
Polygenic Panels Predicting the Susceptibility of Multiple Upper Aerodigestive Tract Cancer in Oral Cancer Patients

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. DNA Extraction
2.3. SNP Array Genotyping and Quality Control
2.4. Statistics for Array Analysis
2.5. Polygenic Risk Score
3. Results
3.1. Characteristics of Study Population
3.2. Upper Aerodigestive Tract MPT Related SNPs
3.3. Multivariate Analysis
3.4. Polygenic Risk Score Construction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taiwan Cancer Registry. 2010 Annual Report. 1 January 2012. Available online: http://crs.cph.ntu.edu.tw/ (accessed on 16 May 2021).
- Liao, C.-T.; Wang, H.-M.; Ng, S.-H.; Yen, T.-C.; Lee, L.-Y.; Hsueh, C.; Wei, F.-C.; Chen, I.-H.; Kang, C.-J.; Huang, S.-F.; et al. Good tumor control and survivals of squamous cell carcinoma of buccal mucosa treated with radical surgery with or without neck dissection in Taiwan. Oral Oncol. 2006, 42, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Mohrenweiser, H.W. Genetic Variation and Exposure Related Risk Estimation: Will Toxicology Enter a New Era? DNA Repair and Cancer as a Paradigm. Toxicol. Pathol. 2004, 32, 136–145. [Google Scholar] [CrossRef]
- Caporaso, N.; Landi, M.T.; Vineis, P. Relevance of metabolic polymorphisms to human carcinogenesis: Evaluation of epidemiologic evidence. Pharmacogenetics 1991, 1, 4–19. [Google Scholar] [CrossRef] [PubMed]
- Kazma, R.; Babron, M.-C.; Gaborieau, V.; Génin, E.; Brennan, P.; Hung, R.J.; McLaughlin, J.R.; Krokan, H.E.; Elvestad, M.B.; Skorpen, F.; et al. Lung cancer and DNA repair genes: Multilevel association analysis from the International Lung Cancer Consortium. Carcinogenesis 2012, 33, 1059–1064. [Google Scholar] [CrossRef] [Green Version]
- Kazma, R.; Cardin, N.J.; Witte, J.S. Does Accounting for Gene-Environment Interactions Help Uncover Association between Rare Variants and Complex Diseases? Hum. Hered. 2012, 74, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Li, K.; Zhao, L.; Zou, H. DNA repair pathway genes and lung cancer susceptibility: A meta-analysis. Gene 2014, 538, 361–365. [Google Scholar] [CrossRef]
- Du, H.; Guo, N.; Shi, B.; Zhang, Q.; Chen, Z.; Lu, K.; Shu, Y.; Chen, T.; Zhu, L. The Effect of XPD Polymorphisms on Digestive Tract Cancers Risk: A Meta-Analysis. PLoS ONE 2014, 9, e96301. [Google Scholar] [CrossRef] [Green Version]
