
Enhancing the Impact of Genomics Research in Autism through Integration of Research Results into Routine Care Pathways—A Case Series

 ,
,
Abstract
:1. Introduction
2. Methods
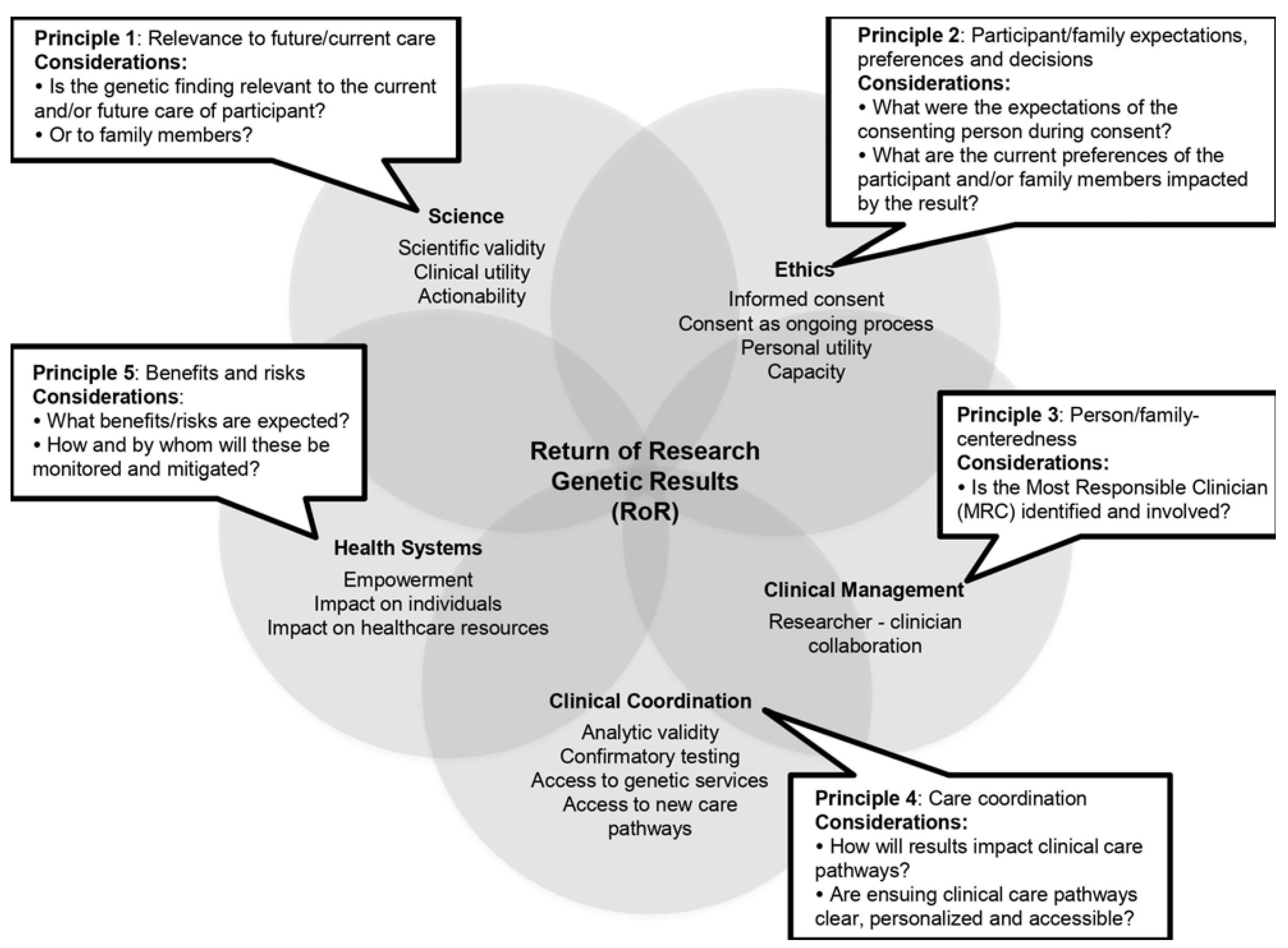
- Relevance of genetic result to current, and future care: genetic and personal health information should be synthesized to determine or confirm if the research result is actionable.
- Participant/family expectations, preferences and decisions: preferences for receipt of research results should be elicited from the individual/family, at the time of consent and when an actionable result is available.
