
Molecular Pathology and Targeted Therapies for Personalized Management of Central Nervous System Germinoma

 , , and
, , and
Abstract
:1. Introduction
2. Clinical Presentation
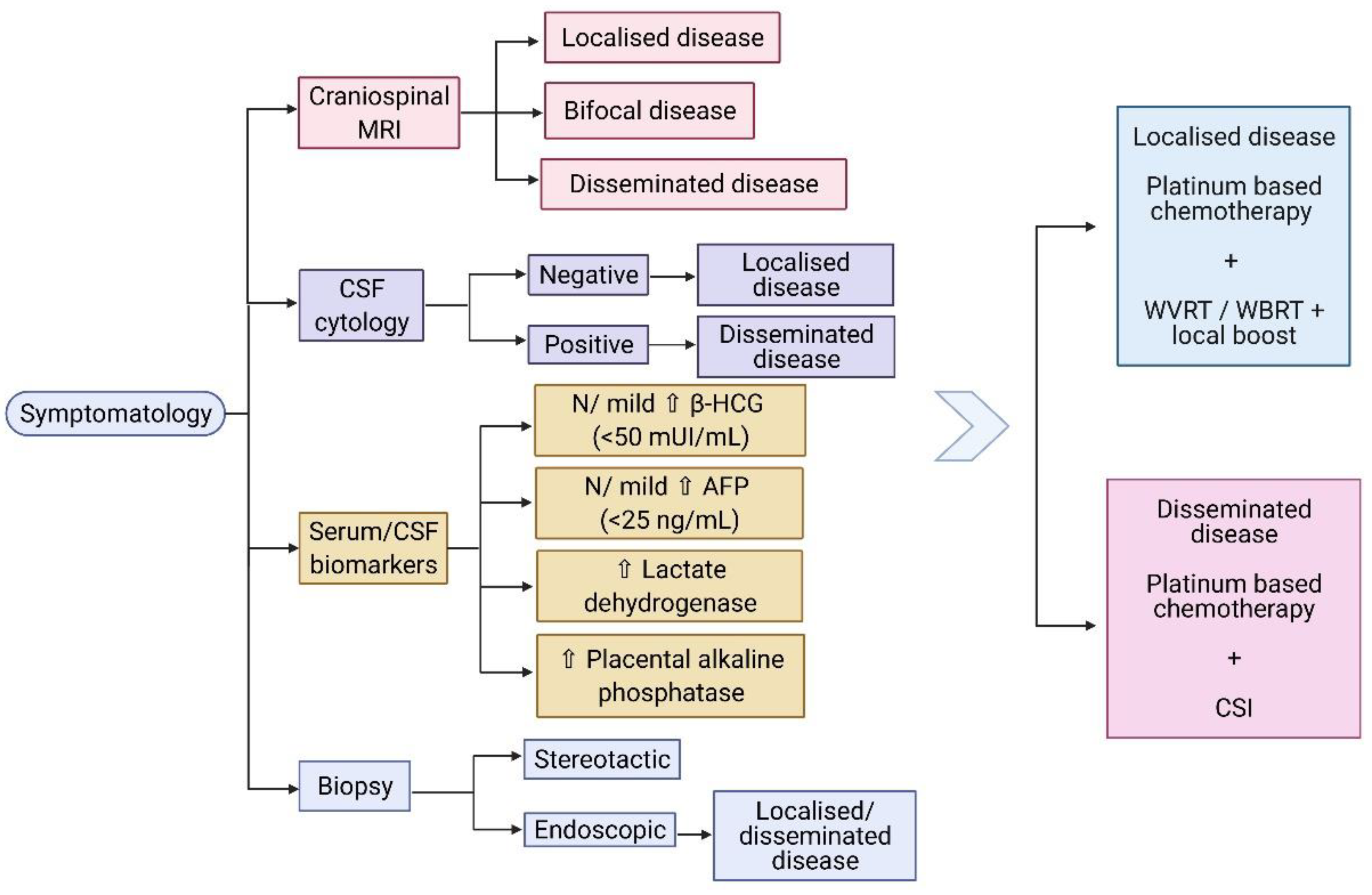
3. Diagnosis
3.1. Biological Markers
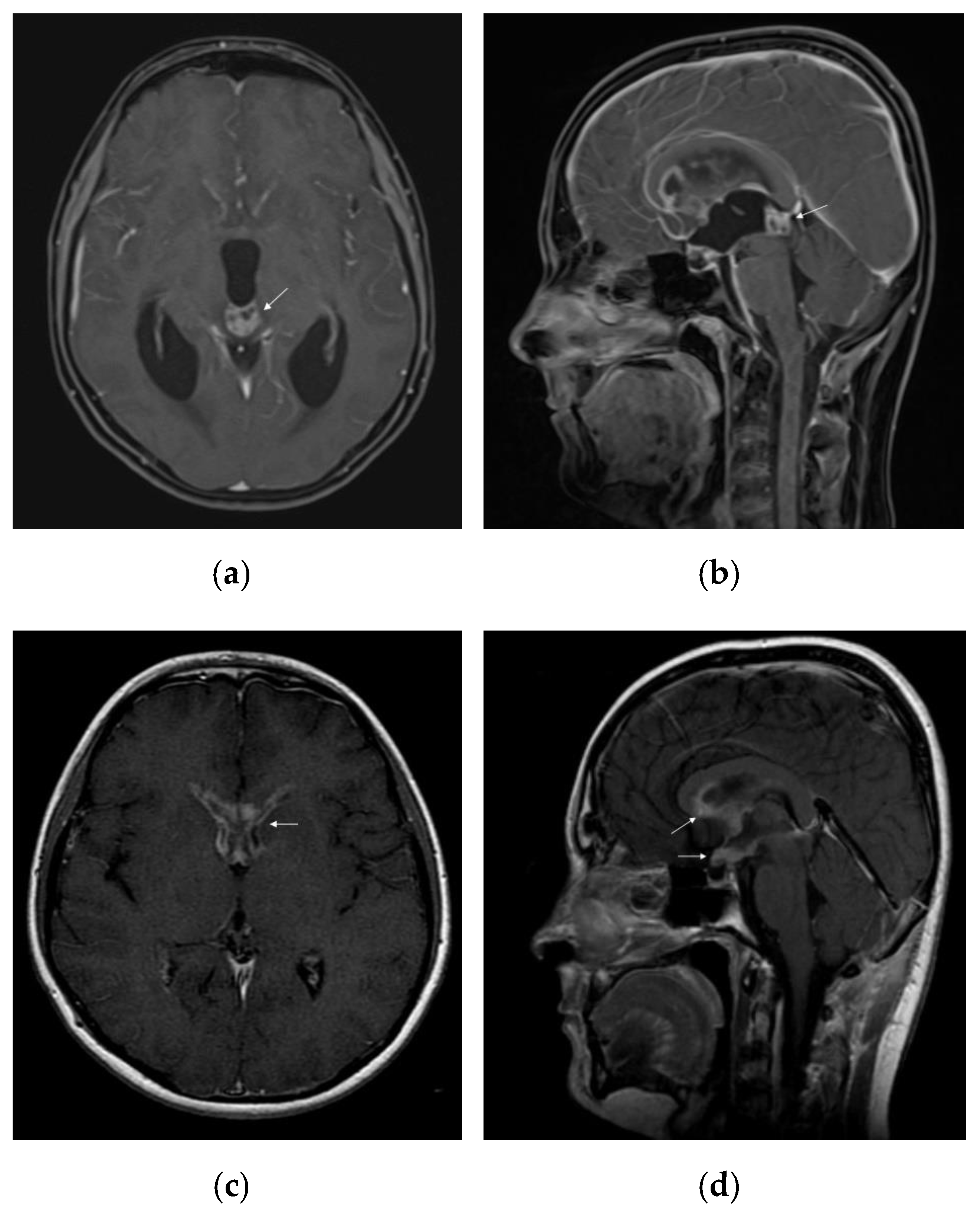
3.2. Radiological Characteristics
3.3. Biopsy
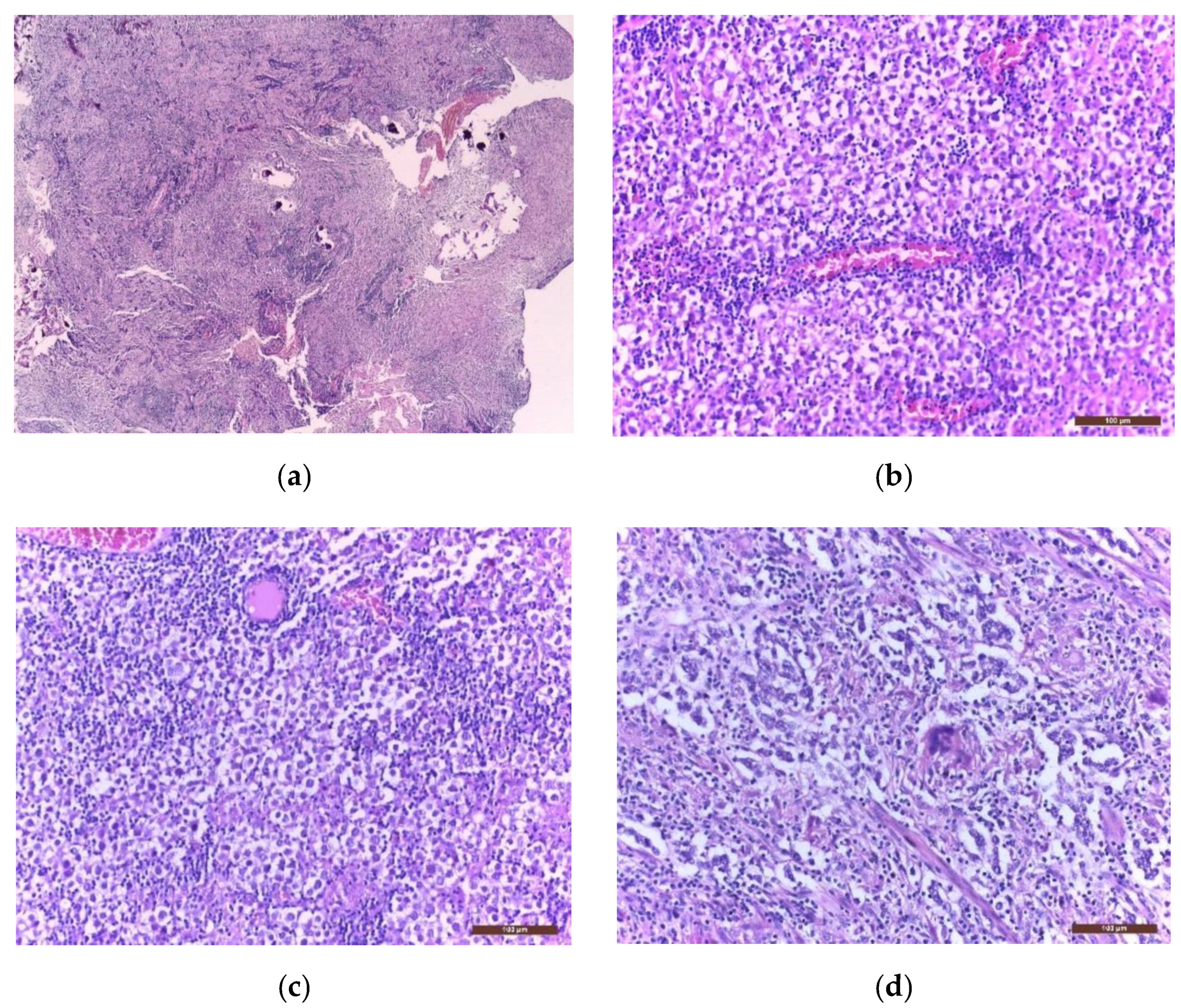
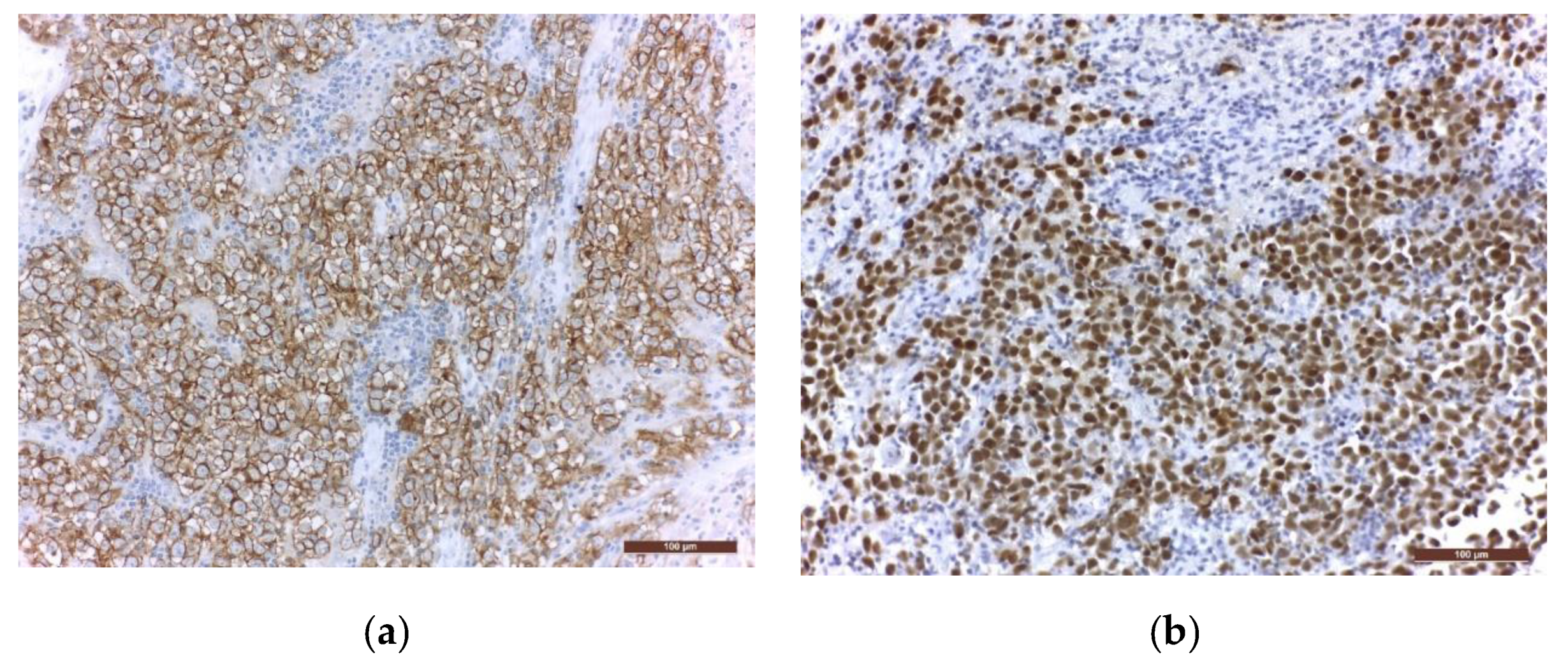
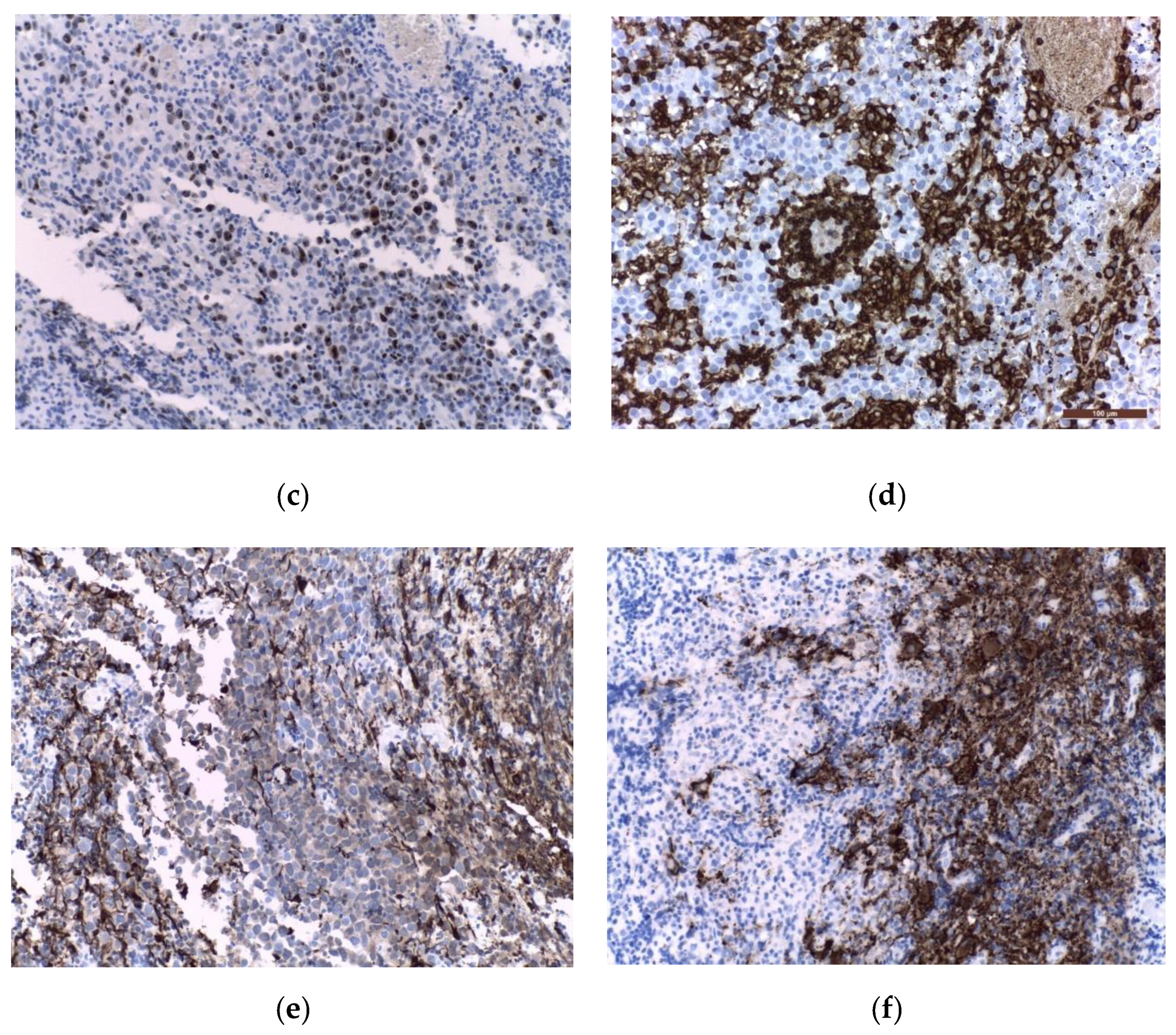
3.4. Histological Diagnosis
4. Staging
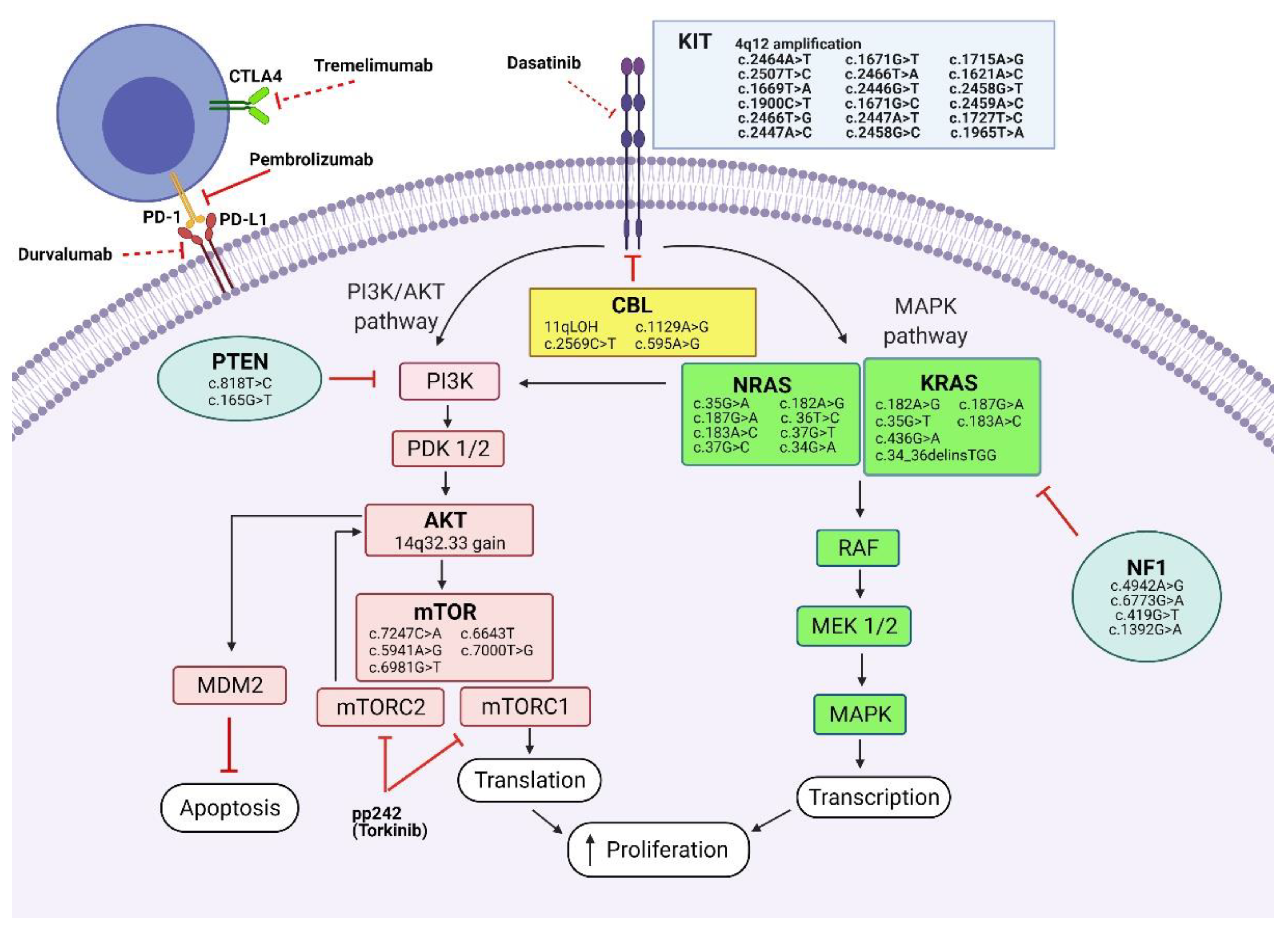
5. Genetic Approach
6. Immunological Approach
7. Current Management

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Chemotherapy Regimen ± Surgery | Radiotherapy | Results | Conclusion |
|---|---|---|---|---|
| Lee et al. 2019 [124] Prospective, multicentre, cohort study Bifocal germinomas treated as disseminated disease 91 germinoma patients: 65 localized diseases 9 bifocal diseases 17 multiple/disseminated cases Median age = 14 years 74.7% male patients | ±Surgery: total/partial resection (11%)/biopsy (89%) 2 courses of: Etoposide 150 mg/m2 Carboplatin 450 mg/m2 alternating with 2 courses of: Etoposide 150 mg/m2 Cyclophosphamide 1000 mg/m2 | Localized disease: CR: focal RT (30.6 Gy) PR: CSI (19.5 Gy) + focal RT (19.8 Gy) Bifocal/multiple/disseminated disease: CR: CSI (19.5 Gy) + focal RT (10.8 Gy) PR: CSI (24 Gy) + focal RT (16.2 Gy) | Median FU = 5.6 years 4 patients with progression/recurrence (4.4%) 5-year OS = 98.8% 5-year PFS = 96.6% | RT for localized pineal/suprasellar germinomas should include the whole ventricle area, whereas basal ganglia/thalamus germinomas should be treated with WBRT. |
| Calaminus et al. SIOP 96, 2013 [76] Prospective, multinational, nonrandomized study 235 germinoma patients: 190 localized diseases: 93 pineal; 53 supra-/intrasellar; 32 bifocal; 11 other 45 disseminated cases: 17 pineal, 13 supra-/intrasellar, 15 bifocal Median age = 13 years 176 males 59 females | ±Surgery: 22 complete resections, 107 subtotal resections/open biopsies, 103 stereotactic biopsies Local/bifocal disease Carboplatin 600 mg/m2/day+ Etoposide 100 mg/m2/day alternating with Etoposide 100 mg/m2/day+ Ifosfamide 1800 mg/m2/day | Local/bifocal disease: Focal RT (40 Gy) | Median FU = 6 years 5-year PFS = 88% OS = 96% 7 recurrences (6 with ventricular relapse) | Ventricular relapses suggest the importance of WVRT Local/bifocal germinomas are successfully treated with reduced dose CSI or with chemotherapy and reduced field RT |
| No chemotherapy | CSI 24 Gy + primary tumour site boost 16 Gy | 5-year PFS = 97% OS = 95% 4 recurrences at original site | ||
| Disseminated disease ±Chemotherapy (same regimen) | Disseminated disease 24 Gy CSI +16 Gy boost at primary tumour site and metastases | 5-year PFS = 100% OS = 98% | ||
| Kretschmar et al. POG 2007 [127] Prospective, phase II study 12 germinomas: 8 localized diseases: 2 pineal, 2 basal ganglia, 1 suprasellar, 3 other 4 disseminated cases Median age = 15.1 years 10 male patients, 2 female patients | ±Surgery: 5/12 patients: partial/total resection 4 courses Cisplatin 20 mg/m2/day+ Etoposide 100 mg/m2/day alternating with Vincristine 1.5 mg/m2 + Cyclophosphamide (CPM) 1 g/m2/day | CR: primary site RT 30.6 Gy; PR: primary site RT 50.4 Gy with 2 cm margin (3D-CRT) or 0.5 cm margin (SRT) Disseminated disease: CR: CSI 30.6 Gy + local boost 50.4 Gy PR: CSI 36 Gy + local boost 54 Gy | Median FU: 5.5 years 11/12 progression-free at median 5.5 years 1/12 refused RT, recurred at 10 months, salvage CSI, progression-free at 4.8 years | Favourable response (91%) and survival in the setting of chemotherapy followed by response-based RT |
| Aoyama et al. 2002 [118] Prospective study, phase II 27 germinomas out of 33 ICGCT: 16 pure germinomas 8 localized diseases: 1 neurohypophysis, 7 pineal 6 multifocal diseases: 4 neurohypophysis + pineal ± ventricle, 1 neurohypophysis + ventricle, 1 bilateral basal ganglia 2 disseminated cases 11 β-HCG secreting germinoma 8 localized diseases: 6 neurohypophysis, 2 pineal 2 multifocal diseases: neurohypophysis + pineal 1 disseminated case Mean age = 15.9 years (including patients with NGGCT) 32 males, 1 female (including patients with NGGCT) | ±Surgery—3 gross total/3 partial resections, 10 biopsies for pure germinomas; 1 gross total/3 partial resections, 7 biopsies for 11 β-HCG secreting germinoma Localised disease: Etoposide (100 mg/m2) + Cisplatin (20 mg/m2) 5 consecutive days every 4 weeks −4 cycles after partial resection/biopsy −3 cycles after total/subtotal resection | Localised disease: Local RT 24 Gy | Mean FU = 4.8 years Pure germinomas: CR = 100% 5-year FSR = 90% 1 recurrence | WV or larger field irradiation (probably 30–40 Gy) is necessary for β-HCG secreting germinomas 24-Gy irradiation to the primary site in combination with EP chemotherapy yielded excellent results in solitary pure germinomas |
| Multifocal/disseminated disease + β-HCG-secreting germinomas: 3–6 cycles of ICE: Ifosfamide (900 mg/m2) + Cisplatin (20 mg/m2) + Etoposide (60 mg/m2) 5 consecutive days every 4 weeks. Recurrence: chemotherapy and reirradiation | β-HCG secreting germinomas: Local irradiation/ 24-Gy WVRT+ 6 Gy neurohypophysis + 10 Gy pineal region Multifocal: 24 Gy WVRT Disseminated: 24 Gy CSI | β-HCG-secreting germinomas: CR = 100% 5-year free survival rate = 44% 5 recurrences No death due to recurrence | ||
| Matsutani, M. and The Japanese Pediatric Brain Tumor Study Group 2001 [128] Prospective, phase II study 75 germinomas 10 germinomas with STGC | Pure germinoma: 8 total resections 3 courses PE: Cisplatin 20 mg/m2 + Etoposide 60 mg/m2 (days 1–5) or CARB-VP: Carboplatin 450 mg/m2 (day 1) + Etoposide 150 mg/m2 (days 1–3). Large tumours or multiple/disseminated tumours: 3 cycles of ICE: Ifosphamide 900 mg/m2 + Cisplatin 20 mg/m2 + Etoposide 60 mg/m2 (days 1–5) | Pure germinoma Local RT 24 Gy | Pure germinoma Median FU = 2.9 years CR = 92% Recurrence = 9 (12%), of which 7 outside of the irradiated area | WBRT is not necessary for germinomas A dose of 24 Gy to the primary tumour site is suitable for obtaining disease control |
| Germinoma with STGC: 1 total resection CARB-VP or PE followed by RT+ same chemotherapy as RT for a total of 5 courses | Germinoma with STGC 30 Gy to a generous local area + 20 Gy to the primary tumour site | Germinoma with STGC CR = 90% No recurrences | ||
| Bamberg et al. MAKEI 83/86/89, 1999 [22] Prospective, multicentre, non-randomized 60 germinomas: 26 pineal, 9 suprasellar, 7 bifocal, 11 multiple midline tumours, 7 frontal horns/lateral ventricles germinomas Median age = 13 years 45 males, 15 females | ±Surgery: 5 complete resections 25 incomplete resections 4 open biopsies 24 stereotactic biopsies ±Chemotherapy (salvation treatment) | MAKEI 83/86: 11 germinomas CSI 36 Gy + local boost 14 Gy (total 50 Gy) | Median FU = 9.8 years 5-year RFS = 100% OS = 100% | Dose reduction of RT is possible with reasonable results |
| MAKEI 89: 49 germinomas 30 Gy (CSI) + local boost 15 Gy (total 34 Gy) | Median FU = 5.1 years 5-year RFS = 89% OS = 92% | |||
| Bouffet et al. SFOP- 1999 [129] Prospective, multicentre study 57 germinomas: 20 pineal, 28 suprasellar, 2 thalamic, 7 bifocal, 6 disseminated cases Median age = 13.5 years 43 males, 14 females | ± Surgery: 6 total resections, 12 partial resections, 7 open biopsies, 22 stereotactic biopsies 4 courses: Carboplatin 600 mg/m2 (day 1)+ Etoposide 150 mg/m2/day (days 1 to 3) alternating with Ifosfamide 1.8 g/m2/day (days 21 to 25) + Etoposide 150 mg/m2/day (days 21 to 23) | Local/bifocal germinoma: 40 Gy RT at primary tumour site Disseminated germinoma: CSI 25–30 Gy + 10 Gy boost on metastasis | Median FU = 3.5 years 3-year RFS = 98% 3-year EFS = 96.4% Recurrence: 4 (3 in second complete remission after salvage chemotherapy ± CSI) | Combination treatment with chemotherapy and local RT yielded favourable survival rates in local and bifocal germinoma |
