
Impact of Pneumococcal Urinary Antigen Testing in COVID-19 Patients: Outcomes from the San Matteo COVID-19 Registry (SMACORE)

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Patients and Study Design
2.2. Microbiological Methods
2.3. Statistical Analysis
3. Results
3.1. Study Population
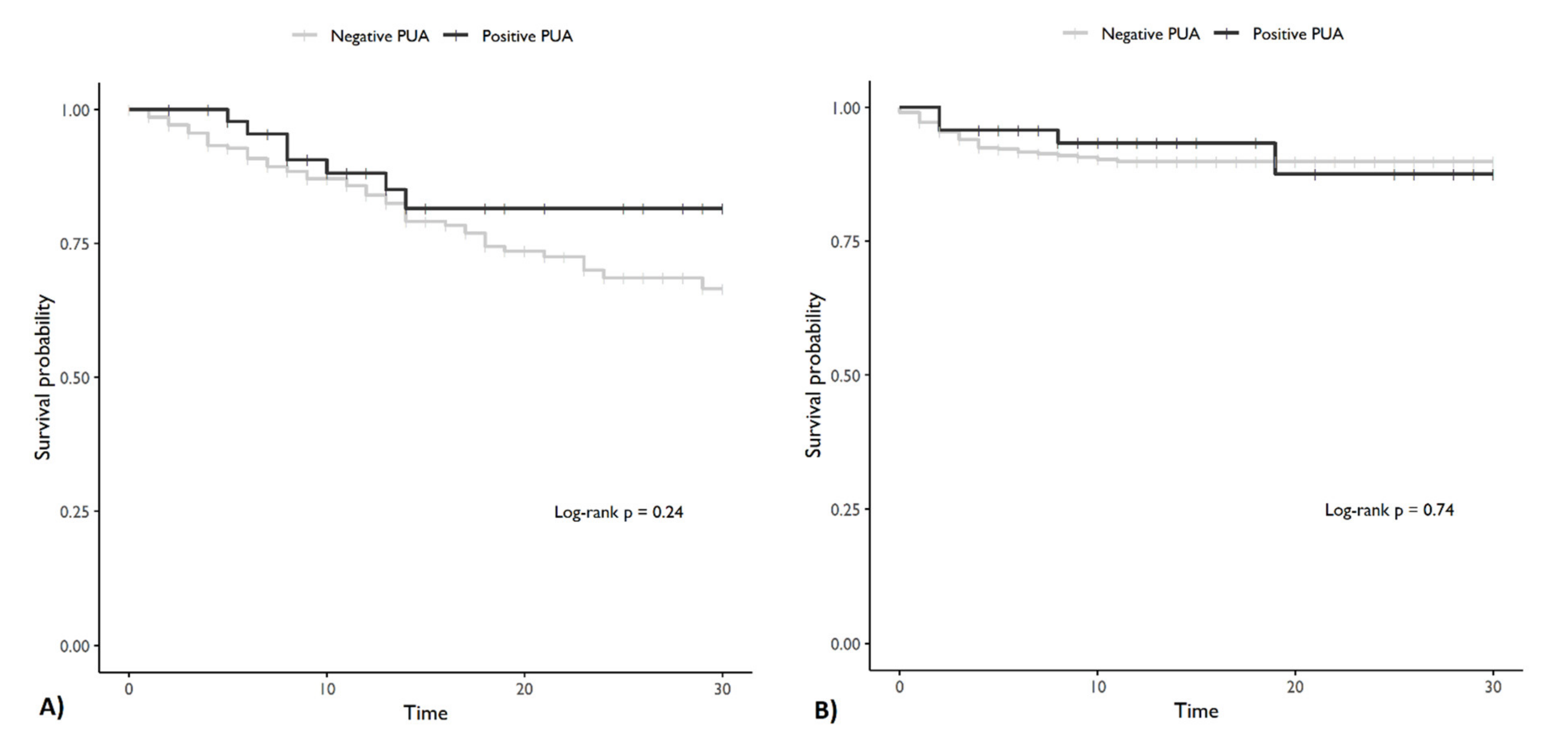
3.2. Effects of Positive Urinary Antigen on Mortality and ICU Admission
3.3. Effects of Positive Urinary Antigen on Length of Stay
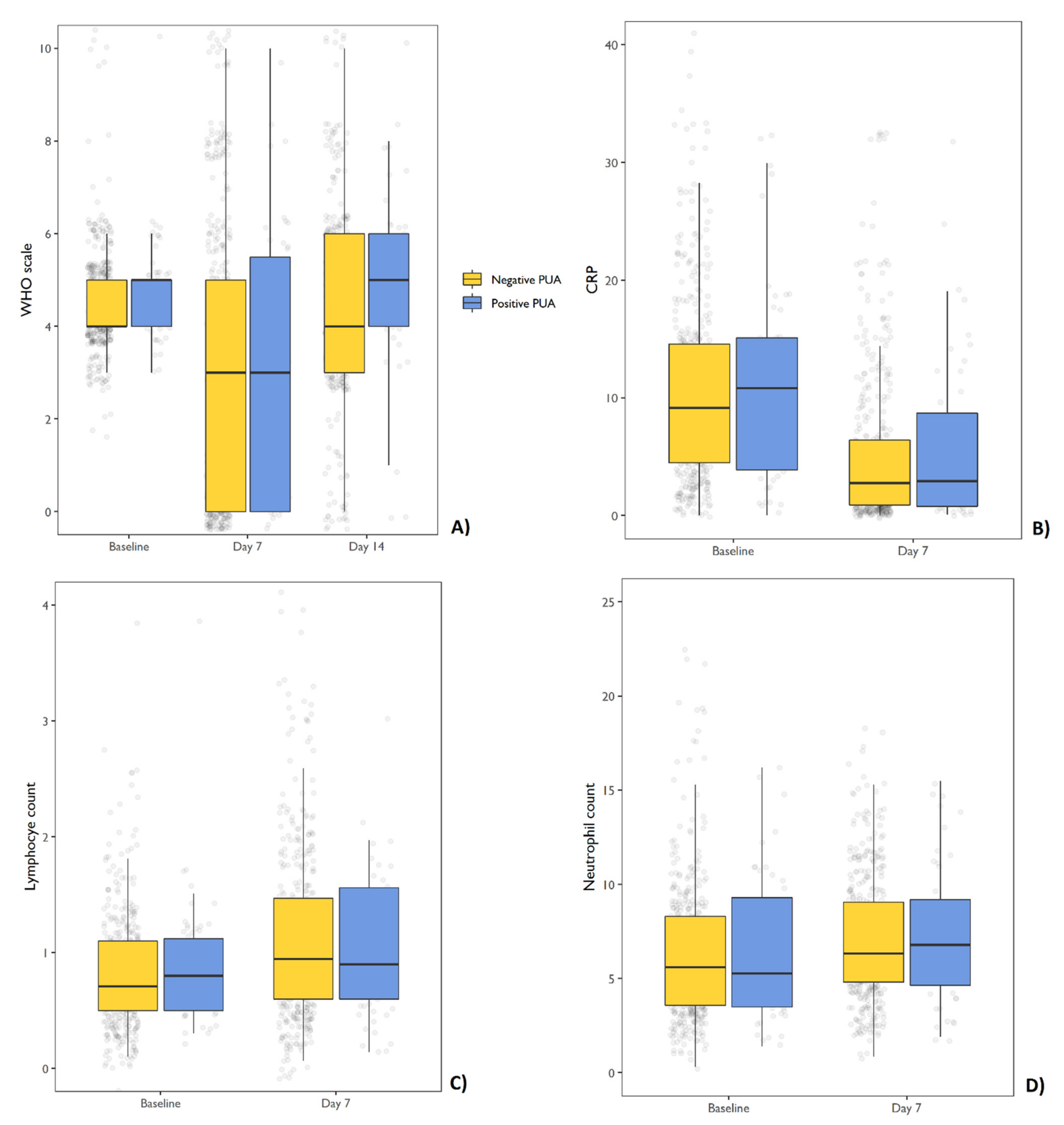
3.4. Effects of Positive Urinary Antigen on Variation of WHO Ordinal Scale and Laboratory Measures
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Esper, F.P.; Spahlinger, T.; Zhou, L. Rate and influence of respiratory virus co-infection on pandemic (H1N1) influenza disease. J. Infect. 2011, 63, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Rice, T.W.; Rubinson, L.; Uyeki, T.M.; Vaughn, F.L.; John, B.B.; Miller, R.R.; Higgs, E.; Randolph, A.; Smoot, B.E.; Thompson, B.T. Critical illness from 2009 pandemic influenza A virus and bacterial coinfection in the United States. Crit. Care Med. 2012, 40, 1487–1498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, X.; Ge, Y.; Wu, T.; Zhao, K.; Chen, Y.; Wu, B.; Zhu, F.; Zhu, B.; Cui, L. Co-infection with respiratory pathogens among COVID-2019 cases. Virus Res. 2020, 285, 198005. [Google Scholar] [CrossRef] [PubMed]
- Toombs, J.M.; Abbeele, K.V.D.; Democratis, J.; Mandal, A.K.J.; Missouris, C.G. Pneumococcal coinfection in COVID-19 patients. J. Med. Virol. 2020, 93, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Gigantesco, A.; Giuliani, M. Quality of life in mental health services with a focus on psychiatric rehabilitation practice. Annali dell’Istituto Superiore di Sanita 2011, 47, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Rothe, K.; Feihl, S.; Schneider, J.; Wallnöfer, F.; Wurst, M.; Lukas, M.; Treiber, M.; Lahmer, T.; Heim, M.; Dommasch, M.; et al. Rates of bacterial co-infections and antimicrobial use in COVID-19 patients: A retrospective cohort study in light of antibiotic stewardship. Eur. J. Clin. Microbiol. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Karami, Z.; Knoop, B.T.; Dofferhoff, A.S.M.; Blaauw, M.J.T.; Janssen, N.A.; van Apeldoorn, M.; Kerckhoffs, A.P.M.; van de Maat, J.S.; Hoogerwerf, J.J.; Oever, J.T. Few bacterial co-infections but frequent empiric antibiotic use in the early phase of hospitalized patients with COVID-19: Results from a multicentre retrospective cohort study in The Netherlands. Infect. Dis. 2020, 53, 102–110. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef]
