA vs. laser ablation (LA) vs. ethanol ablation (EA) | Benign thyroid nodules | RFA had the highest VRR. No significant difference in complication rate. RFA is most efficacious for solid or mostly solid nodules, EA for cyst or mostly cyst nodules. |
| Zheng et al. [148] | Meta-analysis | 2012–2018 | 1461 patients | Cooled MWA vs. uncooled MWA | Benign thyroid nodules | Similar pooled 3-month VRR and pooled proportion of major complications. Uncooled MWA had higher overall and minor complications with more pain and skin burns. |
| Ha et al. [149] | Meta-analysis | 2000–2013 | 184 patients | RFA vs. LA | Benign thyroid nodules | RFA was superior to laser ablation in reducing volume with fewer treatment sessions. No major complications with either. |
| Choi and Jung [150] | Meta-analysis | 2014–2019 | 715 patients | RFA vs. LA vs. MWA | Primary papillary thyroid microcarcinoma (PTMC) | RFA had the highest mean VVR, followed by MWA and LA. Comparable safety profiles. |
| Suh et al. [151] | Meta-analysis | 2008–2015 | 270 patients | RFA vs. EA | Locally recurrent thyroid cancer | RFA had a higher pooled VRR and pooled proportion of complete disappearance than EA. No significant difference in complication or recurrence rates. |
| Tong et al. [152] | Meta-analysis | 2005–2017 | 1187 patients | RFA vs. MWA vs. LA | PTMC | No significant difference in VVR, proportion of complete disappearance and recurrence, and in major complications rate. |
| Cho et al. [153] | Meta-analysis | 1999–2018 | 1208 patients | RFA vs. LA | Benign thyroid nodules | RFA had superior VRRs with less regrowth and delayed surgery. Comparable complication rates. |
| Trimboli et al. [135] | Meta-analysis | 2002–2019 | 3195 nodules | RFA vs. LA | Benign non-functioning solid thyroid nodules | While both were effective in reducing volumes (maintained up to 2–3 years), RFA had superior VRRs. |
| Yang, Hsu, and Liou [154] | Meta-analysis | 1994–2020 | 1514 patients | EA vs. RFA vs. polidocanol sclerotherapy vs. simple aspiration | Benign thyroid cystic nodules | No significant difference in VRR and therapeutic success rate between EA and RFA. EA had a higher pooled VRR than other modalities. |
| Wei et al. [155] | Multicenter retrospective cohort | 2015–2020 | 119 | RFA vs. MWA | Primary hyperparathyroidism | No significant difference in cure rates at 6 months and overall complication rates. |

9. Prostate Tumors
10. Primary and Metastatic Lung Tumors

11. Primary and Metastatic Bone Tumors
12. Primary and Metastatic Soft Tissue Tumors
13. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahmed, M.; Solbiati, L.; Brace, C.L.; Breen, D.J.; Callstrom, M.R.; Charboneau, J.W.; Chen, M.H.; Choi, B.I.; de Baère, T.; Dodd, G.D., III; et al. Image-guided tumor ablation: Standardization of terminology and reporting criteria—A 10-year update. Radiology 2014, 273, 241–260. [Google Scholar] [CrossRef] [PubMed]
- Ridouani, F.; Srimathveeravalli, G. Percutaneous image-guided ablation: From techniques to treatments. Presse Med. 2019, 48, e219–e231. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.A.; Kim, H.S. Interventional radiology and image-guided medicine: Interventional oncology. Semin Oncol. 2011, 38, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Auloge, P.; Cazzato, R.L.; Koch, G.; Caudrelier, J.; De Marini, P.; Garnon, J.; Gangi, A. Percutaneous tumor ablation. Presse Med. 2019, 48, 1146–1155. [Google Scholar] [CrossRef] [PubMed]
- Nadeem, S.; Zhang, P.; Rimner, A.; Sonke, J.J.; Deasy, J.O.; Tannenbaum, A. LDeform: Longitudinal deformation analysis for adaptive radiotherapy of lung cancer. Med. Phys. 2020, 47, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Nakao, M.; Nakamura, M.; Mizowaki, T.; Matsuda, T. Statistical deformation reconstruction using multi-organ shape features for pancreatic cancer localization. Med. Image Anal. 2021, 67, 101829. [Google Scholar] [CrossRef]
- Xu, X.; Carrera, E.; Augello, R.; Daneshkhah, E.; Yang, H. Benchmarks for higher-order modes evaluation in the free vibration response of open thin-walled beams due to the cross-sectional deformations. Thin-Walled Struct. 2021, 166, 107965. [Google Scholar] [CrossRef]
- Goldberg, S.N.; Gazelle, G.S.; Mueller, P.R. Thermal ablation therapy for focal malignancy: A unified approach to underlying principles, techniques, and diagnostic imaging guidance. AJR Am. J. Roentgenol. 2000, 174, 323–331. [Google Scholar] [CrossRef]
- Mauri, G.; Nicosia, L.; Varano, G.M.; Bonomo, G.; Della Vigna, P.; Monfardini, L.; Orsi, F. Tips and tricks for a safe and effective image-guided percutaneous renal tumour ablation. Insights Imaging 2017, 8, 357–363. [Google Scholar] [CrossRef] [Green Version]
- Carriero, S.; Della Pepa, G.; Monfardini, L.; Vitale, R.; Rossi, D.; Masperi, A.; Mauri, G. Role of Fusion Imaging in Image-Guided Thermal Ablations. Diagnostics 2021, 11, 549. [Google Scholar] [CrossRef]
- Zhou, Y.; Yang, Y.; Zhou, B.; Wang, Z.; Zhu, R.; Chen, X.; Ouyang, J.; Li, Q.; Zhou, J. Challenges Facing Percutaneous Ablation in the Treatment of Hepatocellular Carcinoma: Extension of Ablation Criteria. J. Hepatocell. Carcinoma 2021, 8, 625–644. [Google Scholar] [CrossRef] [PubMed]
- Citone, M.; Fanelli, F.; Falcone, G.; Mondaini, F.; Cozzi, D.; Miele, V. A closer look to the new frontier of artificial intelligence in the percutaneous treatment of primary lesions of the liver. Med. Oncol. 2020, 37, 55. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.; Elmoety, A.A.A.; Rostom, Y.A.M.; Shater, M.S.; Lashen, S.A. Percutaneous radiofrequency versus microwave ablation for management of hepatocellular carcinoma: A randomized controlled trial. J. Gastrointest. Oncol. 2019, 10, 562–571. [Google Scholar] [CrossRef] [PubMed]
- Malone, C.D.; Fetzer, D.T.; Monsky, W.L.; Itani, M.; Mellnick, V.M.; Velez, P.A.; Middleton, W.D.; Averkiou, M.A.; Ramaswamy, R.S. Contrast-enhanced US for the Interventional Radiologist: Current and Emerging Applications. Radiographics 2020, 40, 562–588. [Google Scholar] [CrossRef]
- Claudon, M.; Dietrich, C.F.; Choi, B.I.; Cosgrove, D.O.; Kudo, M.; Nolsøe, C.P.; Piscaglia, F.; Wilson, S.R.; Barr, R.G.; Chammas, M.C.; et al. Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) in the liver—Update 2012: A WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultraschall. Med. 2013, 34, 11–29. [Google Scholar] [CrossRef] [Green Version]
- Huang, Q.; Zeng, Q.; Long, Y.; Tan, L.; Zheng, R.; Xu, E.; Li, K. Fusion imaging techniques and contrast-enhanced ultrasound for thermal ablation of hepatocellular carcinoma—A prospective randomized controlled trial. Int. J. Hyperth. 2019, 36, 1207–1215. [Google Scholar] [CrossRef] [Green Version]
- Sánchez, Y.; Anvari, A.; Samir, A.E.; Arellano, R.S.; Prabhakar, A.M.; Uppot, R.N. Navigational Guidance and Ablation Planning Tools for Interventional Radiology. Curr. Probl. Diagn. Radiol. 2017, 46, 225–233. [Google Scholar] [CrossRef]
- Meziane, M. Computed Tomography Fluoroscopy. J. Bronchol. Interv. Pulmonol. 2005, 12, 69–70. [Google Scholar] [CrossRef]
- Maybody, M. An overview of image-guided percutaneous ablation of renal tumors. Semin. Interv. Radiol. 2010, 27, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Lakhoo, J.; Adams, R.; Dave, A.; Luo, L.; Vargo, C.J.; Isaacson, A.J.; Sher, A.; Fischman, A.; Yee, D.C.; Ryan, S.; et al. Radiopaque beads loaded with doxorubicin in the treatment of patients with hepatocellular carcinoma: A retrospective, multi-center study. Cancer Treat Res. Commun. 2020, 25, 100208. [Google Scholar] [CrossRef]
