An Innovative Personalised Management Program for Older Adults with Parkinson’s Disease: New Concepts and Future Directions

 , ,
, ,
Abstract
:1. Article Highlight
2. Introduction
3. What Is Known about the Subtypes of Parkinson’s Disease?
4. How Is Parkinson’s Disease Different in the Older Person?
5. Personalised Medicine for the Older Person with Parkinson’s Disease
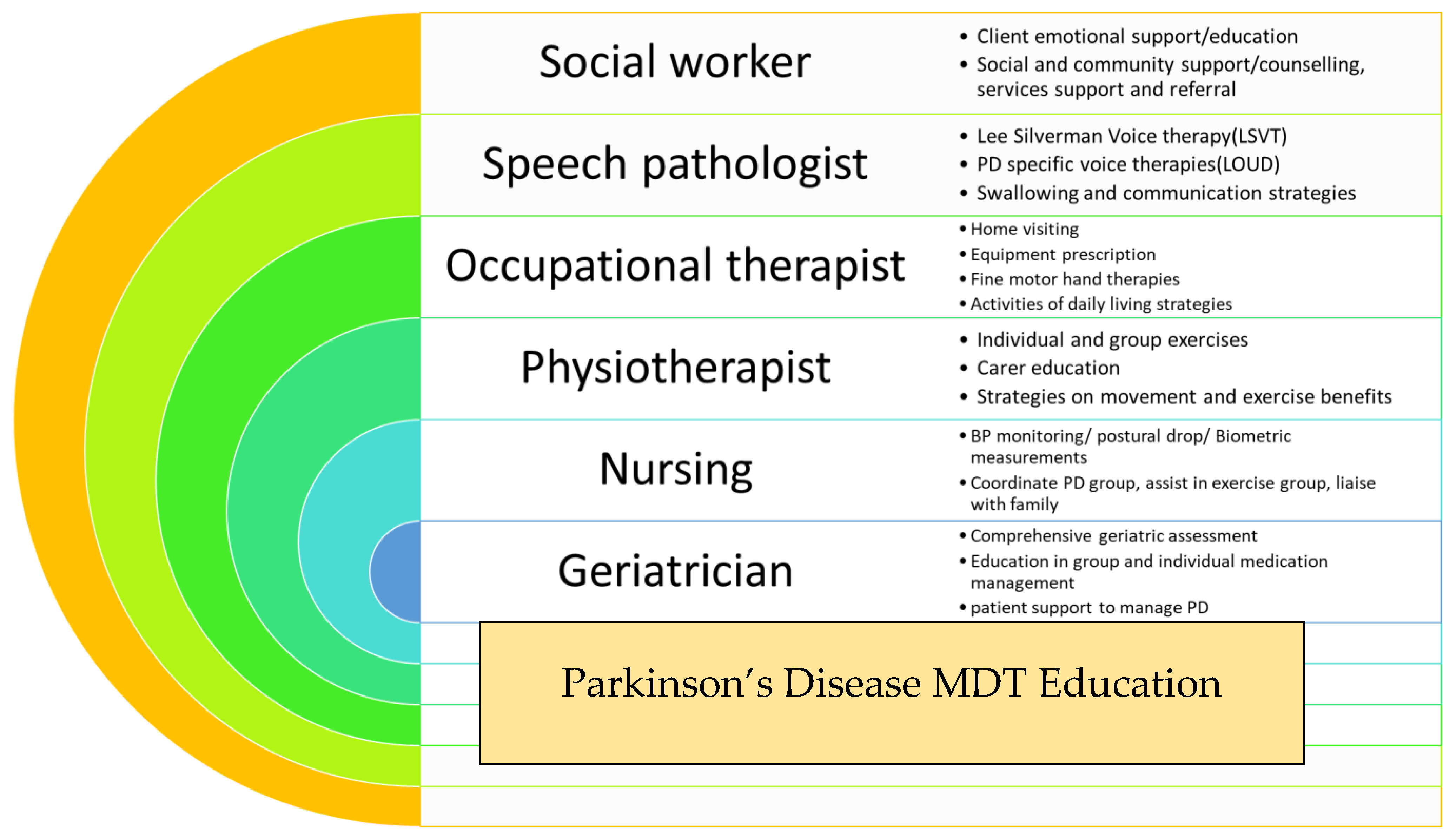
5.1. Parkinson’s Disease Multidisciplinary Education Program
5.2. Comprehensive Geriatric Assessment in the Home
5.3. Establishing an Individualised Management Plan for Older Persons with PD through Questionnaire
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Titova, N.; Padmakumar, C.; Lewis, S.J.G.; Chaudhuri, K.R. Parkinson’s: A syndrome rather than a disease? J. Neural Transm. 2017, 124, 907–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Titova, N.; Chaudhuri, K.R. Personalized Medicine and Nonmotor Symptoms in Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 134, 1257–1281. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, K.R.; Healy, D.G.; Schapira, A.H.V. Non-motor symptoms of Parkinson’s disease: Diagnosis and management. Lancet Neurol. 2006, 5, 235–245. [Google Scholar] [CrossRef]
- Ginsburg, G.S.; Willard, H.F. Genomic and personalized medicine: Foundations and applications. Transl. Res. 2009, 154, 277–287. [Google Scholar] [CrossRef]
- Mu, J.; Chaudhuri, K.R.; Bielza, C.; De Pedro-Cuesta, J.; Larrañaga, P.; Martinez-Martin, P. Parkinson’s Disease Subtypes Identified from Cluster Analysis of Motor and Non-motor Symptoms. Front. Aging Neurosci. 2017, 9, 301. [Google Scholar] [CrossRef] [PubMed]
- Marras, C.; Chaudhuri, K.R. Nonmotor features of Parkinson’s disease subtypes. Mov. Disord. 2016, 31, 1095–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erro, R.; Vitale, C.; Amboni, M.; Picillo, M.; Moccia, M.; Longo, K.; Santangelo, G.; De Rosa, A.; Allocca, R.; Giordano, F.; et al. The Heterogeneity of Early Parkinson’s Disease: A Cluster Analysis on Newly Diagnosed Untreated Patients. PLoS ONE 2013, 8, e70244. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.J.G.; Foltynie, T.; Blackwell, A.D.; Robbins, T.W.; Owen, A.M.; A Barker, R. Heterogeneity of Parkinson’s disease in the early clinical stages using a data driven approach. J. Neurol. Neurosurg. Psychiatry 2005, 76, 343–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryden, L.E.; Lewis, S.J.G. Parkinson’s Disease in the Era of Personalised Medicine: One Size Does Not Fit All. Drugs Aging 2018, 36, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Lenka, A.; Padmakumar, C.; Pal, P.K. Treatment of Older Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 132, 381–405. [Google Scholar] [CrossRef] [PubMed]
- Van Rooden, S.M.; Heiser, W.J.; Kok, J.N.; Verbaan, D.; Van Hilten, J.J.; Marinus, J. The identification of Parkinson’s disease subtypes using cluster analysis: A systematic review. Mov. Disord. 2010, 25, 969–978. [Google Scholar] [CrossRef] [PubMed]