- Bartsch, H.; Nair, U.; Risch, A.; Rojas, M.; Wikman, H.; Alexandrov, K. Genetic polymorphism of CYP genes, alone or in combination, as a risk modifier of tobacco-related cancers. Cancer Epidemiol. Biomark. Prev. 2000, 9, 3–28. [Google Scholar]
- Ho, T.; Wei, Q.; Sturgis, E.M. Epidemiology of carcinogen metabolism genes and risk of squamous cell carcinoma of the head and neck. Head Neck 2007, 29, 682–699. [Google Scholar] [CrossRef] [PubMed]
- Morita, S.; Yano, M.; Tsujinaka, T.; Akiyama, Y.; Taniguchi, M.; Kaneko, K.; Miki, H.; Fujii, T.; Yoshino, K.; Kusuoka, H.; et al. Genetic polymorphisms of drug-metabolizing enzymes and susceptibility to head-and-neck squamous-cell carcinoma. Int. J. Cancer 1999, 80, 685–688. [Google Scholar] [CrossRef]
- Slaughter, D.P.; Southwick, H.W.; Smejkal, W. Field cancerization in oral stratified squamous epithelium; clinical implications of multicentric origin. Cancer 1953, 6, 963–968. [Google Scholar] [CrossRef]
- Liao, C.-T.; Kang, C.-J.; Chang, J.T.-C.; Wang, H.-M.; Ng, S.-H.; Hsueh, C.; Lee, L.-Y.; Lin, C.H.; Cheng, A.-J.; Chen, I.-H.; et al. Survival of second and multiple primary tumors in patients with oral cavity squamous cell carcinoma in the betel quid chewing area. Oral Oncol. 2007, 43, 811–819. [Google Scholar] [CrossRef]
- Ko, Y.-C.; Huang, Y.-L.; Lee, C.-H.; Chen, M.-J.; Lin, L.-M.; Tsai, C.-C. Betel quid chewing, cigarette smoking and alcohol consumption related to oral cancer in Taiwan. J. Oral Pathol. Med. 1995, 24, 450–453. [Google Scholar] [CrossRef]
- González-García, R.; Naval-Gías, L.; Román-Romero, L.; Sastre-Pérez, J.; Rodríguez-Campo, F.J. Local recurrences and second primary tumors from squamous cell carcinoma of the oral cavity: A retrospective analytic study of 500 patients. Head Neck 2009, 31, 1168–1180. [Google Scholar] [CrossRef]
- Chien, H.-T.; Young, C.-K.; Chen, T.-P.; Liao, C.-T.; Wang, H.-M.; Cheng, S.-D.; Huang, S.-F. Alcohol-metabolizing Enzymes’ Gene Polymorphisms and Susceptibility to Multiple Head and Neck Cancers. Cancer Prev. Res. 2019, 12, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.C.; Chow, C.C.; Tellier, L.C.A.M.; Vattikuti, S.; Purcell, S.M.; Lee, J.J. Second-generation PLINK: Rising to the challenge of larger and richer datasets. Gigascience 2015, 4, 7. [Google Scholar] [CrossRef] [PubMed]
