
Patient Satisfaction, Functional Outcomes, and Implant Survivorship in Patients Undergoing Customized Unicompartmental Knee Arthroplasty



Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Campbell, W.C. Interposition of vit allium plates in arthroplasties of the knee: Preliminary report. Am. J. Surg. 1940, 47, 639–641. [Google Scholar] [CrossRef]
- MacIntosh, D. Hemiarthroplasty of the knee using space occupying prosthesis for painful varus and valgus deformities. J. Bone Jt. Surg. 1958, 40, 1431. [Google Scholar]
- McKeever, D.C. Tibial Plateau Prosthesis. Clin. Orthop. Relat. Res. 1960, 18, 86–95. [Google Scholar]
- Johal, S.; Nakano, N.; Baxter, M.; Hujazi, I.; Pandit, H.; Khanduja, V. Unicompartmental Knee Arthroplasty: The Past, Current Controversies, and Future Perspectives. J. Knee Surg. 2018, 31, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Jamali, A.A.; Scott, R.D.; Rubash, H.E.; Freiberg, A.A. Unicompartmental knee arthroplasty: Past, present, and future. Am. J. Orthop. 2009, 38, 17–23. [Google Scholar] [PubMed]
- Lombardi, A.V., Jr.; Berend, K.R.; Walter, C.A.; Aziz-Jacobo, J.; Cheney, N.A. Is recovery faster for mobile-bearing unicompartmental than total knee arthroplasty? Clin. Orthop. Relat. Res. 2009, 467, 1450–1457. [Google Scholar] [CrossRef] [Green Version]
- Kulshrestha, V.; Datta, B.; Kumar, S.; Mittal, G. Outcome of Unicondylar Knee Arthroplasty vs Total Knee Arthroplasty for Early Medial Compartment Arthritis: A Randomized Study. J. Arthroplast. 2017, 32, 1460–1469. [Google Scholar] [CrossRef]
- Liddle, A.D.; Pandit, H.; Judge, A.; Murray, D.W. Patient-reported outcomes after total and unicompartmental knee arthroplasty: A study of 14,076 matched patients from the National Joint Registry for England and Wales. Bone Jt. J. 2015, 97-b, 793–801. [Google Scholar] [CrossRef]
- Ode, Q.; Gaillard, R.; Batailler, C.; Herry, Y.; Neyret, P.; Servien, E.; Lustig, S. Fewer complications after UKA than TKA in patients over 85 years of age: A case-control study. Orthop. Traumatol. Surg. Res. OTSR 2018, 104, 955–959. [Google Scholar] [CrossRef]
- Lim, J.W.; Cousins, G.R.; Clift, B.A.; Ridley, D.; Johnston, L.R. Oxford unicompartmental knee arthroplasty versus age and gender matched total knee arthroplasty—Functional outcome and survivorship analysis. J. Arthroplast. 2014, 29, 1779–1783. [Google Scholar] [CrossRef]
- Wilson, H.A.; Middleton, R.; Abram, S.G.F.; Smith, S.; Alvand, A.; Jackson, W.F.; Bottomley, N.; Hopewell, S.; Price, A.J. Patient relevant outcomes of unicompartmental versus total knee replacement: Systematic review and meta-analysis. BMJ 2019, 364, l352. [Google Scholar] [CrossRef] [Green Version]
- Casper, D.S.; Fleischman, A.N.; Papas, P.V.; Grossman, J.; Scuderi, G.R.; Lonner, J.H. Unicompartmental Knee Arthroplasty Provides Significantly Greater Improvement in Function than Total Knee Arthroplasty Despite Equivalent Satisfaction for Isolated Medial Compartment Osteoarthritis. J. Arthroplast. 2019, 34, 1611–1616. [Google Scholar] [CrossRef]
