
Concurrent Chemoradiation in Anal Cancer Patients Delivered with Bone Marrow-Sparing IMRT: Final Results of a Prospective Phase II Trial

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Study Design and Sample Size Determination
2.3. Radiotherapy Protocol
2.4. Bone Marrow Segmentation
2.5. Planning Process and Delivery
2.6. Chemotherapy
2.7. Toxicity Evaluation and Clinical Assessment
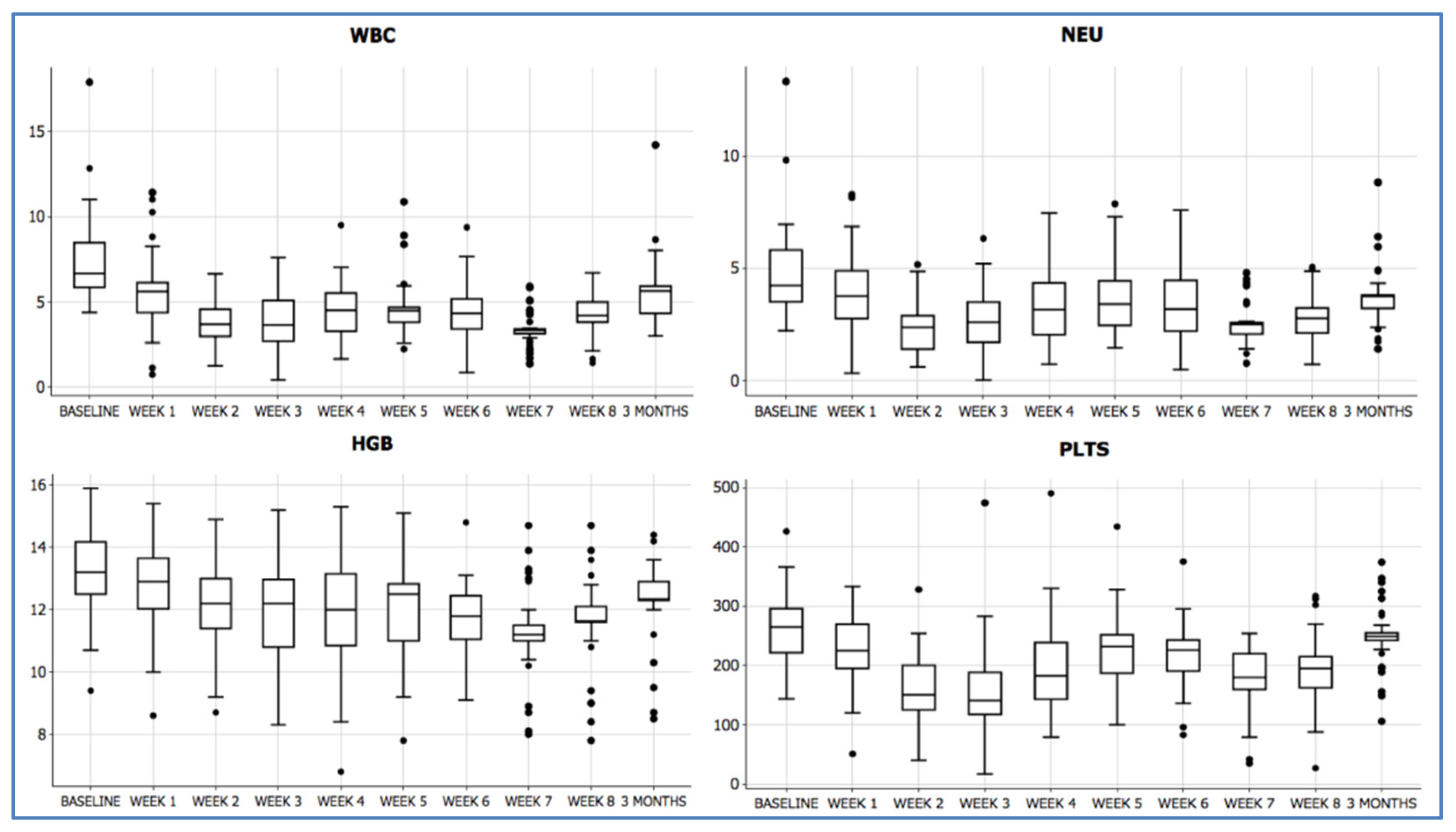
2.8. Hematologic Toxicity Evaluation
2.9. Statistical Analysis
3. Results
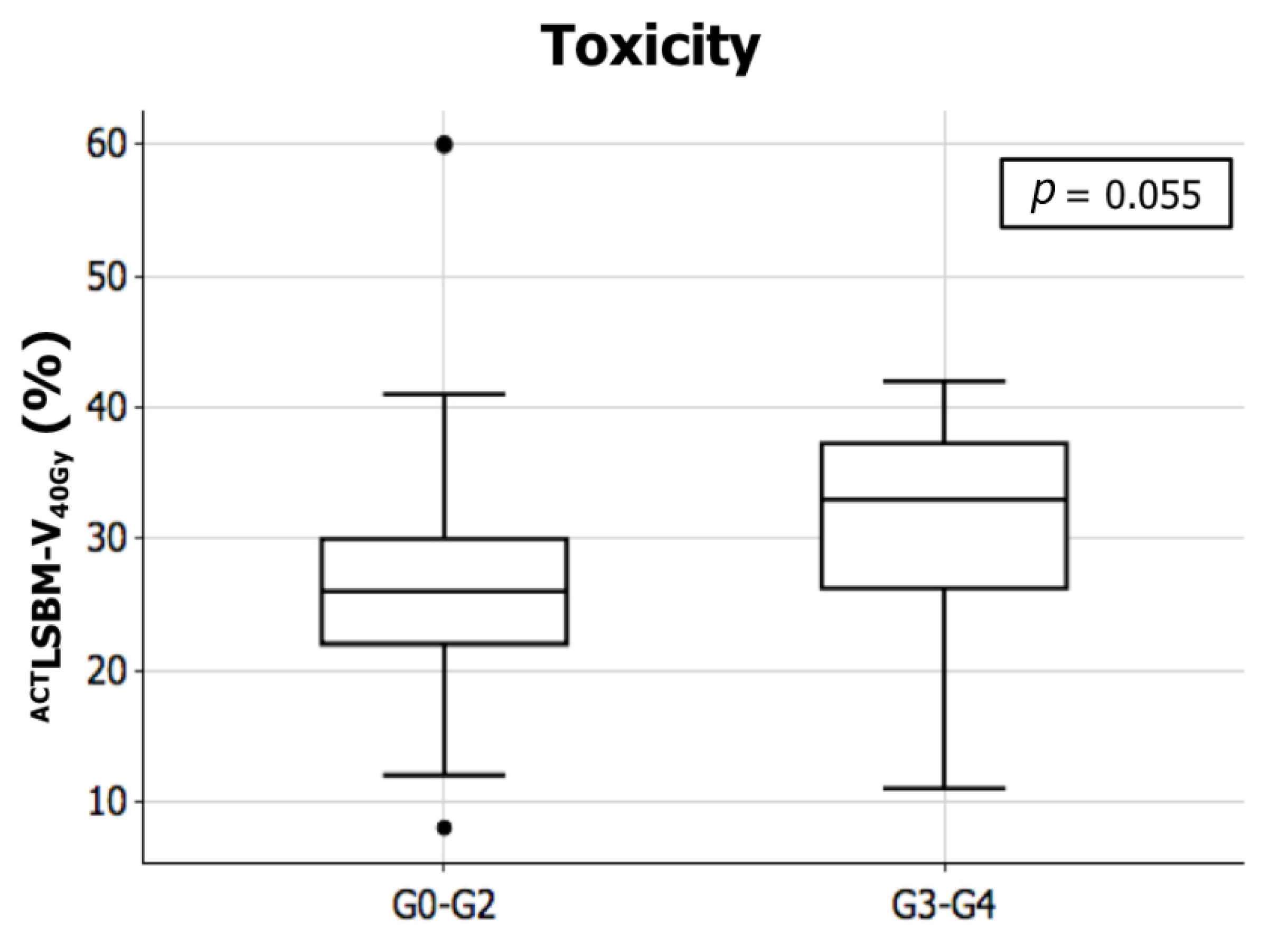
3.1. Acute Hematologic Toxicity and Dosimetric Outcomes
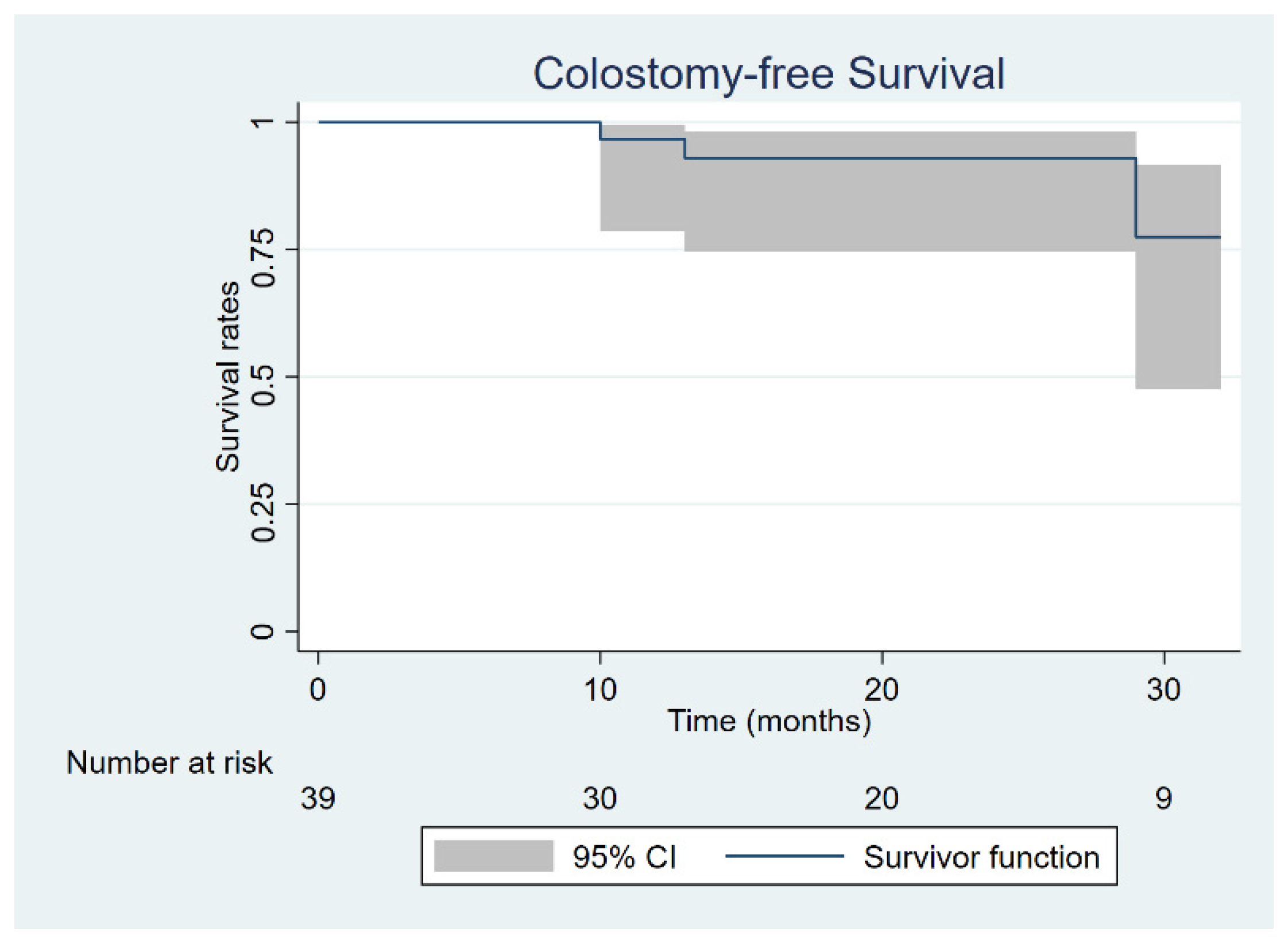
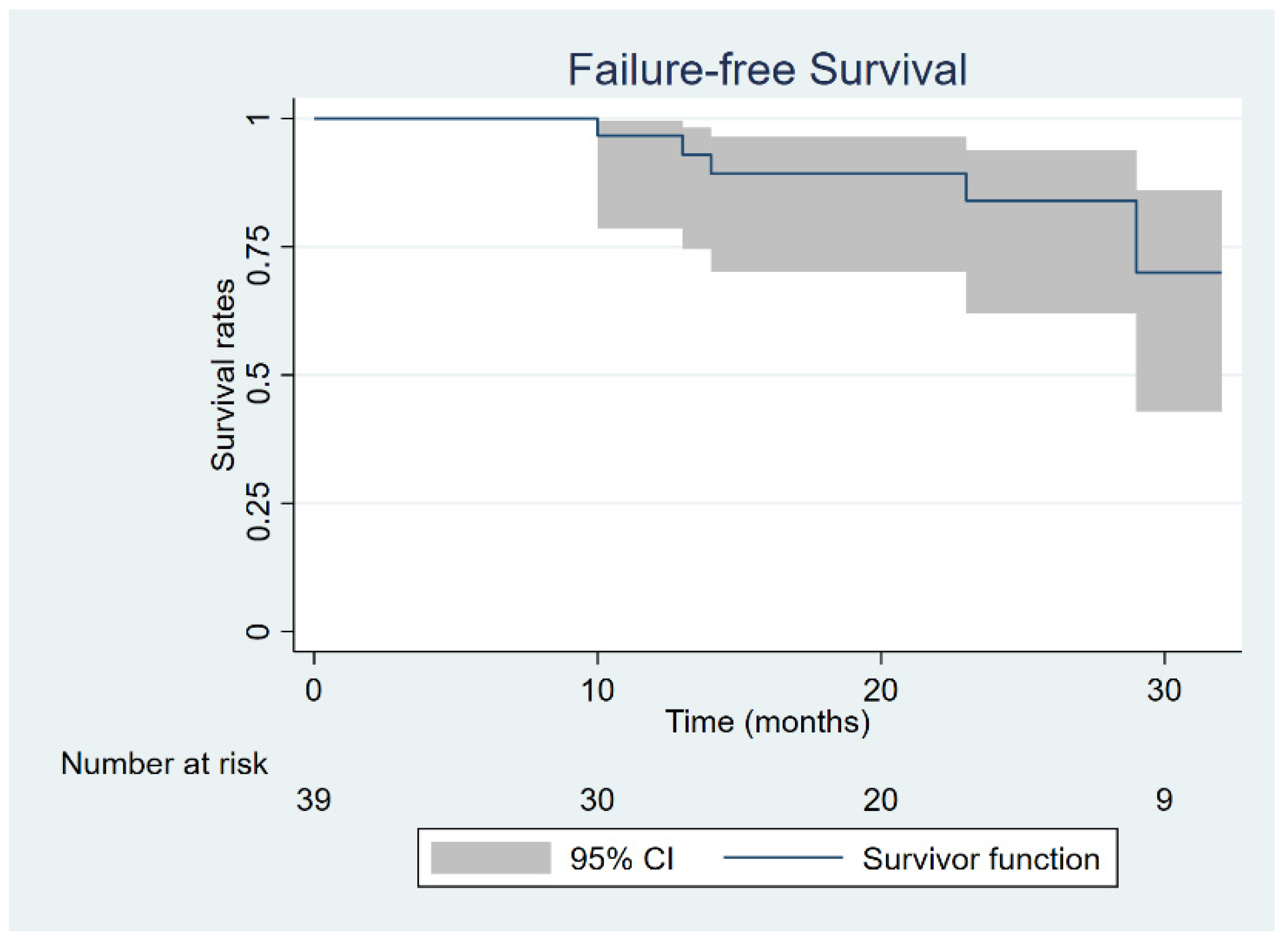
3.2. Oncological Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- James, R.D.; Glynne-Jones, R.; Meadows, H.M.; Cunningham, D.; Myint, A.S.; Saunders, M.P.; Maughan, T.; McDonald, A.; Essapen, S.; Leslie, M.; et al. Mitomycin or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous-cell carcinoma of the anus (ACT II): A randomised, phase 3, open-label, 2 × 2 factorial trial. Lancet Oncol. 2013, 14, 516–524. [Google Scholar] [CrossRef]
- Franco, P.; Mistrangelo, M.; Arcadipane, F.; Munoz, F.; Sciacero, P.; Spadi, R.; Migliaccio, F.; Angelini, V.; Bombaci, S.; Rondi, N.; et al. Intensity-Modulated Radiation Therapy with Simultaneous Integrated Boost Combined with Concurrent Chemotherapy for the Treatment of Anal Cancer Patients: 4-Year Results of a Consecutive Case Series. Cancer Investig. 2015, 33, 259–266. [Google Scholar] [CrossRef] [Green Version]
- Glynne-Jones, R.; Sebag-Montefiore, D.; Adams, R.; McDonald, A.; Gollins, S.; James, R.; Northover, J.M.; Meadows, H.M.; Jitlal, M. “Mind the Gap”—The Impact of Variations in the Duration of the Treatment Gap and Overall Treatment Time in the First UK Anal Cancer Trial (ACT I). Int. J. Radiat. Oncol. 2011, 81, 1488–1494. [Google Scholar] [CrossRef]
