
Clinical Mass Spectrometry Discovered Human IgG Sialylation as a Potential Biosignature for Kidney Function

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents and Standards
2.2. IgG Purification and Ultrahigh Performance Liquid Chromatographic (UHPLC)–Tandem MS (MS/MS) Analysis
2.3. Clinical Sample Collection and Application
2.4. ELISA Assays for Interleukin-6 (IL-6), Tumor Necrosis Factor-α (TNF-α), and Creatinine
2.5. Data Analysis and Statistical Analysis
3. Results
3.1. Clinical Participants
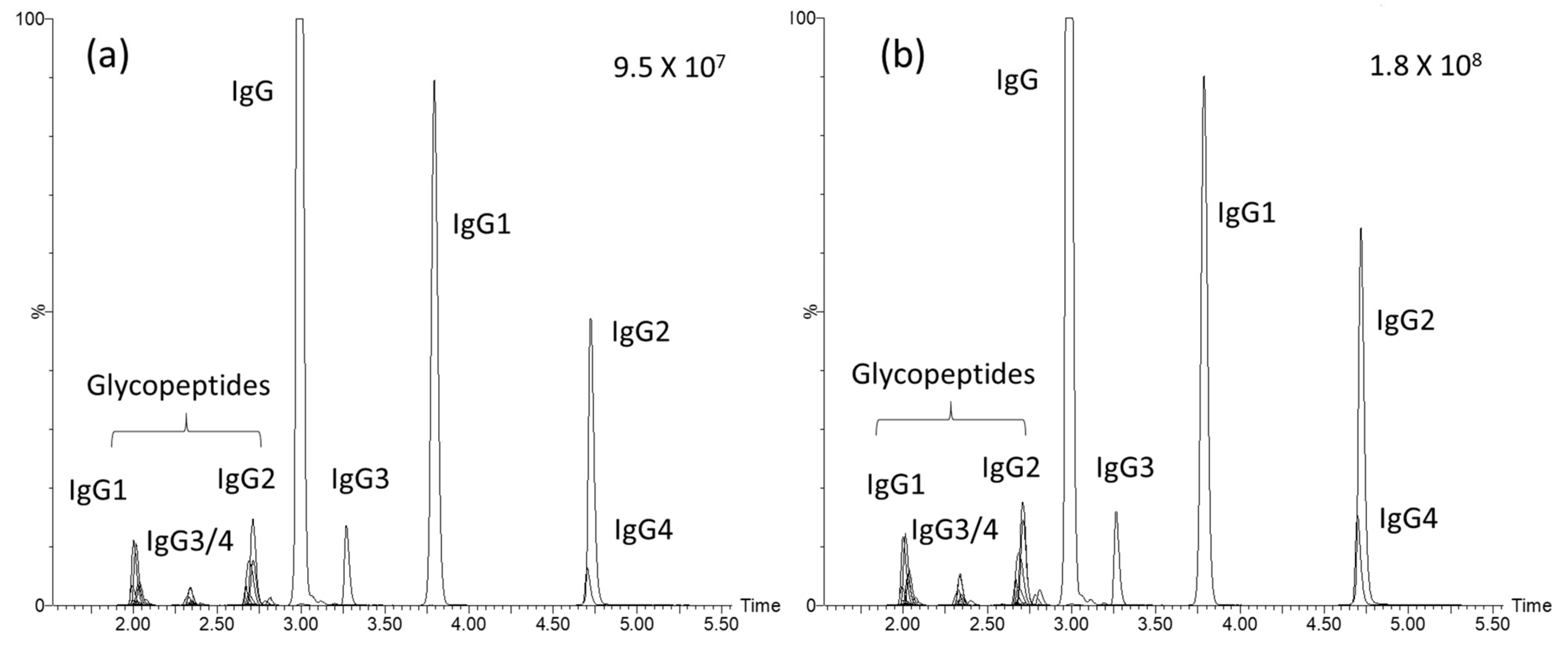
3.2. Performance of the Analytical Platform
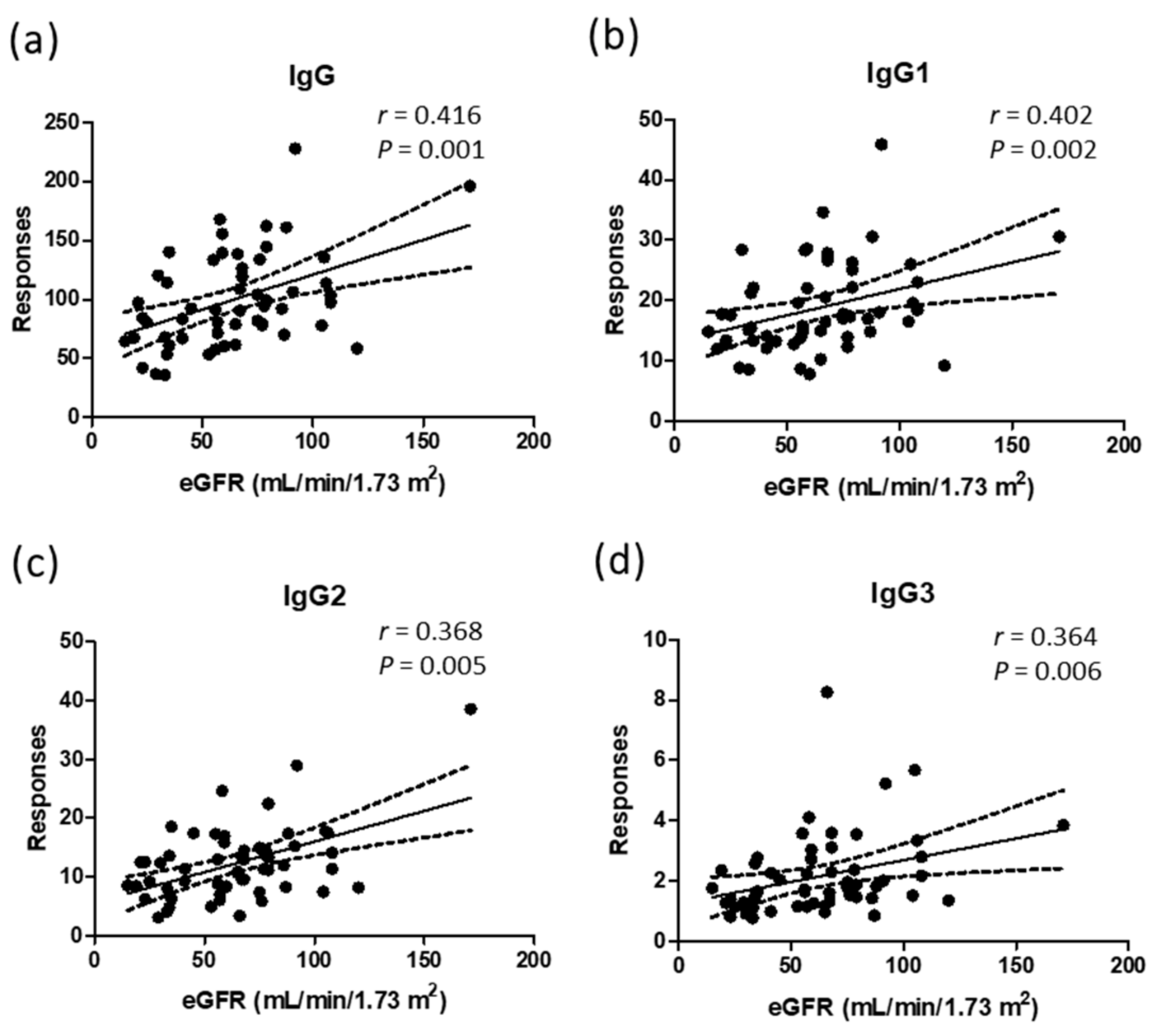
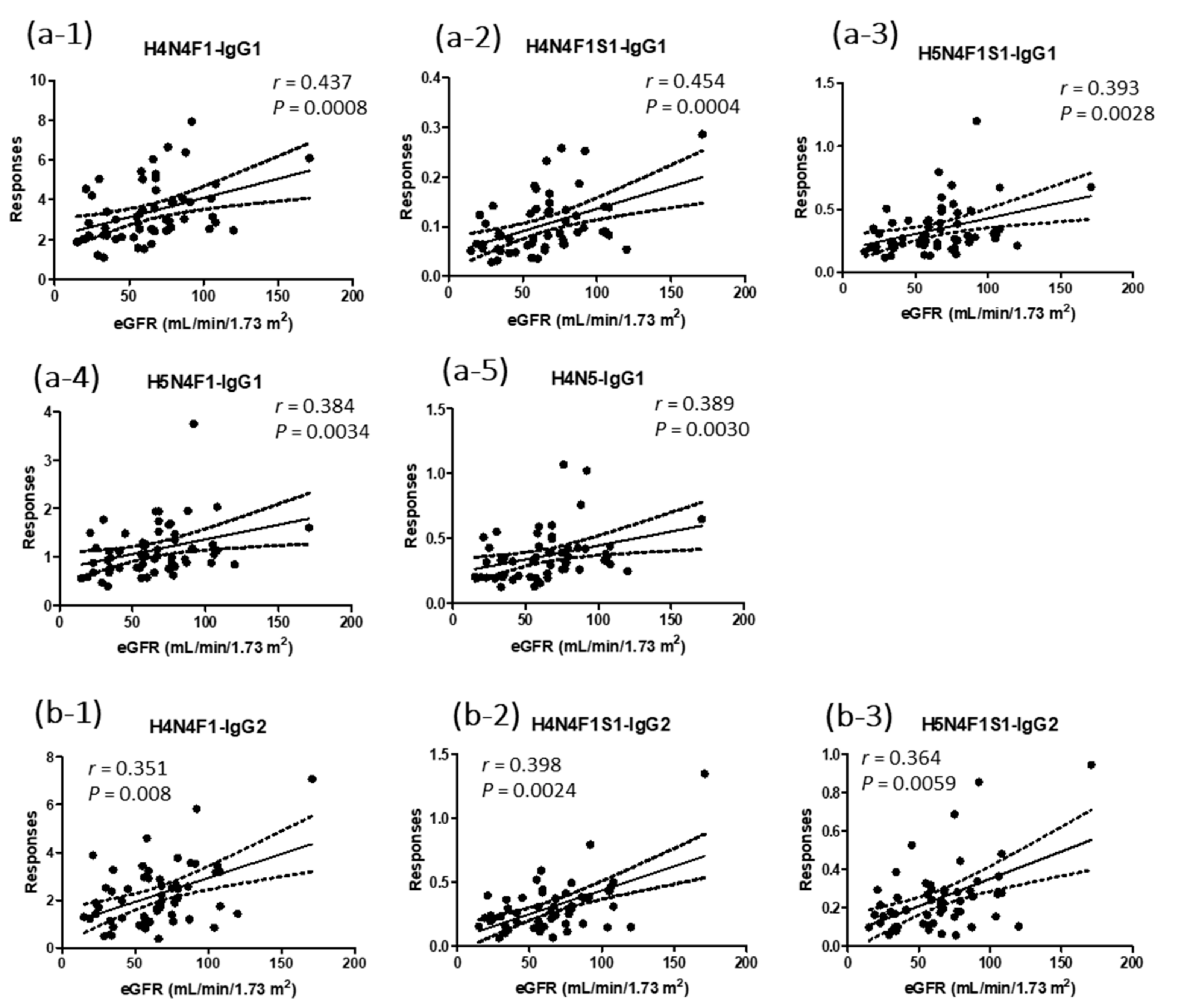
3.3. Correlations of Natural Abundances of IgG Profiles and Glycopeptides to the eGFR
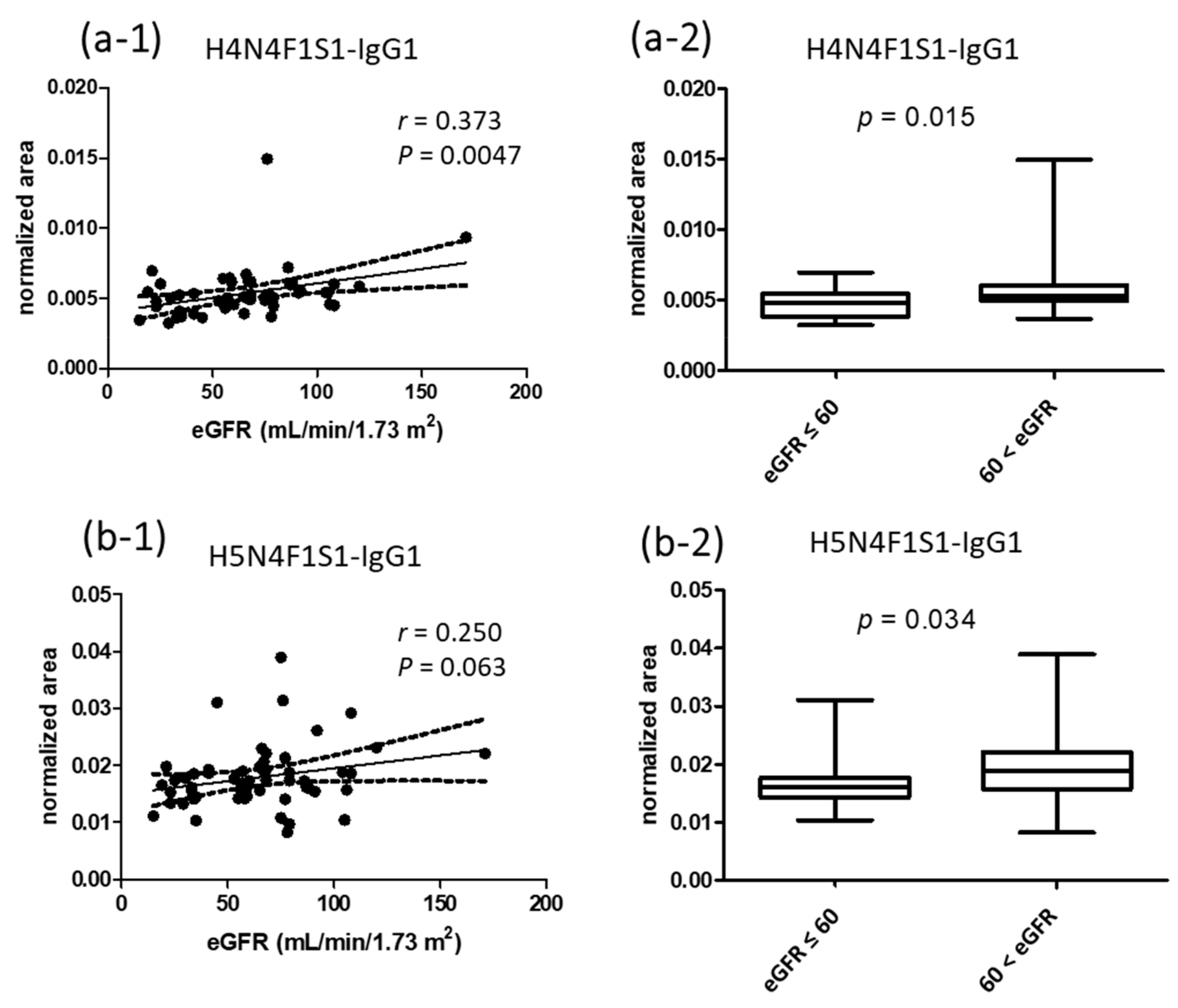
3.4. Correlations of Normalized Signals of Glycopeptides to eGFR Values
3.5. Natural Abundances of IgG Subclasses in Urine Samples
3.6. Quantification Results of IL-6 and TNF-α
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levey, A.S.; Atkins, R.; Coresh, J.; Cohen, E.P.; Collins, A.J.; Eckardt, K.U.; Nahas, M.E.; Jaber, B.L.; Jadoul, M.; Levin, A.; et al. Chronic kidney disease as a global public health problem: Approaches and initiatives—A position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007, 72, 247–259. [Google Scholar] [CrossRef] [Green Version]
- Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [CrossRef] [Green Version]