- Person/family-centeredness: the research team should collaborate with the Most Responsible Clinician (MRC) (primary care or specialist) for the individual/family receiving the genetic result, to foster personalized healthcare pathways.
- Care coordination: routine health services (e.g., access to a genetic specialist) should be actively engaged to ensure that resulting care pathways are clear and accessible.
- Benefits and risks: potential positive and negative impacts of the genetic result on the participant/family and on clinical care pathways should be considered and managed.
3. Results
3.1. Case 3
3.2. Case 4
3.3. Cases 8 and 9
3.4. Case 15
4. Discussion
4.1. Principle 1: Relevance of Genetic Result to Current and Future Care
4.2. Principle 2: Participant/Family Expectations, Preferences and Decisions
4.3. Principle 3. Person/Family-Centeredness
4.4. Principle 4. Care Coordination
4.5. Principle 5: Benefits and Risks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hayeems, R.Z.; Hoang, N.; Chenier, S.; Stavropoulos, D.J.; Pu, S.; Weksberg, R.; Shuman, C. Capturing the clinical utility of genomic testing: Medical recommendations following pediatric microarray. Eur. J. Hum. Genet. 2015, 23, 1135–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malinowski, J.; Miller, D.T.; Demmer, L.; Gannon, J.; Pereira, E.M.; Schroeder, M.C.; Scheuner, M.T.; Tsai, A.C.; Hickey, S.E.; Shen, J.; et al. Systematic evidence-based review: Outcomes from exome and genome sequencing for pediatric patients with congenital anomalies or intellectual disability. Genet. Med. 2020, 22, 986–1004. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, G.B.; Mendelsohn, N.J.; Professional, P.; Guidelines, C. Clinical genetics evaluation in identifying the etiology of autism spectrum disorders: 2013 guideline revisions. Genet. Med. 2013, 15, 399–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barton, K.S.; Tabor, H.K.; Starks, H.; Garrison, N.A.; Laurino, M.; Burke, W. Pathways from autism spectrum disorder diagnosis to genetic testing. Genet. Med. 2018, 20, 737–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramaswami, G.; Geschwind, D.H. Chapter 21—Genetics of autism spectrum disorder. In Handbook of Clinical Neurology; Geschwind, D.H., Paulson, H.L., Klein, C., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 147, pp. 321–329. [Google Scholar]
- Kalia, S.S.; Adelman, K.; Bale, S.J.; Chung, W.K.A.; Eng, C.; Evans, J.P.; Herman, G.E.; Hufnagel, S.B.; Klein, T.E.; Korf, B.R.X.; et al. Recommendations for reporting of secondary findings in clinical exome and genome sequencing, 2016 update (ACMG SF v2.0): A policy statement of the American College of Medical Genetics and Genomics. Genet. Med. 2017, 19, 249–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vorstman, J.A.S.; Parr, J.R.; Moreno-De-Luca, D.; Anney, R.J.L.; Nurnberger, J.I., Jr.; Hallmayer, J.F. Autism genetics: Opportunities and challenges for clinical translation. Nat. Rev. Genet. 2017, 18, 362–376. [Google Scholar] [CrossRef] [PubMed]
- Knoppers, B.M.; Leroux, T.; Doucet, H.; Godard, B.; Laberge, C.; Stanton-Jean, M.; Fortin, S.; Cousineau, J.; Monardes, C.; Girard, N.; et al. Framing genomics, public health research and policy: Points to consider. Public Health Genom. 2010, 13, 224–234. [Google Scholar] [CrossRef]
- Murphy Bollinger, J.; Bridges, J.F.; Mohamed, A.; Kaufman, D. Public preferences for the return of research results in genetic research: A conjoint analysis. Genet. Med. 2014, 16, 932–939. [Google Scholar] [CrossRef] [Green Version]
- Beskow, L.M.; O’Rourke, P.P. Return of Genetic Research Results to Participants and Families: IRB Perspectives and Roles. J. Law Med. Ethics 2015, 43, 502–513. [Google Scholar] [CrossRef]
- Weiner, C.; Presidential Commission for the Study of Bioethical Issues. Anticipate and Communicate: Ethical Management of Incidental and Secondary Findings in the Clinical, Research, and Direct-to-Consumer Contexts (December 2013 Report of the Presidential Commission for the Study of Bioethical Issues). Am. J. Epidemiol. 2014, 180, 562–564. [Google Scholar] [CrossRef] [Green Version]
- Canadian Institutes of Health Research; Natural Sciences and Engineering Research Council of Canada; Social Sciences and Humanities Research Council of Canada. Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans; Government of Canada: Ottawa, ON, Canada, 2014.