| Sawamura et al. 1998 [130] Prospective, multicentre study 12 pure germinomas: 4 pineal, 2 neurohypophyseal, 4 multifocal, 2 disseminated 5 β-HCG secreting germinomas: 1 pineal, 3 neurohypophyseal, 1 disseminated Median age = 17 years 16 males, 1 female | Surgery: 3 total resections, 2 subtotal resections, 2 partial resections, 10 biopsies Local: 3/4 cycles EP: Cisplatin 20 mg/m2/day + Etoposide 100 mg/m2/day 5 consecutive days | Local disease: 24 Gy at primary tumour site | Median FU = 2 years 2-year survival probability = 100% 16 (94%) of the 17 patients were free from recurrence 1 recurrence—currently in second complete remission | Chemotherapy (EP and ICE regimens) followed by reduced volume and dose RT were highly effective in obtaining disease control |
| Multifocal, disseminated, β-HCG secreting germinoma: 3–6 cycles ICE: Ifosfamide 900 mg/m2/day+ Cisplatin 20 mg/m2/day+ Etoposide 60 mg/m2/day 5 consecutive days Recurrent disease—same as disseminated | Multifocal disease: 24 Gy at primary tumour site Disseminated disease: CSI 24 Gy | |||
| Balmaceda et al. 1996 [109] Prospective study 45 germinomas out of 71 ICGCT: 31 pineal, 21 suprasellar, 11 bifocal, 8 other, including 11 leptomeningeal disease Median age = 12.7 years (out of 71 ICGCT) 51 males, 20 females (out of 71 ICGCT) | ±Surgery: 18 total resections, 18 partial resections, 33 biopsies (out of 71 ICGCT) 4 cycles of: Carboplatin 500 mg/m2/day days 1–2+ Etoposide 150 mg/m2/day days 1–3+ Bleomycin 15 mg/m2/day day 3 If CR: 2 more cycles If PR: 2 more cycles + cyclophosphamide ± RT | RT—if less than CR after chemotherapy or progressive/relapsed disease | Median FU: 2.9 years CR = 82% 2-year OS = 84% 20 relapses/45 germinomas | Treatment with chemotherapy alone is characterized by a high rate of tumour recurrence |
8. Future Perspectives
9. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
Appendix A
| Study | Chemotherapy Regimen ± Surgery | Radiotherapy | Results | Conclusion |
|---|---|---|---|---|
| Lee et al. 2021 [156] Retrospective study 189 germinomas: 119 solitary lesions: 46 pineal, 41 suprasellar, 29 basal ganglia/thalamus, 3 other 25 bifocal diseases 45 disseminated diseases Median age = 15 years 151 males, 38 females | No chemotherapy | CSI 24 Gy localised disease/30 Gy disseminated disease+ tumour boost 54 Gy | Median FU = 9.6 years 10-year OS: RT only: 85.2% CRT: 92.8% Relapse: RT only: 10% CRT: 5.8% Salvage treatment: 50% response Hormone replacement correlated with WBRT Secondary malignancy: 5.3%, more frequent in WBRT, CSI | Chemotherapy permits the use of reduced RT dosage The dose and volume of extended-field RT should be reduced in order to prevent late adverse effects |
| 2 cycles: Bleomycin + Etoposide + Cisplatin/ Etoposide + Cisplatin OR 5 cycles Cisplatin + Etoposide + Cyclophosphamide + Vincristine OR “8-in-1”: Solumedrol + Vincristine+ Lomustine + Procarbazine + Hydroxyurea + Cisplatin + Cytosine Arabinoside + Cyclophosphamide | CSI 23 Gy + boost/ WBRT 23 Gy + boost/ WVRT 23 Gy + boost/ Focal RT Tumour boost dose: 45 Gy if CR after chemo 50 Gy if no CR after chemo | |||
| Salvage therapy after relapse: chemotherapy + CSI/chemotherapy only/CSI only | ||||
| Nosrati et al. 2021 [157] Retrospective study 4 localised germinomas out of 18 intracranial germinomas: 1 pineal, 2 suprasellar, 1 bifocal | 4 cycles every 3 weeks: Carboplatin 300 mg/m2+ Etoposide 150 mg/m2 | Simultaneous Integrated Boost (SIB): WVRT 22.5 Gy+ Tumour boost 30 Gy | SIB: EFS = 89.5% SIB: OS = 100% Organ-at-risk doses—comparable between SIB and WVRT only; lower for COG | SIB technique permits higher doses to primary tumour than WVRT only, without further neurocognitive impairment COG protocol–lower doses, but still evaluating efficiency |
| 1 cycle: Carboplatin 450 mg/m2+ Etoposide 150 mg/m2 | WVRT 24 Gy | |||
| 4 cycles every 3 weeks: Carboplatin 600 mg/m2+ Etoposide 150 mg/m2 | Sequential therapy (COG protocol): WVRT 18 Gy+ Tumour boost 12 Gy | |||
| Baroni et al. 2021 [148] Retrospective study 39 germinomas: 15 pineal, 9 sellar/suprasellar, 7 bifocal, 2 thalamus/basal ganglia, 1 other, 5 disseminated cases Median age = 12.1 years 27 males, 12 females | Surgery: 1 complete resection, 6 partial resections, 32 biopsies 2 courses of: Carboplatin + Etoposide alternating with Ifosfamide + Etoposide | FR/ FR + WVRT/ CSI only (1 patient) | Median FU = 6.5 years 5-year PFS = 83.5% 5-year OS = 88.7% 5-year PFS: FR: 63% FR + WVRT: 94% 4 deaths | FR increases the risk of recurrence Chemotherapy and focal RT + WVRT has favourable results in localized germinomas |
| 1st line salvage therapy: Platinum-based chemotherapy + CSI ± FR 2nd line salvage therapy: 4 cycles: Gemcitabine-Paclitaxel-Oxaliplatin + HDC + stem cell rescue | 7 localized germinoma relapsed (5 treated with FR/2 with FR + WVRT) | |||
| Li et al. 2021 [147] Retrospective study 161 basal ganglia germinomas: 68 right, 66 left, 15 bilateral, 12 basal ganglia + sellar Median age = 12 years 150 males, 11 females | 2 cycles every 4 weeks before and after RT: Ifosfamide, 1.5 g/m2 days 1–3+ Etoposide, 70 mg/m2 days 1–3+ Cisplatin, 30 mg/m2 days 1–3 ±Surgery: 15 resection, 15 biopsies | FR/CSI (30 Gy) + tumour boost (10 Gy)/ WBRT (30 Gy) + tumour boost (10 Gy) | Median FU = 6.9 years 5-year DFS = 92% 5-year OS FR = 94.1% 5-year OS WBRT = 97.2% 5-year OS CSI = 100% | WBRT offers a better quality of life compared to CSI and represents an optimal treatment strategy in localized basal ganglia germinomas |
| Kumar et al. 2021 [149] Retrospective study 19 germinomas out of 28 ICGCT: 12 pineal, 3 suprasellar, 4 other Median age = 17 years (including NGGCT) 11 males, 8 females | ±Surgery: 3 total resections, 4 subtotal resections, 7 biopsies, 9 shunts 4–6 cycles: Bleomycin + Etoposide + Cisplatin/ Etoposide + Cisplatin | Local RT/ WVRT + boost/ WBRT + boost/ Disseminated: CSI + boost 3D-CRT/IMRT Total dose: 36–40 Gy | Median FU = 4.4 years 5-year OS = 89% 5-year PFS = 83.1% | Chemotherapy and reduced dose/volume RT has favourable results |
| Rajagopal et al. 2021 [158] Retrospective study 16 germinomas: 6 pineal, 6 suprasellar, 1 bifocal, 2 basal ganglia, 1 other, including 7 disseminated cases Median age = 11 years 11 males, 5 females | ±Surgery: 1 total resection, 3 subtotal resection, 12 biopsies, 3 ventriculoperitoneal shunts, 3 ventriculostomies SIOP CNS GCT 96 protocol/ SIOP CNS GCT II protocol/ physician preference | CSI (24–25 Gy) ± boost (40–44.4 Gy)/ WVRT (24–36 Gy) + boost (36–54 Gy)/ Local RT (40–50 Gy) Recurrence: Chemo + CSI 24 Gy + cranial RT 19.8 Gy | Median FU = 3.5 years 10-year OS = 75.5% 10-year EFS = 61.1% Recurrence: 5 patients | Inferior results are observed in underdeveloped countries due to late diagnosis, poor compliance, suboptimal treatment, and complications of therapy |
| Hong et al. 2020 [146] Retrospective study 66 germinomas + normal tumour markers out of 69 low-risk tumours: 24 pineal, 14 sellar/suprasellar, 17 thalamus/basal ganglia, 10 bifocal, 4 other, including 7 disseminated cases Median age = 11.8 years 55 males, 16 females | ±Surgery: resection/biopsy/endoscopic third ventriculostomy/extraventricular drainage/ventriculoperitoneal shunt Carboplatin 450 mg/m2/day+ Etoposide 100 mg/m2/day Alternating with Cyclophosphamide 1000 mg/m2/day+ Etoposide 150 mg/m2/day | Local RT (40.4 Gy)/ WVRT (19.8 Gy)/ WBRT (30.6 Gy)/ CSI (23.4Gy)—multifocal/metastatic disease, poor response to chemotherapy | Median FU = 8.4 years 10-year EFS = 88.6% 10-year OS = 98.3% 10-year relapse incidence = 9.3% 4 basal ganglia germinoma relapsed Endocrine complications:53.6% | Chemo-radiotherapy achieved favourable results |