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J.; et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003, 108, 2154–2169. [Google Scholar] [PubMed]
- Brück, K.; Stel, V.S.; Gambaro, G.; Hallan, S.; Völzke, H.; Ärnlöv, J.; Kastarinen, M.; Guessous, I.; Vinhas, J.; Stengel, B.; et al. CKD Prevalence Varies across the European General Population. J. Am. Soc. Nephrol. Jasn 2016, 27, 2135–2147. [Google Scholar] [CrossRef]
- Stanifer, J.W.; Jing, B.; Tolan, S.; Helmke, N.; Mukerjee, R.; Naicker, S.; Patel, U. The epidemiology of chronic kidney disease in sub-Saharan Africa: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e174–e181. [Google Scholar] [CrossRef] [Green Version]
- Wen, C.P.; Cheng, T.Y.; Tsai, M.K.; Chang, Y.C.; Chan, H.T.; Tsai, S.P.; Chiang, P.H.; Hsu, C.C.; Sung, P.K.; Hsu, Y.H.; et al. All-cause mortality attributable to chronic kidney disease: A prospective cohort study based on 462 293 adults in Taiwan. Lancet 2008, 371, 2173–2182. [Google Scholar]
- Coresh, J.; Selvin, E.; Stevens, L.A.; Manzi, J.; Kusek, J.W.; Eggers, P.; van Lente, F.; Levey, A.S. Prevalence of chronic kidney disease in the United States. JAMA 2007, 298, 2038–2047. [Google Scholar] [CrossRef] [Green Version]
- Stevens, P.E.; Levin, A. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar]
- Klein, J.; Kavvadas, P.; Prakoura, N.; Karagianni, F.; Schanstra, J.P.; Bascands, J.L.; Charonis, A. Renal fibrosis: Insight from proteomics in animal models and human disease. Proteomics 2011, 11, 805–815. [Google Scholar]
