
Alteration of White Matter in Patients with Central Post-Stroke Pain

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
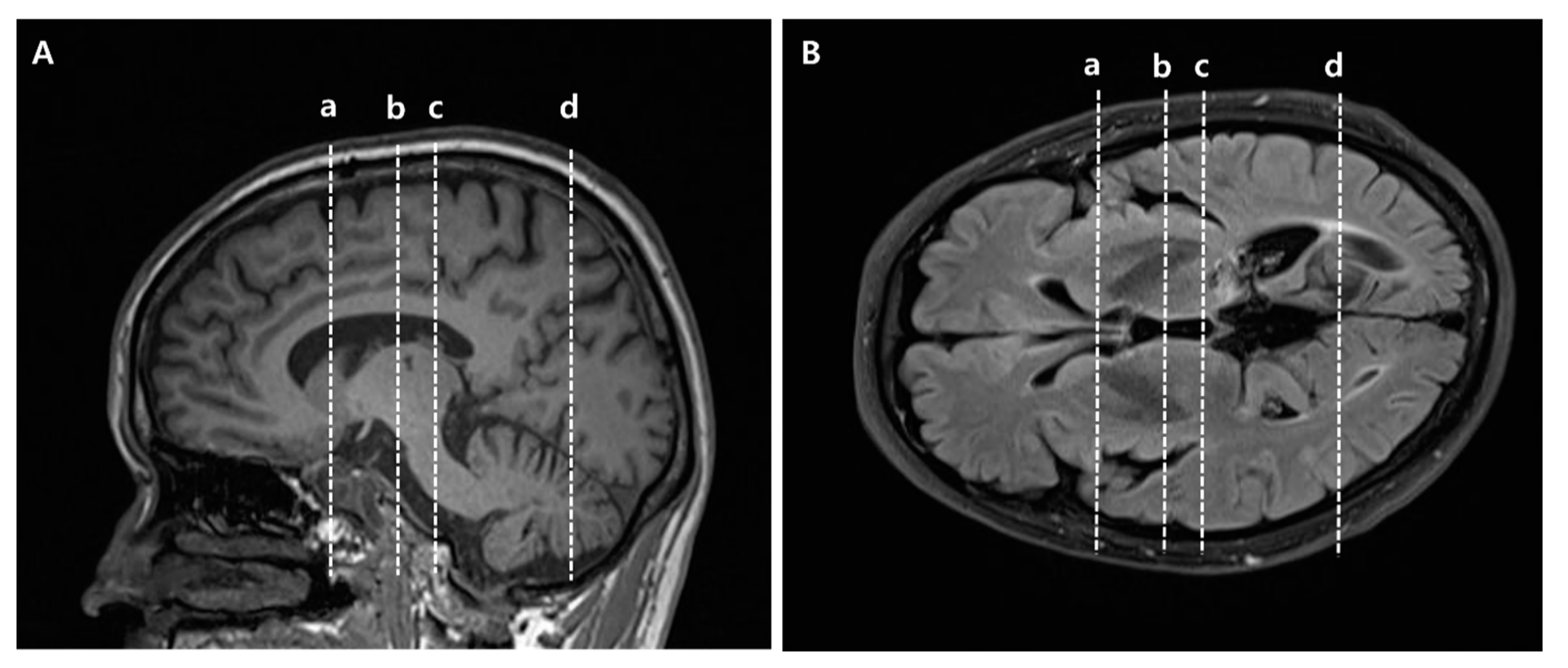
2.2. Diffusion Tensor Imaging Acquisition and Image Processing
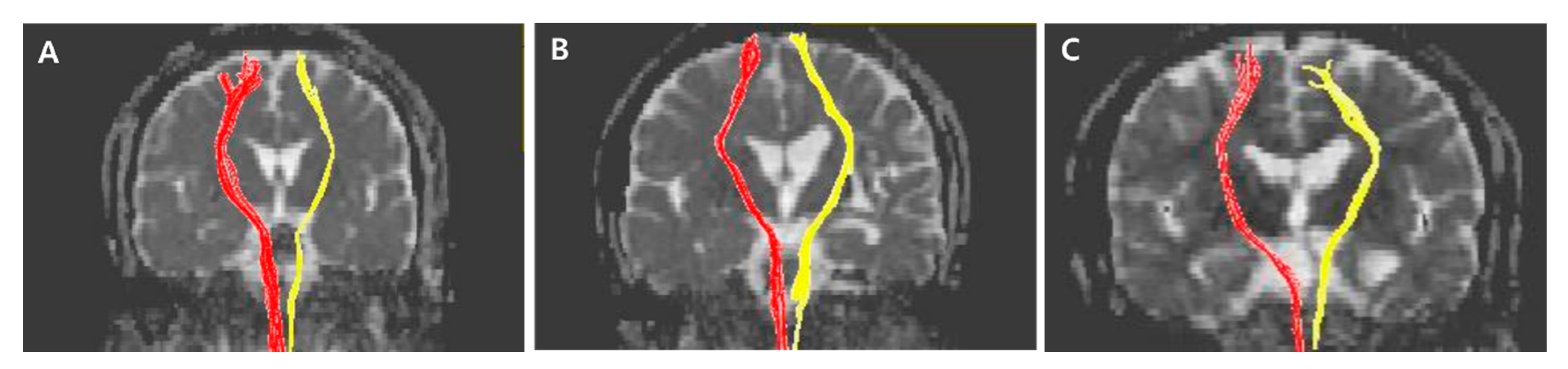
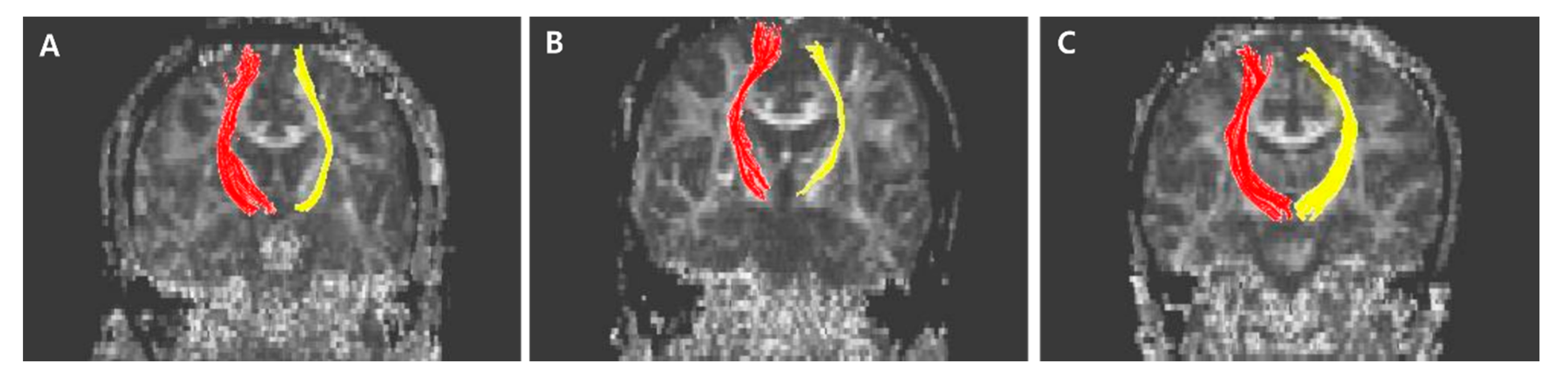
2.3. Diffusion Tensor Tractography
2.4. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klit, H.; Finnerup, N.B.; Jensen, T.S. Central post-stroke pain: Clinical characteristics, pathophysiology, and management. Lancet Neurol. 2009, 8, 857–868. [Google Scholar] [CrossRef]
- Devulder, J.; Crombez, E.; Mortier, E. Central pain: An overview. Acta Neurol. Belg. 2002, 102, 97–103. [Google Scholar]
- Ofek, H.; Defrin, R. The characteristics of chronic central pain after traumatic brain injury. Pain 2007, 131, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Wasner, G.; Lee, B.B.; Engel, S.; McLachlan, E. Residual spinothalamic tract pathways predict development of central pain after spinal cord injury. Brain 2008, 131, 2387–2400. [Google Scholar] [CrossRef] [PubMed]
- Boivie, J.; Leijon, G.; Johansson, I. Central post-stroke pain—A study of the mechanisms through analyses of the sensory abnormalities. Pain 1989, 37, 173–185. [Google Scholar] [CrossRef]
- Vestergaard, K.; Nielsen, J.; Andersen, G.; Ingeman-Nielsen, M.; Arendt-Nielsen, L.; Jensen, T.S. Sensory abnormalities in consecutive, unselected patients with central post-stroke pain. Pain 1995, 61, 177–186. [Google Scholar] [CrossRef]
- Kumar, B.; Kalita, J.; Kumar, G.; Misra, U.K. Central poststroke pain: A review of pathophysiology and treatment. Anesth. Analg. 2009, 108, 1645–1657. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.H.; Son, S.M.; Jang, S.H. Identification of spinothalamic tract and its related thalamocortical fibers in human brain. Neurosci. Lett. 2010, 468, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Bowsher, D.; Leijon, G.; Thuomas, K.A. Central poststroke pain: Correlation of mri with clinical pain characteristics and sensory abnormalities. Neurology 1998, 51, 1352–1358. [Google Scholar] [CrossRef]