| 14 germinomas + high tumour markers out of 58 high-risk tumours: 28 pineal, 13 sellar/suprasellar, 7 thalamus/basal ganglia, 7 bifocal, 3 other, including 7 disseminated cases Median age = 12.2 years 47 males, 11 females | Carboplatin 450 mg/m2/day+ Etoposide 150 mg/m2/day Bleomycin 15 mg/m2/day Alternating with Cyclophosphamide 2000 mg/m2/day+ Etoposide 150 mg/m2/day+ Bleomycin 15 mg/m2/day | WVRT (23.4 Gy)/ WBRT (30.6 Gy)/ CSI (23.4 Gy) | Median FU = 8.3 years 10-year EFS = 100% 10-year OS = 100% 10-year relapse incidence = 5.6% Endocrine complications:53.4% | Germinoma with elevated tumour markers could benefit from a lower intensity treatment |
| Chou et al. 2020 [159] Retrospective study 24 germinomas: 17 pineal, 13 suprasellar, 7 periventricular, 2 basal ganglia 13 isolated tumours 11 multifocal tumours 5 β-hCG-secreting germinomas Median age = 14.1 years 20 males, 4 females | Surgery: 1 total resection, 9 subtotal resections, 14 biopsies Short-course neoadjuvant chemotherapy: 2 courses of Cisplatin 20 mg/m2+ Etoposide 40 or 100 mg/m2 for 5 days | WVRT/WBRT (23.4 Gy) without local boost | Median FU = 8.8 years 100% complete remission 5-year DFS β-hCG-secreting germinomas = 60% 5-year DFS normal β-hCG level germinomas = 100% | CNS germinoma patients with normal β-hCG levels may benefit from short course chemotherapy and low dose RT without local boost |
| Shimizu et al. 2020 [119] Retrospective study 40 pure germinomas+ 30 germinomas with STGC out of 110 ICGCT: 52 pineal, 39 suprasellar, 16 basal ganglia, 10 other Median age = 14 years (including NGGCT) 90 males, 20 females (including NGGCT) | ±Surgery: 1 total resection, 2 subtotal resections, 10 partial resections, 17 biopsies 2 courses before RT and 1 after: Carboplatin 300 mg/m2, day 1+ Etoposide 100 mg/m2, days 1–3 OR Chemotherapy only | WVRT (30 Gy) ± tumour boost (10 Gy) if remnant tumours/ Basal ganglia germinoma: WBRT (30 Gy)/ RT only | Median FU = 11 years 5-year OS = 97.1% 10-year OS = 95.7% 20-year OS = 93.2% 5-year PFS = 91.4% 10-year PFS = 86.6% 20-year PFS = 86.6% No neurocognitive disorders No treatment-related deaths | The CRT regimens presented yielded favourable results in pure germinomas and germinomas with STGC Further studies might attempt further reduction of RT dosage |
| 2 courses before RT and 1 after: Cisplatin 20 mg/m2 + Etoposide 60 mg/m2, days 1–5 | Focal RT 40 Gy | |||
| Multifocal/disseminated Carboplatin 300 mg/m2, day 1+ Etoposide 100 mg/m2, days 1–3+ Ifosfamide 1500 mg/m2, days 1–3 | Multifocal/disseminated CSI (30 Gy) | |||
| Esfahani et al. 2020 [60] Retrospective study 33 germinomas: 15 suprasellar, 14 bifocal, 4 basal ganglia + suprasellar, including 12 disseminated cases Out of all 42 ICGCT: Mean age suprasellar tumours = 11.2 years Mean age bifocal tumours = 13.4 years 26 males,16 females | Neoadjuvant chemotherapy (COG protocol) ±Surgery: resection/biopsy/second-look surgery, endoscopic/craniotomy/transsphenoidal/stereotactic | Suprasellar germinomas: WVRT + local boost /WBRT/Focal RT Suprasellar germinomas + ventricular metastasis: WVRT + local boost/ CSI + local boost Bifocal germinomas ± ventricular metastases: WVRT + local boost/ CSI + local boost Basal ganglia germinoma ±ventricular metastases: CSI + local boost | WVRT + boost: 1 suprasellar germinoma recurrence 2 bifocal germinomas recurrences CSI + boost: 1 bifocal germinoma recurrence | Bifocal germinomas have a higher rate of metastasis and recurrence CSI is recommended for bifocal germinomas with metastasis |
| Li et al. 2020 [160] Retrospective study 49 non-metastatic bifocal germinomas: 34 sellar/suprasellar + pineal, 15 sellar/suprasellar + thalamus/basal ganglia Median age = 13 years 34 males, 15 females | Two courses before and after RT: Ifosfamide 1.5 g/m2 days 1–3+ Etoposide 70 mg/m2 days 1–3+ Cisplatin 30 mg/m2 days 1–3 ±Surgery | CSI + boost/ WBRT + boost/ Focal RT | Median FU = 4.3 years 5-year DFS = 96.7% 5-year OS = 97.3% WBRT—comparable disease-free survival with CSI | Limited field RT could replace CSI in patients with non-metastatic bifocal germinoma |
| 81 non-metastatic bifocal germinoma (literature): sellar/suprasellar + pineal | Not mentioned | Focal RT/WVRT/WBRT/CSI | No difference regarding the disease-free survival | |
| Takada et al. 2018 [161] Retrospective study 6 germinomas + 12 germinomas with STGC, out of 24 ICGCT: 10 pineal, 3 suprasellar, 6 basal ganglia/brainstem, 5 multifocal, 4 disseminated cases Median age = 13 years (including NGGCT) 20 males, 4 females (including NGGCT) | Pure germinoma ±Surgery: 2 partial excisions, 2 biopsies 2–5 courses of conventional dose therapy (CDC): ICE: Ifosfamide + Cisplatin + Etoposide | WVRT 24 Gy | Median follow-up = 9.3 years 10-year OS = 100% 1 recurrence after 10 years | Favourable results obtained with combined treatment: chemotherapy (conventional/intensive) and reduced field and dose irradiation |
| Germinoma with STGC: ±Surgery: 1 total excision, 3 partial excisions, 4 biopsies 2/3 courses of CDC and high-dose chemotherapy (HDC) + PBSCT HDC: PEB/EP/CARE/ICE | WVRT/larger field 24–30 Gy ± local boost irradiation (20 Gy) | 3 patients relapsed and died of their disease 10-year OS = 78.7% | ||
| No chemotherapy | CSI 24 Gy + primary tumour site boost 16 Gy | 5-year PFS = 97% OS = 95% 4 recurrences at original site | ||
| Disseminated disease ±Chemotherapy (same regimen) | Disseminated disease 24 Gy CSI + 16 Gy boost at primary tumour site and metastases | 5-year PFS = 100% OS = 98% | ||
| Cheng et al. 2016 [138] Retrospective study 24 germinomas: 9 suprasellar, 6 pineal, 8 bifocal, 1 basal ganglia, including 4 disseminated cases Median age = 13.3 years 13 males, 11 females | ±Surgery: biopsy, external ventricular drain, septostomy, ventriculostomy, ventricular-peritoneal shunt 2 cycles of Carboplatin 600 mg/m2 + Etoposide 300 mg/m2 alternating with Ifosfamide 9000 mg/m2 + Etoposide 300 mg/m2 OR 3–4 cycles Carboplatin 600 mg/m2 + Etoposide 450 mg/m2 3–4 cycles | WVRT (23.4–24 Gy)/ WVRT (23.4–24 Gy) + boost (16 Gy)/ WBRT (23.4 Gy)/ Focal RT (40 Gy)/ CSI (23.4 Gy) | Median FU = 5 years 5-year PFS = 96% 5-year OS = 100% 1 recurrence No difference in neurocognitive functions between focal RT and WVRT | Successful results in the setting of CRT, with reduces dose and volume RT No relapses in cases of WVRT without boost |
| Weksberg et al. 2012 [162] Retrospective study 20 bifocal germinomas (pineal + suprasellar), including 11 disseminated diseases Median age = 19 years 19 males, 1 female | ±Surgery: 13 biopsies ±Neoadjuvant platinum-based chemotherapy+ Etoposide± Ifosfamide Chemotherapy was not administered to patients who received CSI | Median RT dose = 50 Gy Localized disease: CSI/WBRT/WVI/local RT Disseminated disease: CSI/WBRT/WVRT | Median FU = 8.2 year 5-year PFS = 100% | Bifocal germinomas with no signs of dissemination are candidates for neoadjuvant chemotherapy and spinal sparing RT. CSI represents the treatment of choice for disseminated disease. |
| 60 bifocal (pineal + suprasellar) germinomas (literature) including 14 disseminated diseases Age range: 6–30 years 43 males,11 females, 6 not stated | ±Neoadjuvant platinum-based chemotherapy+ Etoposide± Ifosfamide/Methotrexate | Median RT dose = 40 Gy CSI/WBRT/WVI/local RT | Median FU = 5 years 5-year PFS = 87% | |