- Ahn, J.M.; Kim, B.G.; Yu, M.H.; Lee, I.K.; Cho, J.Y. Identification of diabetic nephropathy-selective proteins in human plasma by multi-lectin affinity chromatography and LC-MS/MS, Proteomics. Clin. Appl. 2010, 4, 644–653. [Google Scholar] [CrossRef]
- Vivekanandan-Giri, A.; Slocum, J.L.; Buller, C.L.; Basrur, V.; Ju, W.; Pop-Busui, R.; Lubman, D.M.; Kretzler, M.; Pennathur, S. Urine glycoprotein profile reveals novel markers for chronic kidney disease. Int. J. Proteom. 2011, 2011, 214715. [Google Scholar] [CrossRef] [PubMed]
- Rossing, K.; Mischak, H.; Dakna, M.; Zürbig, P.; Novak, J.; Julian, B.A.; Good, D.M.; Coon, J.J.; Tarnow, L.; Rossing, P. Urinary proteomics in diabetes and CKD. J. Am. Soc. Nephrol. 2008, 19, 1283–1290. [Google Scholar] [CrossRef]
- Doshi, M.; Lahoti, A.; Danesh, F.R.; Batuman, V.; Sanders, P.W. Paraprotein-Related Kidney Disease: Kidney Injury from Paraproteins-What Determines the Site of Injury? Clin. J. Am. Soc. Nephrol. 2016, 11, 2288–2294. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.T.; Chang, M.C.; Tsai, Y.J.; Ferng, C.; Shih, H.C.; Kuo, Y.P.; Chen, C.H.; Tsai, I.L. Method development of immunoglobulin G purification from micro-volumes of human serum for untargeted and targeted proteomics-based antibody repertoire studies. J. Food Drug Anal. 2019, 27, 475–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gudelj, I.; Lauc, G.; Pezer, M. Immunoglobulin G glycosylation in aging and diseases. Cell Immunol. 2018, 333, 65–79. [Google Scholar] [CrossRef]
