
Invasive Ductal Breast Cancer with Osteoclast-Like Giant Cells: A Case Report Based on the Gene Expression Profile for Changes in Management

 , and
, and
Abstract
:1. Introduction
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.; Zackrisson, S.; Senkus, E. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [Green Version]
- Irelli, A.; Sirufo, M.M.; Scipioni, T.; De Pietro, F.; Pancotti, A.; Ginaldi, L.; De Martinis, M. Denosumab in breast cancer patients receiving aromatase inhibitors: A single-center observational study of effectiveness in adjuvant setting. Indian J. Cancer 2020. [Google Scholar] [CrossRef]
- Irelli, A.; Sirufo, M.M.; D’Ugo, C.; Ginaldi, L.; De Martinis, M. Real-life use of denosumab 120 mg every 12 weeks in prolonged treatment over 2 years of patients with breast cancer bone metastases. J. BUON 2020, 25, 1799–1804. [Google Scholar]
- Irelli, A.; Sirufo, M.M.; Scipioni, T.; De Pietro, F.; Pancotti, A.; Ginaldi, L.; De Martinis, M. Breast cancer patients receiving denosumab during adjuvant aromatase inhibitors treatment: Who are the "inadequate responders" patients to denosumab? J. BUON 2020, 25, 648–654. [Google Scholar]
- Gori, S.; Dieci, M.V.; Modena, A.; AIRTUM Working Group. Neoplasie per single sedi. Mammella. I numeri del cancro in Italia 2020. Intermedia Editore 2020. Available online: https://www.registri-tumori.it/cms/sites/default/files/pubblicazioni/new_NDC2020-operatori-web.pdf (accessed on 11 January 2021).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Irelli, A.; Sirufo, M.M.; Morelli, L.; D’Ugo, C.; Ginaldi, L.; De Martinis, M. Neuroendocrine Cancer of the Breast: A Rare Entity. J. Clin. Med. 2020, 9, 1452. [Google Scholar] [CrossRef]
- Wilson, P.C.; Chagpar, A.B.; Cicek, A.F.; Bossuyt, V.; Buza, N.; Mougalian, S.; Killelea, B.K.; Patel, N.; Harigopal, M. Breast cancer histopathology is predictive of low-risk Oncotype Dx recurrence score. Breast J. 2018, 24, 976–980. [Google Scholar] [CrossRef]
- Parmelee, P.A.; Thuras, P.D.; Katz, I.R.; Lawton, M.P. Validation of the Cumulative Illness Rating Scale in a Geriatric Residential Population. J. Am. Geriatr. Soc. 1995, 43, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in Development of the Index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontol. 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Irelli, A.; Sirufo, M.M.; Scipioni, T.; Aielli, F.; Martella, F.; Ginaldi, L.; Pancotti, A.; De Martinis, M. The VES-13 test as a predictor of toxicity associated with aromatase inhibitors in the adjuvant treatment of breast cancer in elderly patients: A single-center study. Indian J. Cancer 2020. (In press) [Google Scholar]
- Irelli, A.; Sirufo, M.M.; D’Ugo, C.; Ginaldi, L.; De Martinis, M. Sex and Gender Influences on Cancer Immunotherapy Response. Biomedicines 2020, 8, 232. [Google Scholar] [CrossRef]
- Zhang, L.; Hsieh, M.-C.; Petkov, V.; Yu, Q.; Chiu, Y.-W.; Wu, X.-C. Trend and survival benefit of Oncotype DX use among female hormone receptor-positive breast cancer patients in 17 SEER registries, 2004–2015. Breast Cancer Res. Treat. 2020, 180, 491–501. [Google Scholar] [CrossRef]
- Gori, S.; Dieci, M.V.; Biganzoli, L.; Calabrese, M.; Cortesi, L.; Criscitiello, C.; Del Mastro, L.; Dellepiane, C.; Fortunato, L.; Franco, P.; et al. Breast Neoplasms Guidelines, 2020 ed. Available online: https://www.aiom.it/wp-content/uploads/2020/10/20201218_LG_AIOM_NeoplasieMammella.pdf (accessed on 11 January 2021).