- Dreher, M.R.; Sharma, K.V.; Woods, D.L.; Reddy, G.; Tang, Y.; Pritchard, W.F.; Chiesa, O.A.; Karanian, J.W.; Esparza, J.A.; Donahue, D.; et al. Radiopaque drug-eluting beads for transcatheter embolotherapy: Experimental study of drug penetration and coverage in swine. J. Vasc. Interv. Radiol. 2012, 23, 257–264.e254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fartoux, L.; Arrive, L.; Andreani, T.; Serfaty, L.; Chazouillères, O.; Tubiana, J.M.; Poupon, R.; Rosmorduc, O. Treatment of small hepatocellular carcinoma with acetic acid percutaneous injection. Gastroenterol. Clin. Biol. 2005, 29, 1213–1219. [Google Scholar] [CrossRef]
- Livraghi, T.; Giorgio, A.; Marin, G.; Salmi, A.; de Sio, I.; Bolondi, L.; Pompili, M.; Brunello, F.; Lazzaroni, S.; Torzilli, G.; et al. Hepatocellular carcinoma and cirrhosis in 746 patients: Long-term results of percutaneous ethanol injection. Radiology 1995, 197, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Alzubaidi, S.J.; Liou, H.; Saini, G.; Segaran, N.; Scott Kriegshauser, J.; Naidu, S.G.; Patel, I.J.; Oklu, R. Percutaneous Image-Guided Ablation of Lung Tumors. J. Clin. Med. 2021, 10, 5783. [Google Scholar] [CrossRef]
- Hong, K.; Georgiades, C. Radiofrequency ablation: Mechanism of action and devices. J. Vasc. Interv. Radiol. 2010, 21, S179–S186. [Google Scholar] [CrossRef]
- Nelson, K.; Jutric, Z.; Georgiades, C. Physics and Physiology of Thermal Ablations. In Image-Guided Interventions in Oncology; Springer: Berlin/Heidelberg, Germany, 2020; pp. 1–13. [Google Scholar]
- Hinshaw, J.L.; Lubner, M.G.; Ziemlewicz, T.J.; Lee, F.T., Jr.; Brace, C.L. Percutaneous tumor ablation tools: Microwave, radiofrequency, or cryoablation--what should you use and why? Radiographics 2014, 34, 1344–1362. [Google Scholar] [CrossRef]
- Huang, S.; Yu, J.; Liang, P.; Yu, X.; Cheng, Z.; Han, Z.; Li, Q. Percutaneous microwave ablation for hepatocellular carcinoma adjacent to large vessels: A long-term follow-up. Eur. J. Radiol. 2014, 83, 552–558. [Google Scholar] [CrossRef]
- Rubinsky, B.; Lee, C.Y.; Bastacky, J.; Onik, G. The process of freezing and the mechanism of damage during hepatic cryosurgery. Cryobiology 1990, 27, 85–97. [Google Scholar] [CrossRef]
- Abtin, F.; Suh, R.D.; Nasehi, L.; Han, S.X.; Hsu, W.; Quirk, M.; Genshaft, S.; Gutierrez, A.J.; Cameron, R.B. Percutaneous cryoablation for the treatment of recurrent thymoma: Preliminary safety and efficacy. J. Vasc. Interv. Radiol. 2015, 26, 709–714. [Google Scholar] [CrossRef]
- Shiina, S.; Sato, K.; Tateishi, R.; Shimizu, M.; Ohama, H.; Hatanaka, T.; Takawa, M.; Nagamatsu, H.; Imai, Y. Percutaneous Ablation for Hepatocellular Carcinoma: Comparison of Various Ablation Techniques and Surgery. Can. J. Gastroenterol. Hepatol. 2018, 2018, 4756147. [Google Scholar] [CrossRef] [Green Version]
- Mazur, P. Freezing of living cells: Mechanisms and implications. Am. J. Physiol. 1984, 247, C125–C142. [Google Scholar] [CrossRef]
- Staren, E.D.; Sabel, M.S.; Gianakakis, L.M.; Wiener, G.A.; Hart, V.M.; Gorski, M.; Dowlatshahi, K.; Corning, B.F.; Haklin, M.F.; Koukoulis, G. Cryosurgery of breast cancer. Arch. Surg. 1997, 132, 28–34. [Google Scholar] [CrossRef]
- Golberg, A.; Yarmush, M.L. Nonthermal irreversible electroporation: Fundamentals, applications, and challenges. IEEE Trans. Biomed. Eng. 2013, 60, 707–714. [Google Scholar] [CrossRef]
- Faroja, M.; Ahmed, M.; Appelbaum, L.; Ben-David, E.; Moussa, M.; Sosna, J.; Nissenbaum, I.; Goldberg, S.N. Irreversible electroporation ablation: Is all the damage nonthermal? Radiology 2013, 266, 462–470. [Google Scholar] [CrossRef]
- Ahmed, M.; Brace, C.L.; Lee, F.T., Jr.; Goldberg, S.N. Principles of and advances in percutaneous ablation. Radiology 2011, 258, 351–369. [Google Scholar] [CrossRef]
- Copelan, A.; Hartman, J.; Chehab, M.; Venkatesan, A.M. High-Intensity Focused Ultrasound: Current Status for Image-Guided Therapy. Semin. Interv. Radiol. 2015, 32, 398–415. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.S.; Rhim, H.; Choi, M.J.; Lim, H.K.; Choi, D. High-intensity focused ultrasound therapy: An overview for radiologists. Korean J. Radiol. 2008, 9, 291–302. [Google Scholar] [CrossRef] [Green Version]
- Haar, G.T.; Coussios, C. High intensity focused ultrasound: Physical principles and devices. Int. J. Hyperth. 2007, 23, 89–104. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.; Hall, T.L.; Vlaisavljevich, E.; Lee, F.T., Jr. Histotripsy: The first noninvasive, non-ionizing, non-thermal ablation technique based on ultrasound. Int. J. Hyperth. 2021, 38, 561–575. [Google Scholar] [CrossRef]
- Bader, K.B.; Hendley, S.A.; Anthony, G.J.; Bollen, V. Observation and modulation of the dissolution of histotripsy-induced bubble clouds with high-frame rate plane wave imaging. Phys. Med. Biol. 2019, 64, 115012. [Google Scholar] [CrossRef]
- Khokhlova, V.A.; Fowlkes, J.B.; Roberts, W.W.; Schade, G.R.; Xu, Z.; Khokhlova, T.D.; Hall, T.L.; Maxwell, A.D.; Wang, Y.N.; Cain, C.A. Histotripsy methods in mechanical disintegration of tissue: Towards clinical applications. Int. J. Hyperth. 2015, 31, 145–162. [Google Scholar] [CrossRef] [PubMed]
- Vitale, A.; Huo, T.L.; Cucchetti, A.; Lee, Y.H.; Volk, M.; Frigo, A.C.; Cescon, M.; Tuci, F.; Pinna, A.D.; Cillo, U. Survival Benefit of Liver Transplantation Versus Resection for Hepatocellular Carcinoma: Impact of MELD Score. Ann. Surg. Oncol. 2015, 22, 1901–1907. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Yaghmai, V.; Besa, C.; Kim, E.; Gatlin, J.L.; Siddiqui, N.A.; Taouli, B. Imaging assessment of hepatocellular carcinoma response to locoregional and systemic therapy. AJR Am. J. Roentgenol. 2013, 201, 80–96. [Google Scholar] [CrossRef]
- Dodd, G.D., 3rd; Dodd, N.A.; Lanctot, A.C.; Glueck, D.A. Effect of variation of portal venous blood flow on radiofrequency and microwave ablations in a blood-perfused bovine liver model. Radiology 2013, 267, 129–136. [Google Scholar] [CrossRef]
- Primavesi, F.; Swierczynski, S.; Klieser, E.; Kiesslich, T.; Jäger, T.; Urbas, R.; Hutter, J.; Neureiter, D.; Öfner, D.; Stättner, S. Thermographic real-time-monitoring of surgical radiofrequency and microwave ablation in a perfused porcine liver model. Oncol. Lett. 2018, 15, 2913–2920. [Google Scholar] [CrossRef] [Green Version]
- Brace, C.L. Radiofrequency and microwave ablation of the liver, lung, kidney, and bone: What are the differences? Curr. Probl. Diagn. Radiol. 2009, 38, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Rossmann, C.; Garrett-Mayer, E.; Rattay, F.; Haemmerich, D. Dynamics of tissue shrinkage during ablative temperature exposures. Physiol. Meas. 2014, 35, 55–67. [Google Scholar] [CrossRef] [Green Version]
- Radosevic, A.; Quesada, R.; Serlavos, C.; Sánchez, J.; Zugazaga, A.; Sierra, A.; Coll, S.; Busto, M.; Aguilar, G.; Flores, D.; et al. Microwave versus radiofrequency ablation for the treatment of liver malignancies: A randomized controlled phase 2 trial. Sci. Rep. 2022, 12, 316. [Google Scholar] [CrossRef]
- Poulou, L.S.; Botsa, E.; Thanou, I.; Ziakas, P.D.; Thanos, L. Percutaneous microwave ablation vs. radiofrequency ablation in the treatment of hepatocellular carcinoma. World J. Hepatol. 2015, 7, 1054–1063. [Google Scholar] [CrossRef] [PubMed]