- Franco, P.; Arcadipane, F.; Ragona, R.; Mistrangelo, M.; Cassoni, P.; Racca, P.; Morino, M.; Numico, G.; Ricardi, U. Hematologic toxicity in anal cancer patients during combined chemo-radiation: A radiation oncologist perspective. Expert Rev. Anticancer Ther. 2017, 17, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Ajani, J.A.; Winter, K.A.; Gunderson, L.L.; Pedersen, J.; Benson, A.B.; Thomas, C.R.; Mayer, R.J.; Haddock, M.G.; Rich, T.A.; Willett, C. Fluorouracil, Mitomycin, and Radiotherapy vs. Fluorouracil, Cisplatin, and Radiotherapy for Carcinoma of the Anal Canal. JAMA 2008, 299, 1914–1921. [Google Scholar] [CrossRef]
- Kachnic, L.A.; Winter, K.; Myerson, R.J.; Goodyear, M.D.; Willins, J.; Esthappan, J.; Haddock, M.G.; Rotman, M.; Parikh, P.J.; Safran, H.; et al. RTOG 0529: A Phase 2 Evaluation of Dose-Painted Intensity Modulated Radiation Therapy in Combination With 5-Fluorouracil and Mitomycin-C for the Reduction of Acute Morbidity in Carcinoma of the Anal Canal. Int. J. Radiat. Oncol. 2013, 86, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mell, L.K.; Schomas, D.A.; Salama, J.K.; Devisetty, K.; Aydogan, B.; Miller, R.C.; Jani, A.B.; Kindler, H.L.; Mundt, A.J.; Roeske, J.C.; et al. Association Between Bone Marrow Dosimetric Parameters and Acute Hematologic Toxicity in Anal Cancer Patients Treated With Concurrent Chemotherapy and Intensity-Modulated Radiotherapy. Int. J. Radiat. Oncol. 2008, 70, 1431–1437. [Google Scholar] [CrossRef]
- Cheng, J.C.-H.; Bazan, J.G.; Wu, J.-K.; Koong, A.C.; Chang, D.T. Lumbosacral spine and marrow cavity modeling of acute hematologic toxicity in patients treated with intensity modulated radiation therapy for squamous cell carcinoma of the anal canal. Pract. Radiat. Oncol. 2014, 4, 198–206. [Google Scholar] [CrossRef]
