Increased Heschl’s Gyrus Duplication in Schizophrenia Spectrum Disorders: A Cross-Sectional MRI Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. MRI Procedure
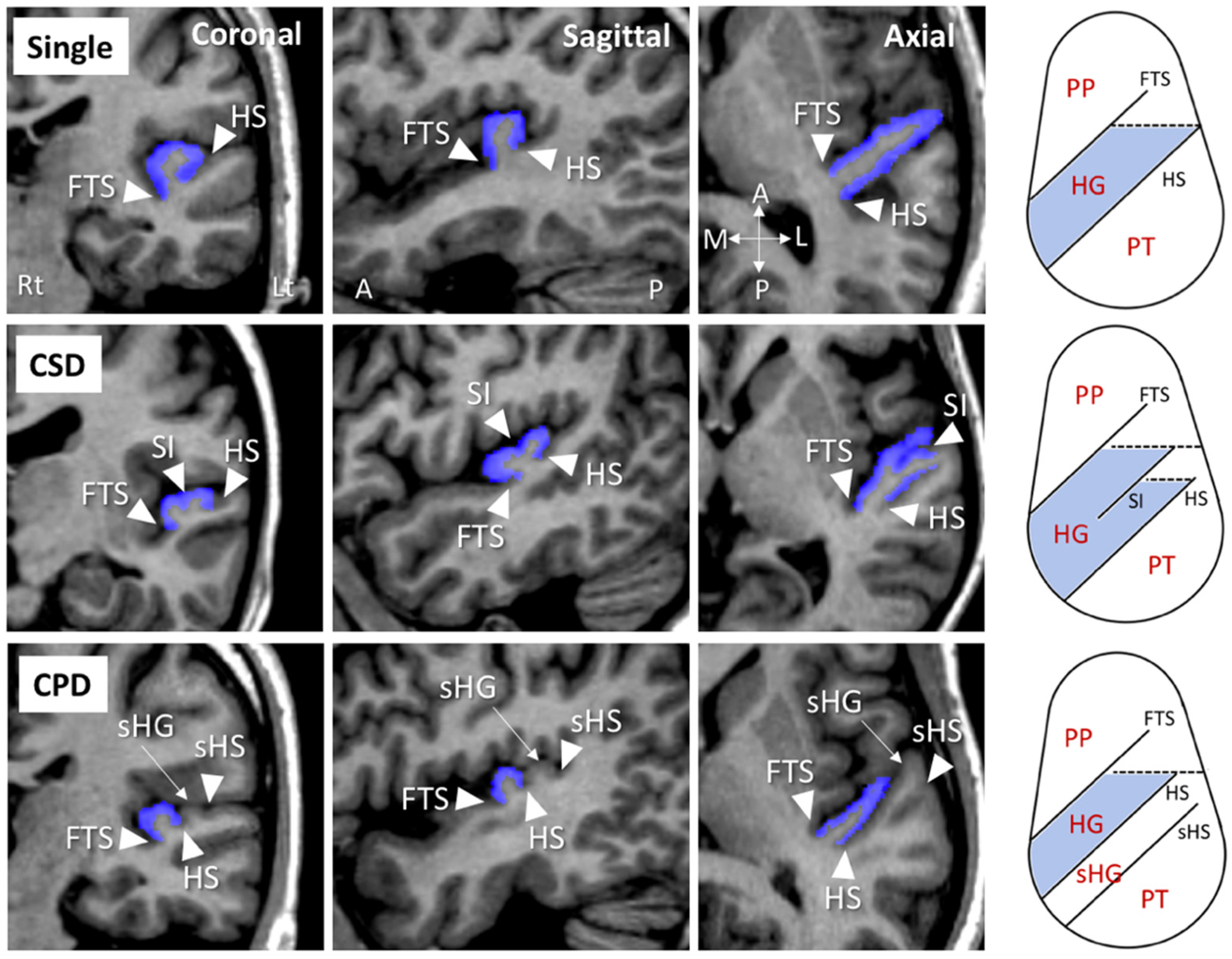
2.3. Assessment of HG Gyrification Patterns
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
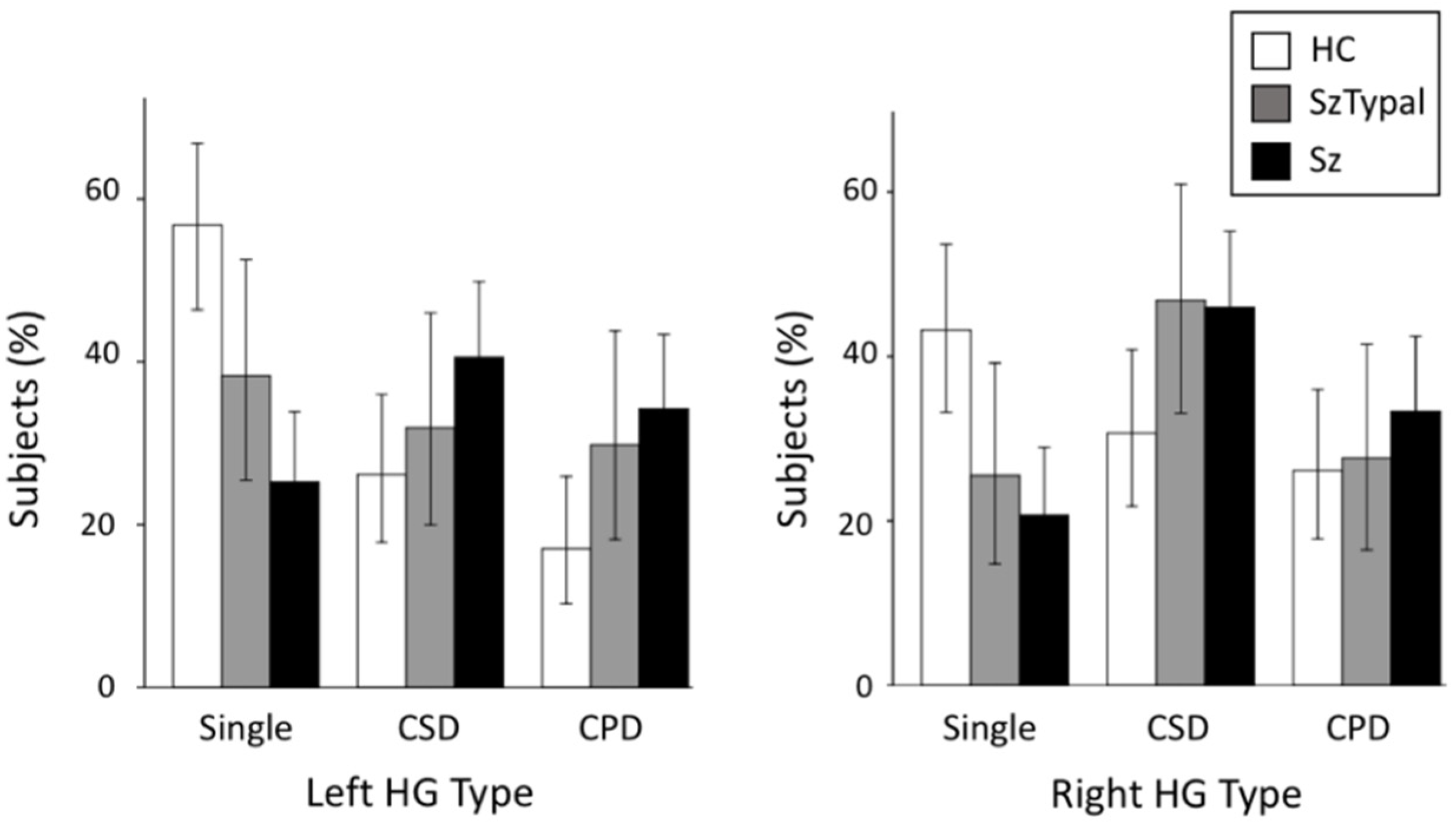
3.2. HG Pattern Distributions
3.3. Relationship between the HG Pattern and Clinical Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Da Costa, S.; van der Zwaag, W.; Marques, J.P.; Frackowiak, R.S.; Clarke, S.; Saenz, M. Human primary auditory cortex follows the shape of Heschl’s gyrus. J. Neurosci. 2011, 31, 14067–14075. [Google Scholar] [CrossRef]
- Rademacher, J.; Morosan, P.; Schormann, T.; A Schleicher, A.; Werner, C.; Freund, H.J.; Zilles, K. Probabilistic mapping and volume measurement of human primary auditory cortex. Neuroimage 2001, 13, 669–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdul-Kareem, I.A.; Sluming, V. Heschl gyrus and its included primary auditory cortex: Structural MRI studies in healthy and diseased subjects. J. Magn. Reson. Imaging 2008, 28, 287–299. [Google Scholar] [CrossRef] [PubMed]
- Leonard, C.M.; Puranik, C.; Kuldau, J.M.; Lombardino, L.J. Normal variation in the frequency and location of human auditory cortex landmarks. Heschl’s gyrus: Where is it? Cereb. Cortex 1998, 8, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Marie, D.; Jobard, G.; Crivello, F.; Perchey, G.; Petit, L.; Mellet, E.; Joliot, M.; Zago, L.; Mazoyer, B.; Tzourio-Mazoyer, N. Descriptive anatomy of Heschl’s gyri in 430 healthy volunteers, including 198 left-handers. Brain Struct. Funct. 2015, 220, 729–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, E.; Schleicher, A.; Omran, H.; Curtis, M.; Zilles, K. The ontogeny of human gyrification. Cereb. Cortex 1995, 5, 56–63. [Google Scholar] [CrossRef]
- Chi, J.G.; Dooling, E.C.; Gilles, F.H. Gyral development of the human brain. Ann. Neurol. 1977, 1, 86–93. [Google Scholar] [CrossRef]
- Tzourio-Mazoyer, N.; Marie, D.; Zago, L.; Jobard, G.; Perchey, G.; Leroux, G.; Mellet, E.; Joliot, M.; Crivello, F.; Petit, L.; et al. Heschl’s gyrification pattern is related to speech-listening hemispheric lateralization: FMRI investigation in 281 healthy volunteers. Brain Struct. Funct. 2015, 220, 1585–1599. [Google Scholar] [CrossRef]
- Insel, T.R. Rethinking schizophrenia. Nature 2010, 468, 187–193. [Google Scholar] [CrossRef] [Green Version]