- Seghier, M.L.; Lazeyras, F.; Vuilleumier, P.; Schnider, A.; Carota, A. Functional magnetic resonance imaging and diffusion tensor imaging in a case of central poststroke pain. J. Pain 2005, 6, 208–212. [Google Scholar] [CrossRef]
- Misra, U.K.; Kalita, J.; Kumar, B. A study of clinical, magnetic resonance imaging, and somatosensory-evoked potential in central post-stroke pain. J. Pain 2008, 9, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- Lau, B.K.; Vaughan, C.W. Descending modulation of pain: The gaba disinhibition hypothesis of analgesia. Curr. Opin. Neurobiol. 2014, 29, 159–164. [Google Scholar] [CrossRef]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.H.; Bai, D.S.; Jeong, J.Y.; Choi, B.Y.; Chang, C.H.; Kim, S.H.; Ahn, S.H.; Jang, S.H. Injury of the spino-thalamo-cortical pathway is necessary for central post-stroke pain. Eur. Neurol. 2010, 64, 163–168. [Google Scholar] [CrossRef]
- Hong, J.H.; Choi, B.Y.; Chang, C.H.; Kim, S.H.; Jung, Y.J.; Lee, D.G.; Kwon, Y.H.; Jang, S.H. The prevalence of central poststroke pain according to the integrity of the spino-thalamo-cortical pathway. Eur. Neurol. 2012, 67, 12–17. [Google Scholar] [CrossRef]
- Jang, S.H.; Lee, J.; Yeo, S.S. Central post-stroke pain due to injury of the spinothalamic tract in patients with cerebral infarction: A diffusion tensor tractography imaging study. Neural. Regen. Res. 2017, 12, 2021–2024. [Google Scholar] [CrossRef]
- Kim, N.Y.; Lee, S.C.; An, Y.S.; Shin, J.C.; Kim, Y.W. Metabolic changes in central poststroke pain following thalamic intracerebral hemorrhage: An 18f-fdg pet study. Clin. Nucl. Med. 2018, 43, e62–e66. [Google Scholar] [CrossRef]