- Franco, P.; Ragona, R.; Arcadipane, F.; Mistrangelo, M.; Cassoni, P.; Rondi, N.; Morino, M.; Racca, P.; Ricardi, U. Dosimetric predictors of acute hematologic toxicity during concurrent intensity-modulated radiotherapy and chemotherapy for anal cancer. Clin. Transl. Oncol. 2017, 19, 67–75. [Google Scholar] [CrossRef]
- Rose, B.S.; Jee, K.-W.; Niemierko, A.; Murphy, J.E.; Blaszkowsky, L.S.; Allen, J.N.; Lee, L.K.; Wang, Y.; Drapek, L.C.; Hong, T.S.; et al. Irradiation of FDG-PET–Defined Active Bone Marrow Subregions and Acute Hematologic Toxicity in Anal Cancer Patients Undergoing Chemoradiation. Int. J. Radiat. Oncol. 2016, 94, 747–754. [Google Scholar] [CrossRef]
- Franco, P.; Arcadipane, F.; Ragona, R.; Lesca, A.; Gallio, E.; Mistrangelo, M.; Cassoni, P.; Arena, V.; Bustreo, S.; Faletti, R.; et al. Dose to specific subregions of pelvic bone marrow defined with FDG-PET as a predictor of hematologic nadirs during concomitant chemoradiation in anal cancer patients. Med. Oncol. 2016, 33, 72. [Google Scholar] [CrossRef]
- Arcadipane, F.; Silvetti, P.; Olivero, F.; Gastino, A.; De Luca, V.; Mistrangelo, M.; Cassoni, P.; Racca, P.; Gallio, E.; Lesca, A.; et al. Bone Marrow-Sparing IMRT in Anal Cancer Patients Undergoing Concurrent Chemo-Radiation: Results of the First Phase of a Prospective Phase II Trial. Cancers 2020, 12, 3306. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th Edition of the AJCC Cancer Staging Manual and the Future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Simon, R. Optimal two-stage designs for phase II clinical trials. Control. Clin. Trials 1989, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Franco, P.; Arcadipane, F.; Ragona, R.; Mistrangelo, M.; Cassoni, P.; Munoz, F.; Rondi, N.; Morino, M.; Racca, P.; Ricardi, U. Volumetric modulated arc therapy (VMAT) in the combined modality treatment of anal cancer patients. Br. J. Radiol. 2016, 89, 20150832. [Google Scholar] [CrossRef] [Green Version]