- Weinberger, D.R. Implications of normal brain development for the pathogenesis of schizophrenia. Arch. Gen. Psychiatry 1987, 44, 660–669. [Google Scholar] [CrossRef]
- Mwansisya, T.E.; Hu, A.; Li, Y.; Chen, X.; Wu, G.; Huang, X.; Lv, D.; Li, Z.; Liu, C.; Xue, Z.; et al. Task and resting-state fMRI studies in first-episode schizophrenia: A systematic review. Schizophr. Res. 2017, 189, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Guo, Q.; Tang, Y.; Li, H.; Zhang, T.; Li, J.; Sheng, J.; Liu, D.; Li, C.; Wang, J. Both volumetry and functional connectivity of Heschl’s gyrus are associated with auditory P300 in first episode schizophrenia. Schizophr. Res. 2014, 160, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Liang, S.; Pu, W.; Song, Y.; Mwansisya, T.E.; Yang, Q.; Liu, H.; Shan, B.; Xue, Z. Reduced cortical thickness in right Heschl’s gyrus associated with auditory verbal hallucinations severity in first-episode schizophrenia. BMC Psychiatry 2015, 15, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, T.; Sasabayashi, D.; Takayanagi, Y.; Furuichi, A.; Kido, M.; Nakamura, M.; Pham, T.V.; Kobayashi, H.; Noguchi, K.; Suzuki, M. Altered Heschl’s gyrus duplication pattern in first-episode schizophrenia. Schizophr Res. 2021. under review. [Google Scholar]
- Hubl, D.; Dougoud-Chauvin, V.; Zeller, M.; Federspiel, A.; Boesch, C.; Strik, W.; Dierks, T.; Koenig, T. Structural analysis of Heschl’s gyrus in schizophrenia patients with auditory hallucinations. Neuropsychobiology 2010, 61, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Suzuki, M. Brain morphologic changes in early stages of psychosis: Implications for clinical application and early intervention. Psychiatry Clin. Neurosci. 2018, 72, 556–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association Press: Washington, DC, USA, 1994. [Google Scholar]
- Siever, L.J.; Kalus, O.F.; Keefe, R.S.E. The boundaries of schizophrenia. Psychiatr. Clin. N. Am. 1993, 16, 217–244. [Google Scholar] [CrossRef]
- Siever, L.J.; Davis, K.L. The pathophysiology of schizophrenia disorders: Perspective from the spectrum. Am. J. Psychiatry 2004, 161, 398–413. [Google Scholar] [CrossRef]
- Zilles, K.; Palomero-Gallagher, N.; Amunts, K. Development of cortical folding during evolution and ontogeny. Trends Neurosci. 2013, 36, 275–284. [Google Scholar] [CrossRef]