- Kim, Y.; Im, S.; Kim, S.H.; Park, G.Y. Laterality of cerebellar afferent and efferent pathways in a healthy right-handed population: A diffusion tensor imaging study. J. Neurosci. Res. 2019, 97, 582–596. [Google Scholar] [CrossRef]
- Lee, K.B.; Lim, S.H.; Kim, K.H.; Kim, K.J.; Kim, Y.R.; Chang, W.N.; Yeom, J.W.; Kim, Y.D.; Hwang, B.Y. Six-month functional recovery of stroke patients: A multi-time-point study. Int. J. Rehabil. Res. 2015, 38, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.H.; Lee, H.D. Central pain due to spinothalamic tract injury caused by indirect head trauma following a pratfall. Brain Inj. 2016, 30, 933–936. [Google Scholar] [CrossRef]
- Tang, S.C.; Lee, L.J.; Jeng, J.S.; Hsieh, S.T.; Chiang, M.C.; Yeh, S.J.; Hsueh, H.W.; Chao, C.C. Pathophysiology of central poststroke pain: Motor cortex disinhibition and its clinical and sensory correlates. Stroke 2019, 50, 2851–2857. [Google Scholar] [CrossRef]
- Yoo, Y.J.; Kim, J.W.; Kim, J.S.; Hong, B.Y.; Lee, K.B.; Lim, S.H. Corticospinal tract integrity and long-term hand function prognosis in patients with stroke. Front. Neurol. 2019, 10, 374. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Kang, W.; Ohn, S.H.; Jung, K.-I.; Bashir, S.; Yoo, W.-K. An Exploration of the Neural Network of Lance-Adams Syndrome: A Case Report. Brain Neurorehabilit. 2021, 14. [Google Scholar] [CrossRef]
- Jiang, H.; van Zijl, P.C.; Kim, J.; Pearlson, G.D.; Mori, S. Dtistudio: Resource program for diffusion tensor computation and fiber bundle tracking. Comput. Methods Programs Biomed. 2006, 81, 106–116. [Google Scholar] [CrossRef]
- Jang, S.H.; Kim, K.; Kim, S.H.; Son, S.M.; Jang, W.H.; Kwon, H.G. The relation between motor function of stroke patients and diffusion tensor imaging findings for the corticospinal tract. Neurosci. Lett. 2014, 572, 1–6. [Google Scholar] [CrossRef]