- Noticewala, M.S.; Geller, J.A.; Lee, J.H.; Macaulay, W. Unicompartmental knee arthroplasty relieves pain and improves function more than total knee arthroplasty. J. Arthroplast. 2012, 27, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Koh, I.J.; Choi, Y.J.; Lee, J.Y.; In, Y. Differences in Patient-Reported Outcomes Between Unicompartmental and Total Knee Arthroplasties: A Propensity Score-Matched Analysis. J. Arthroplast. 2017, 32, 1453–1459. [Google Scholar] [CrossRef]
- Peersman, G.; Verhaegen, J.; Favier, B. The forgotten joint score in total and unicompartmental knee arthroplasty: A prospective cohort study. Int. Orthop. 2019, 43, 2739–2745. [Google Scholar] [CrossRef]
- Meric, G.; Gracitelli, G.C.; Aram, L.J.; Swank, M.L.; Bugbee, W.D. Variability in Distal Femoral Anatomy in Patients Undergoing Total Knee Arthroplasty: Measurements on 13,546 Computed Tomography Scans. J. Arthroplast. 2015, 30, 1835–1838. [Google Scholar] [CrossRef]
- Weinberg, D.S.; Streit, J.J.; Gebhart, J.J.; Williamson, D.F.; Goldberg, V.M. Important Differences Exist in Posterior Condylar Offsets in an Osteological Collection of 1,058 Femurs. J. Arthroplast. 2015, 30, 1434–1438. [Google Scholar] [CrossRef] [PubMed]
- Meier, M.; Zingde, S.; Steinert, A.; Kurtz, W.; Koeck, F.; Beckmann, J. What Is the Possible Impact of High Variability of Distal Femoral Geometry on TKA? A CT Data Analysis of 24,042 Knees. Clin. Orthop. Relat. Res. 2019, 477, 561–570. [Google Scholar] [CrossRef]
- Meier, M.; Zingde, S.; Best, R.; Schroeder, L.; Beckmann, J.; Steinert, A.F. High variability of proximal tibial asymmetry and slope: A CT data analysis of 15,807 osteoarthritic knees before TKA. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2020, 28, 1105–1112. [Google Scholar] [CrossRef]
- Takahashi, T.; Ansari, J.; Pandit, H.G. Kinematically Aligned Total Knee Arthroplasty or Mechanically Aligned Total Knee Arthroplasty. J. Knee Surg. 2018, 31, 999–1006. [Google Scholar] [CrossRef]
- Leyvraz, P.F.; Rakotomanana, L. The anatomy and function of the knee--the quest for the holy grail? J. Bone Jt. Surg. Br. Vol. 2000, 82, 1093–1094. [Google Scholar] [CrossRef]
- Patil, S.; Bunn, A.; Bugbee, W.D.; Colwell, C.W., Jr.; D’Lima, D.D. Patient-specific implants with custom cutting blocks better approximate natural knee kinematics than standard TKA without custom cutting blocks. Knee 2015, 22, 624–629. [Google Scholar] [CrossRef]
- Zeller, I.M.; Sharma, A.; Kurtz, W.B.; Anderle, M.R.; Komistek, R.D. Customized versus Patient-Sized Cruciate-Retaining Total Knee Arthroplasty: An In Vivo Kinematics Study Using Mobile Fluoroscopy. J. Arthroplast. 2017, 32, 1344–1350. [Google Scholar] [CrossRef]
- Fitz, W. Unicompartmental knee arthroplasty with use of novel patient-specific resurfacing implants and personalized jigs. J. Bone Jt. Surg. Am. Vol. 2009, 91 (Suppl. 1), 69–76. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, D.P.; Holmberg, R.R.; Quartulli, M.J.; Barnes, C.L. Tibial plateau coverage in UKA: A comparison of patient specific and off-the-shelf implants. J. Arthroplast. 2014, 29, 1694–1698. [Google Scholar] [CrossRef] [PubMed]