- Zawati, M.H.; Knoppers, B.M. International normative perspectives on the return of individual research results and incidental findings in genomic biobanks. Genet. Med. 2012, 14, 484–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- David, K.L.; Best, R.G.; Brenman, L.M.; Bush, L.; Deignan, J.L.; Flannery, D.; Hoffman, J.D.; Holm, I.; Miller, D.T.; O’Leary, J.; et al. Patient re-contact after revision of genomic test results: Points to consider-a statement of the American College of Medical Genetics and Genomics (ACMG). Genet. Med. 2019, 21, 769–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiesner, G.L.; Kulchak Rahm, A.; Appelbaum, P.; Aufox, S.; Bland, S.T.; Blout, C.L.; Christensen, K.D.; Chung, W.K.; Clayton, E.W.; Green, R.C.; et al. Returning Results in the Genomic Era: Initial Experiences of the eMERGE Network. J. Pers. Med. 2020, 10, 30. [Google Scholar] [CrossRef]
- Fossey, R.; Kochan, D.; Winkler, E.; Pacyna, J.E.; Olson, J.; Thibodeau, S.; Connolly, J.J.; Harr, M.; Behr, M.A.; Prows, C.A.; et al. Ethical Considerations Related to Return of Results from Genomic Medicine Projects: The eMERGE Network (Phase III) Experience. J. Pers. Med. 2018, 8, 2. [Google Scholar] [CrossRef] [Green Version]
- Thorogood, A.; Dalpe, G.; Knoppers, B.M. Return of individual genomic research results: Are laws and policies keeping step? Eur. J. Hum. Genet. 2019, 27, 535–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, M.G.; Dasouki, M.J.; Zhou, X.P.; Talebizadeh, Z.; Brown, M.; Takahashi, T.N.; Miles, J.H.; Wang, C.H.; Stratton, R.; Pilarski, R.; et al. Subset of individuals with autism spectrum disorders and extreme macrocephaly associated with germline PTEN tumour suppressor gene mutations. J. Med. Genet. 2005, 42, 318–321. [Google Scholar] [CrossRef] [Green Version]
- Marcotte, L.; Crino, P.B. The neurobiology of the tuberous sclerosis complex. Neuromol. Med. 2006, 8, 531–546. [Google Scholar] [CrossRef]
- Krueger, D.A.; Northrup, H.; Roberds, S.; Smith, K.; Sampson, J.; Korf, B.; Kwiatkowski, D.J.; Mowat, D.; Nellist, M.; Povey, S.; et al. Tuberous sclerosis complex surveillance and management: Recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr. Neurol. 2013, 49, 255–265. [Google Scholar] [CrossRef] [Green Version]
- Hashemi, B.; Bassett, A.; Chitayat, D.; Chong, K.; Feldman, M.; Flanagan, J.; Goobie, S.; Kawamura, A.; Lowther, C.; Prasad, C.; et al. Deletion of 15q11.2(BP1-BP2) region: Further evidence for lack of phenotypic specificity in a pediatric population. Am. J. Med. Genet. Part A 2015, 167, 2098–2102. [Google Scholar] [CrossRef]
- Babatz, T.D.; Kumar, R.A.; Sudi, J.; Dobyns, W.B.; Christian, S.L. Copy number and sequence variants implicate APBA2 as an autism candidate gene. Autism Res. 2009, 2, 359–364. [Google Scholar] [CrossRef]
- Hand, J.L.; Runke, C.K.; Hodge, J.C. The phenotype spectrum of X-linked ichthyosis identified by chromosomal microarray. J. Am. Acad. Dermatol. 2015, 72, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Martin, A.; Gonzalez-Sarmiento, R.; De Unamuno, P. X-linked ichthyosis: An update. Br. J. Dermatol. 1999, 141, 617–627. [Google Scholar] [CrossRef]