- Barrios, C.; Zierer, J.; Gudelj, I.; Štambuk, J.; Ugrina, I.; Rodríguez, E.; Soler, M.J.; Pavić, T.; Šimurina, M.; Keser, T.; et al. Glycosylation Profile of IgG in Moderate Kidney Dysfunction. J. Am. Soc. Nephrol. 2016, 27, 933–941. [Google Scholar] [CrossRef] [Green Version]
- Shiao, J.Y.; Chang, Y.T.; Chang, M.C.; Chen, M.X.; Liu, L.W.; Wang, X.Y.; Tsai, Y.J.; Kuo, T.C.; Tsai, I.L. Development of efficient on-bead protein elution process coupled to ultra-high performance liquid chromatography-tandem mass spectrometry to determine immunoglobulin G subclass and glycosylation for discovery of bio-signatures in pancreatic disease. J. Chromatogr. A 2020, 1621, 461039. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, R.; Lehoux, S.; Maeda, K.; Tsokos, M.G.; Krishfield, S.; Ellezian, L.Y.; Pollak, M.; Stillman, I.E.; Cummings, R.D.; Tsokos, G.C. Aberrantly glycosylated IgG elicits pathogenic signaling in podocytes and signifies lupus nephritis. JCI Insight 2021, 6, e147789. [Google Scholar] [CrossRef]
- Sołkiewicz, K.; Krotkiewski, H.; Jędryka, M.; Kratz, E.M. Variability of serum IgG sialylation and galactosylation degree in women with advanced endometriosis. Sci. Rep. 2021, 11, 5586. [Google Scholar] [CrossRef]