- Sasabayashi, D.; Takayanagi, Y.; Nishiyama, S.; Takahashi, T.; Furuichi, A.; Kido, M.; Nishikawa, Y.; Nakamura, M.; Noguchi, K.; Suzuki, M. Increased frontal gyrification negatively correlates with executive function in patients with first-episode schizophrenia. Cereb. Cortex 2017, 27, 2686–2694. [Google Scholar] [CrossRef] [Green Version]
- Sasabayashi, D.; Takayanagi, Y.; Takahashi, T.; Nemoto, K.; Furuichi, A.; Kido, M.; Nishikawa, Y.; Nakamura, M.; Noguchi, K.; Suzuki, M. Increased brain gyrification in the schizophrenia spectrum. Psychiatry Clin. Neurosci. 2020, 74, 70–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oertel-Knöchel, V.; Knöchel, C.; Matura, S.; Stäblein, M.; Prvulovic, D.; Maurer, K.; Linden, D.E.; van de Ven, V. Association between symptoms of psychosis and reduced functional connectivity of auditory cortex. Schizophr. Res. 2014, 160, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Shinn, A.K.; Baker, J.T.; Cohen, B.M.; Ongür, D. Functional connectivity of left Heschl’s gyrus in vulnerability to auditory hallucinations in schizophrenia. Schizophr. Res. 2013, 143, 260–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Hu, N.; Zhang, W.; Tao, B.; Dai, J.; Gong, Y.; Tan, Y.; Cai, D.; Lui, S. Dysconnectivity of multiple brain networks in schizophrenia: A meta-analysis of resting-state functional connectivity. Front. Psychiatry 2019, 10, 482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Q.; Shen, J.; Wu, J.; Yu, X.; Lou, W.; Fan, H.; Shi, L.; Wang, D. Altered default mode network functional connectivity in schizotypal personality disorder. Schizophr. Res. 2014, 160, 51–56. [Google Scholar] [CrossRef]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Andreasen, N.C.; Okazaki, Y.; Kitamura, T.; Anzai, N.; Shima, S.; Ohta, T. The Comprehensive Assessment of Symptoms and History (CASH): An Instrument for Assessing Diagnosis and Psychopathology; Seiwa Shoten Publishers: Tokyo, Japan, 1995. (In Japanese) [Google Scholar]
- Andreasen, N.C.; Okazaki, Y.; Anzai, N.; Ohta, T.; Shima, S.; Kitamura, T. The Japanese version of Scale for the Assessment of Negative Symptoms (SANS). Jpn. J. Clin. Psychiatry 1984, 13, 999–1010. (In Japanese) [Google Scholar]
- Andreasen, N.C.; Okazaki, Y.; Kitamura, T.; Anzai, N.; Ohta, T.; Shima, S.; McDonald-Scott, P. Scale for the Assessment of Positive Symptoms (SAPS). Arch. Psychiatr. Diag. Clin. Eval. 1992, 3, 365–377. (In Japanese) [Google Scholar]