- Bomeisl, P.E.; Thompson, C.L.; Harris, L.N.; Gilmore, H.L. Comparison of Oncotype DX Recurrence Score by Histologic Types of Breast Carcinoma. Arch. Pathol. Lab. Med. 2015, 139, 1546–1549. [Google Scholar] [CrossRef] [PubMed]
- Christgen, M.; Gluz, O.; Harbeck, N.; Kates, R.E.; Raap, M.; Christgen, H.; Clemens, M.; Malter, W.; Nuding, B.; Aktas, B.; et al. West German Study Group PlanB Investigators. Differential impact of prognostic parameters in hor-mone receptor-positive lobular breast cancer. Cancer 2020, 126, 4847–4858. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; He, X.; Kalife, E.T.; Ehdaivand, S.; Wang, Y.; Sung, C.J. Relationship of histologic grade and histologic sub-type with oncotype Dx recurrence score; retrospective review of 863 breast cancer oncotype Dx results. Breast Cancer Res. Treat. 2018, 168, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Sparano, J.A.; Gray, R.J.; Ravdin, P.M.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E.; Dees, E.C.; Goetz, M.P.; et al. Clinical and Genomic Risk to Guide the Use of Adjuvant Therapy for Breast Cancer. N. Engl. J. Med. 2019, 380, 2395–2405. [Google Scholar] [CrossRef]
- Albawardi, A.S.; Awwad, A.A.; Almarzooqi, S.S. Mammary carcinoma with osteoclast-like giant cells: A case report. Int. J. Clin. Exp. Pathol. 2014, 7, 9038–9043. [Google Scholar] [PubMed]
- Agnantis, N.T.; Rosen, P.P. Mammary carcinoma with osteoclast-like giant cells. A study of eight cases with fol-low-up data. Am. J. Clin. Pathol. 1979, 72, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Holland, R.; van Haelst, U.J. Mammary carcinoma with osteoclast-like giant cells. Additional observations on six cases. Cancer 1984, 53, 1963–1973. [Google Scholar] [CrossRef]
- Pettinato, G.; Manivel, J.; Picone, A.; Petrella, G.; Insabato, L. Alveolar variant of infiltrating lobular carcinoma of the breast with stromal osteoclast-like giant cells. Pathol. Res. Pr. 1989, 185, 388–394. [Google Scholar] [CrossRef]
- Athanasou, N.A.; Wells, C.A.; Quinn, J.; Ferguson, D.P.; Heryet, A.; McGee, J.O. The origin and nature of stromal osteo-clast-like multinucleated giant cells in breast carcinoma: Implications for tumour osteolysis and macrophage biology. Br. J. Cancer. 1989, 59, 491–498. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, T.; Moriki, T.; Hiroi, M.; Nakayama, H. Invasive Lobular Carcinoma of the Breast with Osteoclastlike Giant Cells. Acta Cytol. 1998, 42, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Niu, Y.; Liao, X.; Li, X.; Zhao, L. Breast carcinoma with osteoclastic giant cells: Case report and review of the litera-ture. Int. J. Clin. Exp. Pathol. 2014, 7, 1788–1791. [Google Scholar]