- Sieswerda, E.; de Boer, M.G.; Bonten, M.M.; Boersma, W.G.; Jonkers, R.E.; Aleva, R.M.; Kullberg, B.-J.; Schouten, J.A.; van de Garde, E.M.; Verheij, T.J.; et al. Recommendations for antibacterial therapy in adults with COVID-19—An evidence based guideline. Clin. Microbiol. Infect. 2021, 27, 61–66. [Google Scholar] [CrossRef]
- Desai, A.; Santonocito, O.; Caltagirone, G.; Kogan, M.; Ghetti, F.; Donadoni, I.; Porro, F.; Savevski, V.; Poretti, D.; Ciccarelli, M.; et al. Effectiveness of Streptococcus Pneumoniae Urinary Antigen Testing in Decreasing Mortality of COVID-19 Co-Infected Patients: A Clinical Investigation. Medicine 2020, 56, 572. [Google Scholar] [CrossRef]
- Bartlett, J.G. Contribution of a urinary antigen assay (binax NOW) to the early diagnosis of pneumococcal pneumonia. Infect. Dis. Clin. Pract. 2004, 12, 264. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Wong, A.; Johnsson, A.; Ininbergs, K.; Athlin, S.; Özenci, V. Comparison of Four Streptococcus pneumoniae Urinary Antigen Tests Using Automated Readers. Microorganisms 2021, 9, 827. [Google Scholar] [CrossRef] [PubMed]
- Molinos, L.; Menendez, R.; Reyes, S.; Rajas, O.; Zalacain, R.; Capelastegui, A.; Cilloniz, C.; Borderias, L.; Martín-Villasclaras, J.J.; Bello, S.; et al. Sensitivity, Specificity, and Positivity Predictors of the Pneumococcal Urinary Antigen Test in Community-Acquired Pneumonia. Ann. Am. Thorac. Soc. 2015, 12, 1482–1489. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO R&D Blueprint Novel Coronavirus COVID-19 Therapeutic Trial Synopsis; World Health Organization: Geneva, Switzerland, 2020; pp. 1–9. [Google Scholar]
- Lim, R.H.; Chow, A.; Ho, H.J. Decline in pneumococcal disease incidence in the time of COVID-19 in Singapore. J. Infect. 2020, 81, e19–e21. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.R.; Yang, C.J.; Huang, W.L.; Chen, Y.H. Decline in invasive pneumococcus diseases while combating the COVID-19 pandemic in Taiwan. Kaohsiung J. Med. Sci. 2020, 36, 572–573. [Google Scholar] [CrossRef] [PubMed]