- Demange, M.K.; Von Keudell, A.; Probst, C.; Yoshioka, H.; Gomoll, A.H. Patient-specific implants for lateral unicompartmental knee arthroplasty. Int. Orthop. 2015, 39, 1519–1526. [Google Scholar] [CrossRef]
- Kang, K.T.; Son, J.; Suh, D.S.; Kwon, S.K.; Kwon, O.R.; Koh, Y.G. Patient-specific medial unicompartmental knee arthroplasty has a greater protective effect on articular cartilage in the lateral compartment: A Finite Element Analysis. Bone Jt. Res. 2018, 7, 20–27. [Google Scholar] [CrossRef]
- Koeck, F.X.; Beckmann, J.; Luring, C.; Rath, B.; Grifka, J.; Basad, E. Evaluation of implant position and knee alignment after patient-specific unicompartmental knee arthroplasty. Knee 2011, 18, 294–299. [Google Scholar] [CrossRef]
- Arnholdt, J.; Holzapfel, B.M.; Sefrin, L.; Rudert, M.; Beckmann, J.; Steinert, A.F. Individualized unicondylar knee replacement: Use of patient-specific implants and instruments. Oper. Orthop. Traumatol. 2017, 29, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Talmo, C.T.; Anderson, M.C.; Jia, E.S.; Robbins, C.E.; Rand, J.D.; McKeon, B.P. High Rate of Early Revision After Custom-Made Unicondylar Knee Arthroplasty. J. Arthroplast. 2018, 33, S100–S104. [Google Scholar] [CrossRef]
- Kozinn, S.C.; Marx, C.; Scott, R.D. Unicompartmental knee arthroplasty. A 4.5-6-year follow-up study with a metal-backed tibial component. J. Arthroplast. 1989, 4, S1–S9. [Google Scholar] [CrossRef]
- Kozinn, S.C.; Scott, R. Unicondylar knee arthroplasty. J. Bone Jt. Surg. Am. Vol. 1989, 71, 145–150. [Google Scholar] [CrossRef]
- Deshmukh, R.V.; Scott, R.D. Unicompartmental knee arthroplasty: Long-term results. Clin. Orthop. Relat. Res. 2001, 392, 272–278. [Google Scholar] [CrossRef]
- Scott, R.D. Unicondylar arthroplasty: Redefining itself. Orthopedics 2003, 26, 951–952. [Google Scholar] [CrossRef]
- Lyman, S.; Lee, Y.Y.; Franklin, P.D.; Li, W.; Cross, M.B.; Padgett, D.E. Validation of the KOOS, JR: A Short-form Knee Arthroplasty Outcomes Survey. Clin. Orthop. Relat. Res. 2016, 474, 1461–1471. [Google Scholar] [CrossRef] [Green Version]
- Aydemir, A.N.; Yucens, M. Trends in unicompartmental knee arthroplasty. Acta Ortop. Bras. 2020, 28, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Hip, Knee & Shoulder Arthroplasty Annual Report 2019; Australian Orthopaedic Association National Joint Replacement Registry, AOANJRR: Adelaide, South Australia. Available online: https://aoanjrr.sahmri.com/documents/10180/668596/Hip%2C+Knee+%26+Shoulder+Arthroplasty/c287d2a3-22df-a3bb-37a2-91e6c00bfcf0 (accessed on 28 May 2020).
- National Joint Registry for England Wales and Northern Ireland 16th Annual Report. Available online: https://reports.njrcentre.org.uk/Portals/0/PDFdownloads/NJR%2016th%20Annual%20Report%202019.pdf (accessed on 28 May 2020).