- Abdelaziz, A.; Elbaz, T.; Shousha, H.I.; Mahmoud, S.; Ibrahim, M.; Abdelmaksoud, A.; Nabeel, M. Efficacy and survival analysis of percutaneous radiofrequency versus microwave ablation for hepatocellular carcinoma: An Egyptian multidisciplinary clinic experience. Surg. Endosc. 2014, 28, 3429–3434. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Yu, X.L.; Han, Z.Y.; Cheng, Z.G.; Liu, F.Y.; Zhai, H.Y.; Mu, M.J.; Liu, Y.M.; Liang, P. Percutaneous cooled-probe microwave versus radiofrequency ablation in early-stage hepatocellular carcinoma: A phase III randomised controlled trial. Gut 2017, 66, 1172–1173. [Google Scholar] [CrossRef] [Green Version]
- Vietti Violi, N.; Duran, R.; Guiu, B.; Cercueil, J.P.; Aubé, C.; Digklia, A.; Pache, I.; Deltenre, P.; Knebel, J.F.; Denys, A. Efficacy of microwave ablation versus radiofrequency ablation for the treatment of hepatocellular carcinoma in patients with chronic liver disease: A randomised controlled phase 2 trial. Lancet Gastroenterol. Hepatol. 2018, 3, 317–325. [Google Scholar] [CrossRef]
- Chong, C.C.N.; Lee, K.F.; Cheung, S.Y.S.; Chu, C.C.M.; Fong, A.K.W.; Wong, J.; Hui, J.W.Y.; Fung, A.K.Y.; Lok, H.T.; Lo, E.Y.J.; et al. Prospective double-blinded randomized controlled trial of Microwave versus RadioFrequency Ablation for hepatocellular carcinoma (McRFA trial). HPB 2020, 22, 1121–1127. [Google Scholar] [CrossRef]
- Han, J.; Fan, Y.C.; Wang, K. Radiofrequency ablation versus microwave ablation for early stage hepatocellular carcinoma: A PRISMA-compliant systematic review and meta-analysis. Medicine 2020, 99, e22703. [Google Scholar] [CrossRef]
- Shibata, T.; Iimuro, Y.; Yamamoto, Y.; Maetani, Y.; Ametani, F.; Itoh, K.; Konishi, J. Small hepatocellular carcinoma: Comparison of radio-frequency ablation and percutaneous microwave coagulation therapy. Radiology 2002, 223, 331–337. [Google Scholar] [CrossRef]
- Glassberg, M.B.; Ghosh, S.; Clymer, J.W.; Wright, G.W.J.; Ferko, N.; Amaral, J.F. Microwave ablation compared with hepatic resection for the treatment of hepatocellular carcinoma and liver metastases: A systematic review and meta-analysis. World J. Surg. Oncol. 2019, 17, 98. [Google Scholar] [CrossRef]
- Lencioni, R.A.; Allgaier, H.P.; Cioni, D.; Olschewski, M.; Deibert, P.; Crocetti, L.; Frings, H.; Laubenberger, J.; Zuber, I.; Blum, H.E.; et al. Small hepatocellular carcinoma in cirrhosis: Randomized comparison of radio-frequency thermal ablation versus percutaneous ethanol injection. Radiology 2003, 228, 235–240. [Google Scholar] [CrossRef]
- Bilchik, A.J.; Wood, T.F.; Allegra, D.; Tsioulias, G.J.; Chung, M.; Rose, D.M.; Ramming, K.P.; Morton, D.L. Cryosurgical ablation and radiofrequency ablation for unresectable hepatic malignant neoplasms: A proposed algorithm. Arch. Surg. 2000, 135, 657–662; discussion 662–654. [Google Scholar] [CrossRef] [Green Version]
- Song, K.D. Percutaneous cryoablation for hepatocellular carcinoma. Clin. Mol. Hepatol. 2016, 22, 509–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, J.; Noda, C.; Erickson, A.; Mokkarala, M.; Charalel, R.; Ramaswamy, R.; Tao, Y.U.; Akinwande, O. Radiofrequency Ablation vs. Cryoablation for Localized Hepatocellular Carcinoma: A Propensity-matched Population Study. Anticancer Res. 2018, 38, 6381–6386. [Google Scholar] [CrossRef] [PubMed]
- McWilliams, J.P.; Yamamoto, S.; Raman, S.S.; Loh, C.T.; Lee, E.W.; Liu, D.M.; Kee, S.T. Percutaneous ablation of hepatocellular carcinoma: Current status. J. Vasc. Interv. Radiol. 2010, 21, S204–S213. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Hou, J.; Ding, Y.; Wu, F.; Hu, Y.; Jiang, Q.; Mao, P.; Yang, Y. Cryoablation Versus Radiofrequency Ablation for Hepatic Malignancies: A Systematic Review and Literature-Based Analysis. Medicine 2015, 94, e2252. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, H.; Yang, W.; Hu, K.; Xie, H.; Hu, K.Q.; Bai, W.; Dong, Z.; Lu, Y.; Zeng, Z.; et al. Multicenter randomized controlled trial of percutaneous cryoablation versus radiofrequency ablation in hepatocellular carcinoma. Hepatology 2015, 61, 1579–1590. [Google Scholar] [CrossRef] [PubMed]
- Meijerink, M.R.; Ruarus, A.H.; Vroomen, L.; Puijk, R.S.; Geboers, B.; Nieuwenhuizen, S.; van den Bemd, B.A.T.; Nielsen, K.; de Vries, J.J.J.; van Lienden, K.P.; et al. Irreversible Electroporation to Treat Unresectable Colorectal Liver Metastases (COLDFIRE-2): A Phase II, Two-Center, Single-Arm Clinical Trial. Radiology 2021, 299, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Frühling, P.; Nilsson, A.; Duraj, F.; Haglund, U.; Norén, A. Single-center nonrandomized clinical trial to assess the safety and efficacy of irreversible electroporation (IRE) ablation of liver tumors in humans: Short to mid-term results. Eur J. Surg. Oncol. 2017, 43, 751–757. [Google Scholar] [CrossRef]
- Tian, G.; Zhao, Q.; Chen, F.; Jiang, T.; Wang, W. Ablation of hepatic malignant tumors with irreversible electroporation: A systematic review and meta-analysis of outcomes. Oncotarget 2017, 8, 5853–5860. [Google Scholar] [CrossRef] [Green Version]
- Gupta, P.; Maralakunte, M.; Sagar, S.; Kumar, M.P.; Bhujade, H.; Chaluvashetty, S.B.; Kalra, N. Efficacy and safety of irreversible electroporation for malignant liver tumors: A systematic review and meta-analysis. Eur. Radiol. 2021, 31, 6511–6521. [Google Scholar] [CrossRef]
- Yu, M.; Li, S. Irreversible electroporation for liver cancer ablation: A meta analysis. Eur. J. Surg. Oncol. 2021; in press. [Google Scholar] [CrossRef]
- Lyu, T.; Wang, X.; Su, Z.; Shangguan, J.; Sun, C.; Figini, M.; Wang, J.; Yaghmai, V.; Larson, A.C.; Zhang, Z. Irreversible electroporation in primary and metastatic hepatic malignancies: A review. Medicine 2017, 96, e6386. [Google Scholar] [CrossRef]
- Cheung, T.T.; Fan, S.T.; Chu, F.S.; Jenkins, C.R.; Chok, K.S.; Tsang, S.H.; Dai, W.C.; Chan, A.C.; Chan, S.C.; Yau, T.C.; et al. Survival analysis of high-intensity focused ultrasound ablation in patients with small hepatocellular carcinoma. HPB 2013, 15, 567–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, T.T.; Chu, F.S.; Jenkins, C.R.; Tsang, D.S.; Chok, K.S.; Chan, A.C.; Yau, T.C.; Chan, S.C.; Poon, R.T.; Lo, C.M.; et al. Tolerance of high-intensity focused ultrasound ablation in patients with hepatocellular carcinoma. World J. Surg. 2012, 36, 2420–2427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, G.; Luo, G.; He, L.; Li, J.; Shan, H.; Zhang, R.; Li, Y.; Gao, X.; Lin, S.; Wang, G. Follow-up of high-intensity focused ultrasound treatment for patients with hepatocellular carcinoma. Ultrasound Med. Biol. 2011, 37, 1993–1999. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, H.; Ito, R.; Ohto, M.; Sakamoto, A.; Karasawa, E.; Yamaguchi, T.; Shinozuka, N.; Zhu, H.; Wanga, Z.B. Treatment of small hepatocellular carcinomas with US-guided high-intensity focused ultrasound. Ultrasound Med. Biol. 2011, 37, 1222–1229. [Google Scholar] [CrossRef]
- Ng, K.K.; Poon, R.T.; Chan, S.C.; Chok, K.S.; Cheung, T.T.; Tung, H.; Chu, F.; Tso, W.K.; Yu, W.C.; Lo, C.M.; et al. High-intensity focused ultrasound for hepatocellular carcinoma: A single-center experience. Ann. Surg. 2011, 253, 981–987. [Google Scholar] [CrossRef] [Green Version]
- Ji, Y.; Zhu, J.; Zhu, L.; Zhu, Y.; Zhao, H. High-Intensity Focused Ultrasound Ablation for Unresectable Primary and Metastatic Liver Cancer: Real-World Research in a Chinese Tertiary Center with 275 Cases. Front. Oncol. 2020, 10, 519164. [Google Scholar] [CrossRef]