- Weng, C.H.; Hu, C.C.; Yu, C.C.; Lin, J.L.; Yang, C.W.; Hung, C.C.; Hsu, C.W.; Yen, T.H. Immunoglobulin G levels can predict non-diabetic renal disease in patients with type 2 diabetes mellitus. J. Diabetes 2012, 4, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, R.; Maeda, K.; Tsokos, M.G.; Pavlakis, M.; Stillman, I.E.; Tsokos, G.C. N-glycosylated IgG in patients with kidney transplants increases calcium/calmodulin kinase IV in podocytes and causes injury. Am. J. Transplant. 2021, 21, 148–160. [Google Scholar] [CrossRef]
- Singh, S.S.; Heijmans, R.; Meulen, C.K.E.; Lieverse, A.G.; Gornik, O.; Sijbrands, E.J.G.; Lauc, G.; van Hoek, M. Association of the IgG N-glycome with the course of kidney function in type 2 diabetes. BMJ Open Diabetes Res. Care 2020, 8, e001026. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.T.; Ahmed, F.A.; Hamm, L.L.; Teran, F.J.; Chen, C.S.; Liu, Y.; Shah, K.; Rifai, N.; Batuman, V.; Simon, E.E.; et al. Association of C-reactive protein, tumor necrosis factor-alpha, and interleukin-6 with chronic kidney disease. BMC Nephrol. 2015, 16, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pucic, M.; Muzinic, A.; Novokmet, M.; Skledar, M.; Pivac, N.; Lauc, G.; Gornik, O. Changes in plasma and IgG N-glycome during childhood and adolescence. Glycobiology 2012, 22, 975–982. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.; Wang, Y.; Qiu, L.; Qin, X.; Liu, H.; Wang, X.; Wang, Y.; Song, G.; Li, F.; Guo, Y.; et al. Human IgG Fc-glycosylation profiling reveals associations with age, sex, female sex hormones and thyroid cancer. J. Proteom. 2012, 75, 2824–2834. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| eGFR (mL/min/1.73 m2) | eGFR ≤ 30 | 30 < eGFR ≤ 60 | 60 < eGFR ≤ 90 | 90 < eGFR |