| Combined analysis: 80 bifocal germinoma (pineal+ suprasellar), including 25 disseminated cases 62 males, 12 females, 6 not stated Age range: 6–33 years | 55 localized diseases: 5-year PFS = 95% 5-year PFS (CSI) = 100% 5-year PFS (WBRT/WVI /local RT) = 88% 5-year PFS (WBRT/WVI /local RT + Chemo) = 96% | 25 disseminated disease: 5-year PFS = 80% 5-year PFS (CSI)= 100% 5-year PFS (WBRT/WVI /local RT + Chemo) = 69% | ||
| Macdonald et al. 2011 [163] Retrospective study 13 germinoma patients: 7 suprasellar, 2 basal ganglia + thalamus, 4 multiple midline tumours Age range: 6–20 years 5 males, 8 females | ±Chemotherapy cisplatin, carboplatin, etoposide, ifosphamide, cyclophosphamide, vincristine ±Surgery | CSI (18–23 Gy) + involved field (5.4–36 Gy)/ WVRT (19.5–23.4 Gy) + involved field (7.2–22 Gy)/ WBRT (25.5 Gy) + involved field (19.8 Gy) * 3D PT compared to IMRT and IMPT | Median FU = 2.3 years Local control= 100% No CNS recurrences PFS = 95% OS = 100% | Favourable preliminary results Proton therapy provides superior dose-distribution, with greater normal tissue saving, compared to IMRT |
| Eom et al. 2008 [164] Retrospective study 81 germinoma patients: 22 suprasellar, 26 pineal, 13 suprasellar + pineal, 3 suprasellar + other, 17 other, including 21 disseminated cases Median age = 14.6 years (RT only group) Median age = 17.5 years (CRT group) 65 males, 16 females | Surgery: 27 stereotactic biopsies, 20 endoscopic biopsies, 10 open biopsies, 12 partial resections, 9 subtotal resections, 3 total resections No chemotherapy | CSI: 21 Gy—negative seeding 36 Gy—positive seeding +involved field 54 Gy | Median follow-up = 5.7 years No relapse 5-year OS = 100% 5-year RFS = 100% | Chemoradiotherapy provides better quality of live, but more relapses. Ventricles should be included in the RT field for the treatment of localized disease |
| 42 patients: chemo + RT 1–4 cycles of Bleomycin + Etoposide, and Cisplatin/Etoposide + Cisplatin OR 1–5 cycles of Cisplatin, Etoposide, Cyclophosphamide and Vincristine OR Solumedrol, Vincristine, Lomustine, Procarbazine, Hydroxyurea, Cisplatin, Cytosine arabinoside, and Cyclophosphamide | Localised disease/negative seeding: 50 Gy at tumour site Multifocal disease/positive seeding: CSI 23.4 Gy+ Local boost: 45 Gy—if CR after chemo 54 Gy—if PR after chemo | 4 relapses in patients with involved-field RT 5-years RFS = 88% 5-year OS = 93% | ||
| Lafay-Cousin et al. 2006 [23] Retrospective 6 patients with bifocal germinomas out of 17 germinomas: 4 pineal + suprasellar, 1 pineal + third ventricle floor, 1 pineal + tuber cinereum Median age = 12.8 years 5 males, 1 female | ±Surgery: 3 third ventricle ventriculostomies + biopsies 3/4 cycles of Etoposide + Cisplatin OR 2 courses of Carboplatin + Etoposide alternating with 2 courses of Ifosfamide + Etoposide | WVRT 24–40 Gy ±boost at both tumour sites (16 Gy) | Median FU = 4 years CR = 100% No persistent disease/recurrence | Bifocal germinoma (pineal + suprasellar) can be treated as locoregional disease with chemotherapy and limited field radiation (WVRT ± boost) |
| Modak et al. 2004 [165] Retrospective 9 patients with relapsed germinoma out of 21 CNS relapsed GCT: 3 intracranial, 1 spinal cord, 1 intracranial + spinal cord, 1 ventricular, 1 pineal + abdominal, 1 pineal + lateral horn, 1 leptomeningeal dissemination Age range: 7–31 years 7 males, 2 females | ±Surgery: 4 biopsies Thiotepa 200 mg/m2/d for 3 days with ASCR; followed 4 weeks later by Thiotepa 200 mg/m2/d for 3 days with ASCR Or Carboplatin 500 mg/m2/d on days 1–3 +Thiotepa 300 mg/m2/d on days 4–6 +Etoposide 250 mg/m2/d on days 4–6 Or Carboplatin 500 mg/m2/d on days 1–3 +Thiotepa 300 mg/m2/d on days 4–6 +Temozolomide 150–250 mg/m2/d | Post-chemotherapy adjuvant RT: −cranial irradiation −CSI ± focal irradiation | Median FU = 4 years OS = 78% PFS = 78% 2 deaths: −1 progressive disease (PD) −1 pulmonary fibrosis secondary to bleomycin and spinal irradiation | High dose chemotherapy followed by ASCR represents an effective alternative therapy for patients with relapsed CNS germinomas |
| Haas-Kogan et al. 2003 [166] Retrospective 49 germinomas: 41 localized 8 disseminated Median age = 15 years 32 males, 17 females | ±Surgery: 22 biopsies, 19 subtotal resections, 5 total resections ±Chemotherapy | Localised disease: CSI/WBRT/WVRT (32.4 Gy) + local boost/Local RT Disseminated disease: CSI | Median FU = 7.5 years 5-year OS = 93% 5-year PFS = 88% 5 relapses 2 deaths | CSI is not necessary for localized disease; WVRT + local boost (total of 45–50 Gy) is recommended in localized disease |
| Fouladi et al, 1998 [167] Retrospective study 16 germinomas: 6 pineal, 3 suprasellar, 3 bifocal, 4 metastatic Median age: 11.5 years (RT only group) Median age = 10.8 years (CRT group) 13 males, 3 females | Surgery: 16 biopsies No chemotherapy | Local/metastatic disease: CSI 24–35 Gy (median dose 25 Gy) + tumour boost 15–30.6 Gy (median dose 15.5 Gy) | Median FU = 7 years 10 years EFS = 87.5% OS = 100% | Adjuvant chemotherapy permits RT dose reduction and elimination of CSI (in localised disease) with no significant differences in OS and EFS |
| 2–3 cycles every 4 weeks: Cisplatin 20 mg/m2/day (days 1–5)+ Etoposide 120 mg/m2/day (days 1–5)± Bleomycin 15 mg/m2 (days 1, 8, 15) OR Carboplatin + Etoposide + Ifosfamide OR Cisplatin + Etoposide + Cyclophosphamide | Local disease: 25–36 Gy (median dose 35 Gy) at primary tumour site Metastatic disease: 25–35 Gy at primary tumour site + 20–25 Gy spinal RT (median dose 25 Gy) | Median FU = 3.4 years EFS = 75% OS = 87% | ||
| Huh et al. 1996 [168] Retrospective study 32 germinomas: 4 pineal, 14 suprasellar, 2 bifocal, 12 basal ganglia and thalamus, including 3 disseminated cases Median age = 14 years 24 males, 8 females | Surgery: 1 total resection, 4 subtotal resections, 11 partial resection, 16 biopsies No chemotherapy | CSI/WBRT ± boost RT tumour bed 54 Gy Whole-brain 36 Gy Spinal axis 24 Gy | Median FU = 5.1 years 10-year OS 97% 1 death (persistent tumour) No intracranial or spinal recurrence | Radiotherapy alone yielded favourable results |
References
- Gittleman, H.; Cioffi, G.; Vecchione-Koval, T.; Ostrom, Q.T.; Kruchko, C.; Osorio, D.S.; Finlay, J.L.; Barnholtz-Sloan, J.S. Descriptive epidemiology of germ cell tumors of the central nervous system diagnosed in the United States from 2006 to 2015. J. Neuro Oncol. 2019, 143, 251–260. [Google Scholar] [CrossRef]
- Schneider, D.T.; Calaminus, G.; Koch, S.; Teske, C.; Schmidt, P.; Haas, R.J.; Harms, D.; Göbel, U. Epidemiologic analysis of 1442 children and adolescents registered in the German germ cell tumor protocols. Pediatr. Blood Cancer 2004, 42, 169–175. [Google Scholar] [CrossRef]
- Kurucu, N.; Akyüz, C.; Varan, A.; Zorlu, F.; Aydin, B.; Söylemezoglu, F.; Yalcin, B.; Kutluk, T.; Büyükpamukcus, M. Primary intracranial germ cell tumors in children 36-year experience of a single center. J. Cancer Res. Ther. 2020, 16, 1459–1465. [Google Scholar] [CrossRef]
- Takami, H.; Perry, A.; Graffeo, C.S.; Giannini, C.; Narita, Y.; Nakazato, Y.; Saito, N.; Nishikawa, R.; Matsutani, M.; Ichimura, K.; et al. Comparison on epidemiology, tumor location, histology, and prognosis of intracranial germ cell tumors between Mayo Clinic and Japanese consortium cohorts. J. Neurosurg. 2020, 134, 446–456. [Google Scholar] [CrossRef]
- Louis, D.N.; Ohgaki, H.; Wiestier, O.D.; Cavenee, W.K. (Eds.) WHO Classification of Tumours of the Central Nervous System, 4th ed.; International Agency for Research on Cancer (IARC): Lyon, France, 2016; pp. 284–287.