- Chan, A.C.; Cheung, T.T.; Fan, S.T.; Chok, K.S.; Chan, S.C.; Poon, R.T.; Lo, C.M. Survival analysis of high-intensity focused ultrasound therapy versus radiofrequency ablation in the treatment of recurrent hepatocellular carcinoma. Ann. Surg. 2013, 257, 686–692. [Google Scholar] [CrossRef]
- Yu, S.J.; Yoon, J.H.; Lee, J.M.; Lee, J.Y.; Kim, S.H.; Cho, Y.Y.; Yoo, J.J.; Lee, M.; Lee, D.H.; Cho, Y.; et al. Percutaneous ethanol injection therapy is comparable to radiofrequency ablation in hepatocellular carcinoma smaller than 1.5 cm: A matched case-control comparative analysis. Medicine 2016, 95, e4551. [Google Scholar] [CrossRef]
- Yang, B.; Zan, R.Y.; Wang, S.Y.; Li, X.L.; Wei, M.L.; Guo, W.H.; You, X.; Li, J.; Liao, Z.Y. Radiofrequency ablation versus percutaneous ethanol injection for hepatocellular carcinoma: A meta-analysis of randomized controlled trials. World J. Surg. Oncol. 2015, 13, 96. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Ren, Y.; Sun, T.; Cao, Y.; Yan, L.; Zhang, W.; Ouyang, T.; Zheng, C. The efficacy of radiofrequency ablation versus cryoablation in the treatment of single hepatocellular carcinoma: A population-based study. Cancer Med. 2021, 10, 3715–3725. [Google Scholar] [CrossRef]
- Glassberg, M.B.; Ghosh, S.; Clymer, J.W.; Qadeer, R.A.; Ferko, N.C.; Sadeghirad, B.; Wright, G.W.; Amaral, J.F. Microwave ablation compared with radiofrequency ablation for treatment of hepatocellular carcinoma and liver metastases: A systematic review and meta-analysis. OncoTargets Ther. 2019, 12, 6407–6438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.R.; Thomas, S. Complications of image-guided thermal ablation of liver and kidney neoplasms. Semin. Interv. Radiol. 2014, 31, 138–148. [Google Scholar] [CrossRef] [Green Version]
- Lahat, E.; Eshkenazy, R.; Zendel, A.; Zakai, B.B.; Maor, M.; Dreznik, Y.; Ariche, A. Complications after percutaneous ablation of liver tumors: A systematic review. Hepatobiliary Surg. Nutr. 2014, 3, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, A.; Grand, D.; Charpentier, K.P. Irreversible electroporation of hepatocellular carcinoma: Patient selection and perspectives. J. Hepatocell. Carcinoma 2017, 4, 49–58. [Google Scholar] [CrossRef] [Green Version]
- Alnaggar, M.; Qaid, A.M.; Chen, J.; Niu, L.; Xu, K. Irreversible electroporation of malignant liver tumors: Effect on laboratory values. Oncol. Lett. 2018, 16, 3881–3888. [Google Scholar] [CrossRef] [Green Version]
- Tsang, S.H.; Ma, K.W.; She, W.H.; Chu, F.; Lau, V.; Lam, S.W.; Cheung, T.T.; Lo, C.M. High-intensity focused ultrasound ablation of liver tumors in difficult locations. Int. J. Hyperth. 2021, 38, 56–64. [Google Scholar] [CrossRef]
- Herr, H.W. A history of partial nephrectomy for renal tumors. J. Urol. 2005, 173, 705–708. [Google Scholar] [CrossRef]
- Pierorazio, P.M.; Johnson, M.H.; Patel, H.D.; Sozio, S.M.; Sharma, R.; Iyoha, E.; Bass, E.B.; Allaf, M.E. AHRQ Comparative Effectiveness Reviews. In Management of Renal Masses and Localized Renal Cancer; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2016. [Google Scholar]
- Ljungberg, B.; Cowan, N.C.; Hanbury, D.C.; Hora, M.; Kuczyk, M.A.; Merseburger, A.S.; Patard, J.J.; Mulders, P.F.; Sinescu, I.C. EAU guidelines on renal cell carcinoma: The 2010 update. Eur. Urol. 2010, 58, 398–406. [Google Scholar] [CrossRef]
- Thompson, R.H.; Atwell, T.; Schmit, G.; Lohse, C.M.; Kurup, A.N.; Weisbrod, A.; Psutka, S.P.; Stewart, S.B.; Callstrom, M.R.; Cheville, J.C.; et al. Reply to Pascal Mouracade’s letter to the editor re: R. Houston Thompson, Tom Atwell, Grant Schmit; et al. Comparison of partial nephrectomy and percutaneous ablation for cT1 renal masses. Eur Urol 2015;67:252–9. Eur. Urol. 2015, 68, e84–e85. [Google Scholar] [CrossRef]
- Gervais, D.A.; McGovern, F.J.; Wood, B.J.; Goldberg, S.N.; McDougal, W.S.; Mueller, P.R. Radio-frequency ablation of renal cell carcinoma: Early clinical experience. Radiology 2000, 217, 665–672. [Google Scholar] [CrossRef] [Green Version]
- Jasinski, M.; Siekiera, J.; Chlosta, P.; Mikolajczak, W.; Drewa, T. Radiofrequency ablation of small renal masses as an alternative to nephron-sparing surgery: Preliminary results. Wideochir. Inne Tech. Maloinwazyjne 2011, 6, 242–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frey, G.T.; Sella, D.M.; Atwell, T.D. Image-Guided Renal Intervention. Radiol. Clin. N. Am. 2015, 53, 1005–1019. [Google Scholar] [CrossRef] [PubMed]
- Cazalas, G.; Jambon, E.; Coussy, A.; Le Bras, Y.; Petitpierre, F.; Berhnard, J.C.; Grenier, N.; Marcelin, C. Local recurrence and other oncologic outcomes after percutaneous image-guided tumor ablations on stageT1b renal cell carcinoma: A systematic review and network meta-analysis. Int. J. Hyperth. 2021, 38, 1295–1303. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Kidney Cancer (Version 4.2022). Available online: https://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf (accessed on 1 January 2022).
- Thompson, R.H.; Atwell, T.; Schmit, G.; Lohse, C.M.; Kurup, A.N.; Weisbrod, A.; Psutka, S.P.; Stewart, S.B.; Callstrom, M.R.; Cheville, J.C.; et al. Comparison of partial nephrectomy and percutaneous ablation for cT1 renal masses. Eur. Urol. 2015, 67, 252–259. [Google Scholar] [CrossRef]
- Atwell, T.D.; Schmit, G.D.; Boorjian, S.A.; Mandrekar, J.; Kurup, A.N.; Weisbrod, A.J.; Chow, G.K.; Leibovich, B.C.; Callstrom, M.R.; Patterson, D.E.; et al. Percutaneous ablation of renal masses measuring 3.0 cm and smaller: Comparative local control and complications after radiofrequency ablation and cryoablation. AJR Am. J. Roentgenol. 2013, 200, 461–466. [Google Scholar] [CrossRef]
- El Dib, R.; Touma, N.J.; Kapoor, A. Cryoablation vs. radiofrequency ablation for the treatment of renal cell carcinoma: A meta-analysis of case series studies. BJU Int. 2012, 110, 510–516. [Google Scholar] [CrossRef]
- Atwell, T.D.; Carter, R.E.; Schmit, G.D.; Carr, C.M.; Boorjian, S.A.; Curry, T.B.; Thompson, R.H.; Kurup, A.N.; Weisbrod, A.J.; Chow, G.K.; et al. Complications following 573 percutaneous renal radiofrequency and cryoablation procedures. J. Vasc. Interv. Radiol. 2012, 23, 48–54. [Google Scholar] [CrossRef]
- Andrews, J.R.; Atwell, T.; Schmit, G.; Lohse, C.M.; Kurup, A.N.; Weisbrod, A.; Callstrom, M.R.; Cheville, J.C.; Boorjian, S.A.; Leibovich, B.C.; et al. Oncologic Outcomes Following Partial Nephrectomy and Percutaneous Ablation for cT1 Renal Masses. Eur. Urol. 2019, 76, 244–251. [Google Scholar] [CrossRef]
- Zhong, J.; Wah, T.M. Renal ablation: Current management strategies and controversies. Chin. Clin. Oncol. 2019, 8, 63. [Google Scholar] [CrossRef]
- Psutka, S.P.; Feldman, A.S.; McDougal, W.S.; McGovern, F.J.; Mueller, P.; Gervais, D.A. Long-term oncologic outcomes after radiofrequency ablation for T1 renal cell carcinoma. Eur. Urol. 2013, 63, 486–492. [Google Scholar] [CrossRef]