|---|---|---|---|---|
| Number of participants | 8 | 19 | 21 | 9 |
| Gender | Male: 8 | Male: 14; Female: 5 | Male: 10; Female: 11 | Male: 3; Female: 6 |
| Age (years old) | 56.5 ± 13.7 | 59.5 ± 11.9 | 62.5 ± 11.1 | 52.6 ± 16.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kao, C.-C.; Wang, S.-Y.; Chuang, Y.-K.; Lee, W.-Y.; Chang, W.-C.; Wu, M.-S.; Kuo, T.-C.; Tsai, I.-L. Clinical Mass Spectrometry Discovered Human IgG Sialylation as a Potential Biosignature for Kidney Function. J. Pers. Med. 2021, 11, 761. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080761
Kao C-C, Wang S-Y, Chuang Y-K, Lee W-Y, Chang W-C, Wu M-S, Kuo T-C, Tsai I-L. Clinical Mass Spectrometry Discovered Human IgG Sialylation as a Potential Biosignature for Kidney Function. Journal of Personalized Medicine. 2021; 11(8):761. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080761
Chicago/Turabian StyleKao, Chih-Chin, San-Yuan Wang, Yung-Kun Chuang, Wei-Yuan Lee, Wei-Chiao Chang, Mai-Szu Wu, Tai-Chih Kuo, and I-Lin Tsai. 2021. "Clinical Mass Spectrometry Discovered Human IgG Sialylation as a Potential Biosignature for Kidney Function" Journal of Personalized Medicine 11, no. 8: 761. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080761