- Amin-Chowdhury, Z.; Aiano, F.; Mensah, A.; Sheppard, C.; Litt, D.; Norman, K.F.; Andrews, N.; Mary, E.; Ramsay, F.F.P.H.; Shamez, N.; et al. Impact of the COVID-19 Pandemic on Invasive Pneumococcal Disease and Risk of Pneumococcal Coinfection with SARS-CoV-2: Prospective National Cohort Study, England. Clin. Infect. Dis. 2021, 72, e65–e75. [Google Scholar] [CrossRef]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and treatment of adults with community-acquired pneumonia. Am. J. Respir. Crit. Care Med. 2019, 200, E45–E67. [Google Scholar] [CrossRef]
- Falcone, M.; Tiseo, G.; Giordano, C.; Leonildi, A.; Menichini, M.; Vecchione, A.; Pistello, M.; Guarracino, F.; Ghiadoni, L.; Forfori, F.; et al. Predictors of hospital-acquired bacterial and fungal superinfections in COVID-19: A prospective observational study. J. Antimicrob. Chemother. 2020, 1–7. [Google Scholar] [CrossRef]
- Andreo, F.; Prat, C.; Ruiz-Manzano, J.; Lores, L.; Blanco, S.; Cuesta, M.A.; Gimenez, M.; Domínguez, J. Persistence of Streptococcus pneumoniae urinary antigen excretion after pneumococcal pneumonia. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 28, 197–201. [Google Scholar] [CrossRef]
- Grijalva, C.G.; Wunderink, R.G.; Zhu, Y.; Williams, D.J.; Balk, R.; Fakhran, S.; Courtney, D.M.; Anderson, E.J.; Qi, C.; Trabue, C.; et al. In-Hospital Pneumococcal Polysaccharide Vaccination Is Associated With Detection of Pneumococcal Vaccine Sero-types in Adults Hospitalized for Community-Acquired Pneumonia. Open Forum Infect. Dis. 2015, 2. [Google Scholar] [CrossRef] [Green Version]
- Gabarre, P.; Dumas, G.; Dupont, T.; Darmon, M.; Azoulay, E.; Zafrani, L. Acute kidney injury in critically ill patients with COVID-19. Intensive Care Med. 2020, 46, 1339–1348. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Whole Sample (n = 469) | Negative PUA (n = 427) | Positive PUA (n = 42) | p-Value | |
|---|---|---|---|---|---|
| Sex, n (%) | Male | 320 (68.2) | 295 (69.1) | 25 (59.5) | |
| Female | 149 (31.8) | 132 (30.9) | 17 (40.5) | 0.27 | |
| Age, n (%) | mean (sd) | 67.6 (14.7) | 67.6 (14.7) | 67.6 (14.5) | 0.98 |
| Death, n (%) | yes | 84 (17.9) | 79 (18.5) | 5 (11.9) | |
| no | 385 (82.1) | 348 (81.5) | 37 (88.1) | 0.39 | |
| ICU admission, n (%) | yes | 43 (9.2) | 40 (9.4) | 3 (7.1) | |