- Bloem, B.R.; Henderson, E.J.; Dorsey, E.R.; Okun, M.S.; Okubadejo, N.; Chan, P.; Andrejack, J.; Darweesh, S.K.L.; Munneke, M. Integrated and patient-centred management of Parkinson’s disease: A network model for reshaping chronic neurological care. Lancet Neurol. 2020, 19, 623–634. [Google Scholar] [CrossRef]
- Legg, A.M.; Andrews, S.E.; Huynh, H.; Ghane, A.; Tabuenca, A.; Sweeny, K. Patients’ anxiety and hope: Predictors and adherence intentions in an acute care context. Health Expect. 2014, 18, 3034–3043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, S.J.G.; Gangadharan, S.; Padmakumar, C.P. Parkinson’s disease in the older patient. Clin. Med. 2016, 16, 376–378. [Google Scholar] [CrossRef] [PubMed]
- Fleisher, J.E.; Stern, M.B. Medication nonadherence in Parkinson’s disease. Curr. Neurol. Neurosci. Rep. 2013, 13, 382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curtis, J.R.; Safford, M.M. Management of Osteoporosis among the Elderly with Other Chronic Medical Conditions. Drugs Aging 2012, 29, 549–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espay, A.J.; Hausdorff, J.M.; Sánchez-Ferro, Á.; Klucken, J.; Merola, A.; Bonato, P.; Paul, S.S.; Horak, F.B.; Vizcarra, J.A.; Mestre, T.A.; et al. A roadmap for implementation of patient-centered digital outcome measures in Parkinson’s disease obtained using mobile health technologies. Mov. Disord. 2019, 34, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, K.R.; Martinez-Martin, P. Quantitation of non-motor symptoms in Parkinson’s disease. Eur. J. Neurol. 2008, 15, 2–8. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Older persons with PD have different care needs compared to a younger person with PD. |
| We do not have enough evidence-based medicine to identify what those specific care needs are; there is a big scope for future studies in this clinical domain. |
| There is an increasing amount of evidence advocating the need for monotherapy with L-Dopa in the very frail elderly cohort of people with PD. Whether this is the best approach, we need more studies. |
| Cognitive impairment plays an important role in deciding which medication should be prescribed in an older person with PD. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varma, P.; Narayan, L.; Alty, J.; Painter, V.; Padmakumar, C. An Innovative Personalised Management Program for Older Adults with Parkinson’s Disease: New Concepts and Future Directions. J. Pers. Med. 2021, 11, 43. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11010043
Varma P, Narayan L, Alty J, Painter V, Padmakumar C. An Innovative Personalised Management Program for Older Adults with Parkinson’s Disease: New Concepts and Future Directions. Journal of Personalized Medicine. 2021; 11(1):43. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11010043
Chicago/Turabian StyleVarma, Piyush, Lakshanaa Narayan, Jane Alty, Virginia Painter, and Chandrasekhara Padmakumar. 2021. "An Innovative Personalised Management Program for Older Adults with Parkinson’s Disease: New Concepts and Future Directions" Journal of Personalized Medicine 11, no. 1: 43. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11010043