- Atwell, T.D.; Vlaminck, J.J.; Boorjian, S.A.; Kurup, A.N.; Callstrom, M.R.; Weisbrod, A.J.; Lohse, C.M.; Hartman, W.R.; Stockland, A.H.; Leibovich, B.C.; et al. Percutaneous cryoablation of stage T1b renal cell carcinoma: Technique considerations, safety, and local tumor control. J. Vasc. Interv. Radiol. 2015, 26, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Schmit, G.D.; Atwell, T.D.; Callstrom, M.R.; Farrell, M.A.; Leibovich, B.C.; Patterson, D.E.; Chow, G.K.; Blute, M.L.; Charboneau, J.W. Percutaneous cryoablation of renal masses >or=3 cm: Efficacy and safety in treatment of 108 patients. J. Endourol. 2010, 24, 1255–1262. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Arellano, R.S. Thermal Ablation of T1c Renal Cell Carcinoma: A Comparative Assessment of Technical Performance, Procedural Outcome, and Safety of Microwave Ablation, Radiofrequency Ablation, and Cryoablation. J. Vasc. Interv. Radiol. 2018, 29, 943–951. [Google Scholar] [CrossRef]
- Martin, J.; Athreya, S. Meta-analysis of cryoablation versus microwave ablation for small renal masses: Is there a difference in outcome? Diagn. Interv. Radiol. 2013, 19, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Herwald, S.E.; McCarthy, C.; Uppot, R.N.; Arellano, R.S. Radiofrequency Ablation, Cryoablation, and Microwave Ablation for T1a Renal Cell Carcinoma: A Comparative Evaluation of Therapeutic and Renal Function Outcomes. J. Vasc. Interv. Radiol. 2019, 30, 1035–1042. [Google Scholar] [CrossRef] [PubMed]
- Kurup, A.N. Percutaneous ablation for small renal masses-complications. Semin. Interv. Radiol. 2014, 31, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Dong, X.; Li, X.; Yu, J.; Yu, M.A.; Yu, X.; Liang, P. Complications of ultrasound-guided percutaneous microwave ablation of renal cell carcinoma. OncoTargets Ther. 2016, 9, 5903–5909. [Google Scholar] [CrossRef] [Green Version]
- Patel, I.J.; Rahim, S.; Davidson, J.C.; Hanks, S.E.; Tam, A.L.; Walker, T.G.; Wilkins, L.R.; Sarode, R.; Weinberg, I. Society of Interventional Radiology Consensus Guidelines for the Periprocedural Management of Thrombotic and Bleeding Risk in Patients Undergoing Percutaneous Image-Guided Interventions-Part II: Recommendations: Endorsed by the Canadian Association for Interventional Radiology and the Cardiovascular and Interventional Radiological Society of Europe. J. Vasc. Interv. Radiol. 2019, 30, 1168–1184.e1161. [Google Scholar] [CrossRef] [Green Version]
- Samadi, K.; Arellano, R.S. Ureteral protection during microwave ablation of renal cell carcinoma: Combined use of pyeloperfusion and hydrodissection. Diagn. Interv. Radiol. 2018, 24, 388–391. [Google Scholar] [CrossRef]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Behrman, S.W.; Benson, A.B.; Cardin, D.B.; Chiorean, E.G.; Chung, V.; Czito, B.; Del Chiaro, M.; et al. Pancreatic Adenocarcinoma, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2021, 19, 439–457. [Google Scholar] [CrossRef]
- Granata, V.; Grassi, R.; Fusco, R.; Setola, S.V.; Palaia, R.; Belli, A.; Miele, V.; Brunese, L.; Grassi, R.; Petrillo, A.; et al. Assessment of Ablation Therapy in Pancreatic Cancer: The Radiologist’s Challenge. Front. Oncol. 2020, 10, 560952. [Google Scholar] [CrossRef] [PubMed]
- Paiella, S.; Salvia, R.; Ramera, M.; Girelli, R.; Frigerio, I.; Giardino, A.; Allegrini, V.; Bassi, C. Local Ablative Strategies for Ductal Pancreatic Cancer (Radiofrequency Ablation, Irreversible Electroporation): A Review. Gastroenterol. Res. Pract. 2016, 2016, 4508376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Veldhuisen, E.; van den Oord, C.; Brada, L.J.; Walma, M.S.; Vogel, J.A.; Wilmink, J.W.; Del Chiaro, M.; van Lienden, K.P.; Meijerink, M.R.; van Tienhoven, G.; et al. Locally Advanced Pancreatic Cancer: Work-Up, Staging, and Local Intervention Strategies. Cancers 2019, 11, 976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walma, M.S.; Rombouts, S.J.; Brada, L.J.H.; Borel Rinkes, I.H.; Bosscha, K.; Bruijnen, R.C.; Busch, O.R.; Creemers, G.J.; Daams, F.; van Dam, R.M.; et al. Radiofrequency ablation and chemotherapy versus chemotherapy alone for locally advanced pancreatic cancer (PELICAN): Study protocol for a randomized controlled trial. Trials 2021, 22, 313. [Google Scholar] [CrossRef]
- Rombouts, S.J.; Vogel, J.A.; van Santvoort, H.C.; van Lienden, K.P.; van Hillegersberg, R.; Busch, O.R.; Besselink, M.G.; Molenaar, I.Q. Systematic review of innovative ablative therapies for the treatment of locally advanced pancreatic cancer. Br. J. Surg. 2015, 102, 182–193. [Google Scholar] [CrossRef]
- Narayanan, G.; Doshi, M.H. Ablation for Pancreatic Carcinoma. Endovasc. Today 2015, 14, 96–99. [Google Scholar]
- Maiettini, D.; Mauri, G.; Varano, G.; Bonomo, G.; Della Vigna, P.; Rebonato, A.; Orsi, F. Pancreatic ablation: Minimally invasive treatment options. Int. J. Hyperth. 2019, 36, 53–58. [Google Scholar] [CrossRef]
- Narayanan, G.; Daye, D.; Wilson, N.M.; Noman, R.; Mahendra, A.M.; Doshi, M.H. Ablation in Pancreatic Cancer: Past, Present and Future. Cancers 2021, 13, 2511. [Google Scholar] [CrossRef]
- Donlon, P.; Dennedy, M.C. Thermal ablation in adrenal disorders: A discussion of the technology, the clinical evidence and the future. Curr. Opin. Endocrinol. Diabetes Obes. 2021, 28, 291–302. [Google Scholar] [CrossRef]
- Yamakado, K. Image-guided ablation of adrenal lesions. Semin. Interv. Radiol. 2014, 31, 149–156. [Google Scholar] [CrossRef] [Green Version]
- Dennedy, M.C.; Annamalai, A.K.; Prankerd-Smith, O.; Freeman, N.; Vengopal, K.; Graggaber, J.; Koulouri, O.; Powlson, A.S.; Shaw, A.; Halsall, D.J.; et al. Low DHEAS: A Sensitive and Specific Test for the Detection of Subclinical Hypercortisolism in Adrenal Incidentalomas. J. Clin. Endocrinol. Metab. 2017, 102, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, J.; Raymond, A.; Somasundaram, A.; Loya, M.F.; Nezami, N. Novel Protocol for CT-Guided Percutaneous Ablation of Hyperplastic Adrenal Glands in Cushing Syndrome. CardioVascular Interv. Radiol. 2022, 45, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Rosiak, G.; Milczarek, K.; Konecki, D.; Otto, M.; Rowinski, O.; Zgliczynski, W. Percutaneous Bilateral Adrenal Radiofrequency Ablation in Severe Adrenocorticotropic Hormone-dependent Cushing Syndrome. J. Clin. Imaging Sci. 2020, 10, 60. [Google Scholar] [CrossRef] [PubMed]
- Pan, S.; Baal, J.D.; Chen, W.C.; Baal, U.; Pai, J.S.; Baal, J.H.; Zagoria, R. Image-Guided Percutaneous Ablation of Adrenal Metastases: A Meta-Analysis of Efficacy and Safety. J. Vasc. Interv. Radiol. 2021, 32, 527–535.e521. [Google Scholar] [CrossRef]
- Kohlenberg, J.; Welch, B.; Hamidi, O.; Callstrom, M.; Morris, J.; Sprung, J.; Bancos, I.; Young, W., Jr. Efficacy and Safety of Ablative Therapy in the Treatment of Patients with Metastatic Pheochromocytoma and Paraganglioma. Cancers 2019, 11, 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkatesan, A.M.; Locklin, J.; Dupuy, D.E.; Wood, B.J. Percutaneous ablation of adrenal tumors. Tech. Vasc. Interv. Radiol. 2010, 13, 89–99. [Google Scholar] [CrossRef] [Green Version]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Spiezia, S.; Garberoglio, R.; Milone, F.; Ramundo, V.; Caiazzo, C.; Assanti, A.P.; Deandrea, M.; Limone, P.P.; Macchia, P.E.; Lombardi, G.; et al. Thyroid nodules and related symptoms are stably controlled two years after radiofrequency thermal ablation. Thyroid 2009, 19, 219–225. [Google Scholar] [CrossRef]
- Huh, J.Y.; Baek, J.H.; Choi, H.; Kim, J.K.; Lee, J.H. Symptomatic benign thyroid nodules: Efficacy of additional radiofrequency ablation treatment session—Prospective randomized study. Radiology 2012, 263, 909–916. [Google Scholar] [CrossRef]