- Matsutani, M.; Sano, K.; Takakura, K.; Fujimaki, T.; Nakamura, O.; Funata, N.; Seto, T. Primary intracranial germ cell tumors: A clinical analysis of 153 histologically verified cases. J. Neurosurg. 1997, 86, 446–455. [Google Scholar] [CrossRef] [Green Version]
- Takami, H.; Fukuoka, K.; Fukushima, S.; Nakamura, T.; Mukasa, A.; Saito, N.; Yanagisawa, T.; Nakamura, H.; Sugiyama, K.; Kanamori, M.; et al. Integrated clinical, histopathological, and molecular data analysis of 190 central nervous system germ cell tumors from the iGCT Consortium. Neuro Oncol. 2019, 21, 1565–1577. [Google Scholar] [CrossRef]
- Villano, J.L.; Propp, J.M.; Porter, K.R.; Stewart, A.K.; Valyi-Nagy, T.; Li, X.; Engelhard, H.H.; McCarthy, B.J. Malignant pineal germ-cell tumors: An analysis of cases from three tumor registries. Neuro Oncol. 2008, 10, 121–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tso, W.W.-Y.; Yung, A.W.-Y.; Lau, H.-Y.; Chan, G.C.-F. Basal ganglia germinoma: MRI classification correlates well with neurological and cognitive outcome. J. Pediatr. Hematol. Oncol. 2014, 36, e443–e447. [Google Scholar] [CrossRef] [PubMed]
- de Pémille, C.V.; Bielle, F.; Mokhtari, K.; Kerboua, E.; Alapetite, C.; Idbaih, A. Basal Ganglia Germinoma in an Adult. World Neurosurg. 2016, 92, 584.e11–584.e14. [Google Scholar] [CrossRef] [PubMed]
- Kageyama, H.; Suzuki, T.; Ohara, Y. Intramedullary spinal cord germinoma clinically mimicking multiple sclerosis: A case report. Surg. Neurol. Int. 2019, 10, 201. [Google Scholar] [CrossRef] [PubMed]
- Utsuki, S.; Oka, H.; Tanizaki, Y.; Kondo, K.; Fujii, K. Radiological features of germinoma arising from atypical locations. Neurol. Med. Chir. 2005, 45, 268–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankar, S.; Wu, X.; Kalra, V.B.; Huttner, A.J.; Malhotra, A. Ectopic intracranial germinoma. J. Clin. Neurosci. 2016, 31, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Schulte, S.L.; Waha, A.; Steiger, B.; Denkhaus, D.; Dörner, E.; Calaminus, G.; Leuschner, I.; Pietsch, T. CNS germinomas are characterized by global demethylation, chromosomal instability and mutational activation of the Kit-, Ras/Raf/Erk- and Akt-pathways. Oncotarget 2016, 7, 55026–55042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sano, M.; Jinguji, S.; Yoshimura, J.; Okamoto, K.; Fujii, Y. De Novo Pineal Region Germinoma in the Seventh Decade of Life: A Case Report. NMC Case Rep. J. 2019, 6, 75–78. [Google Scholar] [CrossRef]
- Klopfenstein, J.D.; Lanzino, G.; Kim, L.J.; Spetzler, R.F. Pineal region germinoma in the seventh decade: Case report. Barrow Q. 2002, 18. [Google Scholar]
- Bjornsson, J.; Scheithauer, B.W.; Okazaki, H.; Leech, R.W. Intracranial germ cell tumors: Pathobiological and immunohistochemical aspects of 70 cases. J. Neuropathol. Exp. Neurol. 1985, 44, 32–46. [Google Scholar] [CrossRef] [PubMed]
- Ho, D.M.; Liu, H.-C. Primary intracranial germ cell tumor. Pathologic study of 51 patients. Cancer 1992, 70, 1577–1584. [Google Scholar] [CrossRef]
- Bohara, M.; Hirano, H.; Tokimura, H.; Hanaya, R.; Yonezawa, H.; Campos, F.; Sugiyama, K.; Sugata, S.; Arita, K. Pineal mixed germ cell tumor with a synchronous sellar lesion in the sixth decade. Brain Tumor Pathol. 2011, 28, 163–166. [Google Scholar] [CrossRef]
- Saitoh, M.; Tamaki, N.; Kokunai, T.; Matsumoto, S. Clinico-biological behavior of germ-cell tumors. Child’s Nerv. Syst. 1991, 7, 246–250. [Google Scholar] [CrossRef]
- Merchant, T.E.; Sherwood, S.H.; Mulhern, R.K.; Rose, S.R.; Thompson, S.J.; Sanford, R.A.; Kun, L.E. CNS germinoma: Disease control and long-term functional outcome for 12 children treated with craniospinal irradiation. Int. J. Radiat. Oncol. Biol. Phys. 2000, 46, 1171–1176. [Google Scholar] [CrossRef]
- Bamberg, M.; Kortmann, R.-D.; Calaminus, G.; Becker, G.; Meisner, C.; Harms, D.; Göbel, U. Radiation therapy for intracranial germinoma: Results of the German cooperative prospective trials MAKEI 83/86/89. J. Clin. Oncol. 1999, 17, 2585. [Google Scholar] [CrossRef]
- Lafay-Cousin, L.; Millar, B.-A.; Mabbott, D.; Spiegler, B.; Drake, J.; Bartels, U.; Huang, A.; Bouffet, E. Limited-field radiation for bifocal germinoma. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 486–492. [Google Scholar] [CrossRef]
- Sugiyama, K.; Uozumi, T.; Kiya, K.; Mukada, K.; Arita, K.; Kurisu, K.; Hotta, T.; Ogasawara, H.; Sumida, M. Intracranial germ-cell tumor with synchronous lesions in the pineal and suprasellar regions: Report of six cases and review of the literature. Surg. Neurol. 1992, 38, 114–120. [Google Scholar] [CrossRef]
- Sawamura, Y.; Ikeda, J.; Shirato, H.; Tada, M.; Abe, H. Germ cell tumours of the central nervous system: Treatment consideration based on 111 cases and their long-term clinical outcomes. Eur. J. Cancer 1998, 34, 104–110. [Google Scholar] [CrossRef]
- Chen, R.; Tao, C.; You, C.; Ju, Y. Fast-developing fatal diffuse leptomeningeal dissemination of a pineal germinoma in a young child: A case report and literature review. Br. J. Neurosurg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Hanakita, S.; Takenobu, A.; Kambe, A.; Watanabe, T.; Shin, M.; Teraoka, A. Intramedullary recurrence of germinoma in the spinal cord 15 years after complete remission of a pineal lesion. J. Neurosurg. Spine 2012, 16, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Wenger, M.; Lövblad, K.O.; Markwalder, R.; Taub, E. Late recurrence of pineal germinoma. Surg. Neurol. 2002, 57, 34–39. [Google Scholar] [CrossRef]
- Takami, H.; Graffeo, C.S.; Perry, A.; Giannini, C.; Daniels, D.J. The Third Eye Sees Double: Cohort Study of Clinical Presentation, Histology, Surgical Approaches, and Ophthalmic Outcomes in Pineal Region Germ Cell Tumors. World Neurosurg. 2021, 150, e482–e490. [Google Scholar] [CrossRef]
- Kretschmar, C.S. Germ cell tumors of the brain in children: A review of current literature and new advances in therapy. Cancer Investig. 1997, 15, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Inoue, A.; Ohnishi, T.; Kohno, S.; Ohue, S.; Iwata, S.; Matsumoto, S.; Nishikawa, M.; Ozaki, S.; Mizuno, Y.; Kitazawa, R.; et al. Identification of characteristic features of pineal germinoma that enhance accuracy of preoperative differentiation in pineal region tumors: Its significance on optimum surgical treatment. Neurosurg. Rev. 2018, 41, 197–206. [Google Scholar] [CrossRef]
- Yang, N.; Zhu, H.-J.; Yao, Y.; He, L.-Y.; Li, Y.-X.; You, H.; Zhang, H.-B. Diabetes insipidus with impaired vision caused by germinoma and perioptic meningeal seeding: A case report. World J. Clin. Cases 2021, 9, 1976–1982. [Google Scholar] [CrossRef]
- Oka, H.; Kawano, N.; Tanaka, T.; Utsuki, S.; Kobayashi, I.; Maezawa, H.; Fujii, K. Long-term functional outcome of suprasellar germinomas: Usefulness and limitations of radiotherapy. J. Neuro Oncol. 1998, 40, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Reisch, N.; Kühne-Eversmann, L.; Franke, D.; Beuschlein, F.; Mueller-Lisse, U.G.; Reincke, M.; Seissler, J. Intracranial germinoma as a very rare cause of panhypopituitarism in a 23-year old man. Exp. Clin. Endocrinol. Diabetes 2009, 117, 320–323. [Google Scholar] [CrossRef]
- Mesquita Filho, P.M.; Santos, F.P.; Köhler, L.R.; Manfroi, G.; De Carli, F.; de Araujo, M.A.; Schwingel, D. Suprasellar Germinomas: 2 Case Reports and Literature Review. World Neurosurg. 2018, 117, 165–171. [Google Scholar] [CrossRef]
- Nishio, S.; Inamura, T.; Takeshita, I.; Fukui, M.; Kamikaseda, K. Germ cell tumor in the hypothalamo-neurohypophysial region: Clinical features and treatment. Neurosurg. Rev. 1993, 16, 221–227. [Google Scholar] [CrossRef]
- Wellons, J.C., III; Reddy, A.T.; Tubbs, R.S.; Abdullatif, H.; Oakes, W.J.; Blount, J.P.; Grabb, P.A. Neuroendoscopic findings in patients with intracranial germinomas correlating with diabetes insipidus. J. Neurosurg. Pediatr. 2004, 100, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Reddy, A.T.; Wellons, J.C., III; Allen, J.C.; Fiveash, J.B.; Abdullatif, H.; Braune, K.W.; Grabb, P.A. Refining the staging evaluation of pineal region germinoma using neuroendoscopy and the presence of preoperative diabetes insipidus. Neuro Oncol. 2004, 6, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, H.-Y.; Chiu, C.-F.; Jung, S.-M.; Wong, A.M.-C.; Wu, C.-T.; Lo, F.-S. Neurological and endocrinological manifestations of 49 children with intracranial pure germinoma at initial diagnosis in Taiwan. Pediatr. Neonatol. 2021, 62, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Saeki, N.; Tamaki, K.; Murai, H.; Kubota, M.; Yamaura, A.; Uchida, D.; Noguchi, Y.; Nakamura, S.; Tatsuno, I.; Wada, K.; et al. Long-term outcome of endocrine function in patients with neurohypophyseal germinomas. Endocr. J. 2000, 47, 83–89. [Google Scholar] [CrossRef] [Green Version]
- Das, K.K.; Joseph, J.; Singh, A.K.; Sharma, P.; Sardhara, J.; Bhaisora, K.S.; Mehrotra, A.; Srivastava, A.K.; Jaiswal, S.; Sahu, R.N.; et al. Capsuloganglionic Germinoma: A Rare Site for Uncommon Childhood Tumor. Asian J. Neurosurg. 2018, 13, 492–495. [Google Scholar] [CrossRef]
- Goswami, S.; Chakraborty, P.P.; Bhattacharjee, R.; Roy, A.; Thukral, A.; Selvan, C.; Ghosh, S.; Mukhopadhyay, S.; Chowdhury, S. Precocious puberty: A blessing in disguise! Indian J. Endocrinol. Metab. 2013, 17, S111–S113. [Google Scholar] [CrossRef]
- Yeo, K.K.; Kayser, K.; Margol, A.S.; Wong, K.K.; Robison, N.; Finlay, J.; Dhall, G. Clinical and neuropsychological outcome of pediatric non-midline central nervous system germinoma treated with chemotherapy and reduced dose/volume irradiation: The Children’s Hospital Los Angeles experience. Pediatr. Blood Cancer 2019, 66, e27983. [Google Scholar] [CrossRef]
- Huang, Z.-C.; Dong, Q.; Song, E.-P.; Chen, Z.-J.; Zhang, J.-H.; Hou, B.; Lu, Z.-Q.; Qin, F. Germinomas of the basal ganglia and thalamus: Four case reports. World J. Clin. Cases 2020, 8, 4558–4564. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.A.; Bhatti, M.T.; Giannini, C.; Eckel, L.J.; Garrity, J.A.; Chen, J.J. Intracranial Pure Germinoma with Optic Nerve Infiltration. J. Neuro Ophthalmol. 2020, 40, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Hayden, J.; Murray, M.J.; Bartels, U.; Ajithkumar, T.; Muthusamy, B.; Penn, A.; Calaminus, G.; Nicholson, J. Symptom interval and treatment burden for patients with malignant central nervous system germ cell tumours. Arch. Dis. Child. 2020, 105, 247–252. [Google Scholar] [CrossRef]
- Haase, J.; Nørgaard-Pedersen, B. Alpha-feto-protein (AFP) and human chorionic gonadotropin (HCG) as biochemical markers of intracranial germ-cell tumours. Acta Neurochir. 1979, 50, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Arita, N.; Ushio, Y.; Hayakawa, T.; Uozumi, T.; Watanabe, M.; Mori, T.; Mogami, H. Serum levels of alpha-fetoprotein, human chorionic gonadotropin and carcinoembryonic antigen in patients with primary intracranial germ cell tumors. Oncodev. Biol. Med. 1980, 1, 235–240. [Google Scholar]
- Utsuki, S.; Oka, H.; Tanaka, S.; Tanizaki, Y.; Fujii, K. Long-term outcome of intracranial germinoma with hCG elevation in cerebrospinal fluid but not in serum. Acta Neurochir. 2002, 144, 1151–1155. [Google Scholar] [CrossRef]
- Utsuki, S.; Kawano, N.; Oka, H.; Tanaka, T.; Suwa, T.; Fujii, K. Cerebral germinoma with syncytiotrophoblastic giant cells: Feasibility of predicting prognosis using the serum hCG level. Acta Neurochir. 1999, 141, 975–978. [Google Scholar] [CrossRef]
- Srinivasan, N.; Pakala, A.; Mukkamalla, C.; Oswal, A. Pineal germinoma. South. Med. J. 2010, 103, 1031–1037. [Google Scholar] [CrossRef]
- Takami, H.; Perry, A.; Graffeo, C.S.; Giannini, C.; Daniels, D.J. Novel Diagnostic Methods and Posttreatment Clinical Phenotypes Among Intracranial Germ Cell Tumors. Neurosurgery 2020, 87, 563–572. [Google Scholar] [CrossRef]