- Purcell, S.; Chang, C. PLINK 1.90. Available online: https://www.cog-genomics.org/plink2/ (accessed on 16 May 2021).
- Potjer, T.P.; Van Der Grinten, T.W.J.; Lakeman, I.M.M.; Bollen, S.H.; Rodríguez-Girondo, M.; Iles, M.M.; Barrett, J.H.; Kiemeney, L.A.; Gruis, N.A.; Van Asperen, C.J.; et al. Association between a 46-SNP Polygenic Risk Score and melanoma risk in Dutch patients with familial melanoma. J. Med. Genet. 2020. [Google Scholar] [CrossRef]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its Associated Cutoff Point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef] [Green Version]
- Bongers, V.; Braakhuis, B.J.; Tobi, H.; Lubsen, H.; Snow, G.B. The relation between cancer incidence among relatives and the occurrence of multiple primary carcinomas following head and neck cancer. Cancer Epidemiol. Biomark. Prev. 1996, 5, 595–598. [Google Scholar]
- Bugter, O.; Van Iwaarden, D.L.; Dronkers, E.A.; De Herdt, M.J.; Wieringa, M.H.; Verduijn, G.M.; Mureau, M.A.; Hove, I.T.; Van Meerten, E.; Hardillo, J.A.; et al. Survival of patients with head and neck cancer with metachronous multiple primary tumors is surprisingly favorable. Head Neck 2019, 41, 1648–1655. [Google Scholar] [CrossRef] [PubMed]
- Braakhuis, B.J.; Tabor, M.P.; Leemans, C.R.; van der Waal, I.; Snow, G.B.; Brakenhoff, R.H. Second primary tumors and field cancerization in oral and oropharyngeal cancer: Molecular techniques provide new insights and definitions. Head Neck 2002, 24, 198–206. [Google Scholar] [CrossRef] [PubMed]
- MorrisAndrew, L.G.T.; Sikora, A.G.; Hayes, R.B.; Patel, S.G.; Ganly, I. Anatomic sites at elevated risk of second primary cancer after an index head and neck cancer. Cancer Causes Control 2011, 22, 671–679. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Liu, J.; Liang, X.; Chen, J.; Hong, J.; Li, L.; He, Q.; Cai, X. History and progression of Fat cadherins in health and disease. OncoTargets Ther. 2016, 9, 7337–7343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michmerhuizen, N.L.; Birkeland, A.C.; Bradford, C.R.; Brenner, J.C. Genetic determinants in head and neck squamous cell carcinoma and their influence on global personalized medicine. Genes Cancer 2016, 7, 182–200. [Google Scholar] [CrossRef] [Green Version]