- Bernardi, S.; Dobrinja, C.; Fabris, B.; Bazzocchi, G.; Sabato, N.; Ulcigrai, V.; Giacca, M.; Barro, E.; De Manzini, N.; Stacul, F. Radiofrequency ablation compared to surgery for the treatment of benign thyroid nodules. Int. J. Endocrinol. 2014, 2014, 934595. [Google Scholar] [CrossRef] [Green Version]
- Trimboli, P.; Castellana, M.; Sconfienza, L.M.; Virili, C.; Pescatori, L.C.; Cesareo, R.; Giorgino, F.; Negro, R.; Giovanella, L.; Mauri, G. Efficacy of thermal ablation in benign non-functioning solid thyroid nodule: A systematic review and meta-analysis. Endocrine 2020, 67, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Yoo, W.S.; Park, Y.J.; Park, D.J.; Yun, T.J.; Choi, S.H.; Sohn, C.H.; Lee, K.E.; Sung, M.W.; Youn, Y.K.; et al. Efficacy and Safety of Radiofrequency Ablation for Treatment of Locally Recurrent Thyroid Cancers Smaller than 2 cm. Radiology 2015, 276, 909–918. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.R.; Baek, J.H.; Choi, Y.J.; Lee, J.H. Longer-term outcomes of radiofrequency ablation for locally recurrent papillary thyroid cancer. Eur. Radiol. 2019, 29, 4897–4903. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Jung, S.L.; Bae, J.S.; Lee, S.H.; Jung, C.K.; Jang, J.; Shin, N.Y.; Choi, H.S.; Ahn, K.J.; Kim, B.S. Comparison of efficacy and complications between radiofrequency ablation and repeat surgery in the treatment of locally recurrent thyroid cancers: A single-center propensity score matching study. Int. J. Hyperth. 2019, 36, 359–367. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.K.; Baek, J.H.; Lee, J.H.; Kim, W.B.; Kim, T.Y.; Shong, Y.K.; Hong, S.J. Efficacy and safety of radiofrequency ablation for treating locoregional recurrence from papillary thyroid cancer. Eur. Radiol. 2015, 25, 163–170. [Google Scholar] [CrossRef]
- Li, J.; Liu, Y.; Liu, J.; Yang, P.; Hu, X.; Qian, L. A comparative study of short-term efficacy and safety for thyroid micropapillary carcinoma patients after microwave ablation or surgery. Int. J. Hyperth. 2019, 36, 640–646. [Google Scholar] [CrossRef]
- Gong, L.; Tang, W.; Lu, J.; Xu, W. Thermal ablation versus parathyroidectomy for secondary hyperparathyroidism: A meta-analysis. Int. J. Surg. 2019, 70, 13–18. [Google Scholar] [CrossRef]
- Ye, J.; Huang, W.; Huang, G.; Qiu, Y.; Peng, W.; Lan, N.; Xie, X.; Liu, B. Efficacy and safety of US-guided thermal ablation for primary hyperparathyroidism: A systematic review and meta-analysis. Int. J. Hyperth. 2020, 37, 245–253. [Google Scholar] [CrossRef]
- Cao, X.J.; Zhao, Z.L.; Wei, Y.; Peng, L.L.; Li, Y.; Yu, M.A. Efficacy and safety of microwave ablation treatment for secondary hyperparathyroidism: Systematic review and meta-analysis. Int. J. Hyperth. 2020, 37, 316–323. [Google Scholar] [CrossRef]
- Zhou, X.; Shen, Y.; Zhu, Y.; Lv, Q.; Pu, W.; Gao, L.; Gu, M.; Li, C. Ultrasound-guided microwave ablation for secondary hyperparathyroidism: A systematic review and meta-analysis. Int. J. Hyperth. 2021, 38, 1285–1294. [Google Scholar] [CrossRef]
- Erturk, M.S.; Cekic, B.; Sarı, I.K.; Pamuk, B.O. Microwave ablation as an efficient therapy for primary hyperparathyroidism: Efficacy and predictors of treatment success. Int. J. Clin. Pract. 2021, 75, e14580. [Google Scholar] [CrossRef] [PubMed]
- Guo, D.M.; Chen, Z.; Zhai, Y.X.; Su, H.H. Comparison of radiofrequency ablation and microwave ablation for benign thyroid nodules: A systematic review and meta-analysis. Clin. Endocrinol. 2021, 95, 187–196. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Zhao, W.; Xia, Z.; Su, A.; Li, Z.; Zhu, J. Comparative efficacy of different ultrasound-guided ablation for the treatment of benign thyroid nodules: Systematic review and network meta-analysis of randomized controlled trials. PLoS ONE 2021, 16, e0243864. [Google Scholar] [CrossRef]
- Zheng, B.W.; Wang, J.F.; Ju, J.X.; Wu, T.; Tong, G.; Ren, J. Efficacy and safety of cooled and uncooled microwave ablation for the treatment of benign thyroid nodules: A systematic review and meta-analysis. Endocrine 2018, 62, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Ha, E.J.; Baek, J.H.; Kim, K.W.; Pyo, J.; Lee, J.H.; Baek, S.H.; Døssing, H.; Hegedüs, L. Comparative efficacy of radiofrequency and laser ablation for the treatment of benign thyroid nodules: Systematic review including traditional pooling and bayesian network meta-analysis. J. Clin. Endocrinol. Metab. 2015, 100, 1903–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, Y.; Jung, S.L. Efficacy and Safety of Thermal Ablation Techniques for the Treatment of Primary Papillary Thyroid Microcarcinoma: A Systematic Review and Meta-Analysis. Thyroid 2020, 30, 720–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suh, C.H.; Baek, J.H.; Choi, Y.J.; Lee, J.H. Efficacy and Safety of Radiofrequency and Ethanol Ablation for Treating Locally Recurrent Thyroid Cancer: A Systematic Review and Meta-Analysis. Thyroid 2016, 26, 420–428. [Google Scholar] [CrossRef]
- Tong, M.; Li, S.; Li, Y.; Li, Y.; Feng, Y.; Che, Y. Efficacy and safety of radiofrequency, microwave and laser ablation for treating papillary thyroid microcarcinoma: A systematic review and meta-analysis. Int. J. Hyperth. 2019, 36, 1278–1286. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.J.; Baek, J.H.; Chung, S.R.; Choi, Y.J.; Lee, J.H. Long-Term Results of Thermal Ablation of Benign Thyroid Nodules: A Systematic Review and Meta-Analysis. Endocrinol. Metab. 2020, 35, 339–350. [Google Scholar] [CrossRef]
- Yang, C.C.; Hsu, Y.; Liou, J.Y. Efficacy of Ethanol Ablation for Benign Thyroid Cysts and Predominantly Cystic Nodules: A Systematic Review and Meta-Analysis. Endocrinol. Metab. 2021, 36, 81–95. [Google Scholar] [CrossRef]
- Wei, Y.; Peng, C.Z.; Wang, S.R.; He, J.F.; Peng, L.L.; Zhao, Z.L.; Cao, X.J.; Li, Y.; Yu, M.A. Effectiveness and Safety of Thermal Ablation in the Treatment of Primary Hyperparathyroidism: A Multicenter Study. J. Clin. Endocrinol. Metab. 2021, 106, 2707–2717. [Google Scholar] [CrossRef] [PubMed]
- Hussain, I.; Ahmad, S.; Aljammal, J. Radiofrequency Ablation of Parathyroid Adenoma: A Novel Treatment Option for Primary Hyperparathyroidism. AACE Clin. Case Rep. 2021, 7, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Ha, E.J.; Baek, J.H.; Lee, J.H. The efficacy and complications of radiofrequency ablation of thyroid nodules. Curr. Opin. Endocrinol. Diabetes Obes. 2011, 18, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Tourinho-Barbosa, R.R.; Batista, L.T.; Cathelineau, X.; Sanchez-Macias, J.; Sanchez-Salas, R. Ablative options for prostate cancer management. Turk J. Urol. 2021, 47, S49–S55. [Google Scholar] [CrossRef]
- Linares-Espinós, E.; Carneiro, A.; Martínez-Salamanca, J.I.; Bianco, F.; Castro-Alfaro, A.; Cathelineau, X.; Valerio, M.; Sanchez-Salas, R. New technologies and techniques for prostate cancer focal therapy. Minerva Urol. Nefrol. 2018, 70, 252–263. [Google Scholar] [CrossRef]
- Natarajan, S.; Raman, S.; Priester, A.M.; Garritano, J.; Margolis, D.J.; Lieu, P.; Macairan, M.L.; Huang, J.; Grundfest, W.; Marks, L.S. Focal Laser Ablation of Prostate Cancer: Phase I Clinical Trial. J. Urol. 2016, 196, 68–75. [Google Scholar] [CrossRef]
- Walser, E.; Nance, A.; Ynalvez, L.; Yong, S.; Aoughsten, J.S.; Eyzaguirre, E.J.; Williams, S.B. Focal Laser Ablation of Prostate Cancer: Results in 120 Patients with Low- to Intermediate-Risk Disease. J. Vasc. Interv. Radiol. 2019, 30, 401–409.e402. [Google Scholar] [CrossRef]