- Khong, K.; Zhang, Y.; Tomic, M.; Lindfors, K.K.; Aminololama-Shakeri, S. Aggressive Metaplastic Carcinoma of the Breast with Osteoclastic Giant Cells. J. Radiol. Case Rep. 2015, 9, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Peña-Jaimes, L.; González-García, I.; Reguero-Callejas, M.E.; Pinilla-Pagnon, I.; Pérez-Mies, B.; Albarrán-Artahona, V.; Martínez-Jañez, N.; Rosa-Rosa, J.M.; Palacios, J. Pleomorphic lobular carcinoma of the breast with osteoclast-like giant cells: A case report and review of the literature. Diagn. Pathol. 2018, 13, 62. [Google Scholar] [CrossRef]
- Zhou, S.; Yu, L.; Zhou, R.; Li, X.; Yang, W. Invasive breast carcinomas of no special type with osteoclast-like giant cells frequently have a luminal phenotype. Virchows Arch. 2014, 464, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Shishido-Hara, Y.; Kurata, A.; Fujiwara, M.; Itoh, H.; Imoto, S.; Kamma, H. Two cases of breast carcinoma with osteo-clastic giant cells: Are the osteoclastic giant cells pro-tumoural differentiation of macrophages? Diagn Pathol. 2010, 23, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohashi, R.; Yanagihara, K.; Namimatsu, S.; Sakatani, T.; Takei, H.; Naito, Z.; Shimizu, A. Osteoclast-like giant cells in invasive breast cancer predominantly possess M2-macrophage phenotype. Pathol. Res. Pr. 2018, 214, 253–258. [Google Scholar] [CrossRef]
- Ohashi, R.; Hayama, A.; Matsubara, M.; Watarai, Y.; Sakatani, T.; Naito, Z.; Shimizu, A. Breast carcinoma with osteo-clast-like giant cells: A cytological-pathological correlation with a literature review. Ann. Diagn Pathol. 2018, 33, 1–5. [Google Scholar] [CrossRef]
- Güth, U.; Borovecki, A.; Amann, E.; Rechsteiner, M.; Tinguely, M. Pleomorphic lobular breast carcinoma with osteo-clast like giant cells in the era of genomic testing. Curr. Probl. Cancer Case Rep. 2020, 1, 100008. [Google Scholar] [CrossRef]
- Stratton, A.; Plackett, T.P.; Belnap, C.M.; Lin-Hurtubise, K.M. Infiltrating Mammary Carcinoma with Osteoclast-like Giant Cells. Hawaii Med. J. 2010, 69, 284–285. [Google Scholar]
- Zagelbaum, N.K.; Ward, M.F.; Okby, N.; Karpoff, H. Invasive ductal carcinoma of the breast with osteoclast-like giant cells and clear cell features: A case report of a novel finding and review of the literature. World J. Surg. Oncol. 2016, 14, 227. [Google Scholar] [CrossRef] [Green Version]