- Kawasaki, Y.; Suzuki, M.; Nohara, S.; Hagino, H.; Matsui, M.; Yamashita, I.; Takahashi, T.; Chitnis, X.; McGuire, P.K.; Seto, H.; et al. Structural brain differences in patients with schizotypal disorder and schizophrenia demonstrated by voxel-based morphometry. Eur. Arch. Psychiatry Clin. Neurosci. 2004, 254, 406–414. [Google Scholar] [CrossRef]
- Suzuki, M.; Zhou, S.-Y.; Takahashi, T.; Hagino, H.; Kawasaki, Y.; Niu, L.; Matsui, M.; Seto, H.; Kurachi, M. Differential contributions of prefrontal and temporolimbic pathology to mechanisms of psychosis. Brain 2005, 128, 2109–2122. [Google Scholar] [CrossRef]
- Nordentoft, M.; Thorup, A.; Petersen, L.; Øhlenschlæger, J.; Melau, M.; Christensen, T.Ø.; Krarup, G. Transition rates from schizotypal disorder to psychotic disorder for first-contact patients included in the OPUS trial. A randomized clinical trial of integrated treatment and standard treatment. Schizophr. Res. 2006, 83, 29–40. [Google Scholar] [CrossRef]
- Takahashi, T.; Suzuki, M.; Tsunoda, M.; Kawamura, Y.; Takahashi, N.; Maeno, N.; Kawasaki, Y.; Zhou, S.Y.; Hagino, H.; Niu, L.; et al. The association of genotypic combination of the DRD3 and BDNF polymorphisms on the adhesio interthalamica and medial temporal lobe structures. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 1236–1342. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Wood, S.J.; Yung, A.R.; Soulsby, B.; McGorry, P.D.; Suzuki, M.; Kawasaki, Y.; Phillips, L.J.; Velakoulis, D.; Pantelis, C. Progressive gray matter reduction of the superior temporal gyrus during transition to psychosis. Arch. Gen. Psychiatry 2009, 66, 366–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, T.; Suzuki, M.; Zhou, S.Y.; Tanino, R.; Nakamura, K.; Kawasaki, Y.; Seto, H.; Kurachi, M. A follow-up MRI study of the superior temporal subregions in schizotypal disorder and first-episode schizophrenia. Schizophr. Res. 2010, 119, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Takahashi, T.; Takayanagi, Y.; Sasabayashi, D.; Katagiri, N.; Sakuma, A.; Obara, C.; Koike, S.; Yamasue, H.; Furuichi, A.; et al. Surface morphology of the orbitofrontal cortex in individuals at risk of psychosis. Eur. Arch. Psychiatry Clin. Neurosci. 