- Carr, C.; O’Neill, B.E.; Hochhalter, C.B.; Strong, M.J.; Ware, M.L. Biomarkers of Pineal Region Tumors: A Review. Ochsner J. 2019, 19, 26–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aihara, Y.; Watanabe, S.; Amano, K.; Komatsu, K.; Chiba, K.; Imanaka, K.; Hori, T.; Ohba, T.; Dairoku, H.; Okada, Y.; et al. Placental alkaline phosphatase levels in cerebrospinal fluid can have a decisive role in the differential diagnosis of intracranial germ cell tumors. J. Neurosurg. 2018, 131, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Chiba, K.; Aihara, Y.; Komori, T.; Kawamata, T. Placental alkaline phosphatase in cerebrospinal fluid as a biomarker for optimizing surgical treatment strategies for pineal region germ cell tumors. Brain Tumor Pathol. 2020, 37, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Morana, G.; Alves, C.A.; Tortora, D.; Finlay, J.L.; Severino, M.; Nozza, P.; Ravegnani, M.; Pavanello, M.; Milanaccio, C.; Maghnie, M.; et al. T2*-based MR imaging (gradient echo or susceptibility-weighted imaging) in midline and off-midline intracranial germ cell tumors: A pilot study. Neuroradiology 2018, 60, 89–99. [Google Scholar] [CrossRef]
- Awa, R.; Campos, F.; Arita, K.; Sugiyama, K.; Tominaga, A.; Kurisu, K.; Yamasaki, F.; Karki, P.; Tokimura, H.; Fukukura, Y.; et al. Neuroimaging diagnosis of pineal region tumors-quest for pathognomonic finding of germinoma. Neuroradiology 2014, 56, 525–534. [Google Scholar] [CrossRef]
- Chavhan, G.B.; Babyn, P.S.; Thomas, B.; Shroff, M.M.; Haacke, E.M. Principles, techniques, and applications of T2*-based MR imaging and its special applications. Radiographics 2009, 29, 1433–1449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takano, M.; Kinoshita, Y.; Sugiyama, K.; Kolakshyapati, M.; Takayasu, T.; Yonezawa, U.; Taguchi, A.; Akiyama, Y.; Amatya, V.J.; Takeshima, Y.; et al. Detecting non-germinomatous germ cell tumor component by arterial spin labeling perfusion-weighted MR imaging in central nervous system germ cell tumor. Eur. J. Radiol. 2021, 136, 109523. [Google Scholar] [CrossRef] [PubMed]
- Esfahani, D.R.; Alden, T.; DiPatri, A.; Xi, G.; Goldman, S.; Tomita, T. Pediatric Suprasellar Germ Cell Tumors: A Clinical and Radiographic Review of Solitary vs. Bifocal Tumors and Its Therapeutic Implications. Cancers 2020, 12, 2621. [Google Scholar] [CrossRef]
- Mootha, S.L.; Barkovich, A.J.; Grumbach, M.M.; Edwards, M.S.; Gitelman, S.E.; Kaplan, S.L.; Conte, F.A. Idiopathic hypothalamic diabetes insipidus, pituitary stalk thickening, and the occult intracranial germinoma in children and adolescents. J. Clin. Endocrinol. Metab. 1997, 82, 1362–1367. [Google Scholar] [CrossRef]
- Devuyst, F.; Kazakou, P.; Baleriaux, D.; Alexopoulou, O.; Burniat, A.; Salenave, S.; Chanson, P.; Corvilain, B.; Maiter, D. Central diabetes insipidus and pituitary stalk thickening in adults: Distinction of neoplastic from non-neoplastic lesions. Eur. J. Endocrinol. 2020, 183, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Ram, N.; Batool, S.; Mushtaq, N. A Case Report Emphasizing the Importance of Early Diagnosis and Management of Intracranial Germinoma. Cureus 2020, 12, e11721. [Google Scholar] [CrossRef] [PubMed]
- Dias, D.; Vilar, H.; Passos, J.; Leite, V. Central diabetes insipidus caused by a pituitary stalk germinoma resembling infundibuloneurohypophysitis. BMJ Case Rep. 2020, 13, e234724. [Google Scholar] [CrossRef]
- Bóssolo, A.G.; Garcia, M.M.; Davila, K.; Brau, R.; Ortiz, J.S.; Martinez, J.H. A Rare Localized Pituitary Stalk Germinoma Presenting in the Third Decade. Case Rep. Endocrinol. 2018, 2018, 1746917. [Google Scholar] [CrossRef]
- Zhou, X.; Zhu, H.; Yao, Y.; Lian, X.; Feng, F.; Wang, L.; Liu, S.; Deng, K.; You, H.; Yang, H.; et al. Etiological Spectrum and Pattern of Change in Pituitary Stalk Thickening: Experience in 321 Patients. J. Clin. Endocrinol. Metab. 2019, 104, 3419–3427. [Google Scholar] [CrossRef]
- Wu, C.-C.; Guo, W.-Y.; Chang, F.-C.; Luo, C.-B.; Lee, H.-J.; Chen, Y.-W.; Lee, Y.-Y.; Wong, T.-T. MRI features of pediatric intracranial germ cell tumor subtypes. J. Neuro Oncol. 2017, 134, 221–230. [Google Scholar] [CrossRef]
- Balossier, A.; Blond, S.; Reyns, N. Endoscopic Versus Stereotactic Procedure for Pineal Tumor Biopsies: Focus on Overall Efficacy Rate. World Neurosurg. 2016, 92, 223–228. [Google Scholar] [CrossRef]
- Kanamori, M.; Takami, H.; Yamaguchi, S.; Sasayama, T.; Yoshimoto, K.; Tominaga, T.; Inoue, A.; Ikeda, N.; Kambe, A.; Kumabe, T.; et al. So-called bifocal tumors with diabetes insipidus and negative tumor markers: Are they all germinoma? Neuro Oncol. 2020, 23, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Day, E.L.; Smith, E.R.; Fehnel, K.P. Single-institution case series of pituitary biopsy for suspected germinoma in the pediatric population: Diagnostic utility, operative risks, and biopsy approaches. Sci. Rep. 2020, 10, 15257. [Google Scholar] [CrossRef]
- Liu, W.; Raynald; Tian, Y.; Gong, J.; Ma, Z.; Ma’ruf, L.; Li, C. Simultaneous single-trajectory endoscopic biopsy and third ventriculostomy in pediatric pineal region tumors. Acta Neurol. Belg. 2020. [Google Scholar] [CrossRef]
- Gao, Y.; Jiang, J.; Liu, Q. Clinicopathological and immunohistochemical features of primary central nervous system germ cell tumors: A 24-years experience. Int. J. Clin. Exp. Pathol. 2014, 7, 6965–6972. [Google Scholar]
- Zapka, P.; Dörner, E.; Dreschmann, V.; Sakamato, N.; Kristiansen, G.; Calaminus, G.; Vokuhl, C.; Leuschner, I.; Pietsch, T. Type, Frequency, and Spatial Distribution of Immune Cell Infiltrates in CNS Germinomas: Evidence for Inflammatory and Immunosuppressive Mechanisms. J. Neuropathol. Exp. Neurol. 2018, 77, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Cao, D.; Liu, A.; Wang, F.; Allan, R.W.; Mei, K.; Peng, Y.; Du, J.; Guo, S.; Abel, T.W.; Lane, Z.; et al. RNA-binding protein LIN28 is a marker for primary extragonadal germ cell tumors: An immunohistochemical study of 131 cases. Mod. Pathol. 2011, 24, 288–296. [Google Scholar] [CrossRef]
- Pantazis, G.; Harter, P.N.; Capper, D.; Kohlhof, P.; Mittelbronn, M.; Schittenhelm, J. The embryonic stem cell factor UTF1 serves as a reliable diagnostic marker for germinomas. Pathology 2014, 46, 225–229. [Google Scholar] [CrossRef]
- Calaminus, G.; Kortmann, R.; Worch, J.; Nicholson, J.C.; Alapetite, C.; Garrè, M.L.; Patte, C.; Ricardi, U.; Saran, F.; Frappaz, D. SIOP CNS GCT 96: Final report of outcome of a prospective, multinational nonrandomized trial for children and adults with intracranial germinoma, comparing craniospinal irradiation alone with chemotherapy followed by focal primary site irradiation for patients with localized disease. Neuro Oncol. 2013, 15, 788–796. [Google Scholar] [CrossRef]
- Allen, J.C. Controversies in the management of intracranial germ cell tumors. Neurol. Clin. 1991, 9, 441–452. [Google Scholar] [CrossRef]
- Aoyama, I.; Kondo, A.; Ogawa, H.; Ikai, Y. Germinoma in siblings: Case reports. Surg. Neurol. 1994, 41, 313–317. [Google Scholar] [CrossRef]
- Nitta, N.; Fukami, T.; Nozaki, K. Germinoma in two brothers: Case report. Neurol. Med. Chir. 2013, 53, 703–706. [Google Scholar] [CrossRef] [Green Version]
- Doknic, M.; Savic, D.; Manojlovic-Gacic, E.; Savo, R.; Bokun, J.; Milenkovic, T.; Pavlovic, S.; Vreca, M.; Andjelkovic, M.; Stojanovic, M.; et al. Clinical case seminar: Familial intracranial germinoma. Endokrynol. Pol. 2018, 69, 612–618. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, K.; Mineharu, Y.; Imamura, H.; Asai, K.; Imai, Y.; Ichimura, K.; Sakai, N. Intracranial germinomas in a father and his son. Child’s Nerv. Syst. 2014, 30, 2143–2146. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, S.; Yamashita, S.; Kobayashi, H.; Takami, H.; Fukuoka, K.; Nakamura, T.; Yamasaki, K.; Matsushita, Y.; Nakamura, H.; Totoki, Y.; et al. Genome-wide methylation profiles in primary intracranial germ cell tumors indicate a primordial germ cell origin for germinomas. Acta Neuropathol. 2017, 133, 445–462. [Google Scholar] [CrossRef] [PubMed]
- Amatruda, J.F.; Ross, J.A.; Christensen, B.; Fustino, N.J.; Chen, K.S.; Hooten, A.J.; Nelson, H.; Kuriger, J.K.; Rakheja, D.; Frazier, A.L.; et al. DNA methylation analysis reveals distinct methylation signatures in pediatric germ cell tumors. BMC Cancer 2013, 13, 313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakata, Y.; Yagishita, A.; Arai, N. Two patients with intraspinal germinoma associated with Klinefelter syndrome: Case report and review of the literature. Am. J. Neuroradiol. 2006, 27, 1204–1210. [Google Scholar] [PubMed]
- Matsumura, N.; Kurimoto, M.; Endo, S.; Fukuda, O.; Takaku, A. Intracranial germinoma associated with Down’s syndrome. Pediatr. Neurosurg. 1998, 29, 199–202. [Google Scholar] [CrossRef]
- Fukushima, S.; Otsuka, A.; Suzuki, T.; Yanagisawa, T.; Mishima, K.; Mukasa, A.; Saito, N.; Kumabe, T.; Kanamori, M.; Tominaga, T.; et al. Mutually exclusive mutations of KIT and RAS are associated with KIT mRNA expression and chromosomal instability in primary intracranial pure germinomas. Acta Neuropathol. 2014, 127, 911–925. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Yamaguchi, S.; Burstein, M.D.; Terashima, K.; Chang, K.; Ng, H.-K.; Nakamura, H.; He, Z.; Doddapaneni, H.; Lewis, L.; et al. Novel somatic and germline mutations in intracranial germ cell tumours. Nature 2014, 511, 241–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ichimura, K.; Fukushima, S.; Totoki, Y.; Matsushita, Y.; Otsuka, A.; Tomiyama, A.; Niwa, T.; Takami, H.; Nakamura, T.; Suzuki, T.; et al. Recurrent neomorphic mutations of MTOR in central nervous system and testicular germ cell tumors may be targeted for therapy. Acta Neuropathol. 2016, 131, 889–901. [Google Scholar] [CrossRef] [PubMed]
- Kamakura, Y.; Hasegawa, M.; Minamoto, T.; Yamashita, J.; Fujisawa, H. C-kit gene mutation: Common and widely distributed in intracranial germinomas. J. Neurosurg. Pediatr. 2006, 104, 173–180. [Google Scholar] [CrossRef]
- Sakuma, Y.; Sakurai, S.; Oguni, S.; Satoh, M.; Hironaka, M.; Saito, K. c-kit gene mutations in intracranial germinomas. Cancer Sci. 2004, 95, 716–720. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.-P.; Jiang, J.-Y.; Liu, Q. Expression and mutation of c-Kit in intracranial germ cell tumors: A single-centre retrospective study of 30 cases in China. Oncol. Lett. 2016, 11, 2971–2976. [Google Scholar] [CrossRef] [Green Version]
- Low, S.Y.Y.; Cheng, H.; Zou, R.; Ng, L.P.; Kuick, C.H.; Sulaiman, N.B.S.; Chang, K.T.E.; Low, D.C.Y.; Zhou, L.; Seow, W.T. Molecular exploration of paediatric intracranial germinomas from multi-ethnic Singapore. BMC Neurol. 2020, 20, 415. [Google Scholar] [CrossRef]
- Ventura, M.; Gomes, L.; Rosmaninho-Salgado, J.; Barros, L.; Paiva, I.; Melo, M.; Oliveira, D.; Carrilho, F. Bifocal germinoma in a patient with 16p11.2 microdeletion syndrome. Endocrinol. Diabetes Metab. Case Rep. 2019, 2019. [Google Scholar] [CrossRef]
- Wang, H.-W.; Wu, Y.-H.; Hsieh, J.-Y.; Liang, M.-L.; Chao, M.-E.; Liu, D.-J.; Hsu, M.-T.; Wong, T.-T. Pediatric primary central nervous system germ cell tumors of different prognosis groups show characteristic miRNome traits and chromosome copy number variations. BMC Genom. 2010, 11, 132. [Google Scholar] [CrossRef] [Green Version]
- Takayasu, T.; Shah, M.; Dono, A.; Yan, Y.; Borkar, R.; Putluri, N.; Zhu, J.-J.; Hama, S.; Yamasaki, F.; Tahara, H.; et al. Cerebrospinal fluid ctDNA and metabolites are informative biomarkers for the evaluation of CNS germ cell tumors. Sci. Rep. 2020, 10, 14326. [Google Scholar] [CrossRef]
- Palmer, R.D.; Murray, M.J.; Saini, H.K.; van Dongen, S.; Abreu-Goodger, C.; Muralidhar, B.; Pett, M.R.; Thornton, C.M.; Nicholson, J.C.; Enright, A.J.; et al. Malignant germ cell tumors display common microRNA profiles resulting in global changes in expression of messenger RNA targets. Cancer Res. 2010, 70, 2911–2923. [Google Scholar] [CrossRef] [Green Version]
- Murray, M.J.; Ajithkumar, T.; Harris, F.; Williams, R.M.; Jalloh, I.; Cross, J.; Ronghe, M.; Ward, D.; Scarpini, C.G.; Nicholson, J.C.; et al. Clinical utility of circulating miR-371a-3p for the management of patients with intracranial malignant germ cell tumors. Neuro Oncol. Adv. 2020, 2, vdaa048. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04435756 (accessed on 14 May 2021).