- Jamiyan, T.; Kuroda, H.; Hayashi, M.; Abe, A.; Shimizu, K.; Imai, Y. Ductal carcinoma in situ of the breast with osteoclast-like giant cells: A case report with immunohistochemical analysis. Hum. Pathol. Case Rep. 2020, 20, 200383. [Google Scholar] [CrossRef]
- Andre, F.; Ismaila, N.; Henry, N.L.; Somerfield, M.R.; Bast, R.C.; Barlow, W.; Collyar, D.E.; Hammond, M.E.; Kuderer, N.M.; Liu, M.C.; et al. Use of Biomarkers to Guide Decisions on Adjuvant Systemic Therapy for Women With Early-Stage Invasive Breast Cancer: ASCO Clinical Practice Guideline Up-date-Integration of Results From TAILORx. J. Clin. Oncol. 2019, 37, 1956–1964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E.; Dees, E.C.; Perez, E.A.; Olson, J.A.; et al. Prospective Validation of a 21-Gene Expression Assay in Breast Cancer. N. Engl. J. Med. 2015, 373, 2005–2014. [Google Scholar] [CrossRef]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E., Jr.; Dees, E.C.; Goetz, M.P.; Olson, J.A., Jr.; et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer. N. Engl. J. Med. 2018, 379, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Dieci, M.V.; Guarneri, V.; Zustovich, F.; Mion, M.; Morandi, P.; Bria, E.; Merlini, L.; Bullian, P.; Oliani, C.; Gori, S.; et al. Impact of 21-Gene Breast Cancer Assay on Treatment Decision for Patients with T1–T3, N0–N1, Estrogen Receptor-Positive/Human Epidermal Growth Receptor 2-Negative Breast Cancer: Final Results of the Prospective Multicenter ROXANE Study. Oncologist 2019, 24, 1424–1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizuno, Y.; Fuchikami, H.; Takeda, N.; Yamada, J.; Inoue, Y.; Seto, H.; Sato, K. Comparing Oncotype DX Recurrence Score Categories with Immunohistochemically Defined Luminal Subtypes. J. Cancer Ther. 2016, 7, 223–231. [Google Scholar] [CrossRef] [Green Version]
- Acs, G.; Esposito, N.N.; Kiluk, J.; Loftus, L.; Laronga, C. A mitotically active, cellular tumor stroma and/or inflammatory cells associated with tumor cells may contribute to intermediate or high Oncotype DX Recurrence Scores in low-grade invasive breast carcinomas. Mod. Pathol. 2011, 25, 556–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acs, G.; Kiluk, J.; Loftus, L.; Laronga, C. Comparison of Oncotype DX and Mammostrat risk estimations and corre-lations with histologic tumor features in low-grade, estrogen receptor-positive invasive breast carcinomas. Mod. Pathol. 2013, 26, 1451–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
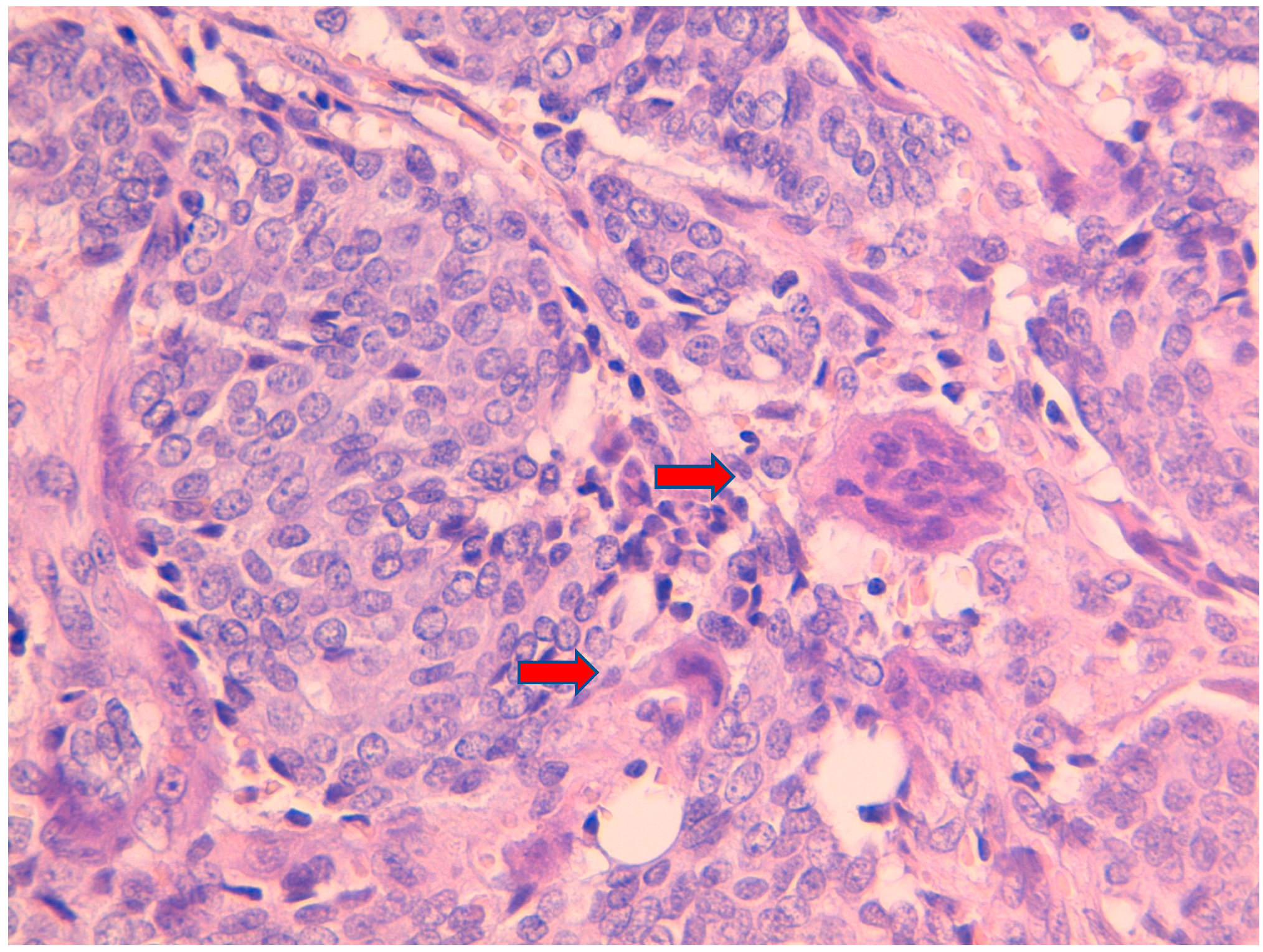
 ).
).
).
).
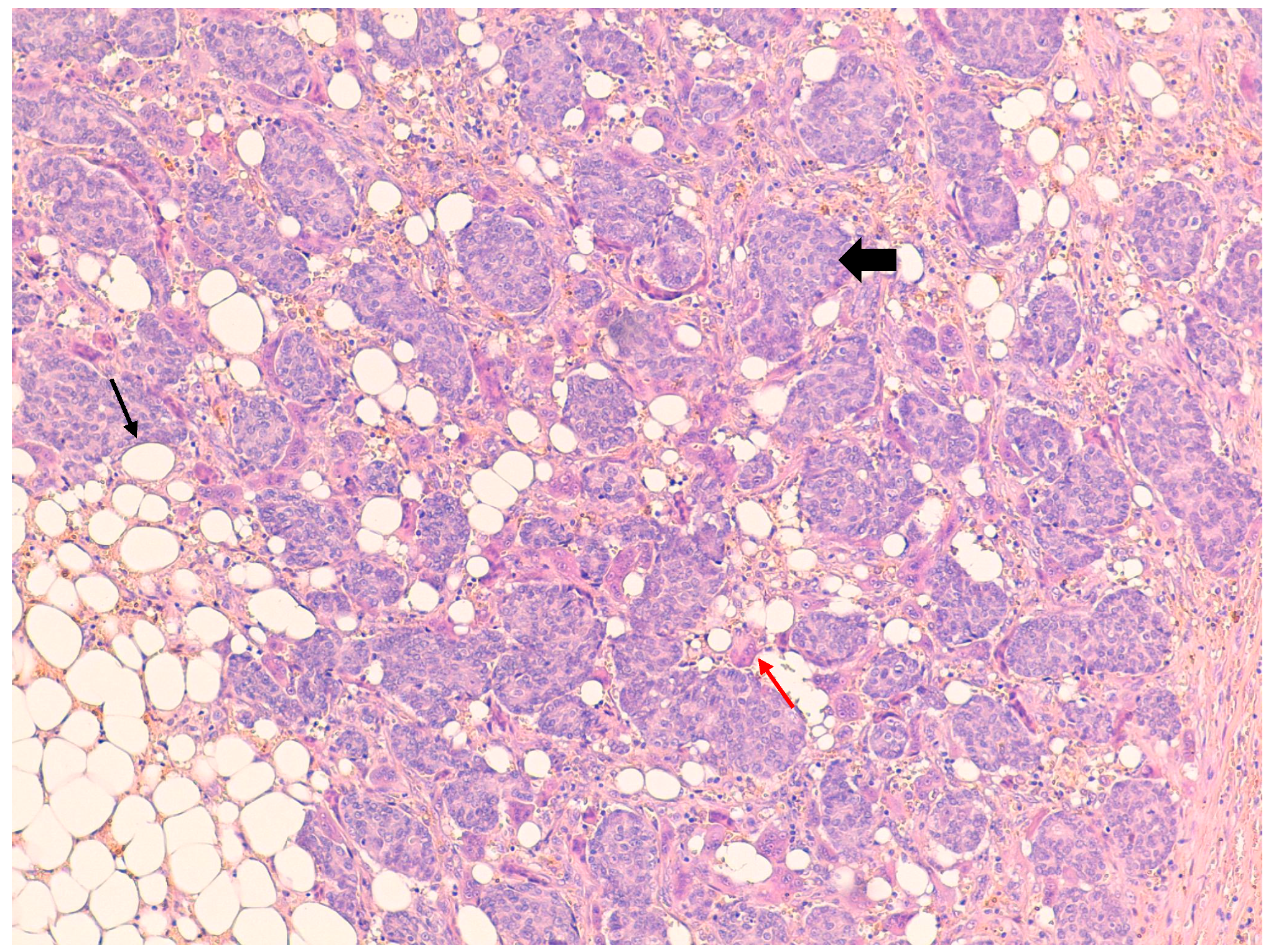
 ) are present immersed in the stroma containing adipocytes (↑).