- Myerson, R.J.; Garofalo, M.C.; El Naqa, I.; Abrams, R.A.; Apte, A.; Bosch, W.R.; Das, P.; Gunderson, L.L.; Hong, T.S.; Kim, J.J.; et al. Elective Clinical Target Volumes for Conformal Therapy in Anorectal Cancer: A Radiation Therapy Oncology Group Consensus Panel Contouring Atlas. Int. J. Radiat. Oncol. 2009, 74, 824–830. [Google Scholar] [CrossRef] [Green Version]
- Ng, M.; Leong, T.; Chander, S.; Chu, J.; Kneebone, A.; Carroll, S.; Wiltshire, K.; Ngan, S.; Kachnic, L. Australasian Gastrointestinal Trials Group (AGITG) Contouring Atlas and Planning Guidelines for Intensity-Modulated Radiotherapy in Anal Cancer. Int. J. Radiat. Oncol. 2012, 83, 1455–1462. [Google Scholar] [CrossRef]
- Arcadipane, F.; Franco, P.; Ceccarelli, M.; Furfaro, G.; Rondi, N.; Trino, E.; Martini, S.; Iorio, G.C.; Mistrangelo, M.; Cassoni, P.; et al. Image-guided IMRT with simultaneous integrated boost as per RTOG 0529 for the treatment of anal cancer. Asia-Pac. J. Clin. Oncol. 2018, 14, 217–223. [Google Scholar] [CrossRef]
- Mell, L.K.; Kochanski, J.D.; Roeske, J.C.; Haslam, J.J.; Mehta, N.; Yamada, S.D.; Hurteau, J.A.; Collins, Y.C.; Lengyel, E.; Mundt, A.J. Dosimetric predictors of acute hematologic toxicity in cervical cancer patients treated with concurrent cisplatin and intensity-modulated pelvic radiotherapy. Int. J. Radiat. Oncol. 2006, 66, 1356–1365. [Google Scholar] [CrossRef]
- Franco, P.; Ragona, R.; Arcadipane, F.; Mistrangelo, M.; Cassoni, P.; Rondi, N.; Morino, M.; Racca, P.; Ricardi, U. Lumbar-sacral bone marrow dose modeling for acute hematological toxicity in anal cancer patients treated with concurrent chemo-radiation. Med. Oncol. 2016, 33, 137. [Google Scholar] [CrossRef]
- Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. Available online: www.evs.nci.nih.gov (accessed on 12 December 2020).
- UKCCCR Anal Cancer Trial Working Party; UK Co-Ordination Committee on Cancer Research. Epidermoid anal cancer: Results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. Lancet 1996, 348, 1049–1054. [Google Scholar] [CrossRef]
- Bartelink, H.; Roelofsen, F.; Eschwege, F.; Rougier, P.; Bosset, J.F.; Gonzalez, D.G.; Peiffert, D.; Van Glabbeke, M.; Pierart, M. Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: Results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups. J. Clin. Oncol. 1997, 15, 2040–2049. [Google Scholar] [CrossRef] [PubMed]
- Flam, M.; John, M.; Pajak, T.F.; Petrelli, N.; Myerson, R.; Doggett, S.; Quivey, J.; Rotman, M.; Kerman, H.; Coia, L.; et al. Role of mitomycin in combination with fluorouracil and radiotherapy, and of salvage chemoradiation in the definitive nonsurgical treatment of epidermoid carcinoma of the anal canal: Results of a phase III randomized intergroup study. J. Clin. Oncol. 1996, 14, 2527–2539. [Google Scholar] [CrossRef]
- White, E.C.; Goldman, K.; Aleshin, A.; Lien, W.W.; Rao, A.R. Chemoradiotherapy for squamous cell carcinoma of the anal canal: Comparison of one versus two cycles mitomycin-C. Radiother. Oncol. 2015, 117, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Mell, L.K.; Sirák, I.; Wei, L.; Tarnawski, R.; Mahantshetty, U.; Yashar, C.M.; McHale, M.T.; Xu, R.; Honerkamp-Smith, G.; Carmona, R.; et al. Bone Marrow-sparing Intensity Modulated Radiation Therapy With Concurrent Cisplatin For Stage IB-IVA Cervical Cancer: An International Multicenter Phase II Clinical Trial (INTERTECC-2). Int. J. Radiat. Oncol. 