- Murray, M.J.; Bell, E.; Raby, K.L.; Rijlaarsdam, M.A.; Gillis, A.J.M.; Looijenga, L.H.J.; Brown, H.; Destenaves, B.; Nicholson, J.C.; Coleman, N. A pipeline to quantify serum and cerebrospinal fluid microRNAs for diagnosis and detection of relapse in paediatric malignant germ-cell tumours. Br. J. Cancer 2016, 114, 151–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobo, J.; Rodrigues, Â.; Guimarães, R.; Cantante, M.; Lopes, P.; Mauricio, J.; Oliveira, J.; Jeronimo, C.; Henrique, R. Detailed Characterization of Immune Cell Infiltrate and Expression of Immune Checkpoint Molecules PD-L1/CTLA-4 and MMR Proteins in Testicular Germ Cell Tumors Disclose Novel Disease Biomarkers. Cancers 2019, 11, 1535. [Google Scholar] [CrossRef] [Green Version]
- Nishimoto, M.; Ohara, K.; Kamamoto, D.; Tamura, R.; Miwa, T.; Yoshida, K.; Sasaki, H. Tumor immune microenvironment is associated with the growth of intracranial germinomas. J. Neuro Oncol. 2020, 146, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Takami, H.; Fukushima, S.; Aoki, K.; Satomi, K.; Narumi, K.; Hama, N.; Matsushita, Y.; Fukuoka, K.; Yamasaki, K.; Nakamura, T.; et al. Intratumoural immune cell landscape in germinoma reveals multipotent lineages and exhibits prognostic significance. Neuropathol. Appl. Neurobiol. 2020, 46, 111–124. [Google Scholar] [CrossRef]
- Liu, B.; Arakawa, Y.; Yokogawa, R.; Tokunaga, S.; Terada, Y.; Murata, D.; Matsui, Y.; Fujimoto, K.-I.; Fukui, N.; Tanji, M.; et al. PD-1/PD-L1 expression in a series of intracranial germinoma and its association with Foxp3+ and CD8+ infiltrating lymphocytes. PLoS ONE 2018, 13, e0194594. [Google Scholar] [CrossRef] [Green Version]
- Wildeman, M.E.; Shepard, M.J.; Oldfield, E.H.; Lopes, M.B.S. Central Nervous System Germinomas Express Programmed Death Ligand 1. J. Neuropathol. Exp. Neurol. 2018, 77, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Maity, A.; Shu, H.-K.; Janss, A.; Belasco, J.B.; Rorke, L.; Phillips, P.C.; Sutton, L.N.; Goldwein, J.W. Craniospinal radiation in the treatment of biopsy-proven intracranial germinomas: Twenty-five years’ experience in a single center. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 1165–1170. [Google Scholar] [CrossRef] [PubMed]
- Bishr, M.K.; Zaghloul, M.S.; Elmaraghi, C.; Galal, A.; Abdelaziz, M.S.; Elghazawy, H.I.; Shaheen, H.; Ramzy, E.S.; Mesbah, A.; Eissa, S.K.; et al. The radiotherapy utilization rate in pediatric tumors: An analysis of 13,305 patients. Radiother. Oncol. 2020, 154, 220–226. [Google Scholar] [CrossRef]
- Kellie, S.J.; Boyce, H.; Dunkel, I.J.; Diez, B.; Rosenblum, M.; Brualdi, L.; Finlay, J.L. Intensive cisplatin and cyclophosphamide-based chemotherapy without radiotherapy for intracranial germinomas: Failure of a primary chemotherapy approach. Pediatr. Blood Cancer 2004, 43, 126–133. [Google Scholar] [CrossRef]
- Kellie, S.J.; Boyce, H.; Dunkel, I.J.; Diez, B.; Rosenblum, M.; Brualdi, L.; Finlay, J.L. Primary chemotherapy for intracranial nongerminomatous germ cell tumors: Results of the second international CNS germ cell study group protocol. J. Clin. Oncol. 2004, 22, 846–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balmaceda, C.; Heller, G.; Rosenblum, M.; Diez, B.; Villablanca, J.G.; Kellie, S.; Maher, P.; Vlamis, V.; Walker, R.W.; Leibel, S.; et al. Chemotherapy without irradiation—A novel approach for newly diagnosed CNS germ cell tumors: Results of an international cooperative trial. The First International Central Nervous System Germ Cell Tumor Study. J. Clin. Oncol. 1996, 14, 2908–2915. [Google Scholar] [CrossRef] [PubMed]
- Packer, R.J.; Cohen, B.H.; Cooney, K. Intracranial germ cell tumors. Oncologist 2000, 5, 312–320. [Google Scholar] [CrossRef] [Green Version]
- Fu, H.; Guo, X.; Li, R.; Xing, B. Radiotherapy and chemotherapy plus radiation in the treatment of patients with pure intracranial germinoma: A meta-analysis. J. Clin. Neurosci. 2017, 43, 32–38. [Google Scholar] [CrossRef]
- Bhimani, A.D.; Barrington, N.M.; Aguilar, T.M.; Arnone, G.D.; Mehta, A.I. Pituitary germinomas: A multi-institutional study analyzing patient demographics and management patterns. Pituitary 2020, 23, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.J.; Metayer, L.E.; Mallucci, C.L.; Hale, J.P.; Nicholson, J.C.; Kirollos, R.W.; Burke, G.A.A. Intra-abdominal metastasis of an intracranial germinoma via ventriculo-peritoneal shunt in a 13-year-old female. Br. J. Neurosurg. 2011, 25, 747–749. [Google Scholar] [CrossRef]
- Roth, J.; Constantini, S. Combined rigid and flexible endoscopy for tumors in the posterior third ventricle. J. Neurosurg. 2015, 122, 1341–1346. [Google Scholar] [CrossRef] [Green Version]
- Abbassy, M.; Aref, K.; Farhoud, A.; Hekal, A. Outcome of single-trajectory rigid endoscopic third ventriculostomy and biopsy in the management algorithm of pineal region tumors: A case series and review of the literature. Child’s Nerv. Syst. 2018, 34, 1335–1344. [Google Scholar] [CrossRef]
- Shahrestani, S.; Ravi, V.; Strickland, B.; Rutkowski, M.; Zada, G. Pure Endoscopic Supracerebellar Infratentorial Approach to the Pineal Region: A Case Series. World Neurosurg. 2020, 137, e603–e609. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Zhou, Q.; Zhu, W.; Wu, Q.; Xie, T.; Wu, S.; Hu, F.; Yu, Y.; Sun, C.; Li, C.; et al. The Purely Endoscopic Supracerebellar Infratentorial Approach for Resecting Pineal Region Tumors with Preservation of Cerebellomesencephalic Vein: Technical Note and Preliminary Clinical Outcomes. World Neurosurg. 2019, 128, e334–e339. [Google Scholar] [CrossRef]
- Aoyama, H.; Shirato, H.; Ikeda, J.; Fujieda, K.; Miyasaka, K.; Sawamura, Y. Induction chemotherapy followed by low-dose involved-field radiotherapy for intracranial germ cell tumors. J. Clin. Oncol. 2002, 20, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, H.; Motomura, K.; Ohka, F.; Aoki, K.; Tanahashi, K.; Hirano, M.; Chalise, L.; Nishikawa, T.; Yamaguchi, J.; Yoshida, J.; et al. Long-term survival in patients with primary intracranial germ cell tumors treated with surgery, platinum-based chemotherapy, and radiotherapy: A single-institution study. J. Neurosurg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Alapetite, C.; Brisse, H.; Patte, C.; Raquin, M.A.; Gaboriaud, G.; Carrie, C.; Habrand, J.L.; Thiesse, P.; Cuilliere, J.C.; Bernier, V.; et al. Pattern of relapse and outcome of non-metastatic germinoma patients treated with chemotherapy and limited field radiation: The SFOP experience. Neuro Oncol. 2010, 12, 1318–1325. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Qi, S.-T.; Fan, J.; Fang, L.-X.; Qiu, B.-H.; Liu, Y.; Qiu, X.-Y. Bifocal germinomas in the pineal region and hypothalamo-neurohypophyseal axis: Primary or metastasis? J. Clin. Neurosci. 2016, 34, 151–157. [Google Scholar] [CrossRef]
- Shibamoto, Y.; Sasai, K.; Oya, N.; Hiraoka, M. Intracranial germinoma: Radiation therapy with tumor volume-based dose selection. Radiology 2001, 218, 452–456. [Google Scholar] [CrossRef]
- Rogers, S.J.; Mosleh-Shirazi, M.A.; Saran, F.H. Radiotherapy of localised intracranial germinoma: Time to sever historical ties? Lancet Oncol. 2005, 6, 509–519. [Google Scholar] [CrossRef]
- Lee, D.S.; Lim, D.H.; Kim, I.H.; Kim, J.-Y.; Han, J.W.; Yoo, K.H.; Park, K.D.; Park, H.J.; Chung, N.-G.; Suh, C.-O.; et al. Upfront chemotherapy followed by response adaptive radiotherapy for intracranial germinoma: Prospective multicenter cohort study. Radiother. Oncol. 2019, 138, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Jennings, M.T.; Gelman, R.; Hochberg, F. Intracranial germ-cell tumors: Natural history and pathogenesis. J. Neurosurg. 1985, 63, 155–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Park, Y.; Lee, S.U.; Kim, T.; Choi, Y.-K.; Kim, J.-Y. Differential dosimetric benefit of proton beam therapy over intensity modulated radiotherapy for a variety of targets in patients with intracranial germ cell tumors. Radiat. Oncol. 2015, 10, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kretschmar, C.; Kleinberg, L.; Greenberg, M.; Burger, P.; Holmes, E.; Wharam, M. Pre-radiation chemotherapy with response-based radiation therapy in children with central nervous system germ cell tumors: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2007, 48, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Matsutani, M.; The Japanese Pediatric Brain Tumor Study Group. Combined chemotherapy and radiation therapy for CNS germ cell tumors—The Japanese experience. J. Neuro Oncol. 2001, 54, 311–316. [Google Scholar] [CrossRef]
- Bouffet, E.; Baranzelli, M.C.; Patte, C.; Portas, M.; Edan, C.; Chastagner, P.; Mechinaud-Lacroix, F.; Kalifa, C. Combined treatment modality for intracranial germinomas: Results of a multicentre SFOP experience. Br. J. Cancer 1999, 79, 1199–1204. [Google Scholar] [CrossRef] [Green Version]
- Sawamura, Y.; Shirato, H.; Ikeda, J.; Tada, M.; Ishii, N.; Kato, T.; Abe, H.; Fujieda, K. Induction chemotherapy followed by reduced-volume radiation therapy for newly diagnosed central nervous system germinoma. J. Neurosurg. 1998, 88, 66–72. [Google Scholar] [CrossRef]
- Toll, S.A.; Jones, M.T.; Yoshida, E.J.; Dhall, G.; Olch, A.J.; Wong, K.K. The relationship between ventricular volume and whole-brain irradiation dose in central nervous system germ cell tumors. Pediatr. Blood Cancer 2019, 66, e28005. [Google Scholar] [CrossRef]
- Iorio-Morin, C.; Kano, H.; Huang, M.; Lunsford, L.D.; Simonová, G.; Liscak, R.; Cohen-Inbar, O.; Sheehan, J.; Lee, C.-C.; Wu, H.-M.; et al. Histology-Stratified Tumor Control and Patient Survival After Stereotactic Radiosurgery for Pineal Region Tumors: A Report From the International Gamma Knife Research Foundation. World Neurosurg. 2017, 107, 974–982. [Google Scholar] [CrossRef]
- Spiegler, B.J.; Bouffet, E.; Greenberg, M.L.; Rutka, J.T.; Mabbott, D.J. Change in neurocognitive functioning after treatment with cranial radiation in childhood. J. Clin. Oncol. 2004, 22, 706–713. [Google Scholar] [CrossRef]
- Padovani, L.; André, N.; Constine, L.S.; Muracciole, X. Neurocognitive function after radiotherapy for paediatric brain tumours. Nat. Rev. Neurol. 2012, 8, 578–588. [Google Scholar] [CrossRef] [PubMed]
- Mulhern, R.K.; Merchant, T.E.; Gajjar, A.; Reddick, W.E.; Kun, L.E. Late neurocognitive sequelae in survivors of brain tumours in childhood. Lancet Oncol. 2004, 5, 399–408. [Google Scholar] [CrossRef]
- Yang, J.C.; Terezakis, S.A.; Dunkel, I.J.; Gilheeney, S.W.; Wolden, S.L. Intensity-Modulated Radiation Therapy with Dose Painting: A Brain-Sparing Technique for Intracranial Germ Cell Tumors. Pediatr. Blood Cancer 2016, 63, 646–651. [Google Scholar] [CrossRef] [Green Version]
- Phi, J.H.; Cho, B.-K.; Kim, S.-K.; Paeng, J.C.; Kim, I.-O.; Kim, I.H.; Kim, D.G.; Jung, H.-W.; Kim, J.E.; Wang, K.-C. Germinomas in the basal ganglia: Magnetic resonance imaging classification and the prognosis. J. Neuro Oncol. 2010, 99, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.; Kilday, J.-P.; Laperriere, N.; Janzen, L.; Drake, J.; Bouffet, E.; Bartels, U. Outcomes of children with central nervous system germinoma treated with multi-agent chemotherapy followed by reduced radiation. J. Neuro Oncol. 2016, 127, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Shikama, N.; Ogawa, K.; Tanaka, S.; Toita, T.; Nakamura, K.; Uno, T.; Ohnishi, H.; Itami, J.; Tada, T.; Saeki, N. Lack of benefit of spinal irradiation in the primary treatment of intracranial germinoma: A multiinstitutional, retrospective review of 180 patients. Cancer 2005, 104, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.; Goddard, K.; Laperriere, N.; Dang, J.; Bouffet, E.; Bartels, U.; Hodgson, D.; Tyldesley, S.; Hukin, J.; Cheng, S.; et al. Long term toxicity of intracranial germ cell tumor treatment in adolescents and young adults. J. Neuro Oncol. 2020, 149, 523–532. [Google Scholar] [CrossRef]
- Xiang, B.; Zhu, X.; He, M.; Wu, W.; Pang, H.; Zhang, Z.; Yang, Y.; Li, Y.; Wang, Y.; Wang, Y.; et al. Pituitary Dysfunction in Patients with Intracranial Germ Cell Tumors Treated with Radiotherapy. Endocr. Pract. 2020, 26, 1458–1468. [Google Scholar] [CrossRef]
- Kumanogoh, A.; Kasayama, S.; Kouhara, H.; Koga, M.; Arita, N.; Hayakawa, T.; Kishimoto, T.; Sato, B. Effects of therapy on anterior pituitary functions in patients with primary intracranial germ cell tumor. Endocr. J. 1994, 41, 287–292. [Google Scholar] [CrossRef] [Green Version]
- Ueba, T.; Yamashita, K.; Fujisawa, I.; Nakao, S.; Ooyama, K.; Yorihuji, T.; Kato, S.F.; Seto, S.; Kageyama, N. Long-term follow-up of 5 patients with intracranial germinoma initially treated by chemotherapy alone. Acta Neurochir. 2007, 149, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Nam, D.-H.; Wang, K.-C.; Shin, C.-H.; Yang, S.-W.; Cho, B.-K. A simple method of predicting hormonal outcome in children with intracranial germinoma. Child’s Nerv. Syst. 1999, 15, 179–184. [Google Scholar] [CrossRef]
- Matsuo, A.; Kawahara, I.; Moritsuka, T.; Honda, K.; Ito, T.; Haraguchi, W.; Hiu, T.; Ono, T.; Ushijima, R.; Tsutsumi, K. A Case of Radiation-induced Glioblastoma 29 Years after Treatments for Germinoma. No Shinkei Geka 2020, 48, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.T.; Lee, D.H.; Kim, B.K.; An, H.Y.; Choi, J.Y.; Phi, J.H.; Cheon, J.-E.; Kang, H.J.; Kim, S.-K.; Kim, J.-Y.; et al. Treatment outcome and long-term follow-up of central nervous system germ cell tumor using upfront chemotherapy with subsequent photon or proton radiation therapy: A single tertiary center experience of 127 patients. BMC Cancer 2020, 20, 979. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Feng, J.; Chen, L.; Li, Y.; Wang, J.; Lv, W.; Li, Y.; Liu, Y.; Liu, S.; Luo, S.; et al. Relapse pattern and quality of life in patients with localized basal ganglia germinoma receiving focal radiotherapy, whole-brain radiotherapy, or craniospinal irradiation. Radiother. Oncol. 2021, 158, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Baroni, L.V.; Oller, A.; Freytes, C.S.; Sampor, C.V.; Pinto, N.; Fernandez, N.P.; Rugilo, C.; Lubieniecki, F.; Zubizarreta, P.; Alderete, D. Intracranial germ cells tumour: A single institution experience in Argentina. J. Neuro Oncol. 2021, 152, 363–372. [Google Scholar] [CrossRef]
- Kumar, N.; Madan, R.; Dracham, C.B.; Khosla, D.; Das, N.; Dey, T.; Elangovan, A.; Tripathi, M.; Gupta, K.; Ahuja, C.K.; et al. Multimodality treatment for Central Nervous System Germ Cell Tumors: Disease spectrum and management strategies—A tertiary care center experience from India. Clin. Neurol. Neurosurg. 2021, 202, 106481. [Google Scholar] [CrossRef]
- Kelly, C.M.; Sainz, L.G.; Chi, P. The management of metastatic GIST: Current standard and investigational therapeutics. J. Hematol. Oncol. 2021, 14, 2. [Google Scholar] [CrossRef]
- Zalcberg, J.R. Ripretinib for the treatment of advanced gastrointestinal stromal tumor. Ther. Adv. Gastroenterol. 2021, 14. [Google Scholar] [CrossRef]
- Osorio, D.S.; Finlay, J.L.; Dhall, G.; Goldman, S.; Eisenstat, D.; Brown, R.J. Feasibility of dasatinib in children and adolescents with new or recurrent central nervous system germinoma. Pediatr. Blood Cancer 2013, 60, E100–E102. [Google Scholar] [CrossRef]
- Dasatinib, Ifosfamide, Carboplatin, and Etoposide in Treating Young Patients with Metastatic or Recurrent Malignant Solid Tumors. Available online: https://clinicaltrials.gov/ct2/show/record/NCT00788125 (accessed on 14 May 2021).