- Jang, S.H.; Seo, J.P.; Lee, S.J. Diffusion tensor tractography studies of central post-stroke pain due to the spinothalamic tract injury: A mini-review. Front. Neurol. 2019, 10, 787. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.; Jung, Y.; Kwon, H.K.; Pyun, S.B. Complex Regional Pain Syndrome of Non-hemiplegic Upper Limb in a Stroke Patient: A Case Report. Ann. Rehabil. Med. 2018, 42, 175–179. [Google Scholar] [CrossRef] [Green Version]
- Mori, S.; Kaufmann, W.E.; Davatzikos, C.; Stieltjes, B.; Amodei, L.; Fredericksen, K.; Pearlson, G.D.; Melhem, E.R.; Solaiyappan, M.; Raymond, G.V.; et al. Imaging cortical association tracts in the human brain using diffusion-tensor-based axonal tracking. Magn. Reson. Med. 2002, 47, 215–223. [Google Scholar] [CrossRef]
- Wakana, S.; Jiang, H.; Nagae-Poetscher, L.M.; van Zijl, P.C.; Mori, S. Fiber tract-based atlas of human white matter anatomy. Radiology 2004, 230, 77–87. [Google Scholar] [CrossRef]
- George, K.; Das, J.M. Neuroanatomy, thalamocortical radiations. In Statpearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CPSP | Stroke Control | Normal Control | p | |
|---|---|---|---|---|
| Subjects, n | 17 | 26 | 34 | |
| Age, years | 57.3 (51.75–62.25) | 53.17 (44.0–67.25) | 57.9 (51.0–64.0) | |
| Female sex, n (%) | 4 (23.5) | 8 (30.8) | 10 (29.4) | 0.867 |
| Stroke type, n (%) | ||||
| Hemorrhage | 9 (52.9) | 14 (53.8) | N/A | 0.954 |
| Infarction | 8 (47.1) | 12 (46.2) | N/A | |
| Brain injury location, n (%) | ||||
| Basal ganglia | 10 (58.8) | 15 (57.7) | N/A | 0.810 |
| Thalamus | 6 (35.3) | 8 (30.8) | N/A | |
| Both | 1 (5.9) | 3 (11.5) | N/A | |
| Stroke side, Left/Right, n (%) | 12/5 (70.6/29.4) | 18/8 (69.2/30.8) | N/A | 0.925 |
| Comorbidity | ||||
| Diabetus Mellitus | 4 (23.5) | 1 (3.8) | 5(14.7) | 0.159 |
| Hypertension | 9 (52.9) | 16 (61.5) | 12 (35.3) | 0.118 |
| Arterial fibrillation | 0 (0) | 2 (7.7) | 0 (0) | 0.133 |