- Tao, S.; Wang, Z.; Feng, J.; Hsu, F.-C.; Jin, G.; Kim, S.-T.; Zhang, Z.; Gronberg, H.; Zheng, L.S.; Isaacs, W.B.; et al. A genome-wide search for loci interacting with known prostate cancer risk-associated genetic variants. Carcinogenesis 2012, 33, 598–603. [Google Scholar] [CrossRef] [Green Version]
- Drummond, J.B.; Tucholski, J.; Haroutunian, V.; Meador-Woodruff, J.H. Transmembrane AMPA receptor regulatory protein (TARP) dysregulation in anterior cingulate cortex in schizophrenia. Schizophr. Res. 2013, 147, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Di Credico, G.; Polesel, J.; Dal Maso, L.; Pauli, F.; Torelli, N.; Luce, D.; Radoï, L.; Matsuo, K.; Serraino, D.; Brennan, P.; et al. Alcohol drinking and head and neck cancer risk: The joint effect of intensity and duration. Br. J. Cancer 2020, 123, 1456–1463. [Google Scholar] [CrossRef] [PubMed]
- Eng, M.Y.; Luczak, S.E.; Wall, T.L. ALDH2, ADH1B, and ADH1C Genotypes in Asians: A Literature Review. Alcohol Res. Health J. Natl. Inst. Alcohol Abus. Alcohol. 2007, 30, 22–27. [Google Scholar]
- Jeon, J.-H.; Kim, M.G.; Park, J.Y.; Lee, J.H.; Kim, M.J.; Myoung, H.; Choi, S.W. Analysis of the outcome of young age tongue squamous cell carcinoma. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 41. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-T.; Wang, H.-M.; Hsieh, L.-L.; Chang, J.T.-C.; Ng, S.-H.; Hsueh, C.; Lee, L.-Y.; Lin, C.H.; Chen, I.-H.; Kang, C.-J.; et al. Higher distant failure in young age tongue cancer patients. Oral Oncol. 2006, 42, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Fang, Q.; Guo, S. A comparison of oral squamous cell carcinoma between young and old patients in a single medical center in China. Int. J. Clin. Exp. Med. 2015, 8, 12418–12423. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Cancer Patients [n (%)] | Normal Patients [n (%)] | p Value |
|---|---|---|---|
| Age (±S.D.) | 52.58 (±10.92) | 43.66 (±15.67) | |
| Range | 25–88 | 18–99 | |
| Tumor subsites | |||
| Oral cavity cancer | 364 (51.1) | ||
| Oropharynx | 135 (19.0) | ||
| Hypopharynx | 190 (29.7) | ||
| Larynx | 14 (0.2) | ||
| Nasal cavity | 2 (0.3) | ||
| Skin | 1 (0.1) | ||
| Esophagus | 6 (0.8) | ||
| Gender | |||
| Male | 707 (99.3) | 398 (100.0) | 0.168 * |
| Female 1 | 5 (0.7) | 0 (0) | |
| Alcohol drinking | |||
| Yes | 481(79.9) | 264 (66.3) | <0.001 |
| No | 121(20.1) | 134 (33.7) | |
| AQ chewing | |||
| Yes | 498 (82.6) | 82 (20.6) | <0.001 |