| no | 426 (90.8) | 387 (90.6) | 39 (92.9) | 0.84 | |
| CCI, M (sd) | 3.5 (2.3) | 3.4 (2.3) | 3.8 (2.3) | 0.27 | |
| missing | 43 | 43 | 0 | ||
| Severe immunodepression, n (%) | 13 (3.0) | 11 (2.8) | 2 (4.9) | 0.8 | |
| missing | 39 | 38 | 1 | ||
| Previous lung disease, n (%) | No | 228 (64.0) | 205 (64.3) | 23 (62.2) | |
| Yes | 128 (36.0) | 114 (35.7) | 14 (37.8) | 0.94 | |
| missing | 113 | 108 | 5 | ||
| Days since onset of symptoms, M (sd) | 6.3 (3.8) | 6.2 (3.8) | 6.6 (3.9) | 0.53 | |
| missing | 65 | 63 | 2 | ||
| Steroid treatment before hospitalization, n (%) | No | 309 (74.5) | 281 (75.1) | 28 (68.3) | |
| Yes | 106 (25.5) | 93 (24.9) | 13 (31.7) | 0.44 | |
| missing | 54 | 53 | 1 | ||
| Antibiotic treatment before hospitalization (n of atb), n (%) | 0 | 281 (67.2) | 250 (66.5) | 31 (73.8) | |
| 1 | 125 (29.9) | 117 (31.1) | 8 (19.0) | ||
| 2 | 12 (2.9) | 9 (2.4) | 3 (7.1) | 0.07 | |
| missing | 51 | 51 | 0 | ||
| Antibiotic treatment during hospitalization (n of atb), n (%) | 0 | 18 (4.7) | 16 (4.7) | 2 (5.1) | |
| 1 | 254 (66.7) | 227 (66.4) | 27 (69.2) | ||
| 2 | 103 (27.0) | 94 (27.5) | 9 (23.1) | ||
| 3 | 6 (1.6) | 5 (1.5) | 1 (2.6) | 0.9 | |
| Radiological findings at CT scan | No CT scan | 256 (71.9) | 228 (71.7) | 28 (73.7) | |
| GGO | 21 (5.9) | 20 (6.3) | 1 (2.6) | ||
| FO | 8 (2.2) | 7 (2.2) | 1 (2.6) | ||
| GGO+FO | 69 (19.4) | 61 (19.2) | 8 (21.1) | ||
| others | 2 (0.6) | 2 (0.6) | 0 (0.0) | 0.89 | |
| missing | 113 | 109 | 4 | ||
| Radiological findings at chest X-ray | 0 | 17 (4.8) | 17 (5.3) | 0 (0.0) | |
| GGO | 126 (35.3) | 120 (37.6) | 6 (15.8) | ||
| FO | 55 (15.4) | 45 (14.1) | 10 (26.3) | ||
| GGO+FO | 151 (42.3) | 130 (40.8) | 21 (55.3) | ||
| others | 8 (2.2) | 7 (2.2) | 1 (2.6) | 0.02 | |
| missing | 112 | 108 | 4 | ||
| WHO ordinal scale at admission | mean (sd) | 4.5 (1.1) | 4.5 (1) | 4.9 (1.2) | 0.01 |
| missing | 46 | 46 | 0 | ||
| WHO ordinal scale at day 7 | mean (sd) | 4.4 (1.9) | 4.3 (1.9) | 5 (1.9) | 0.02 |
| missing | 70 | 69 | 1 | ||
| WHO ordinal scale at day 14 | mean (sd) | 3.1 (2.7) | 3.1 (2.7) | 3.2 (2.7) | 0.91 |
| missing | 144 | 140 | 4 | ||
| C-reactive protein at admission (mg/mL), M (sd) | 11 (8.6) | 10.9 (8.6) | 12.5 (9) | 0.28 | |
| missing | 42 | 38 | 4 | ||
| Procalcitonin at admission (ng/mL), M (sd) | 1.1 (5.8) | 1.1 (6) | 1.4 (3.7) | 0.76 | |