- Caulfield, T.; McGuire, A.L.; Cho, M.; Buchanan, J.A.; Burgess, M.M.; Danilczyk, U.; Diaz, C.M.; Fryer-Edwards, K.; Green, S.K.; Hodosh, M.A.; et al. Research ethics recommendations for whole-genome research: Consensus statement. PLoS Biol. 2008, 6, e73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarvik, G.P.; Amendola, L.M.; Berg, J.S.; Brothers, K.; Clayton, E.W.; Chung, W.; Evans, B.J.; Evans, J.P.; Fullerton, S.M.; Gallego, C.J.; et al. Return of genomic results to research participants: The floor, the ceiling, and the choices in between. Am. J. Hum. Genet. 2014, 94, 818–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zawati, M.H.; Parry, D.; Thorogood, A.; Nguyen, M.T.; Boycott, K.M.; Rosenblatt, D.; Knoppers, B.M. Reporting results from whole-genome and whole-exome sequencing in clinical practice: A proposal for Canada? J. Med. Genet. 2014, 51, 68–70. [Google Scholar] [CrossRef] [PubMed]
- Fabsitz, R.R.; McGuire, A.L.; Sharp, R.R.; Puggal, M.; Beskow, L.M.; Biesecker, L.G.; Bookman, E.B.; Burke, W.; Burchard, E.G.; Church, G.; et al. Ethical and practical guidelines for reporting genetic research results to study participants: Updated guidelines from a National Heart, Lung, and Blood Institute working group. Circ. Cardiovasc. Genet. 2010, 3, 574–580. [Google Scholar] [CrossRef]
- Miller, D.T.; Adam, M.P.; Aradhya, S.; Biesecker, L.G.; Brothman, A.R.; Carter, N.P.; Church, D.M.; Crolla, J.A.; Eichler, E.E.; Epstein, C.J.; et al. Consensus statement: Chromosomal microarray is a first-tier clinical diagnostic test for individuals with developmental disabilities or congenital anomalies. Am. J. Hum. Genet. 2010, 86, 749–764. [Google Scholar] [CrossRef]
- Green, R.C.; Berg, J.S.; Grody, W.W.; Kalia, S.S.; Korf, B.R.; Martin, C.L.; McGuire, A.L.; Nussbaum, R.L.; O’Daniel, J.M.; Ormond, K.E.; et al. ACMG recommendations for reporting of incidental findings in clinical exome and genome sequencing. Genet. Med. 2013, 15, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Regier, D.A.; Peacock, S.J.; Pataky, R.; van der Hoek, K.; Jarvik, G.P.; Hoch, J.; Veenstra, D. Societal preferences for the return of incidental findings from clinical genomic sequencing: A discrete-choice experiment. CMAJ 2015, 187, E190–E197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McBride, K.A.; Hallowell, N.; Tattersall, M.H.; Kirk, J.; Ballinger, M.L.; Thomas, D.M.; Mitchell, G.; Young, M.A. Timing and context: Important considerations in the return of genetic results to research participants. J. Community Genet. 2016, 7, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Bledsoe, M.J.; Grizzle, W.E.; Clark, B.J.; Zeps, N. Practical implementation issues and challenges for biobanks in the return of individual research results. Genet. Med. 2012, 14, 478–483. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, S.; Love-Nichols, J.A.; Dies, K.A.; Ledbetter, D.H.; Martin, C.L.; Chung, W.K.; Firth, H.V.; Frazier, T.; Hansen, R.L.; Prock, L.; et al. Meta-analysis and multidisciplinary consensus statement: Exome sequencing is a first-tier clinical diagnostic test for individuals with neurodevelopmental disorders. Genet. Med. 2019, 21, 2413–2421. [Google Scholar] [CrossRef] [Green Version]
- Carroll, J.C.; Makuwaza, T.; Manca, D.P.; Sopcak, N.; Permaul, J.A.; O’Brien, M.A.; Heisey, R.; Eisenhauer, E.A.; Easley, J.; Krzyzanowska, M.K.; et al. Primary care providers’ experiences with and perceptions of personalized genomic medicine. Can. Fam. Physician 2016, 62, e626–e635. [Google Scholar] [PubMed]