- Huber, P.M.; Afzal, N.; Arya, M.; Boxler, S.; Dudderidge, T.; Emberton, M.; Guillaumier, S.; Hindley, R.G.; Hosking-Jervis, F.; Leemann, L.; et al. Focal HIFU therapy for anterior compared to posterior prostate cancer lesions. World J. Urol. 2021, 39, 1115–1119. [Google Scholar] [CrossRef]
- van Velthoven, R.; Aoun, F.; Marcelis, Q.; Albisinni, S.; Zanaty, M.; Lemort, M.; Peltier, A.; Limani, K. A prospective clinical trial of HIFU hemiablation for clinically localized prostate cancer. Prostate Cancer Prostatic. Dis. 2016, 19, 79–83. [Google Scholar] [CrossRef]
- Bass, E.J.; Ahmed, H.U. Focal therapy in prostate cancer: A review of seven common controversies. Cancer Treat. Rev. 2016, 51, 27–34. [Google Scholar] [CrossRef]
- Connor, M.J.; Gorin, M.A.; Ahmed, H.U.; Nigam, R. Focal therapy for localized prostate cancer in the era of routine multi-parametric MRI. Prostate Cancer Prostatic Dis. 2020, 23, 232–243. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef]
- Rakauskas, A.; Marra, G.; Heidegger, I.; Kasivisvanathan, V.; Kretschmer, A.; Zattoni, F.; Preisser, F.; Tilki, D.; Tsaur, I.; van den Bergh, R.; et al. Focal Therapy for Prostate Cancer: Complications and Their Treatment. Front Surg. 2021, 8, 696242. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Siegel, R.L.; Jemal, A. Lung Cancer Statistics. Adv. Exp. Med. Biol. 2016, 893, 1–19. [Google Scholar] [CrossRef]
- Mazzone, P. Preoperative evaluation of the lung resection candidate. Clevel. Clin. J. Med. 2012, 79, S17–S22. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.; Eiken, P.; Blackmon, S. Image guided thermal ablation in lung cancer treatment. J. Thorac. Dis. 2020, 12, 7039–7047. [Google Scholar] [CrossRef]
- Chi, J.; Ding, M.; Shi, Y.; Wang, T.; Cui, D.; Tang, X.; Li, P.; Zhai, B. Comparison study of computed tomography-guided radiofrequency and microwave ablation for pulmonary tumors: A retrospective, case-controlled observational study. Thorac. Cancer 2018, 9, 1241–1248. [Google Scholar] [CrossRef]
- Macchi, M.; Belfiore, M.P.; Floridi, C.; Serra, N.; Belfiore, G.; Carmignani, L.; Grasso, R.F.; Mazza, E.; Pusceddu, C.; Brunese, L.; et al. Radiofrequency versus microwave ablation for treatment of the lung tumours: LUMIRA (lung microwave radiofrequency) randomized trial. Med. Oncol. 2017, 34, 96. [Google Scholar] [CrossRef]
- Bi, N.; Shedden, K.; Zheng, X.; Kong, F.S. Comparison of the Effectiveness of Radiofrequency Ablation With Stereotactic Body Radiation Therapy in Inoperable Stage I Non-Small Cell Lung Cancer: A Systemic Review and Pooled Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 1378–1390. [Google Scholar] [CrossRef] [Green Version]
- Jiang, B.; McClure, M.A.; Chen, T.; Chen, S. Efficacy and safety of thermal ablation of lung malignancies: A Network meta-analysis. Ann. Thorac. Med. 2018, 13, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Z.; Wang, Y.; Zhang, J.; Zheng, J.; Li, W. A Meta-Analysis of Clinical Outcomes After Radiofrequency Ablation and Microwave Ablation for Lung Cancer and Pulmonary Metastases. J. Am. Coll. Radiol. 2019, 16, 302–314. [Google Scholar] [CrossRef] [PubMed]
- Hiraki, T.; Gobara, H.; Fujiwara, H.; Ishii, H.; Tomita, K.; Uka, M.; Makimoto, S.; Kanazawa, S. Lung Cancer Ablation: Complications. Semin. Interv. Radiol. 2013, 30, 169–175. [Google Scholar]
- Kashima, M.; Yamakado, K.; Takaki, H.; Kodama, H.; Yamada, T.; Uraki, J.; Nakatsuka, A. Complications after 1000 lung radiofrequency ablation sessions in 420 patients: A single center’s experiences. AJR Am. J. Roentgenol. 2011, 197, W576–W580. [Google Scholar] [CrossRef]
- Zheng, A.; Wang, X.; Yang, X.; Wang, W.; Huang, G.; Gai, Y.; Ye, X. Major complications after lung microwave ablation: A single-center experience on 204 sessions. Ann. Thorac. Surg. 2014, 98, 243–248. [Google Scholar] [CrossRef]
- Vyas, V.; Paul, M. Catastrophic complications following cryoablation of lung cancer. Bayl. Univ. Med Cent. Proc. 2020, 34, 131–132. [Google Scholar] [CrossRef]
- Li, S.; Peng, Y.; Weinhandl, E.D.; Blaes, A.H.; Cetin, K.; Chia, V.M.; Stryker, S.; Pinzone, J.J.; Acquavella, J.F.; Arneson, T.J. Estimated number of prevalent cases of metastatic bone disease in the US adult population. Clin. Epidemiol. 2012, 4, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Cazzato, R.L.; Arrigoni, F.; Boatta, E.; Bruno, F.; Chiang, J.B.; Garnon, J.; Zugaro, L.; Giordano, A.V.; Carducci, S.; Varrassi, M.; et al. Percutaneous management of bone metastases: State of the art, interventional strategies and joint position statement of the Italian College of MSK Radiology (ICoMSKR) and the Italian College of Interventional Radiology (ICIR). Radiol. Med. 2019, 124, 34–49. [Google Scholar] [CrossRef]
- Gangi, A.; Tsoumakidou, G.; Buy, X.; Quoix, E. Quality improvement guidelines for bone tumour management. Cardiovasc. Interv. Radiol. 2010, 33, 706–713. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.H.; Xiao, L.F.; Yan, F.F.; Chen, S.L.; Zhang, C.; Lei, J.; Deng, Z.M. Use of percutaneous microwave ablation for the treatment of bone tumors: A retrospective study of clinical outcomes in 47 patients. Cancer Imaging 2019, 19, 87. [Google Scholar] [CrossRef] [Green Version]
- Koo, J.S.; Chung, S.H. The Efficacy of Radiofrequency Ablation for Bone Tumors Unsuitable for Radical Excision. Clin. Orthop. Surg. 2021, 13, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Gennaro, N.; Sconfienza, L.M.; Ambrogi, F.; Boveri, S.; Lanza, E. Thermal ablation to relieve pain from metastatic bone disease: A systematic review. Skelet. Radiol. 2019, 48, 1161–1169. [Google Scholar] [CrossRef] [PubMed]
- Rehnitz, C.; Sprengel, S.D.; Lehner, B.; Ludwig, K.; Omlor, G.; Merle, C.; Kauczor, H.U.; Ewerbeck, V.; Weber, M.A. CT-guided radiofrequency ablation of osteoid osteoma and osteoblastoma: Clinical success and long-term follow up in 77 patients. Eur. J. Radiol. 2012, 81, 3426–3434. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, M.; Arai, Y.; Myoui, A.; Gobara, H.; Sone, M.; Rosenthal, D.I.; Tsushima, Y.; Kanazawa, S.; Ehara, S.; Endo, K. Phase I/II Multi-Institutional Study of Percutaneous Radiofrequency Ablation for Painful Osteoid Osteoma (JIVROSG-0704). Cardiovasc. Interv. Radiol. 2016, 39, 1464–1470. [Google Scholar] [CrossRef]
- Tanigawa, N.; Arai, Y.; Yamakado, K.; Aramaki, T.; Inaba, Y.; Kanazawa, S.; Matsui, O.; Miyazaki, M.; Kodama, Y.; Anai, H.; et al. Phase I/II Study of Radiofrequency Ablation for Painful Bone Metastases: Japan Interventional Radiology in Oncology Study Group 0208. Cardiovasc. Interv. Radiol. 2018, 41, 1043–1048. [Google Scholar] [CrossRef]
- Goetz, M.P.; Callstrom, M.R.; Charboneau, J.W.; Farrell, M.A.; Maus, T.P.; Welch, T.J.; Wong, G.Y.; Sloan, J.A.; Novotny, P.J.; Petersen, I.A.; et al. Percutaneous image-guided radiofrequency ablation of painful metastases involving bone: A multicenter study. J. Clin. Oncol. 2004, 22, 300–306. [Google Scholar] [CrossRef]
- Cazzato, R.L.; Garnon, J.; Caudrelier, J.; Rao, P.P.; Koch, G.; Gangi, A. Percutaneous radiofrequency ablation of painful spinal metastasis: A systematic literature assessment of analgesia and safety. Int. J. Hyperth. 2018, 34, 1272–1281. [Google Scholar] [CrossRef]
- Callstrom, M.R.; Dupuy, D.E.; Solomon, S.B.; Beres, R.A.; Littrup, P.J.; Davis, K.W.; Paz-Fumagalli, R.; Hoffman, C.; Atwell, T.D.; Charboneau, J.W.; et al. Percutaneous image-guided cryoablation of painful metastases involving bone: Multicenter trial. Cancer 2013, 119, 1033–1041. [Google Scholar] [CrossRef] [Green Version]