| missing | 169 | 160 | 9 | ||
| Neutrophil count at admission (103/mm3), M (sd) | 36.9 (440.8) | 39.8 (461.6) | 6.7 (3.6) | 0.66 | |
| missing | 49 | 44 | 5 | ||
| Lymphocyte count at admission (103/mm3), M (sd) | 9.9 (101.7) | 10.6 (106.5) | 1.7 (5.2) | 0.6 | |
| missing | 47 | 42 | 5 | ||
| C-reactive protein at day 7 (mg/mL), M (sd) | 5 (6.3) | 5 (6.2) | 5.5 (7.6) | 0.69 | |
| missing | 211 | 196 | 15 | ||
| Neutrophil count at day 7 (103/mm3) | 10.4 (52) | 10.6 (54.8) | 7.8 (3.8) | 0.79 | |
| missing | 208 | 192 | 16 | ||
| Lymphocyte count at day 7 (103/mm3), M (sd) | 1.2 (1.6) | 1.3 (1.7) | 1.1 (0.5) | 0.52 | |
| missing | 208 | 192 | 16 | ||
| Variable | HR | 95% CI | p-Value |
|---|---|---|---|
| 30 days mortality | |||
| Age | 1.09 | [1.06–1.12] | <0.001 |
| CCI | 0.98 | [0.84–1.14] | 0.78 |
| Severe immunosuppression | 5.87 | [0.87–1.03] | 0.01 |
| Days since onset of symptoms | 0.95 | [0.87–1.03] | 0.20 |
| WHO ordinal scale at admission | 1.21 | [1.02–1.43] | 0.04 |
| CRP levels (mg/mL) | 1.02 | [1–1.04] | 0.03 |
| Positive PUA | 0.53 | [0.22–1.28] | 0.16 |
| ICU admission | |||
| CCI | 0.85 | [0.73–0.99] | 0.05 |
| Antibiotic treatment before hospitalization (atb = 1) | 2.2 | [1.12–4.35] | 0.03 |
| Antibiotic treatment before hospitalization (atb = 2) | 3.67 | [1.06–12.75] | 0.05 |
| PCTI levels (ng/mL) | 1.04 | [1.01–1.07] | 0.01 |
| Positive PUA | 0.8 | [0.25–2.54] | 0.70 |
| Variable | Estimate | SE | p-Value |
|---|---|---|---|
| Intercept | −3.64 | 5.26 | 0.49 |
| Antibiotic treatment before hospitalization (atb = 1) | 0.29 | 1.56 | 0.85 |
| Antibiotic treatment before hospitalization (atb = 2) | 7.24 | 4.07 | 0.08 |
| Antibiotic treatment during hospitalization (atb = 1) | −2.13 | 3.57 | 0.55 |
| Antibiotic treatment during hospitalization (atb = 2) | −2.31 | 3.67 | 0.53 |
| Antibiotic treatment during hospitalization (atb = 3) | 19.02 | 6.62 | <0.001 |
| WHO ordinal scale at admission | 3.51 | 0.81 | <0.001 |
| CT scan GGO | 5.64 | 3.23 | 0.08 |
| CT scan FO | 0.45 | 5.48 | 0.93 |
| CT scan GGO and FO | 10.17 | 1.93 | <0.001 |
| CT scan others | 4.11 | 8.49 | 0.63 |
| Chest X-ray GGO | 1.83 | 3.52 | 0.60 |
| Chest X-ray FO | 4.36 | 3.74 | 0.25 |
| Chest X-ray GGO and FO | 2.93 | 3.63 | 0.42 |
| Chest X-ray others | 4.29 | 6.53 | 0.51 |
| CRP at admission (mg/mL) | 0.14 | 0.09 | 0.13 |
