
Identifying a Common Functional Framework for Apathy Large-Scale Brain Network

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
- 3D T1-Magnetization Prepared Rapid Acquisition Gradient Echo (MPRAGE), voxel size 0.8 × 0.8 × 0.8 mm3, Field of View (FOV) 214 mm × 214 mm2, TR/TE/TI = 2400/2.25/1000 ms, scan time 5:03.
- Resting-state fMRI, sequence Echo Planar Imaging-Gradient Echo (EPI-GRE), voxel-size 4 × 4 × 4 mm3, TR/TE = 1000/21.4 ms, 350 measurements, bandwidth: 2230 Hz, scan time 6:02.
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levy, R.; Dubois, B. Apathy and the functional anatomy of the prefrontal cortex-basal ganglia circuits. CEREB Cortex 2006, 16, 916–928. [Google Scholar] [CrossRef] [Green Version]
- Van Reekum, R.; Stuss, D.T.; Ostrander, L. Apathy: Why care? J. Neuropsychiatry Clin. Neurosci. 2005, 17, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Starkstein, S.E.; Mayberg, H.S.; Preziosi, T.J.; Andrezejewski, P.; Leiguarda, R.; Robinson, R.G. Reliability, validity, and clinical correlates of apathy in Parkinson’s disease. J. Neuropsychiatry Clin. Neurosci. 1992, 4, 134–139. [Google Scholar] [CrossRef]
- Levy, M.L.; Miller, B.L.; Cummings, J.L.; Fairbanks, L.A.; Craig, A. Alzheimer disease and frontotemporal dementias. Behavioral distinctions. Arch. Neurol. 1996, 53, 687–690. [Google Scholar] [CrossRef]
- Raimo, S.; Santangelo, G.; D’Iorio, A.; Trojano, L.; Grossi, D. Neural correlates of apathy in patients with neurodegenerative disorders: An activation likelihood estimation (ALE) meta-analysis. Brain Imaging Behav. 2019, 13, 1815–1834. [Google Scholar] [CrossRef] [PubMed]
- Eslinger, P.J.; Moore, P.; Antani, S.; Anderson, C.; Grossman, M. Apathy in frontotemporal dementia: Behavioral and neuroimaging correlates. Behav. Neurol. 2012, 25, 127–136. [Google Scholar] [CrossRef]
- Sheelakumari, R.; Bineesh, C.; Varghese, T.; Kesavadas, K.; Verghese, J.; Mathuranath, P.S. Neuroanatomical correlates of apathy and disinhibition in behavioural variant frontotemporal dementia. Brain Imaging Behav. 2020, 14, 2004–2011. [Google Scholar] [CrossRef] [PubMed]
- Kumfor, F.; Zhen, A.; Hodges, J.R.; Piguet, O.; Irish, M. Apathy in Alzheimer’s disease and frontotemporal dementia: Distinct clinical profiles and neural correlates. Cortex 2018, 103, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Wen, M.C.; Chan, L.L.; Tan, L.C.; Tan, E.K. Depression, anxiety, and apathy in Parkinson’s disease: Insights from neuroimaging studies. Eur. J. Neurol. 2016, 23, 1001–1019. [Google Scholar] [CrossRef]