) are present immersed in the stroma containing adipocytes (↑).
) are present immersed in the stroma containing adipocytes (↑).
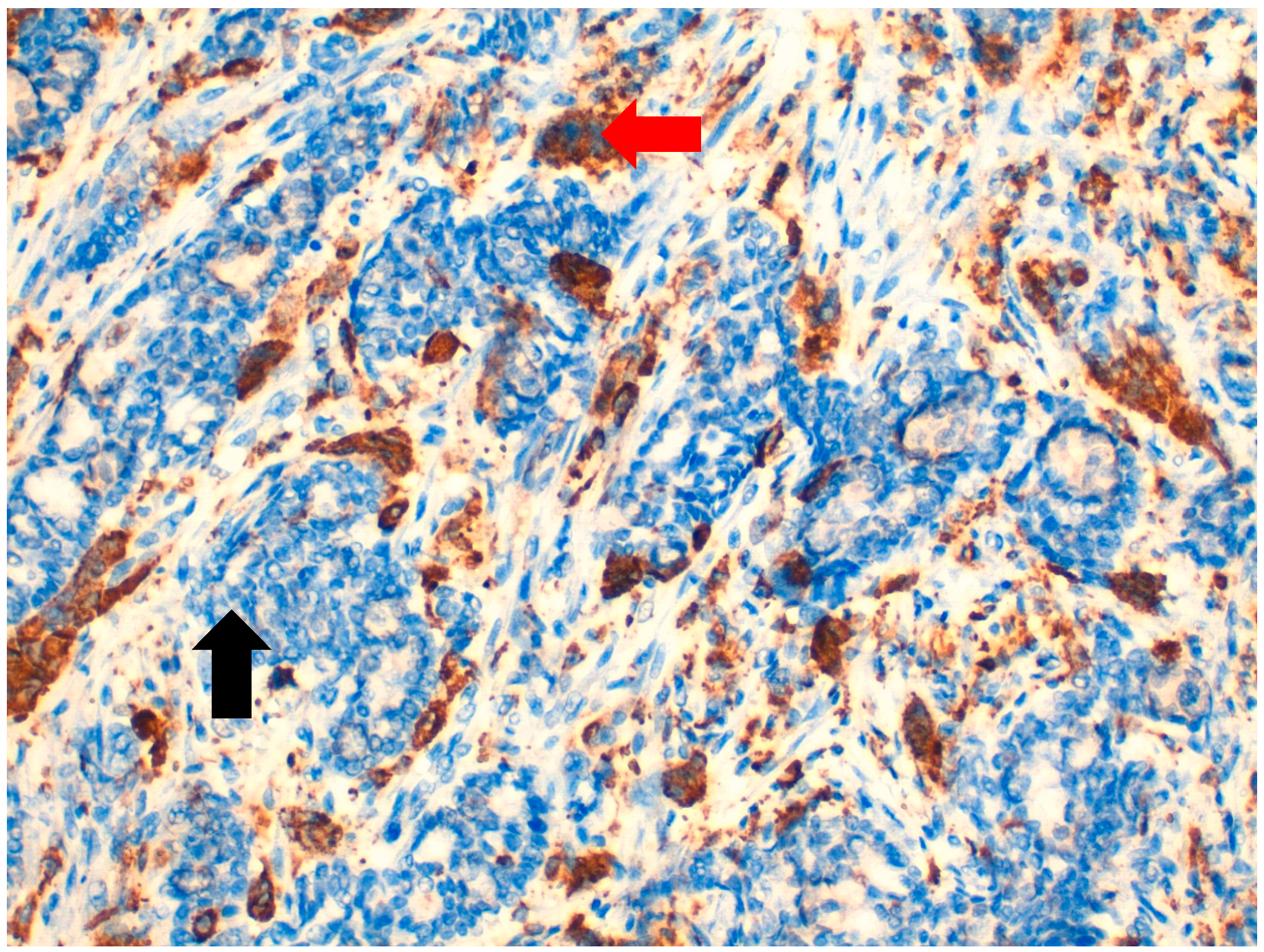
) are present immersed in the stroma containing adipocytes (↑). ), unlike neoplastic cells, which are CD68-negative ( ).