| No | 105 (17.4) | 316 (79.4) | |
| Cigarette smoking | |||
| Yes | 549 (91.0) | 228 (57.3) | <0.001 |
| No | 54 (9.0) | 170 (42.7) | |
| Number of malignances | |||
| Single primary | 426 (59.8) | ||
| Multiple primary tumors | 286 (40.2) | ||
| Multiple oral cavity cancers | 111 (38.8) | ||
| Multiple upper aerodigestive tract MPTs | 120 (42.0) | ||
| Non-oral and non-aerodigestive tract MPTs | 55 (19.2) |
| CHR | SNP | Minor Allele | Frequency (ADT) | Frequency (Oral Cancer) | Major Allele | Frequency (Normal Population) |
|---|---|---|---|---|---|---|
| 1 | rs118169127 | C | 0.088 | 0.02181 | T | 0.06675 |
| 2 | rs112433986 | - | 0.024 | 0.0755 | A | 0.08629 |
| 5 | rs848 | A | 0.4355 | 0.3138 | C | 0.2834 |
| 6 | rs79454125 | C | 0.024 | 0.07191 | T | 0.04672 |
| 6 | rs9490776 | A | 0.02846 | 0.09532 | G | 0.1083 |
| 7 | rs76367287 | C | 0.124 | 0.04849 | A | 0.09068 |
| 9 | rs141057871 | A | 0.2195 | 0.1221 | G | 0.1322 |
| 9 | rs7847271 | A | 0.04 | 0.1271 | G | 0.07305 |
| 10 | rs11255400 | A | 0.028 | 0.08361 | G | 0.03526 |
| 11 | rs12797844 | C | 0.02016 | 0.06376 | T | 0.02519 |
| 11 | rs7129229 | T | 0.2358 | 0.1421 | A | 0.1344 |
| 13 | rs9554264 | T | 0.348 | 0.2258 | C | 0.306 |
| 14 | rs1959792 | T | 0.2621 | 0.151 | C | 0.1679 |
| 16 | rs61401220 | - | 0.108 | 0.04348 | T | 0.03914 |
| 17 | rs9897457 | C | 0.148 | 0.2559 | T | 0.1856 |
| 17 | rs3760265 | T | 0.188 | 0.09866 | C | 0.154 |
| 19 | Affx-15929578 (rs28933396) | A | 0.03361 | 0.1747 | G | 0 |
| 23 | rs149089400 | A | 0.08 | 0.01974 | G | 0.01741 |
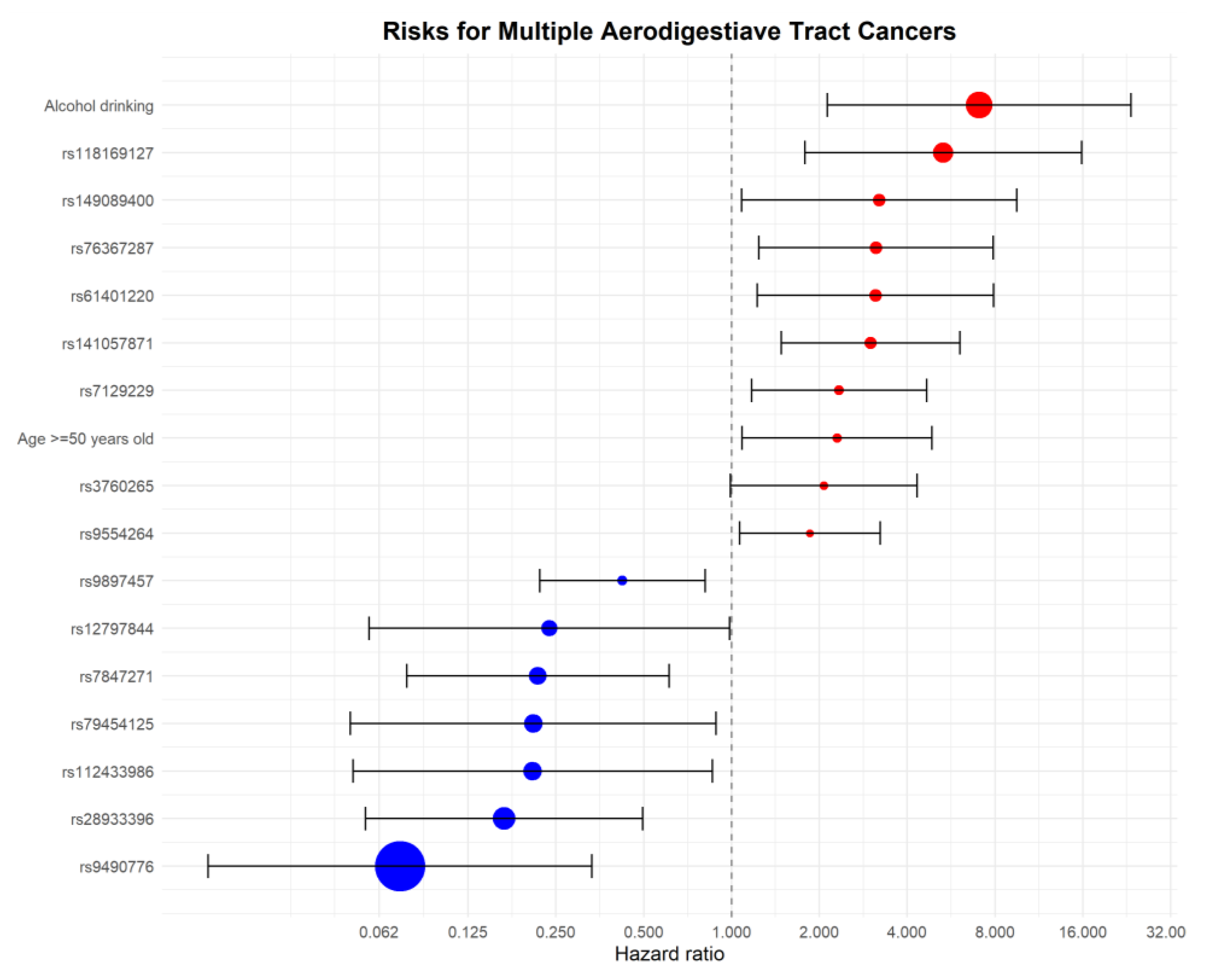
| Name | β | p Value | Hazard Ratio (95% Confidence Interval) |
|---|---|---|---|
| Alcohol drinking | 1.956 | 0.001 | 7.071 (2.134–23.434) |
| rs118169127 | 1.671 | 0.003 | 5.320 (1.785–15.854) |
| rs149089400 | 1.165 | 0.036 | 3.206 (1.082–9.500) |
| rs76367287 | 1.139 | 0.016 | 3.123 (1.239–7.874) |
| rs61401220 | 1.137 | 0.017 | 3.117 (1.227–7.921) |
| rs141057871 | 1.098 | 0.002 | 2.998 (1.482–6.062) |
| rs7129229 | 0.849 | 0.016 | 2.336 (1.170–4.665) |
| Age ≥ 50 years old | 0.834 | 0.029 | 2.302 (1.088–4.868) |
| rs3760265 | 0.728 | 0.053 | 2.071 (0.990–4.332) |
| rs9554264 | 0.618 | 0.029 | 1.856 (1.066–3.230) |
| rs9897457 | −0.862 | 0.010 | 0.422 (0.220–0.812) |
| rs12797844 | −1.437 | 0.048 | 0.238 (0.057–0.985) |
| rs7847271 | −1.529 | 0.004 | 0.217 (0.077–0.610) |