- Reijnders, J.S.; Scholtissen, B.; Weber, W.E.J. Neuroanatomical correlates of apathy in Parkinson’s disease: A magnetic resonance imaging study using voxel-based morphometry. Mov. Disord. 2010, 25, 2318–2325. [Google Scholar] [CrossRef]
- Huang, C.; Ravdin, L.D.; Nirenberg, M.J.; Piboolnurak, P.; Severt, L.; Maniscalco, J.S.; Solnes, L.; Dorfman, B.J.; Henchcliffe, C. Neuroimaging Markers of Motor and Nonmotor Features of Parkinson’s Disease: An [18F]Fluorodeoxyglucose Positron Emission Computed Tomography Study. Dement. Geriatr. Cogn. Disord. 2013, 35, 183–196. [Google Scholar] [CrossRef]
- Farb, N.A.; Grady, C.L.; Strother, S.; Tang-Wai, D.F.; Masellis, M.; Black, S.; Freedman, M.; Pollock, B.G.; Campbell, K.L.; Hasher, L.; et al. Abnormal network connectivity in frontotemporal dementia: Evidence for prefrontal isolation. Cortex 2013, 49, 1856–1873. [Google Scholar] [CrossRef]
- Raimo, S.; Trojano, L.; Spitaleri, D.; Petretta, V.; Grossi, D.; Santangelo, G. Apathy in multiple sclerosis: A validation study of the apathy evaluation scale. J. Neurol. Sci. 2014, 347, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Marin, R.S.; Biedrzycki, R.C.; Firinciogullari, S. Reliability and validity of the Apathy Evaluation Scale. Psychiatry Res. 1991, 38, 143–162. [Google Scholar] [CrossRef]
- Dale, A.M.; Fischl, B.; Sereno, M.I. Cortical Surface-Based analysis. I. Segmentation and surface reconstruction. Neuroimage 1999, 9, 179–194. [Google Scholar] [CrossRef] [PubMed]
- Fischl, B.; Dale, A.M. Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc. Natl. Acad. Sci. USA 2000, 97, 11050–11055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitfield-Gabrieli, S.; Nieto-Castanon, A. Conn: A functional connectivity toolbox for correlated and anticorrelated brain networks. Brain Connect. 2012, 2, 125–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing author(s). J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Cummings, J.L.; Back, C. The cholinergic hypothesis of neuropsychiatric symptoms in Alzheimer’s disease. Am. J. Geriatr. Psychiatry 1998, 6, S64–S78. [Google Scholar] [CrossRef]
- Wildgruber, D.; Riecker, A.; Hertrich, I.; Erb, M.; Grodd, W.; Ethofer, T. Identification of emotional intonation evaluated by fMRI. Neuroimage 2005, 24, 1233–1241. [Google Scholar] [CrossRef] [PubMed]