), unlike neoplastic cells, which are CD68-negative ( ).
), unlike neoplastic cells, which are CD68-negative ( ).
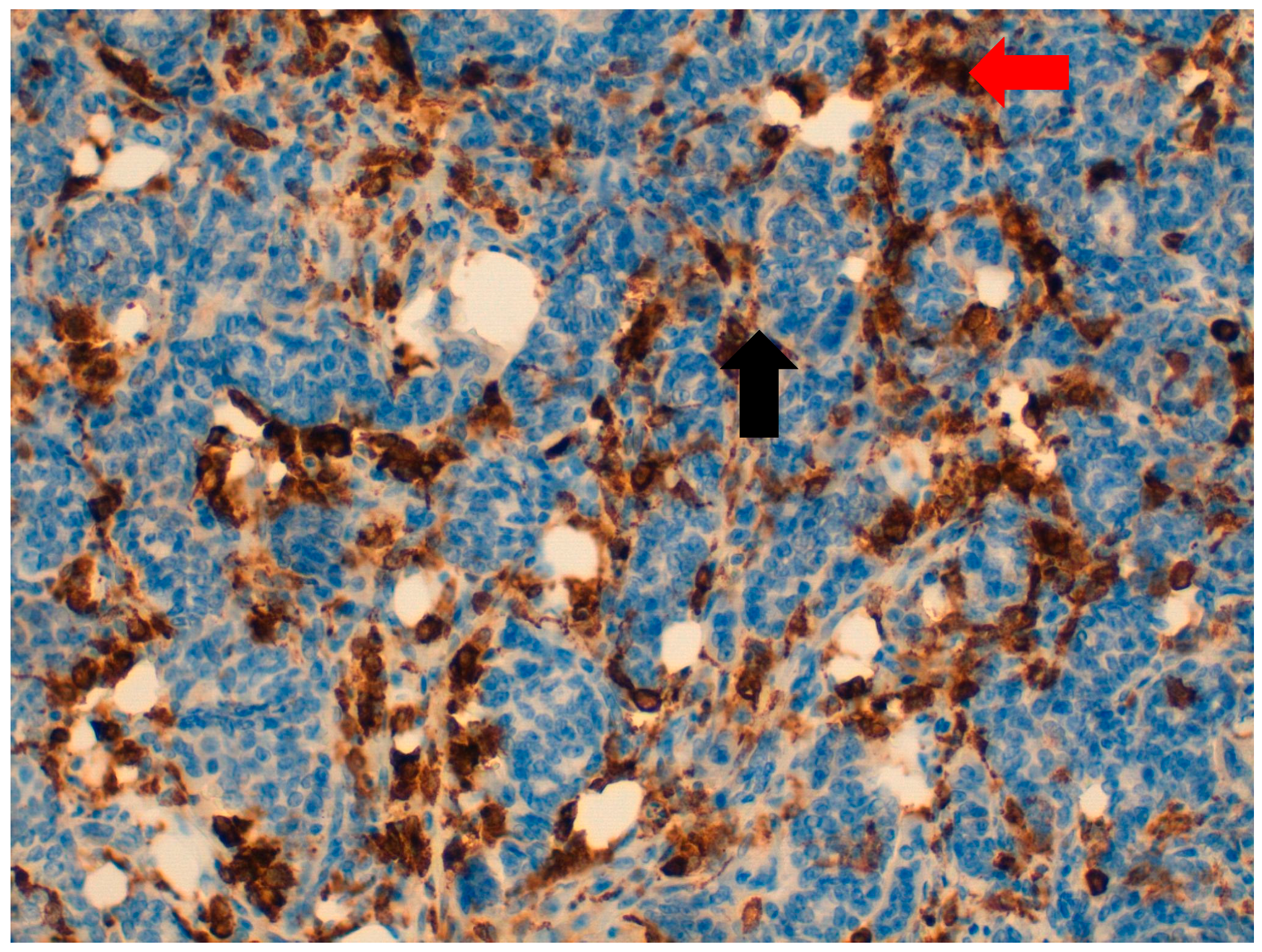
), unlike neoplastic cells, which are CD68-negative ( ). ), unlike neoplastic cells, which are CD163-negative ( ).
), unlike neoplastic cells, which are CD163-negative ( ).
), unlike neoplastic cells, which are CD163-negative ( ).