- Santiago, E.; Pauly, V.; Brun, G.; Guenoun, D.; Champsaur, P.; Le Corroller, T. Percutaneous cryoablation for the treatment of osteoid osteoma in the adult population. Eur. Radiol. 2018, 28, 2336–2344. [Google Scholar] [CrossRef]
- Whitmore, M.J.; Hawkins, C.M.; Prologo, J.D.; Marshall, K.W.; Fabregas, J.A.; Yim, D.B.; Monson, D.; Oskouei, S.V.; Fletcher, N.D.; Williams, R.S. Cryoablation of Osteoid Osteoma in the Pediatric and Adolescent Population. J. Vasc. Interv. Radiol. 2016, 27, 232–237. [Google Scholar] [CrossRef]
- Cazzato, R.L.; de Rubeis, G.; de Marini, P.; Dalili, D.; Koch, G.; Auloge, P.; Garnon, J.; Gangi, A. Percutaneous microwave ablation of bone tumors: A systematic review. Eur. Radiol. 2021, 31, 3530–3541. [Google Scholar] [CrossRef] [PubMed]
- Dalili, D.; Isaac, A.; Bazzocchi, A.; Åström, G.; Bergh, J.; Lalam, R.; Weber, M.A.; Fritz, J.; Mansour, R. Interventional Techniques for Bone and Musculoskeletal Soft Tissue Tumors: Current Practices and Future Directions—Part I. Ablation. Semin. Musculoskelet. Radiol. 2020, 24, 692–709. [Google Scholar] [CrossRef] [PubMed]
- Deib, G.; Deldar, B.; Hui, F.; Barr, J.S.; Khan, M.A. Percutaneous Microwave Ablation and Cementoplasty: Clinical Utility in the Treatment of Painful Extraspinal Osseous Metastatic Disease and Myeloma. AJR Am. J. Roentgenol. 2019, 212, 1377–1384. [Google Scholar] [CrossRef] [PubMed]
- Cazzato, R.L.; Palussière, J.; Auloge, P.; Rousseau, C.; Koch, G.; Dalili, D.; Buy, X.; Garnon, J.; De Marini, P.; Gangi, A. Complications Following Percutaneous Image-guided Radiofrequency Ablation of Bone Tumors: A 10-year Dual-Center Experience. Radiology 2020, 296, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Kurup, A.N.; Schmit, G.D.; Morris, J.M.; Atwell, T.D.; Schmitz, J.J.; Weisbrod, A.J.; Woodrum, D.A.; Eiken, P.W.; Callstrom, M.R. Avoiding Complications in Bone and Soft Tissue Ablation. Cardiovasc. Interv. Radiol. 2017, 40, 166–176. [Google Scholar] [CrossRef]
- Foster, R.C.; Stavas, J.M. Bone and soft tissue ablation. Semin. Interv. Radiol. 2014, 31, 167–179. [Google Scholar] [CrossRef] [Green Version]
- Kurtz, J.E.; Buy, X.; Deschamps, F.; Sauleau, E.; Bouhamama, A.; Toulmonde, M.; Honoré, C.; Bertucci, F.; Brahmi, M.; Chevreau, C.; et al. CRYODESMO-O1: A prospective, open phase II study of cryoablation in desmoid tumour patients progressing after medical treatment. Eur. J. Cancer 2021, 143, 78–87. [Google Scholar] [CrossRef]
- Thompson, S.M.; Callstrom, M.R.; McKusick, M.A.; Woodrum, D.A. Initial Results of Image-Guided Percutaneous Ablation as Second-Line Treatment for Symptomatic Vascular Anomalies. Cardiovasc. Interv. Radiol. 2015, 38, 1171–1178. [Google Scholar] [CrossRef] [Green Version]
- Lane, M.D.; Le, H.B.; Lee, S.; Young, C.; Heran, M.K.; Badii, M.; Clarkson, P.W.; Munk, P.L. Combination radiofrequency ablation and cementoplasty for palliative treatment of painful neoplastic bone metastasis: Experience with 53 treated lesions in 36 patients. Skelet. Radiol. 2011, 40, 25–32. [Google Scholar] [CrossRef]
- de Baere, T.; Tselikas, L.; Gravel, G.; Hakime, A.; Deschamps, F.; Honoré, C.; Mir, O.; Lecesne, A. Interventional radiology: Role in the treatment of sarcomas. Eur. J. Cancer 2018, 94, 148–155. [Google Scholar] [CrossRef]
- Nakamura, T.; Matsumine, A.; Yamakado, K.; Matsubara, T.; Takaki, H.; Nakatsuka, A.; Takeda, K.; Abo, D.; Shimizu, T.; Uchida, A. Lung radiofrequency ablation in patients with pulmonary metastases from musculoskeletal sarcomas. Cancer 2009, 115, 3774–3781. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Iguchi, T.; Hiraki, T.; Gobara, H.; Fujiwara, H.; Sakurai, J.; Matsui, Y.; Mitsuhashi, T.; Soh, J.; Toyooka, S.; et al. Radiofrequency ablation of pulmonary metastases from sarcoma: Single-center retrospective evaluation of 46 patients. Jpn. J. Radiol. 2017, 35, 61–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palussière, J.; Italiano, A.; Descat, E.; Ferron, S.; Cornélis, F.; Avril, A.; Brouste, V.; Bui, B.N. Sarcoma lung metastases treated with percutaneous radiofrequency ablation: Results from 29 patients. Ann. Surg. Oncol. 2011, 18, 3771–3777. [Google Scholar] [CrossRef] [PubMed]
- Grilley-Olson, J.E.; Webber, N.P.; Demos, D.S.; Christensen, J.D.; Kirsch, D.G. Multidisciplinary Management of Oligometastatic Soft Tissue Sarcoma. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 939–948. [Google Scholar] [CrossRef] [PubMed]
- Ghanouni, P.; Dobrotwir, A.; Bazzocchi, A.; Bucknor, M.; Bitton, R.; Rosenberg, J.; Telischak, K.; Busacca, M.; Ferrari, S.; Albisinni, U.; et al. Magnetic resonance-guided focused ultrasound treatment of extra-abdominal desmoid tumors: A retrospective multicenter study. Eur. Radiol. 2017, 27, 732–740. [Google Scholar] [CrossRef] [Green Version]
















| Ablation Device | Advantages | Disadvantages |
|---|---|---|
| Ethanol |
|
|
| RFA |
|
|
| Cryoablation |
|
|
| MWA |
|
|
| Laser |
|
|
| IRE |
|
|
| HIFU |
|
|
| Histotripsy |
|
|
| Authors | Study Type | Inclusion Years | Sample Size | Comparison | Cancer | Findings |
|---|---|---|---|---|---|---|
| Chi et al. [172] | Retrospective Cohort + Meta-analysis | 2003–2018 | 590 | RFA vs. MWA | Primary and metastatic lung tumors | No significant difference in complication rates, complete ablation rates, median progression-free and overall survival |
| Macchi et al. [173] | RCT | N/A | 52 | RFA vs. MWA | Stage IV lung cancer | No significant difference in survival. MWA had significantly lower pain levels and a greater tumor size reduction |
| Bi et al. [174] | Meta-analysis | 2004–2012 | 3095 | RFA vs. SBRT | Stage I NSCLC | SBRT had significantly higher local tumor control rates. Comparable overall survival |
| Jiang et al. [175] | Meta-analysis | 2004–2017 | 1840 | RFA vs. MWA vs. cryoablation | Primary and metastatic tumors | RFA and MWA are more effective at controlling local progression rate than cryoablation. Comparable safety profiles across all three. |
| Yuan et al. [176] | Meta-analysis | 2010–2017 | 3432 | RFA vs. MWA | Primary and metastatic tumors | 1–5 year overall survival higher in RFA. No significant difference in median local tumor progression free survival, complete ablation rates, and adverse events. RFA had higher median survival in metastatic tumors. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mansur, A.; Garg, T.; Shrigiriwar, A.; Etezadi, V.; Georgiades, C.; Habibollahi, P.; Huber, T.C.; Camacho, J.C.; Nour, S.G.; Sag, A.A.; et al. Image-Guided Percutaneous Ablation for Primary and Metastatic Tumors. Diagnostics 2022, 12, 1300. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12061300
Mansur A, Garg T, Shrigiriwar A, Etezadi V, Georgiades C, Habibollahi P, Huber TC, Camacho JC, Nour SG, Sag AA, et al. Image-Guided Percutaneous Ablation for Primary and Metastatic Tumors. Diagnostics. 2022; 12(6):1300. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12061300
Chicago/Turabian StyleMansur, Arian, Tushar Garg, Apurva Shrigiriwar, Vahid Etezadi, Christos Georgiades, Peiman Habibollahi, Timothy C. Huber, Juan C. Camacho, Sherif G. Nour, Alan Alper Sag, and et al. 2022. "Image-Guided Percutaneous Ablation for Primary and Metastatic Tumors" Diagnostics 12, no. 6: 1300. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12061300