| PCTI at admission (ng/mL) | 0.49 | 0.19 | 0.01 |
| Positive PUA | 1.71 | 2.37 | 0.47 |
| Variable | Estimate | SE | p-Value |
|---|---|---|---|
| Intercept | 2.30 | 0.38 | <0.001 |
| Time (day 7 vs. day 0) | −0.10 | 0.12 | 0.41 |
| Time (day 14 vs. day 0) | −1.33 | 0.14 | <0.001 |
| PUA | 0.37 | 0.32 | 0.26 |
| Age | 0.03 | 0.01 | <0.001 |
| Time (day 7 vs. day 0) × PUA | 0.19 | 0.36 | 0.60 |
| Time (day 14 vs. day 0) × PUA | −0.38 | 0.39 | 0.34 |
| Variable | C-Reactive Protein (mg/mL) | Lymphocyte Count (103/mm3) | Neutrophil Count (103/mm3) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| est | SE | p-Value | est | SE | p-Value | est | SE | p-Value | |
| Intercept | 6.33 | 1.49 | <0.001 | 148.12 | 48.39 | <0.001 | 3652 | 10.80 | <0.001 |
| Time (day 7 vs. day 0) | −5.87 | 0.54 | <0.001 | −19.89 | 21.74 | 0.36 | −8.55 | 4.70 | 0.07 |
| PUA | 1.01 | 1.27 | 0.43 | −31.22 | 45.30 | 0.49 | −8.61 | 10.25 | 0.40 |
| Age | 0.07 | 0.02 | <0.001 | −1.64 | 0.68 | 0.02 | −0.39 | 0.15 | 0.01 |
| Time (day 7 vs. day 0) × PUA | −0.59 | 1.52 | 0.70 | 26.36 | 65.15 | 0.69 | 8.16 | 14.46 | 0.57 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valsecchi, P.; Colaneri, M.; Zuccaro, V.; Asperges, E.; Costanzo, F.; Mariani, B.; Roda, S.; Minucci, R.; Bertuccio, F.; Fraolini, E.; et al. Impact of Pneumococcal Urinary Antigen Testing in COVID-19 Patients: Outcomes from the San Matteo COVID-19 Registry (SMACORE). J. Pers. Med. 2021, 11, 762. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080762
Valsecchi P, Colaneri M, Zuccaro V, Asperges E, Costanzo F, Mariani B, Roda S, Minucci R, Bertuccio F, Fraolini E, et al. Impact of Pneumococcal Urinary Antigen Testing in COVID-19 Patients: Outcomes from the San Matteo COVID-19 Registry (SMACORE). Journal of Personalized Medicine. 2021; 11(8):762. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080762
Chicago/Turabian StyleValsecchi, Pietro, Marta Colaneri, Valentina Zuccaro, Erika Asperges, Filippo Costanzo, Bianca Mariani, Silvia Roda, Rita Minucci, Francesco Bertuccio, Elia Fraolini, and et al. 2021. "Impact of Pneumococcal Urinary Antigen Testing in COVID-19 Patients: Outcomes from the San Matteo COVID-19 Registry (SMACORE)" Journal of Personalized Medicine 11, no. 8: 762. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080762