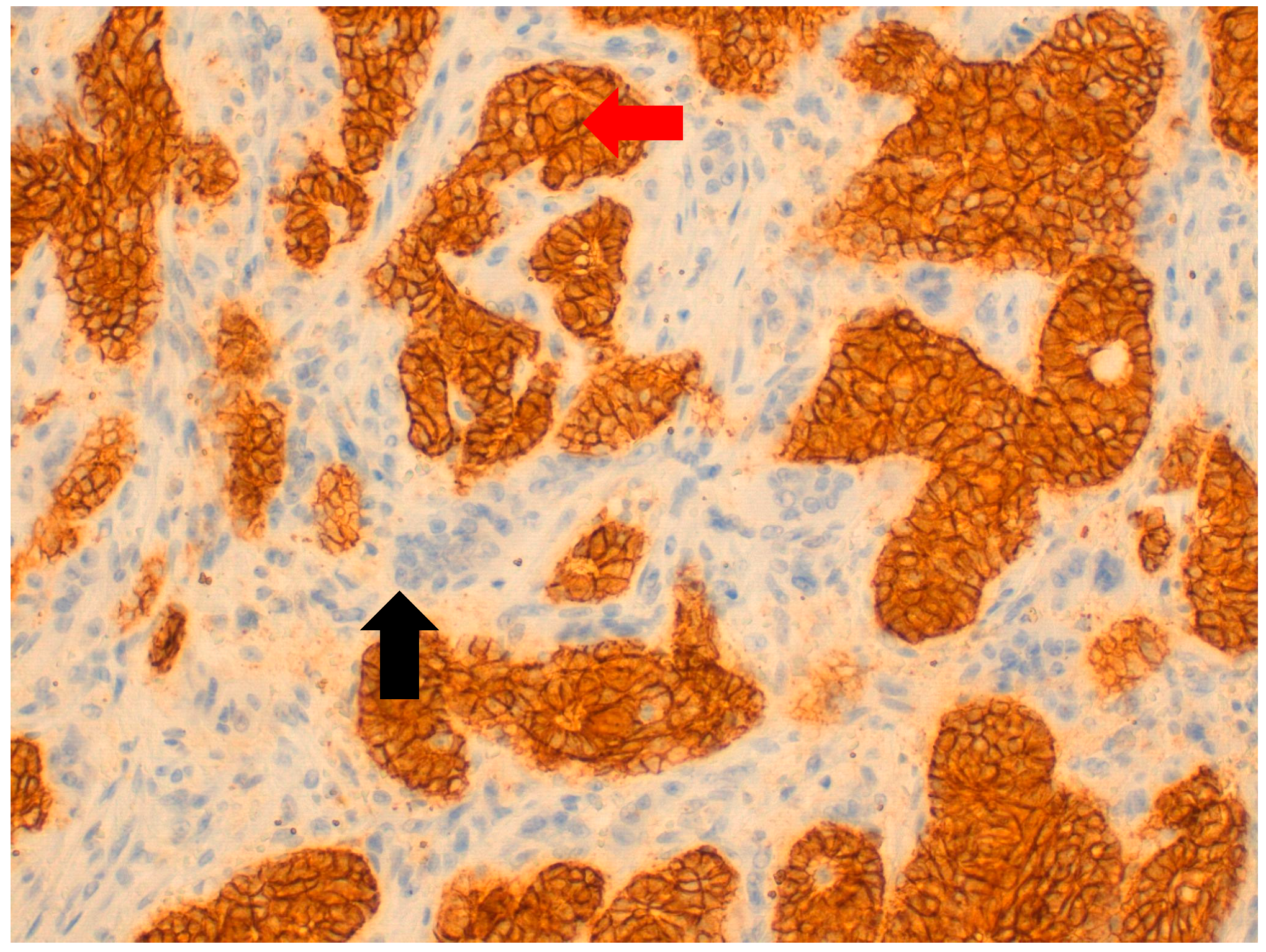
), unlike neoplastic cells, which are CD163-negative ( ). ), unlike OGCs, which are E-cadherin-negative ( ).
), unlike OGCs, which are E-cadherin-negative ( ).
), unlike OGCs, which are E-cadherin-negative ( ).