2019, 269, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Sasabayashi, D.; Takayanagi, Y.; Takahashi, T.; Koike, S.; Yamasue, H.; Katagiri, N.; Sakuma, A.; Obara, C.; Nakamura, M.; Furuichi, A.; et al. Increased occipital gyrification and development of psychotic disorders in individuals with an at-risk mental state: A multicenter study. Biol. Psychiatry 2017, 82, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Suzuki, M.; Zhou, S.Y.; Nakamura, K.; Tanino, R.; Kawasaki, Y.; Seal, M.L.; Seto, H.; Kurachi, M. Prevalence and length of the adhesio interthalamica in schizophrenia spectrum disorders. Psychiatry Res. 2008, 164, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Trzesniak, C.; Kempton, M.J.; Busatto, G.F.; de Oliveira, I.R.; Galvão-de Almeida, A.; Kambeitz, J.; Ferrari, M.C.; Filho, A.S.; Chagas, M.H.; Zuardi, A.W.; et al. Adhesio interthalamica alterations in schizophrenia spectrum disorders: A systematic review and meta-analysis. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 877–886. [Google Scholar] [CrossRef]
- Nishikawa, Y.; Takahashi, T.; Takayanagi, Y.; Furuichi, A.; Kido, M.; Nakamura, M.; Sasabayashi, D.; Noguchi, K.; Suzuki, M. Orbitofrontal sulcogyral pattern and olfactory sulcus depth in the schizophrenia spectrum. Eur. Arch. Psychiatry Clin. Neurosci. 2016, 266, 15–23. [Google Scholar] [CrossRef]
- Fervaha, G.; Remington, G. Neuroimaging findings in schizotypal personality disorder: A systematic review. Prog. Neuropsychopharmacol. Biol. Psychiatry 2013, 43, 96–107. [Google Scholar] [CrossRef]
- Lener, M.S.; Wong, E.; Tang, C.Y.; Byne, W.; Goldstein, K.E.; Blair, N.J.; Haznedar, M.M.; New, A.S.; Chemerinski, E.; Chu, K.W.; et al. White matter abnormalities in schizophrenia and schizotypal personality disorder. Schizophr. Bull. 2015, 41, 300–310. [Google Scholar] [CrossRef]
- Kurachi, M. Pathogenesis of schizophrenia: Part II. Temporo-frontal two-step hypothesis. Psychiatry Clin. Neurosci. 2003, 57, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Gavrilescu, M.; Rossell, S.; Stuart, G.W.; Shea, T.L.; Innes-Brown, H.; Henshall, K.; McKay, C.; Sergejew, A.A.; Copolov, D.; Egan, G.F. Reduced connectivity of the auditory cortex in patients with auditory hallucinations: A resting state functional magnetic resonance imaging study. Psychol. Med. 2010, 40, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- Leonard, C.M.; Eckert, M.A.; Lombardino, L.J.; Oakland, T.; Kranzler, J.; Mohr, C.M.; King, W.M.; Freeman, A. Anatomical risk factors for phonological dyslexia. Cereb. Cortex 2001, 11, 148–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benner, J.; Wengenroth, M.; Reinhardt, J.; Stippich, C.; Schneider, P.; Blatow, M. Prevalence and function of Heschl’s gyrus morphotypes in musicians. Brain Struct. Funct. 2017, 222, 3587–3603. [Google Scholar] [CrossRef] [PubMed]