- Kiedrowski, L.A.; Owens, K.M.; Yashar, B.M.; Schuette, J.L. Parents’ Perspectives on Variants of Uncertain Significance from Chromosome Microarray Analysis. J. Genet. Couns. 2016, 25, 101–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jez, S.; Martin, M.; South, S.; Vanzo, R.; Rothwell, E. Variants of unknown significance on chromosomal microarray analysis: Parental perspectives. J. Community Genet. 2015, 6, 343–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayeems, R.Z.; Babul-Hirji, R.; Hoang, N.; Weksberg, R.; Shuman, C. Parents’ Experience with Pediatric Microarray: Transferrable Lessons in the Era of Genomic Counseling. J. Genet. Couns. 2016, 25, 298–304. [Google Scholar] [CrossRef]


{kind=link}
| RoR Theme | Applicable Questions | Relevant References |
|---|---|---|
| RoR process | Formulated with aid from an independent advisory committee? | Fabsitz et al., 2010 |
| Explicitly stated in the study protocol approved by Ethics Board? | Caulfield et al., 2008 | |
| Miller et al., 2010 | ||
| Pres. Commission. 2013 | ||
| Tri-council Policy 2014 | ||
| Sénécal et al., 2015 | ||
| Thorogood et al., 2019 | ||
| Consistent with legal and ethical frameworks? | Fabstitz et al., 2010 | |
| Wolf et al., 2012 | ||
| Zawati et al., 2014 | ||
| Thorogood et al., 2019 | ||
| Current and future specific tests (e.g., microarray, WES, WGS) characteristics considered? | Fabstitz et al., 2010 | |
| Zawati et al., 2014 | ||
| Thorogood et al., 2019 | ||
| Malinowski et al., 2020 | ||
| Family context considered? | Knoppers et al., 2013 | |
| Zawati et al., 2014 | ||
| Sénécal et al., 2015 | ||
| Thorogood et al., 2019 | ||
| Management of incidental/secondary findings considered? | Wolf et al., 2008 | |
| Pres. Commission. 2013 | ||
| Green et al., 2013 | ||
| Tri-council Policy 2014 | ||
| Thorogood et al., 2019 | ||
| Expertise available to aid result interpretation? | Caulfield et al., 2008 | |
| Wolf et al., 2012 | ||
| Green et al., 2013 | ||
| Tri-council Policy 2014 | ||
| Holm et al., 2014 | ||
| Zawati et al., 2014 | ||
| Sénécal et al., 2015 | ||
| Individual preferences | Preferences for RoR of individual? | Caulfield et al., 2008 |
| Wolf et al., 2008 | ||
| Fabsitz et al., 2010 | ||
| Wolf et al., 2012 | ||
| Green et al., 2013 | ||
| Knoppers et al., 2013 | ||
| Pres. Commission 2013 | ||
| Tri-council Policy 2014 | ||
| Jarvik et al., 2014 | ||
| Holm et al., 2014 | ||
| Zawati et al., 2014 | ||
| Sénécal et al., 2015 | ||
| Thorogood et al., 2019 | ||
| Process of RoR for minors (whose guardians are consented)? | Wolf et al., 2008 | |
| Green et al., 2013 | ||
| Jarvik et al., 2014 | ||
| Zawati et al., 2014 | ||
| Sénécal et al., 2015 | ||
| Preferences for re-contact for results and/or further studies? | Wolf et al., 2008 | |
| Thorogood et al., 2019 | ||
| Involvement of Most Responsible Clinician in RoR process? | Wolf et al., 2008 | |
| Sénécal et al., 2015 | ||
| Criteria for RoR in individual cases | Is the finding primary, secondary or incidental? | Wolf et al., 2008 |
| Pres. Commission.2013 | ||
| Green et al., 2013 | ||
| Thorogood et al., 2019 | ||
| Does it have current and/or future health implication? | Caulfield et al., 2008 | |
| Wolf et al., 2008 | ||
| Fabsitz et al., 2010 | ||
| Green et al., 2013 | ||
| Knoppers et al., 2013 | ||
| Sénécal et al., 2015 | ||
| Thorogood et al., 2019 | ||
| Is it clinically actionable? | Caulfield et al., 2008 | |
| Fabsitz et al., 2010 | ||
| Wolf et al., 2012 | ||
| Green et al., 2013 | ||
| Knoppers et al., 2013 | ||
| Jarvik et al., 2014 | ||
| Sénécal et al., 2015 | ||
| Does it have therapeutic benefit? | Caulfield et al., 2008 | |
| Wolf et al., 2008 | ||
| Fabsitz et al., 2010 | ||
| Green et al., 2013 | ||
| Knoppers et al., 2013 | ||
| Jarvik et al., 2014 | ||
| Sénécal et al., 2015 | ||
| Is it analytically valid? | Caulfield et al., 2008 | |