2017, 97, 536–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuire, S.M.; Menda, Y.; Ponto, L.L.B.; Gross, B.; TenNapel, M.; Smith, B.J.; Bayouth, J.E. Spatial mapping of functional pelvic bone marrow using FLT PET. J. Appl. Clin. Med. Phys. 2014, 15, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Franco, P.; Fiandra, C.; Arcadipane, F.; Trino, E.; Giglioli, F.R.; Ragona, R.; Ricardi, U. Incorporating 18FDG-PET-defined pelvic active bone marrow in the automatic treatment planning process of anal cancer patients undergoing chemo-radiation. BMC Cancer 2017, 17, 710. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N (%) |
|---|---|
| Age | |
| Mean | 64 |
| Range | 29–81 |
| Gender | |
| Female | 30 (77) |
| Male | 9 (23) |
| HIV status | |
| Positive | 2 (5) |
| Negative | 37(95) |
| Primary tumor site | |
| Anal canal | 35 (90) |
| Anal margin | 1 (2) |
| Both | 3 (8) |
| T-stage | |
| T1 | 4 (10) |
| T2 | 15 (38) |
| T3 | 14 (36) |
| T4 | 6 (15) |
| N-stage | |
| N0 | 19 (49) |
| N1 | 20 (51) |
| Global stage | |
| I | 3 (8) |
| IIA | 12 (31) |
| IIB | 4 (10) |
| IIIA | 6 (15) |
| IIIB | 1 (3) |
| IIIC | 13 (33) |
| Grading | |
| G1 | 5 (13) |
| G2 | 10 (26) |
| G3 | 11 (28) |
| NA | 13 (33) |
| Variable | N (%) |
|---|---|
| IMRT approach | |
| Single-arc | 3 (8) |
| Dual-arc | 36 (92) |
| PTV dose-tumor (Gy) | |
| 54 Gy/30 fractions | 36 (92) |
| 50.4 Gy/28 fractions | 3 (8) |
| PTV dose-positive nodes (Gy) 20 pts | |
| 54 Gy/30 fractions | 8 (40) |
| 50.4 Gy/30 fractions | 12 (60) |
| PTV dose-negative nodes (Gy) | |
| 45 Gy/30 fractions | 36 (92) |
| 42 Gy/30 fractions | 3 (8) |
| Chemotherapy | |
| 5-FU + MMC | 39 (100) |
| Cycles | |
| 1 | 2 (5) |
| 2 | 37(95) |
| Chemotherapy dose reduction | |
| Yes | 3 (8) |
| No | 36 (92) |
| RT duration (days) | |
| Mean | 45 |
| Range | 37–77 |
| Acute Toxicity | G0 | G1 | G2 | G3 | G4 |
|---|---|---|---|---|---|
| Skin | 0 (0) | 9 (23) | 23 (59) | 7 (18) | 0 (0) |
| Gastrointestinal | 7 (18) | 13 (33) | 19 (49) | 0 (0) | 0 (0) |