- Golestani, N.; Price, C.J.; Scott, S.K. Born with an ear for dialects? Structural plasticity in the expert phonetician brain. J. Neurosci. 2011, 31, 4213–4220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Concina, G.; Renna, A.; Grosso, A.; Sacchetti, B. The auditory cortex and the emotional valence of sounds. Neurosci. Biobehav. Rev. 2019, 98, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, N.M. New perspectives on the auditory cortex: Learning and memory. Handb. Clin. Neurol. 2015, 129, 117–147. [Google Scholar] [CrossRef]
- Patti, M.A.; Troiani, V. Orbitofrontal sulcogyral morphology is a transdiagnostic indicator of brain dysfunction. Neuroimage Clin. 2018, 17, 910–917. [Google Scholar] [CrossRef]
- Watanabe, H.; Nakamura, M.; Ohno, T.; Itahashi, T.; Tanaka, E.; Ohta, H.; Yamada, T.; Kanai, C.; Iwanami, A.; Kato, N.; et al. Altered orbitofrontal sulcogyral patterns in adult males with high-functioning autism spectrum disorders. Soc. Cogn. Affect. Neurosci. 2014, 9, 520–528. [Google Scholar] [CrossRef]
- Sasabayashi, D.; Takahashi, T.; Takayanagi, Y.; Suzuki, M. Anomalous brain gyrification patterns in major psychiatric disorders: A systematic review and trans-diagnostic integration. Trans. Psychiatry 2021. under review. [Google Scholar]
- McGorry, P.D.; Hickie, I.B.; Yung, A.R.; Pantelis, C.; Jackson, H.J. Clinical staging of psychiatric disorders: A heuristic framework for choosing earlier, safer and more effective interventions. Aust. N. Z. J. Psychiatry 2006, 40, 616–622. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| C | SzTypal | Sz | Group Comparisons | |
|---|---|---|---|---|
| Male/female | 49/39 | 29/18 | 59/52 | Chi squared = 0.98, p = 0.613 |
| Age (years) | 24.1 ± 6.0 | 25.0 ± 5.4 | 25.8 ± 5.4 | F (2, 243) = 2.38, p = 0.095 |
| Height (cm) | 166.3 ± 7.8 | 165.9 ± 8.7 | 164.5 ± 8.0 | F (2, 243) = 1.34, p = 0.264 |
| Education (years) | 15.7 ± 3.0 | 13.1 ± 2.0 | 13.5 ± 2.0 | F (2, 243) = 26.23, p < 0.001; Sz, SzTypal < C |
| Parental education (years) 1 | 13.0 ± 2.3 | 12.3 ± 1.7 | 12.5 ± 2.0 | F (2, 234) = 1.81, p = 0.166 |
| Age of onset (years) | - | - | 22.2 ± 4.7 | - |
| Duration of illness (years) | - | - | 3.6 ± 4.1 | - |
| Dose of medication (HPD equivalent, mg/day) | - | 4.8 ± 5.7 | 10.1 ± 8.8 | F (1, 156) = 14.64, p < 0.001; SzTypal < Sz |
| Duration of medication (years) | - | 1.5 ± 3.0 | 2.7 ± 3.6 | F (1, 156) = 3.70, p = 0.056 |