- Twenty Year Report, January 1999 to December 2018; New Zealand Joint Registry: Auckland, New Zealand. Available online: https://nzoa.org.nz/system/files/DH8328_NZJR_2019_Report_v4_7Nov19.pdf (accessed on 28 May 2020).
- Middleton, S.W.F.; Schranz, P.J.; Mandalia, V.I.; Toms, A.D. The largest survivorship and clinical outcomes study of the fixed bearing Stryker Triathlon Partial Knee Replacement—A multi-surgeon, single centre cohort study with a minimum of two years of follow-up. Knee 2018, 25, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Biswal, S.; Brighton, R.W. Results of unicompartmental knee arthroplasty with cemented, fixed-bearing prosthesis using minimally invasive surgery. J. Arthroplast. 2010, 25, 721–727. [Google Scholar] [CrossRef]
- Whittaker, J.P.; Naudie, D.D.; McAuley, J.P.; McCalden, R.W.; MacDonald, S.J.; Bourne, R.B. Does bearing design influence midterm survivorship of unicompartmental arthroplasty? Clin. Orthop. Relat. Res. 2010, 468, 73–81. [Google Scholar] [CrossRef] [Green Version]
- Reimann, P.; Brucker, M.; Arbab, D.; Lüring, C. Patient satisfaction—A comparison between patient-specific implants and conventional total knee arthroplasty. J. Orthop. 2019, 16, 273–277. [Google Scholar] [CrossRef]
- Raja, A.; Williamson, T.; Horst, P.K. Extrapolation of Normative KOOS, JR Data for the Young Patient Population Undergoing Knee Arthroplasty Procedures. J. Arthroplast. 2018, 33, 3655–3659. [Google Scholar] [CrossRef]
- Dawson, J.; Fitzpatrick, R.; Murray, D.; Carr, A. Questionnaire on the perceptions of patients about total knee replacement. J. Bone Jt. Surg. Br. Vol. 1998, 80, 63–69. [Google Scholar] [CrossRef]
- Polascik, B.A.; Hidaka, C.; Thompson, M.C.; Tong-Ngork, S.; Wagner, J.L.; Plummer, O.; Lyman, S. Crosswalks Between Knee and Hip Arthroplasty Short Forms: HOOS/KOOS JR and Oxford. J. Bone Jt. Surg. Am. Vol. 2020. [Google Scholar] [CrossRef]
- Pandit, H.; Jenkins, C.; Gill, H.S.; Barker, K.; Dodd, C.A.; Murray, D.W. Minimally invasive Oxford phase 3 unicompartmental knee replacement: Results of 1000 cases. J. Bone Jt. Surg. Br. Vol. 2011, 93, 198–204. [Google Scholar] [CrossRef]
- Sun, X.; Su, Z. A meta-analysis of unicompartmental knee arthroplasty revised to total knee arthroplasty versus primary total knee arthroplasty. J. Orthop. Surg. Res. 2018, 13, 158. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.B.T.; Pang, H.N.; Tay, K.J.D.; Chia, S.L.; Lo, N.N.; Yeo, S.J. Clinical outcomes and patient satisfaction following revision of failed unicompartmental knee arthroplasty to total knee arthroplasty are as good as a primary total knee arthroplasty. Knee 2019, 26, 847–852. [Google Scholar] [CrossRef]
- Epinette, J.A.; Brunschweiler, B.; Mertl, P.; Mole, D.; Cazenave, A. Unicompartmental knee arthroplasty modes of failure: Wear is not the main reason for failure: A multicentre study of 418 failed knees. Orthop. Traumatol. Surg. Res. OTSR 2012, 98, S124–S130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der List, J.P.; Zuiderbaan, H.A.; Pearle, A.D. Why Do Medial Unicompartmental Knee Arthroplasties Fail Today? J. Arthroplast. 2016, 31, 1016–1021. [Google Scholar] [CrossRef]