| Urinary | 11 (28) | 19 (49) | 9 (23) | 0 (0) | 0 (0) |
| Genitalia | 12 (31) | 16 (41) | 10 (26) | 1 (3) | 0 (0) |
| Anemia | 22 (56) | 9 (23) | 7 (18) | 1 (3) | 0 (0) |
| Leukopenia | 4 (10) | 11 (28) | 16 (41) | 4 (10) | 4 (10) |
| Neutropenia | 14 (36) | 7 (18) | 8 (21) | 6 (15) | 4 (10) |
| Thrombocytopenia | 26 (67) | 8 (21) | 1 (3) | 3 (8) | 1 (3) |
| PTV | |||
| mean | SD | ||
| PTV-tumor | D98 (Gy)-50.4Gy | 48.0 | 1.0 |
| D2 (Gy)-50.4Gy | 53.0 | 2.0 | |
| D98 (Gy)-54Gy | 51.2 | 1.8 | |
| D2 (Gy)-54Gy | 57.1 | 1.2 | |
| V95 (%) | 95.5 | 3.6 | |
| V107 (%) | 1.6 | 1.5 | |
| PTV-elective volumes | D98 (Gy)-42Gy | 48 | 0 |
| D2 (Gy)-42Gy | 54 | 0 | |
| D98 (Gy)-45Gy | 50.2 | 2.44 | |
| D2 (Gy)-45Gy | 57.55 | 1.36 | |
| V95 (%) | 91.45 | 8.61 | |
| V107 (%) | 2.66 | 2.81 | |
| OARs | |||
| mean | SD | ||
| Bladder | V30 (%) | 40.3 | 13.2 |
| V40 (%) | 19.3 | 13.1 | |
| V50 (%) | 4.5 | 9.3 | |
| D2(Gy) | 47.3 | 4.8 | |
| Mean dose (Gy) | 27.8 | 4.5 | |
| Bowel | V30 (cc) | 198.1 | 94.8 |
| V35 (cc) | 145.6 | 88.1 | |
| V40 (cc) | 19.2 | 32.7 | |
| V45 (cc) | 9.3 | 36.3 | |
| D2(Gy) | 44.3 | 3.0 | |
| Mean dose (Gy) | 20.4 | 12.1 | |
| External genitalia | V20 (%) | 40.8 | 25.5 |
| V30 (%) | 29.5 | 22.6 | |
| V40 (%) | 15.3 | 18.4 | |
| D2(Gy) | 49.4 | 11.9 | |
| Mean dose (Gy) | 23.3 | 11.1 | |
| Femural heads | V30 (%) | 10.8 | 8.3 |
| V40 (%) | 2.4 | 4.5 | |
| V45 (%) | 0.8 | 3.4 | |
| V50 (%) | 0.5 | 3.2 | |
| D2(Gy) | 36.6 | 7.6 | |
| Mean dose (Gy) | 17.5 | 8.8 | |
| Structure | Structure | ||||||
|---|---|---|---|---|---|---|---|
| Parameter | Mean | SD | Parameter | Mean | SD | ||
| ACTPBM | Dmean(Gy) | 23.6 | 4.1 | ACTIBM | Dmean(Gy) | 19.9 | 4.13 |
| V5 | 94.1 | 8.1 | V5 | 93.8 | 7.8 | ||
| V10 | 81.8 | 12.1 | V10 | 77.1 | 12.7 | ||
| V15 | 68.1 | 15.1 | V15 | 66.4 | 15.9 | ||
| V20 | 55.6 | 15.1 | V20 | 44.8 | 16.3 | ||