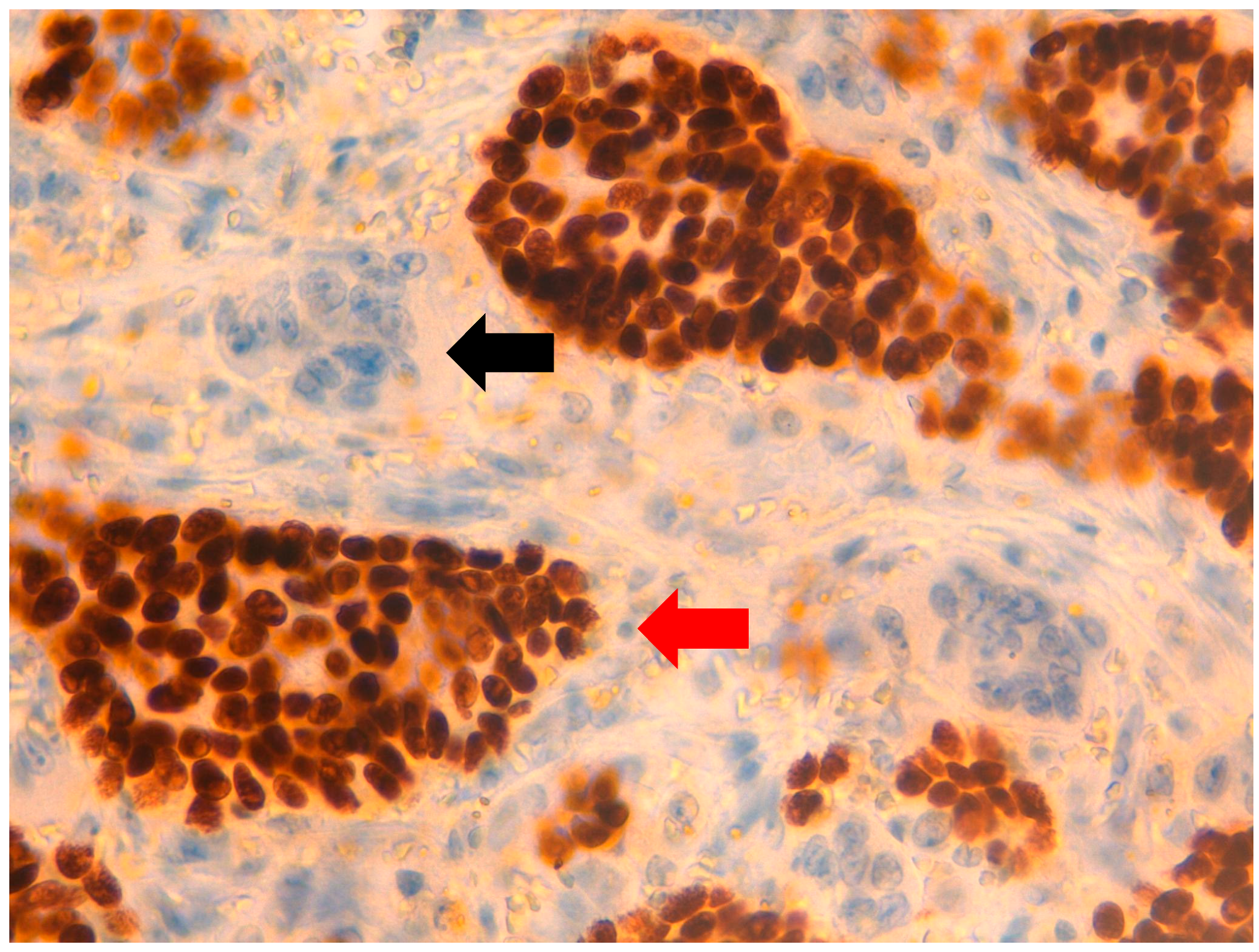
), unlike OGCs, which are E-cadherin-negative ( ). ), unlike OGCs, which are estrogen receptor-negative ( ).
), unlike OGCs, which are estrogen receptor-negative ( ).
), unlike OGCs, which are estrogen receptor-negative ( ).
), unlike OGCs, which are estrogen receptor-negative ( ). ), unlike OGCs which are progesterone receptor-negative ( ).
), unlike OGCs which are progesterone receptor-negative ( ).
), unlike OGCs which are progesterone receptor-negative ( ).
), unlike OGCs which are progesterone receptor-negative ( ). ) and OGCs ( ).
) and OGCs ( ).
) and OGCs ( ).
) and OGCs ( ).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cancer Cells | Osteoclast-Like Giant Cells | |
|---|---|---|
| Estrogen Receptor | + | - |
| Progesterone Receptor | + | - |
| Human Epidermal Growth Factor Receptor 2 | - | - |
| E-cadherin | + | - |
| CD68 | - | + |
| CD163 | - | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Irelli, A.; Sirufo, M.M.; Quaglione, G.R.; De Pietro, F.; Bassino, E.M.; D’Ugo, C.; Ginaldi, L.; De Martinis, M. Invasive Ductal Breast Cancer with Osteoclast-Like Giant Cells: A Case Report Based on the Gene Expression Profile for Changes in Management. J. Pers. Med. 2021, 11, 156. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11020156
Irelli A, Sirufo MM, Quaglione GR, De Pietro F, Bassino EM, D’Ugo C, Ginaldi L, De Martinis M. Invasive Ductal Breast Cancer with Osteoclast-Like Giant Cells: A Case Report Based on the Gene Expression Profile for Changes in Management. Journal of Personalized Medicine. 2021; 11(2):156. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11020156
Chicago/Turabian StyleIrelli, Azzurra, Maria Maddalena Sirufo, Gina Rosaria Quaglione, Francesca De Pietro, Enrica Maria Bassino, Carlo D’Ugo, Lia Ginaldi, and Massimo De Martinis. 2021. "Invasive Ductal Breast Cancer with Osteoclast-Like Giant Cells: A Case Report Based on the Gene Expression Profile for Changes in Management" Journal of Personalized Medicine 11, no. 2: 156. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11020156