| Medication type (typical/atypical/mixed) 2 | - | 14/26/0 | 40/65/4 | Fisher’s exact test, p = 0.636 |
| Total SAPS scores 3 | - | 16.0 ± 9.2 | 27.2 ± 20.9 | F (1, 147) = 11.86, p < 0.001; SzTypal < Sz |
| Total SANS scores 3 | - | 41.9 ± 21.7 | 49.8 ± 22.8 | F (1, 147) = 3.93, p = 0.049; SzTypal < Sz |
| Healthy Controls | |||||
| Right HG pattern (N (%)) | |||||
| Single | CSD | CPD | Total | ||
| Left HG pattern (N (%)) | Single | 25 (28.4) | 13 (14.8) | 12 (13.6) | 50 (56.8) |
| CSD | 8 (9.1) | 9 (10.2) | 6 (6.8) | 23 (26.1) | |
| CPD | 5 (5.7) | 5 (5.7) | 5 (5.7) | 15 (17.0) | |
| Total | 38 (43.2) | 27 (30.7) | 23 (26.1) | 88 (100.0) | |
| Schizotypal Disorder | |||||
| Right HG pattern (N (%)) | |||||
| Single | CSD | CPD | Total | ||
| Left HG pattern (N (%)) | Single | 7 (14.9) | 5 (10.6) | 6 (12.8) | 18 (38.3) |
| CSD | 2 (4.3) | 10 (21.3) | 3 (6.4) | 15 (31.9) | |
| CPD | 3 (6.4) | 7 (14.9) | 4 (8.5) | 14 (29.8) | |
| Total | 12 (25.5) | 22 (46.8) | 13 (27.7) | 47 (100.0) | |
| Schizophrenia | |||||
| Right HG pattern (N (%)) | |||||
| Single | CSD | CPD | Total | ||
| Left HG pattern (N (%)) | Single | 11 (9.9) | 11 (9.9) | 6 (5.4) | 28 (25.2) |
| CSD | 8 (7.2) | 25 (22.5) | 12 (10.8) | 45 (40.5) | |
| CPD | 4 (3.6) | 15 (13.5) | 19 (17.1) | 38 (34.2) | |
| Total | 23 (20.7) | 51 (45.9) | 37 (33.3) | 111 (100.0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takahashi, T.; Sasabayashi, D.; Takayanagi, Y.; Furuichi, A.; Kido, M.; Pham, T.V.; Kobayashi, H.; Noguchi, K.; Suzuki, M. Increased Heschl’s Gyrus Duplication in Schizophrenia Spectrum Disorders: A Cross-Sectional MRI Study. J. Pers. Med. 2021, 11, 40. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11010040
Takahashi T, Sasabayashi D, Takayanagi Y, Furuichi A, Kido M, Pham TV, Kobayashi H, Noguchi K, Suzuki M. Increased Heschl’s Gyrus Duplication in Schizophrenia Spectrum Disorders: A Cross-Sectional MRI Study. Journal of Personalized Medicine. 2021; 11(1):40. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11010040
Chicago/Turabian StyleTakahashi, Tsutomu, Daiki Sasabayashi, Yoichiro Takayanagi, Atsushi Furuichi, Mikio Kido, Tien Viet Pham, Haruko Kobayashi, Kyo Noguchi, and Michio Suzuki. 2021. "Increased Heschl’s Gyrus Duplication in Schizophrenia Spectrum Disorders: A Cross-Sectional MRI Study" Journal of Personalized Medicine 11, no. 1: 40. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11010040