| V30 | 33.9 | 11.1 | V30 | 20.2 | 11.8 | ||
| V40 | 15.4 | 6.4 | V40 | 6.4 | 5.7 | ||
| V45 | 4.1 | 3.4 | V45 | 1.3 | 2.6 | ||
| V50 | 0.5 | 1.1 | V50 | 0.1 | 0.4 | ||
| ACTLSBM | Dmean(Gy) | 29.7 | 11.8 | ACTLPBM | Dmean (Gy) | 24.5 | 5.8 |
| V5 | 95.22 | 7.8 | V5 | 96.6 | 8.8 | ||
| V10 | 89.2 | 11.3 | V10 | 85.9 | 15.9 | ||
| V15 | 81.5 | 13.9 | V15 | 70.5 | 21.2 | ||
| V20 | 72.8 | 14.2 | V20 | 57.3 | 21.1 | ||
| V30 | 52.8 | 12.7 | V30 | 35.0 | 16.2 | ||
| V40 | 27.4 | 10.2 | V40 | 16.1 | 9.6 | ||
| V45 | 7.1 | 5.6 | V45 | 5.1 | 4.9 | ||
| V50 | 0.9 | 2.1 | V50 | 0.7 | 1.6 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arcadipane, F.; Silvetti, P.; Olivero, F.; Gastino, A.; Carlevato, R.; Chiovatero, I.; Spinelli, L.; Mistrangelo, M.; Cassoni, P.; Ritorto, G.; et al. Concurrent Chemoradiation in Anal Cancer Patients Delivered with Bone Marrow-Sparing IMRT: Final Results of a Prospective Phase II Trial. J. Pers. Med. 2021, 11, 427. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050427
Arcadipane F, Silvetti P, Olivero F, Gastino A, Carlevato R, Chiovatero I, Spinelli L, Mistrangelo M, Cassoni P, Ritorto G, et al. Concurrent Chemoradiation in Anal Cancer Patients Delivered with Bone Marrow-Sparing IMRT: Final Results of a Prospective Phase II Trial. Journal of Personalized Medicine. 2021; 11(5):427. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050427
Chicago/Turabian StyleArcadipane, Francesca, Patrick Silvetti, Francesco Olivero, Alessio Gastino, Roberta Carlevato, Ilaria Chiovatero, Lavinia Spinelli, Massimiliano Mistrangelo, Paola Cassoni, Giuliana Ritorto, and et al. 2021. "Concurrent Chemoradiation in Anal Cancer Patients Delivered with Bone Marrow-Sparing IMRT: Final Results of a Prospective Phase II Trial" Journal of Personalized Medicine 11, no. 5: 427. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050427