| rs79454125 | −1.566 | 0.034 | 0.209 (0.049–0.886) |
| rs112433986 | −1.570 | 0.030 | 0.208 (0.050–0.858) |
| rs28933396 | −1.795 | 0.001 | 0.166 (0.056–0.496) |
| rs9490776 | −2.617 | 0.001 | 0.073 (0.016–0.332) |
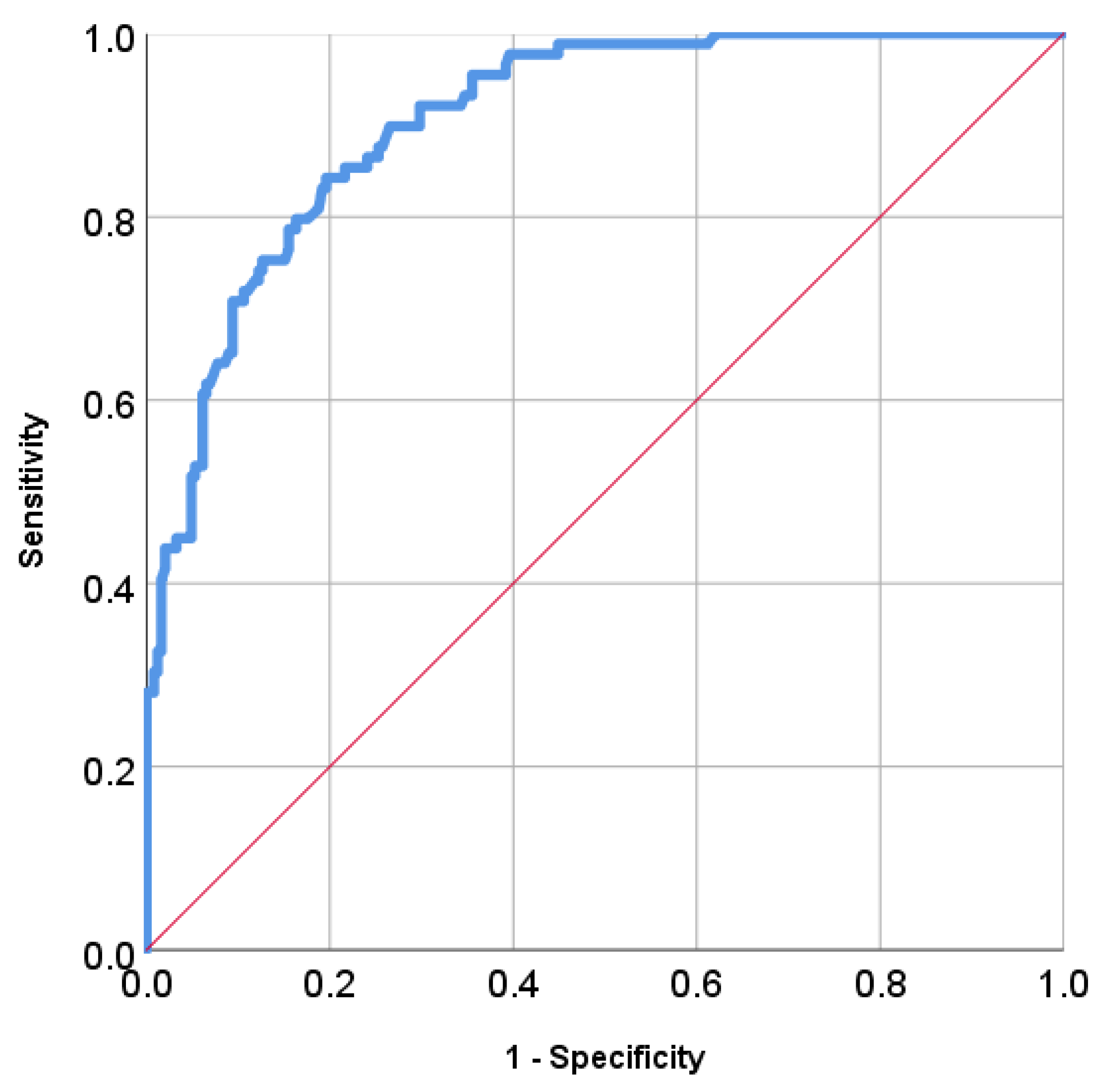
| Positive if Greater than or Equal to | Sensitivity | 1—Specificity | Specificity | Youden Index (Sensitivity + Specificity − 1) |
|---|---|---|---|---|
| −7.655000 | 1.000 | 1.000 | 0.000 | 0.000 |
| −6.304500 | 1.000 | 0.996 | 0.004 | 0.004 |
| −5.194500 | 1.000 | 0.988 | 0.012 | 0.012 |
| −4.094000 | 1.000 | 0.967 | 0.033 | 0.033 |
| −3.065500 | 1.000 | 0.902 | 0.098 | 0.098 |
| −2.113000 | 1.000 | 0.853 | 0.147 | 0.147 |
| −1.190000 | 1.000 | 0.763 | 0.237 | 0.237 |
| −0.100500 | 1.000 | 0.653 | 0.347 | 0.347 |
| 0.106000 | 0.989 | 0.584 | 0.416 | 0.405 |
| 1.101500 | 0.955 | 0.380 | 0.620 | 0.575 |
| 2.100000 | 0.865 | 0.241 | 0.759 | 0.624 |
| 2.353000 | 0.843 | 0.208 | 0.792 | 0.635 |
| 2.364500 | 0.843 | 0.204 | 0.796 | 0.639 |
| 2.390500 | 0.843 | 0.200 | 0.800 | 0.643 |
| 2.426500 | 0.843 | 0.196 | 0.804 | 0.647 |
| 2.486500 | 0.831 | 0.196 | 0.804 | 0.636 |
| 2.539500 | 0.831 | 0.192 | 0.808 | 0.640 |
| 2.560000 | 0.809 | 0.188 | 0.812 | 0.621 |
| 3.046500 | 0.742 | 0.122 | 0.878 | 0.619 |
| 4.092000 | 0.438 | 0.033 | 0.967 | 0.406 |
| 5.108500 | 0.213 | 0.000 | 1.000 | 0.213 |
| 6.067000 | 0.090 | 0.000 | 1.000 | 0.090 |
| 8.356000 | 0.011 | 0.000 | 1.000 | 0.011 |
| 9.973000 | 0.000 | 0.000 | 1.000 | 0.000 |
| CHR | SNP | A1 | A2 | MAF | Position | ENST No. | Genes | |
|---|---|---|---|---|---|---|---|---|
| 1 | rs118169127 | C | T | 0.05116 | p13.2 | ENST00000369732 | OVGP1//oviductal glycoprotein 1 | Downstream |
| 2 | rs112433986 | - | A | 0.06891 | q35 | ENST00000273067 | MARCH4//membrane associated ring finger 4 | Intron |
| 5 | rs848 | A | C | 0.3199 | q31.1 | ENST00000304506 | IL13//interleukin 13 | UTR-3 |
| 6 | rs79454125 | C | T | 0.06208 | q14.1 | ENST00000306270 | IBTK//inhibitor of Bruton agammaglobulinemia tyrosine kinase | Upstream |
| 6 | rs9490776 | A | G | 0.08999 | q22.31 | ENST00000334268 | TRDN//triadin | Intron |
| 7 | rs76367287 | C | A | 0.07755 | q36.3 | ENST00000444158 | uncharacterized LOC101927914 | |
| 9 | rs141057871 | A | G | 0.1576 | p22.3 | ENST00000422223 | FREM1//FRAS1 related extracellular matrix 1 | Upstream |