- Zschäbitz, S.; Lasitschka, F.; Hadaschik, B.; Hofheinz, R.-D.; Jentsch-Ullrich, K.; Grüner, M.; Jäger, D.; Grüllich, C. Response to anti-programmed cell death protein-1 antibodies in men treated for platinum refractory germ cell cancer relapsed after high-dose chemotherapy and stem cell transplantation. Eur. J. Cancer 2017, 76, 1–7. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03158064 (accessed on 14 May 2021).
- Lee, J.H.; Eom, K.-Y.; Phi, J.H.; Park, C.-K.; Kim, S.K.; Cho, B.-K.; Kim, T.M.; Heo, D.S.; Hong, K.T.; Choi, J.Y.; et al. Long-Term Outcomes and Sequelae Analysis of Intracranial Germinoma: Need to Reduce the Extended-Field Radiotherapy Volume and Dose to Minimize Late Sequelae. Cancer Res. Treat. 2021. [Google Scholar] [CrossRef]
- Nosrati, J.; Olch, A.J.; Abel, R.J.; Wong, K. Neoadjuvant Chemotherapy and Whole Ventricular Irradiation for Pure Intracranial Germinoma: A Comparison of Three Brain-Sparing Techniques. Cureus 2021, 13, e13670. [Google Scholar] [CrossRef]
- Rajagopal, R.; Leong, S.H.; Jawin, V.; Foo, J.C.; Ahmad Bahuri, N.F.; Mun, K.S.; Azman, R.R.; Loh, J.; Yap, T.Y.; Ariffin, H.; et al. Challenges in the Management of Childhood Intracranial Germ Cell Tumors in Middle-Income Countries: A 20-Year Retrospective Review From a Single Tertiary Center in Malaysia. J. Pediatr. Hematol. Oncol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Chou, Y.-C.; Wu, Y.-Y.; Hung, S.-P.; Tsang, N.-M.; Pai, P.-C.; Jaing, T.-H.; Lin, C.-Y.; Hsieh, C.-E.; Fan, K.-H.; Kao, W.-H.; et al. Treatment of Primary Central Nervous System Germinomas With Short-course Induction Chemotherapy Followed by Low-dose Radiotherapy Without a Tumor Bed Boost: Prognostic Impact of Human Chorionic Gonadotropin. J. Pediatr. Hematol. Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Lv, W.; Li, C.; Yang, J.; Chen, J.; Feng, J.; Chen, L.; Ma, Z.; Li, Y.; Wang, J.; et al. Comparison between Craniospinal Irradiation and Limited-Field Radiation in Patients with Non-metastatic Bifocal Germinoma. Cancer Res. Treat. 2020, 52, 1050–1058. [Google Scholar] [CrossRef]
- Takada, A.; Ii, N.; Hirayama, M.; Toyoda, H.; Matsubara, T.; Toyomasu, Y.; Kawamura, T.; Daimon, T.; Sakuma, H.; Nomoto, Y. Long-term follow-up of intensive chemotherapy followed by reduced-dose and reduced-field irradiation for intracranial germ cell tumor. J. Neurosurg. Pediatr. 2018, 23, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Weksberg, D.C.; Shibamoto, Y.; Paulino, A.C. Bifocal intracranial germinoma: A retrospective analysis of treatment outcomes in 20 patients and review of the literature. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1341–1351. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, S.M.; Trofimov, A.; Safai, S.; Adams, J.; Fullerton, B.; Ebb, D.; Tarbell, N.J.; Yock, T.I. Proton radiotherapy for pediatric central nervous system germ cell tumors: Early clinical outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 121–129. [Google Scholar] [CrossRef]
- Eom, K.-Y.; Kim, I.H.; Park, C.I.; Kim, H.J.; Kim, J.H.; Kim, K.; Kim, S.K.; Wang, K.-C.; Cho, B.-G.; Jung, H.-W.; et al. Upfront chemotherapy and involved-field radiotherapy results in more relapses than extended radiotherapy for intracranial germinomas: Modification in radiotherapy volume might be needed. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Modak, S.; Gardner, S.; Dunkel, I.J.; Balmaceda, C.; Rosenblum, M.K.; Miller, D.C.; Halpern, S.; Finlay, J.L. Thiotepa-based high-dose chemotherapy with autologous stem-cell rescue in patients with recurrent or progressive CNS germ cell tumors. J. Clin. Oncol. 2004, 22, 1934–1943. [Google Scholar] [CrossRef] [PubMed]
- Haas-Kogan, D.A.; Missett, B.T.; Wara, W.M.; Donaldson, S.S.; Lamborn, K.R.; Prados, M.D.; Fisher, P.G.; Huhn, S.L.; Fisch, B.M.; Berger, M.S.; et al. Radiation therapy for intracranial germ cell tumors. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 511–518. [Google Scholar] [CrossRef]
- Fouladi, M.; Grant, R.; Baruchel, S.; Chan, H.; Malkin, D.; Weitzman, S.; Greenberg, M.L. Comparison of survival outcomes in patients with intracranial germinomas treated with radiation alone versus reduced-dose radiation and chemotherapy. Child’s Nerv. Syst. 1998, 14, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Huh, S.J.; Shin, K.H.; Kim, I.M.; Ahn, Y.C.; Ha, S.W.; Park, C.I. Radiotherapy of intracranial germinomas. Radiother. Oncol. 1996, 38, 19–23. [Google Scholar] [CrossRef]






| Neurologic Symptoms | Endocrine Symptoms | Ophthalmologic Symptoms |
|---|---|---|
| headaches | diabetes insipidus | Parinaud’s syndrome |
| nausea | GH insufficiency | visual field deficits |
| projectile vomiting | hypogonadism | acuity deficits |
| papilledema | secondary hypothyroidism | |
| lethargy hemiparesis | hypocortisolaemia (secondary adrenal insufficiency) | |
| ataxia | menstrual irregularities | |
| precocious puberty |
| Staining | Location | Germinoma Cells | Syncytiotrophoblastic Cells |
|---|---|---|---|
| PLAP | Cytoplasm | + | − |
| C-kit | Membrane | + | − |
| OCT 3/4 | Nucleus | + | − |
| HCG | Cytoplasm | − | + |
| AFP | Cytoplasm | − | − |
| CD30 | Membrane | − | + |
| CK AE1/3 | Cytoplasm | − | + |
| D2-40 | Membrane | + | − |
| LIN28 | Ribosomes | + | − |
| HPL | Cytoplasm | − | + |
| NANOG | Nucleus | + | − |
| ESRG | Nucleus | + | − |
| UTF1 | Nucleus | + | − |
| SALL4 | Nucleus | + | − |
| Genetic Alteration | Genes/Chromosomes; Comments |
|---|---|
| DNA hypomethylation | Similarity to primordial cells; genomic instability |
| Chromosomal aberrations | |
| Gains | 1q (56.7–65%), 2q, 4q, 7 (59%), 8 (67%), 11p, 12p (36.4–82%), 21q (63.6–76%) and × (53.5–72.7%) |
| Losses | 1p/q, 3p/q, 4p, 5q (39%), 9q (39%), 9p, 10p/q, 11q (41–45.5%), 11p, 13q (45–53.3%), 15q, 16p (37%), 17q (36.4%), 18p/q, 19p/q, 20p |
| Syndromes | Association with Down, Klinefelter syndromes |
| Gene mutations | |
| KIT | Gain of function mutations |
| MAPK pathway | KRAS, NRAS, HRAS, RRAS2 |
| PI3K pathway | AKT, MTOR |
| Overexpressed genes | Expressed at 4q13.3–4q28.3: DDIT4L, BANK1, CXCL9, CXCL11, HERC5, ELOVL6 |
| Genes involving self-renewal mechanisms | POU5F1 (expressed at chr1q13.13), NANOG, DPP4, KLF4 |
| Other genes | CBL, NF1, PTEN, BCORL1, NFE2L3, NFE2L3, HNRNPA2B1 |
| MiRNA dysregulation | Proposed biomarkers for diagnosis and prognosis |
| Study | KIT Mutation | RAS Mutation |
|---|---|---|
| Schulte et al. [14] | 17.3% | 34.6% |
| Fukushima et al. [86] | 40% | 20% |
| Wang et al. [87] | 24% | 19% |
| Ichimura et al. [88] | 40% | 19% |
| Kamakura et al. [89] | 23% | Not evaluated |
| Sakuma et al. [90] | 25% | Not evaluated |
| Gao et al. [91] | 5.9% | Not evaluated |
| Study | Chr. | Gene | AA Mutation | CDS Mutation |
|---|---|---|---|---|
| Ichimura et al. [88] Schulte et al. [14] Fukushima et al. [86] Wang et al. [87] Sakuma et al. [90] Takayasu et al. [95] Low et al. [92] | 4q12 | KIT | p.Asn822Tyr p.Met836Thr p.557W>R p.Arg634Trp p.Asn822Lys p.Asp816Ala p.Asn655Lys p.820D>Y p.Asp572Gly p.Trp557Cys p.Asn822Lys p.Asp816Tyr p.Trp557Cys p.Asp816Val p.Asp820His p.Leu576Pro p.D820A p.M541L | c.2464A>T c.2507T>C c.1669T>A c.1900C>T c.2466T>G c.2447A>C c.1965T>A c.2458G>T c.1715A>G c.1671G>T c.2466T>A c.2446G>T c.1671G>C c.2447A>T c.2458G>C c.1727T>C c.2459A>C c.1621A>C |
| +4q12 amplification | ||||
| Ichimura et al. [88] Schulte et al. [14] Fukusima et al. [86] Wang et al. [87] | 12p12.1 | KRAS | p.63E>K p.Gln61Arg p.Gly12Val p.Gln61His p.146A>T p.G12W | c.182A>G c.187G>A c.35G>T c.183A>C c.436G>A c.34_36delinsTGG |
| +12p12 amplification | ||||
| Ichimura et al. [88] Schulte et al. [14] Fukushima et al. [86] Wang et al. [87] Takayasu et al. [95] | 1p13.2 | NRAS | p.12G>D p.Glu63Lys p.Gln61His p.Gly13Arg p.Q61R p.G12B p.G13C p.G12S | c.35G>A c.187G>A c.183A>C c.37G>C c182A>G c.36T>C c.37G>T c.34G>A |
| Ichimura et al. [88] Fukushima et al. [86] | 11p15.5 | HRAS | p.61Q>R | c.182A>G |
| Ichimura et al. [88] Schulte et al. [14] | 11p15.2 | RRAS2 | p.Gly23Cys p.G23A p.G23S p.G24C G24D | c.67G>T GGC → GCC GGC → AGC GGC → TGC GGC → GAC |
| +11p15.2 amplification | ||||
| Ichimura et al. [88] Wang et al. [87] | 1p36.22 | MTOR | p.Ala2416Asp p.Lys1981Glu p.2327M>I p.2334L>V p.Ser2215Pro | c.7247C>A c.5941A>G c.6981G>T c.7000T>G c.6643T>C |
| Ichimura et al. [88] Wang et al. [87] | 11q23.3 | CBL | p.Leu857Phe p.Thr377Ala p.Ile199Val | c.2569C>T c.1129A>G c.595A>G |
| +11qLOH | ||||
| Ichimura et al. [88] Schulte et al. [14] | 17q11 | NF1 | p.Thr1648Ala p.Arg2258Gln p.Gly140Val | c.4942A>G c.6773G>A c.419G>T c.1392G>A (possible splice site disruption) |
| Ichimura et al. [88] Takami et al. [7] | 10q23.31 | PTEN | p.Phe273Ser p.Arg55Ser | c.818T>C c.165G>T |
| Ichimura et al. [88] Wang et al. [87] | Xq26.1 | BCORL1 | p.Thr853Asn | c.2558C>A c.1924Cdel c.4700AAdel |
| Schulte et al. [14] Wang et al. [94] | 7p15.2-p14 | NFE2L3 | Chromosome number gains | |
| Ichimura et al. [88] Schulte et al. [14] | 7p15.2 | HNRNPA2B1 | r.spl10 p.Ser212 * p.69F>S | INV10+1G>T c.635C>A c.206T>C c.878-1G>C (possible splice site disruption) |
| Study | Upregulated | Downregulated |
|---|---|---|
| Murray et al. 2020 [97] | miR-371a-3p | |
| Low et al. 2020 [92] | miR-373-3p | miR-571 |
| miR-373-5p | miR-503-5p | |
| miR-455-5p | miR-324-5p | |
| miR-650 | miR-221-3p | |
| miR-183-5p | miR-132-3p | |
| Murray et al. 2016 [99] | miR–373–3p | |
| miR–367–3p | ||
| miR–302a–3p | ||
| miR–302b–3p | ||
| Wang et al. 2010 [94] | miR-146a | |
| miR-142-5p |
| Study | No. Cases | PD-L1 Expression (Tumour Cells) | PD-1 Expression (Immune Cells) |
|---|---|---|---|
| Nishimoto et al. 2020 [101] | 8 | 100% | 100% TILs |
| Takami et al. 2019 [102] | 32 | 73.5% | 93.8% immune cells |
| Liu et al. 2018 [103] | 25 | 92% | 96% TILs |
| Wildeman et al. 2018 [104] | 21 | 90% | 48% lymphocytes, stromal cells |
| Zapka et al. 2017 [73] | 28 | 0% | 11.9% TILs |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilcus, C.; Silaghi, H.; Georgescu, C.E.; Georgiu, C.; Ciurea, A.I.; Nicoara, S.D.; Silaghi, C.A. Molecular Pathology and Targeted Therapies for Personalized Management of Central Nervous System Germinoma. J. Pers. Med. 2021, 11, 661. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11070661
Ilcus C, Silaghi H, Georgescu CE, Georgiu C, Ciurea AI, Nicoara SD, Silaghi CA. Molecular Pathology and Targeted Therapies for Personalized Management of Central Nervous System Germinoma. Journal of Personalized Medicine. 2021; 11(7):661. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11070661
Chicago/Turabian StyleIlcus, Cristina, Horatiu Silaghi, Carmen Emanuela Georgescu, Carmen Georgiu, Anca Ileana Ciurea, Simona Delia Nicoara, and Cristina Alina Silaghi. 2021. "Molecular Pathology and Targeted Therapies for Personalized Management of Central Nervous System Germinoma" Journal of Personalized Medicine 11, no. 7: 661. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11070661