| Wolf et al., 2008 | ||
| Fabsitz et al., 2010 | ||
| Wolf et al., 2012 | ||
| Knoppers et al., 2013 | ||
| Jarvik et al., 2014 | ||
| Holm et al., 2014 | ||
| Sénécal et al., 2015 | ||
| Thorogood et al., 2019 |
| Case | Biological Sex | Affected Region | Type | Inheritance | Clinical Significance | Age at RoR (Years) | Outcome of RoR |
|---|---|---|---|---|---|---|---|
| 1 | M | hg19 chr1: g.[5663T>G] | SNV | De novo | mTOR involvement | 6 | Result returned Clinical care provided |
| 2 | F | hg19 chr2: g.[230701696G>A] | SNV | De novo | TRIP12 involvement Nonsense mutation | 24 | Result returned Clinical care provided |
| 3 | M | hg19 chr10: g.[89692908C>T] | SNV | De novo | PTEN involvement Known missense effect Characterized syndrome | 10 | Result returned Clinical care provided |
| 4 | F | hg19 chr16: g.[2131695C>T] | SNV | De novo | TSC2 involvement Missense mutation Characterized syndrome | 19 | Result returned Clinical care provided |
| 5 | M | 1q21.1 | CNV dup | De novo | 1.4 Mb del. of 10 genes Characterized syndrome | 14 | Result returned Clinical care provided |
| 6 | M | 1q21.1 | CNV dup | De novo | 1.4 Mb del. of 10 genes Characterized syndrome | 15 | Result returned Clinical care provided |
| 7 | M | 9q21.13 | CNV del | De novo | 4.8 Mb del. of 18 genes | 12 | Lost to follow up |
| 8 | M | 15q11.2 | CNV del | Maternal | VUS 512.4 kb del. of 4 genes | 11 | Result returned Clinical care provided |
| 9 | M | 15q13.1 1q43 | CNV dup CNV dup | Maternal De novo | VUS 254 kb dup. in 1 gene VUS 28.6 kb dup. in 1 gene | 12 | Result returned Clinical care provided |
| 10 | M | 15q13.2 | CNV del | Unknown | 1.59 Mb del. of 5 genes Characterized syndrome | 10 | Results previously identified on clinical genetic testing |
| 11 | M | 16p11.2 | CNV dup | Paternal | 561 kb dup. of 30 genes Characterized syndrome | 20 | Lost to follow up |
| 12 | M | 16p11.2 | CNV dup | De novo | 633 kb dup. of 31 genes Characterized syndrome | 12 | Result returned Clinical care provided |
| 13 | M | 16p13.11 | CNV del | Paternal | 1.2 Mb del. of 13 genes Characterized syndrome | 14 | Result returned Clinical care provided |
| 14 | M | 16p13.11 | CNV del | De novo | 921 kb del. of 9 genes Characterized syndrome | 20 | Result returned Clinical care provided |
| 15 | M | Xp22.31 | CNV del | Maternal | 1.6 Mb del. of 5 genes Characterized syndrome | 22 | Result returned Clinical care provided |
| 16 | M | XXY | Aneu-ploidy | De novo | Characterized syndrome | 22 | Lost to follow up |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peltekova, I.; Buhas, D.; Stern, L.; Kirby, E.; Yusuf, A.; Elsabbagh, M. Enhancing the Impact of Genomics Research in Autism through Integration of Research Results into Routine Care Pathways—A Case Series. J. Pers. Med. 2021, 11, 755. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080755
Peltekova I, Buhas D, Stern L, Kirby E, Yusuf A, Elsabbagh M. Enhancing the Impact of Genomics Research in Autism through Integration of Research Results into Routine Care Pathways—A Case Series. Journal of Personalized Medicine. 2021; 11(8):755. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080755
Chicago/Turabian StylePeltekova, Iskra, Daniela Buhas, Lara Stern, Emily Kirby, Afiqah Yusuf, and Mayada Elsabbagh. 2021. "Enhancing the Impact of Genomics Research in Autism through Integration of Research Results into Routine Care Pathways—A Case Series" Journal of Personalized Medicine 11, no. 8: 755. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080755