| Values | CPSP | P1 | Stroke Control | P2 | Normal Control | P3 | |
|---|---|---|---|---|---|---|---|
| CST | FN | 0.31 (0.06–0.76) | 0.881 | 0.33 (0.05–0.71) | 0.003 | 0.86 (0.46–1.14) | 0.001 |
| FA | 0.75 (0.65–0.94) | 0.881 | 0.79 (0.73–0.90) | <0.001 | 0.96 (0.91–1.03) | <0.001 | |
| STT | FN | 0.47 (0.31–0.69) | 0.728 | 0.40 (0.09–0.86) | <0.001 | 1.4 (0.59–2.73) | <0.001 |
| FA | 0.79 (0.68–0.85) * | <0.001 | 0.98 (0.85–1.11) * | 0.994 | 0.98 (0.91–1.10) * | <0.001 | |
| ATR | FN | 0.76 (0.65–0.94) | 0.823 | 0.68 (0.60–1.10) | 0.005 | 1.00 (0.90–1.26) | 0.002 |
| FA | 0.96 (0.83–1.09) | 0.593 | 0.99 (0.85–1.09) | 0.551 | 1.01 (0.95–1.06) | 0.337 | |
| STR | FN | 0.45 (0.28–0.62) | 0.785 | 0.34 (0.17–0.70) | <0.001 | 0.91 (0.67–1.40) | <0.001 |
| FA | 0.88 (0.83–0.93) * | 0.004 | 1.00 (0.90–1.07) * | 0.836 | 0.97 (0.91–1.04) * | 0.001 | |
| PTR | FN | 0.32 (0.18–0.86) | 0.172 | 0.60 (0.40–1.22) | 0.748 | 0.69 (0.25–1.27) | 0.223 |
| FA | 0.93 (0.87–1.00) | 0.087 | 1.03 (0.93–1.12) | 0.005 | 0.91 (0.84–0.98) | 0.734 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.G.; Hong, B.Y.; Park, H.-Y.; Yoo, Y.J.; Yoon, M.-J.; Kim, J.-S.; Lim, S.H. Alteration of White Matter in Patients with Central Post-Stroke Pain. J. Pers. Med. 2021, 11, 417. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050417
Park JG, Hong BY, Park H-Y, Yoo YJ, Yoon M-J, Kim J-S, Lim SH. Alteration of White Matter in Patients with Central Post-Stroke Pain. Journal of Personalized Medicine. 2021; 11(5):417. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050417
Chicago/Turabian StylePark, Jung Geun, Bo Young Hong, Hae-Yeon Park, Yeun Jie Yoo, Mi-Jeong Yoon, Joon-Sung Kim, and Seong Hoon Lim. 2021. "Alteration of White Matter in Patients with Central Post-Stroke Pain" Journal of Personalized Medicine 11, no. 5: 417. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050417