- Koelsch, S.; Skouras, S.; Lohmann, G. The auditory cortex hosts network nodes influential for emotion processing: An fMRI study on music-evoked fear and joy. PLoS ONE 2018, 13, e0190057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del-Monte, J.; Bayard, S.; Graziani, P.; Gély-Nargeot, M.C. Cognitive, Emotional, and Auto-Activation Dimensions of Apathy in Parkinson’s Disease. Front. Behav. Neurosci. 2017, 11, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamboni, G.; Huey, E.D.; Krueger, F.; Nichelli, P.F.; Grafman, J. Apathy and disinhibition in frontotemporal dementia: Insights into their neural correlates. Neurology 2008, 71, 736–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baggio, H.C.; Segura, B.; Garrido-Millan, J.; Marti, M.; Compta, Y.; Valldeoriola, F.; Tolosa, E.; Junque, C. Resting-state frontostriatal functional connectivity in Parkinson’s disease—Related apathy. Mov. Disord. 2015, 30, 671–679. [Google Scholar] [CrossRef]


{kind=link}
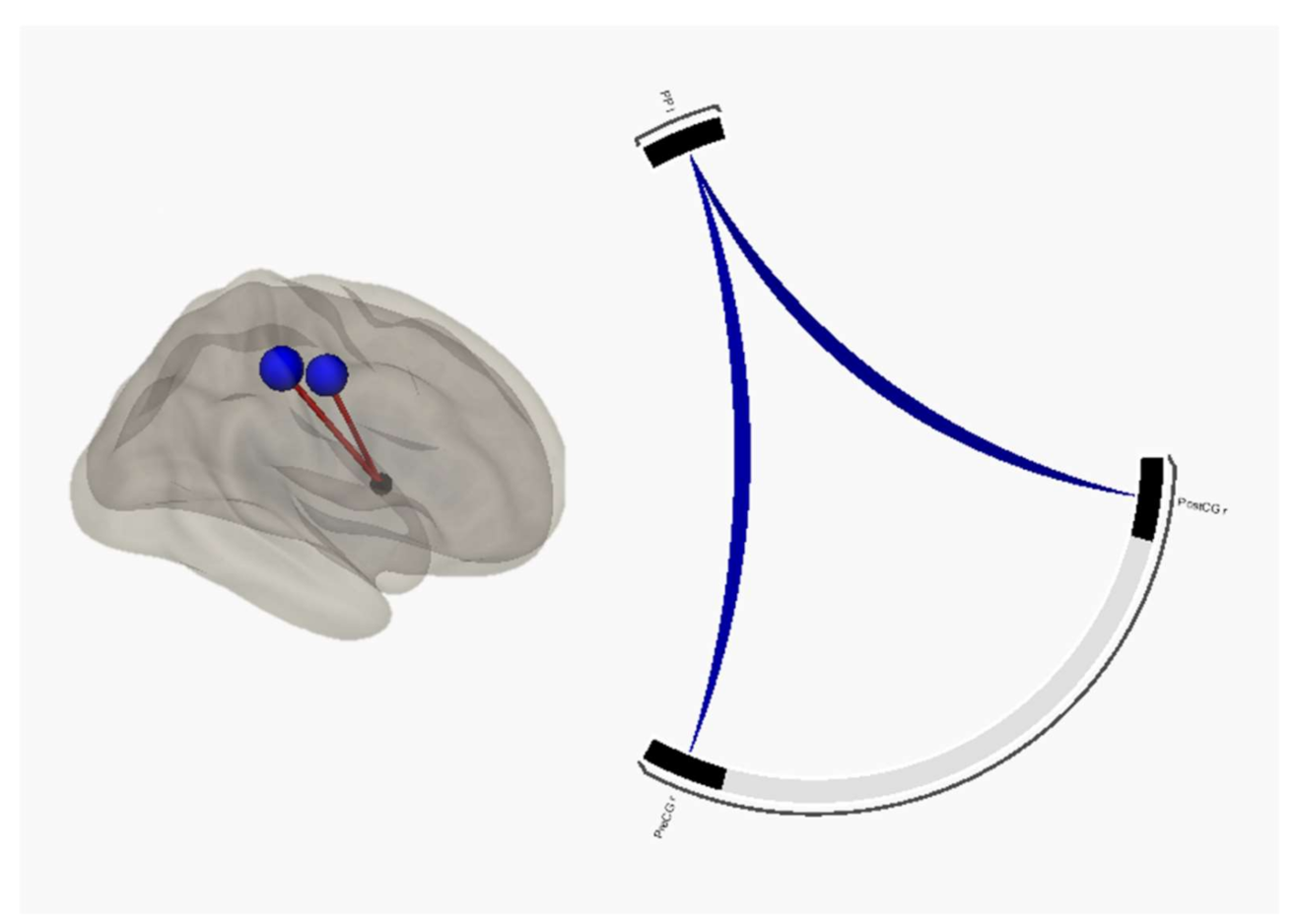
| Apathetic patients > HC | |||
| Seed | Targets | T-score | p-FDR |
| Planum polare left | Postcentral gyrus right | −5 | 0.002 |
| Precentral gyrus right | −4.7 | 0.004 | |
| Apathetic patients > Non-apathetic patients | |||
| Seed | Targets | T-score | p-FDR |
| Planum polare left | Postcentral gyrus right | −3.5 | 0.041 |
| Precentral gyrus right | −3.6 | 0.041 | |
| Apathetic FTD > HC | |||
| Seed | Targets | T-score | p-FDR |
| Planum polare left | Precentral gyrus right | −4.5 | 0.015 |
| Postcentral gyrus right | −4 | 0.041 | |
| Apathetic PD > HC | |||
| Seed | Targets | T-score | p-FDR |
| Planum polare left | Postcentral gyrus right | −4.2 | 0.016 |
| Precentral gyrus right | −3.7 | 0.021 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfano, V.; Longarzo, M.; Mele, G.; Esposito, M.; Aiello, M.; Salvatore, M.; Grossi, D.; Cavaliere, C. Identifying a Common Functional Framework for Apathy Large-Scale Brain Network. J. Pers. Med. 2021, 11, 679. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11070679
Alfano V, Longarzo M, Mele G, Esposito M, Aiello M, Salvatore M, Grossi D, Cavaliere C. Identifying a Common Functional Framework for Apathy Large-Scale Brain Network. Journal of Personalized Medicine. 2021; 11(7):679. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11070679
Chicago/Turabian StyleAlfano, Vincenzo, Mariachiara Longarzo, Giulia Mele, Marcello Esposito, Marco Aiello, Marco Salvatore, Dario Grossi, and Carlo Cavaliere. 2021. "Identifying a Common Functional Framework for Apathy Large-Scale Brain Network" Journal of Personalized Medicine 11, no. 7: 679. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11070679