| 9 | rs7847271 | A | G | 0.09111 | q33.1 | ENST00000341037 | TNC//tenascin C | Intron |
| 10 | rs11255400 | A | G | 0.05518 | p14 | ENST00000344293 | TAF3//TATA box binding protein associated factor 3 | Intron |
| 11 | rs12797844 | C | T | 0.03587 | q13.3 | ENST00000253925 | PPFIA1//protein tyrosine phosphatase, receptor type, f polypeptide (PTPRF), interacting protein (liprin), alpha 1 | Upstream |
| 11 | rs7129229 | T | A | 0.1602 | q14.3 | ENST00000409404 | FAT3//FAT atypical cadherin 3 | Intron |
| 13 | rs9554264 | T | C | 0.2733 | q12.2 | ENST00000241453 | FLT3//fms-related tyrosine kinase 3 | Upstream |
| 14 | rs1959792 | T | C | 0.1858 | q12 | ENST00000546412 | STXBP6//syntaxin binding protein 6 (amisyn) | Upstream intron |
| 16 | rs61401220 | - | T | 0.05045 | q12.1 | ENST00000563826 | LOC101927334 | |
| 17 | rs9897457 | C | T | 0.2128 | p13.1 | ENST00000330767 | TMEM95//transmembrane protein 95 | Downstream |
| 17 | rs3760265 | T | C | 0.1295 | q24.2 | ENST00000533854 | CACNG5//calcium channel, voltage-dependent, gamma subunit 5 | Intron |
| 19 | rs28933396 | A | G | 0.04921 | q13.2 | ENST00000355481 | RYR1//ryanodine receptor 1 (skeletal) | Missense |
| 23 | rs149089400 | A | G | 0.0293 | q27.3 | ENST00000423667 | SPANXN2//SPANX family, member N2 | Upstream intron |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chien, H.-T.; Yeh, C.-C.; Young, C.-K.; Chen, T.-P.; Liao, C.-T.; Wang, H.-M.; Cho, K.-L.; Huang, S.-F. Polygenic Panels Predicting the Susceptibility of Multiple Upper Aerodigestive Tract Cancer in Oral Cancer Patients. J. Pers. Med. 2021, 11, 425. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050425
Chien H-T, Yeh C-C, Young C-K, Chen T-P, Liao C-T, Wang H-M, Cho K-L, Huang S-F. Polygenic Panels Predicting the Susceptibility of Multiple Upper Aerodigestive Tract Cancer in Oral Cancer Patients. Journal of Personalized Medicine. 2021; 11(5):425. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050425
Chicago/Turabian StyleChien, Huei-Tzu, Chi-Chin Yeh, Chi-Kuang Young, Tzu-Ping Chen, Chun-Ta Liao, Hung-Ming Wang, Kai-Lun Cho, and Shiang-Fu Huang. 2021. "Polygenic Panels Predicting the Susceptibility of Multiple Upper Aerodigestive Tract Cancer in Oral Cancer Patients" Journal of Personalized Medicine 11, no. 5: 425. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050425