- Chau, R.; Gulati, A.; Pandit, H.; Beard, D.J.; Price, A.J.; Dodd, C.A.F.; Gill, H.S.; Murray, D.W. Tibial component overhang following unicompartmental knee replacement—Does it matter? Knee 2009, 16, 310–313. [Google Scholar] [CrossRef]
- Gudena, R.; Pilambaraei, M.A.; Werle, J.; Shrive, N.G.; Frank, C.B. A Safe Overhang Limit for Unicompartmental Knee Arthroplasties Based on Medial Collateral Ligament Strains: An In Vitro Study. J. Arthroplast. 2013, 28, 227–233. [Google Scholar] [CrossRef]
- Badawy, M.; Espehaug, B.; Indrekvam, K.; Havelin, L.I.; Furnes, O. Higher revision risk for unicompartmental knee arthroplasty in low-volume hospitals. Acta Orthop. 2014, 85, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Badawy, M.; Fenstad, A.M.; Bartz-Johannessen, C.A.; Indrekvam, K.; Havelin, L.I.; Robertsson, O.; W-Dahl, A.; Eskelinen, A.; Mäkelä, K.; Pedersen, A.B.; et al. Hospital volume and the risk of revision in Oxford unicompartmental knee arthroplasty in the Nordic countries -an observational study of 14,496 cases. BMC Musculoskelet. Disord. 2017, 18, 388. [Google Scholar] [CrossRef]
- Baker, P.; Jameson, S.; Critchley, R.; Reed, M.; Gregg, P.; Deehan, D. Center and surgeon volume influence the revision rate following unicondylar knee replacement: An analysis of 23,400 medial cemented unicondylar knee replacements. J. Bone Jt. Surg. Am. Vol. 2013, 95, 702–709. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
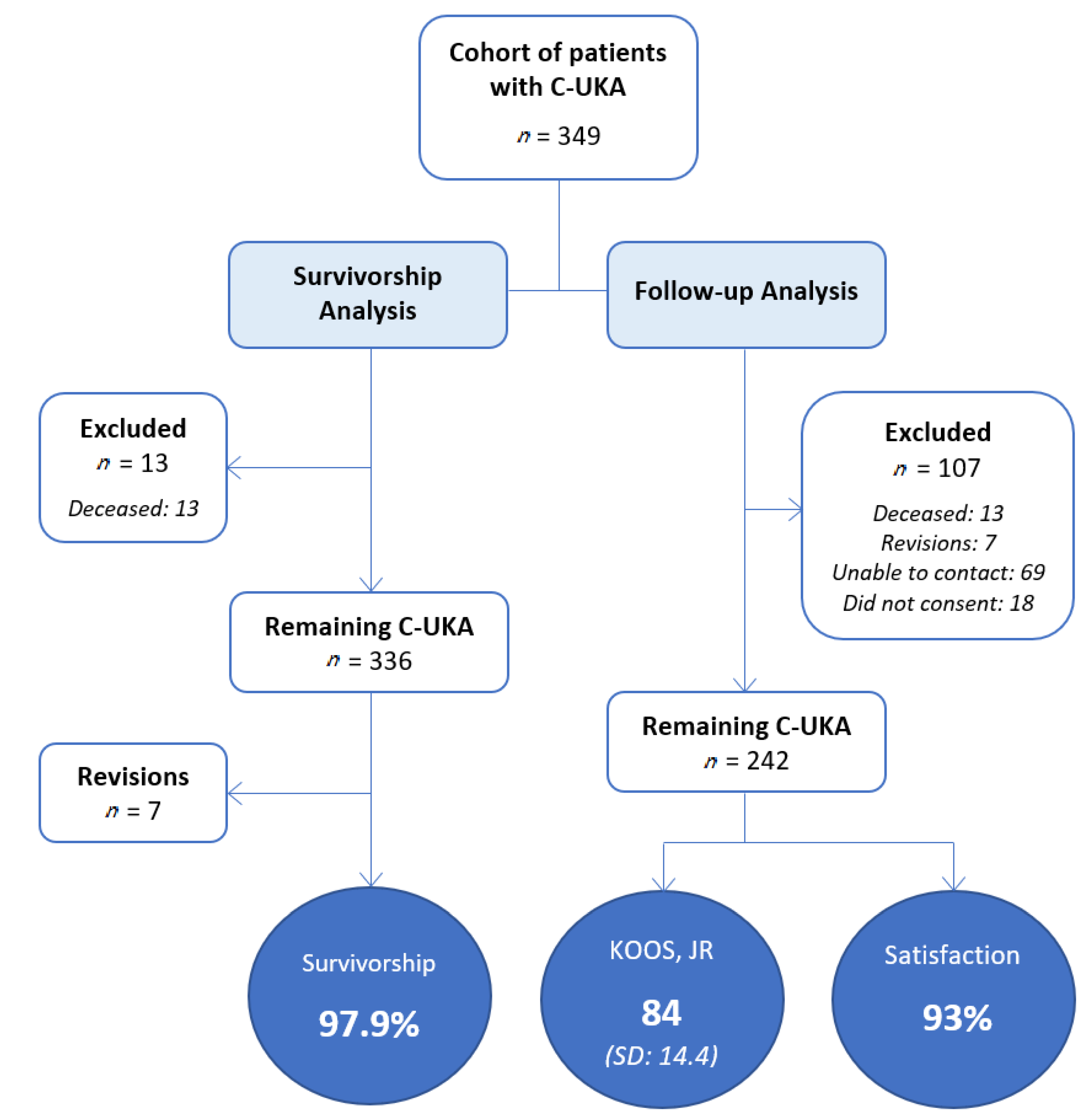
| Number of Knees Included in Revision Rate Analysis | n = 349 (287 medial, 62 lateral) | |
| Number of knees available for follow-up and outcome analysis | n = 242 | |
| Average time to follow-up | 4.2 years (range of 0.1–8.7) | |
| Gender | 40% female | 60% male |
| Age at surgery | 71.1 years (SD: 9.2) | |
| Body mass index (BMI) | 28.8 kg/m2 (SD: 4.7) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pumilia, C.A.; Schroeder, L.; Sarpong, N.O.; Martin, G. Patient Satisfaction, Functional Outcomes, and Implant Survivorship in Patients Undergoing Customized Unicompartmental Knee Arthroplasty. J. Pers. Med. 2021, 11, 753. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080753
Pumilia CA, Schroeder L, Sarpong NO, Martin G. Patient Satisfaction, Functional Outcomes, and Implant Survivorship in Patients Undergoing Customized Unicompartmental Knee Arthroplasty. Journal of Personalized Medicine. 2021; 11(8):753. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080753
Chicago/Turabian StylePumilia, Cyrus Anthony, Lennart Schroeder, Nana O. Sarpong, and Gregory Martin. 2021. "Patient Satisfaction, Functional Outcomes, and Implant Survivorship in Patients Undergoing Customized Unicompartmental Knee Arthroplasty" Journal of Personalized Medicine 11, no. 8: 753. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080753