
Accuracy of Patient-Specific Drilling Guides in Acetabular Fracture Surgery: A Human Cadaver Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Specimens
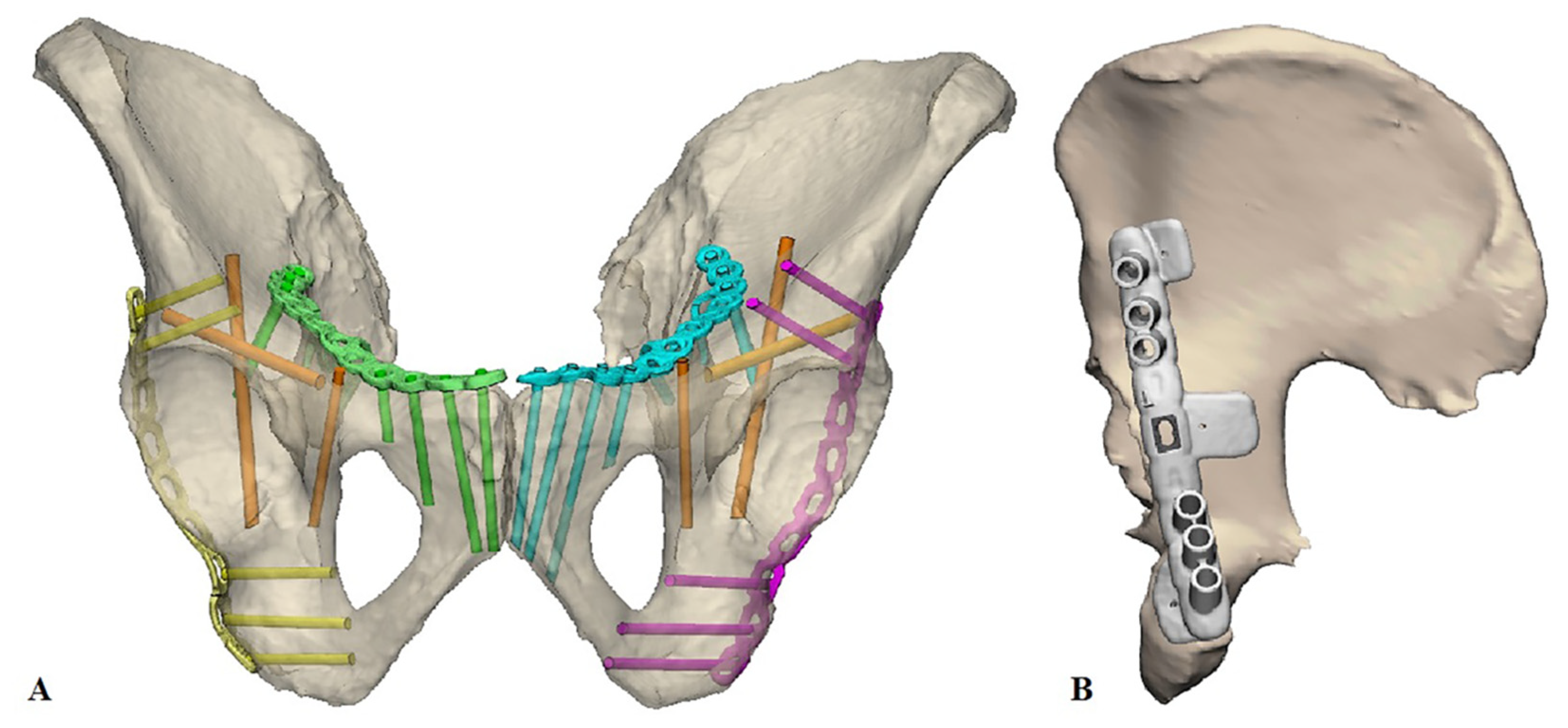
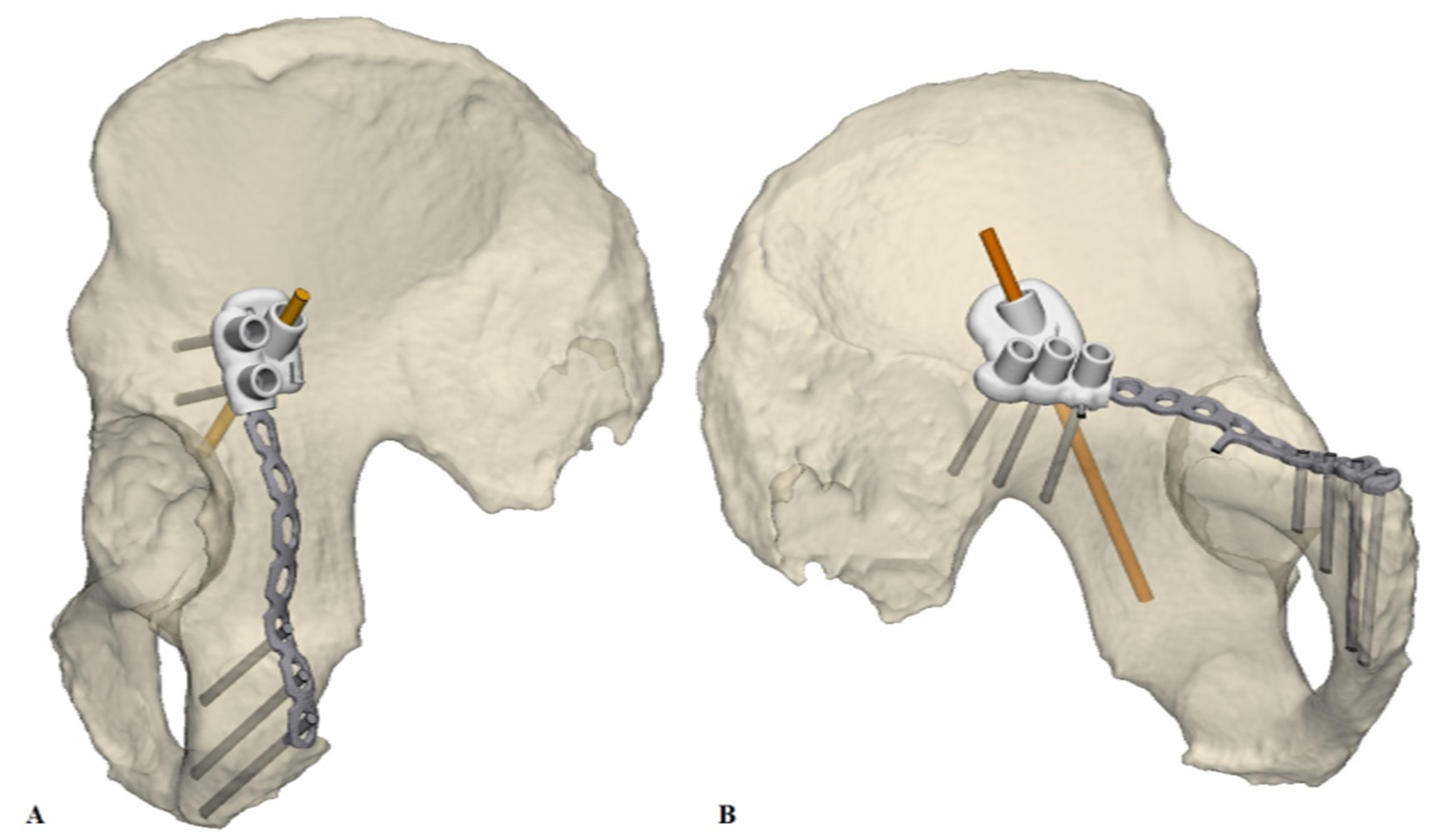
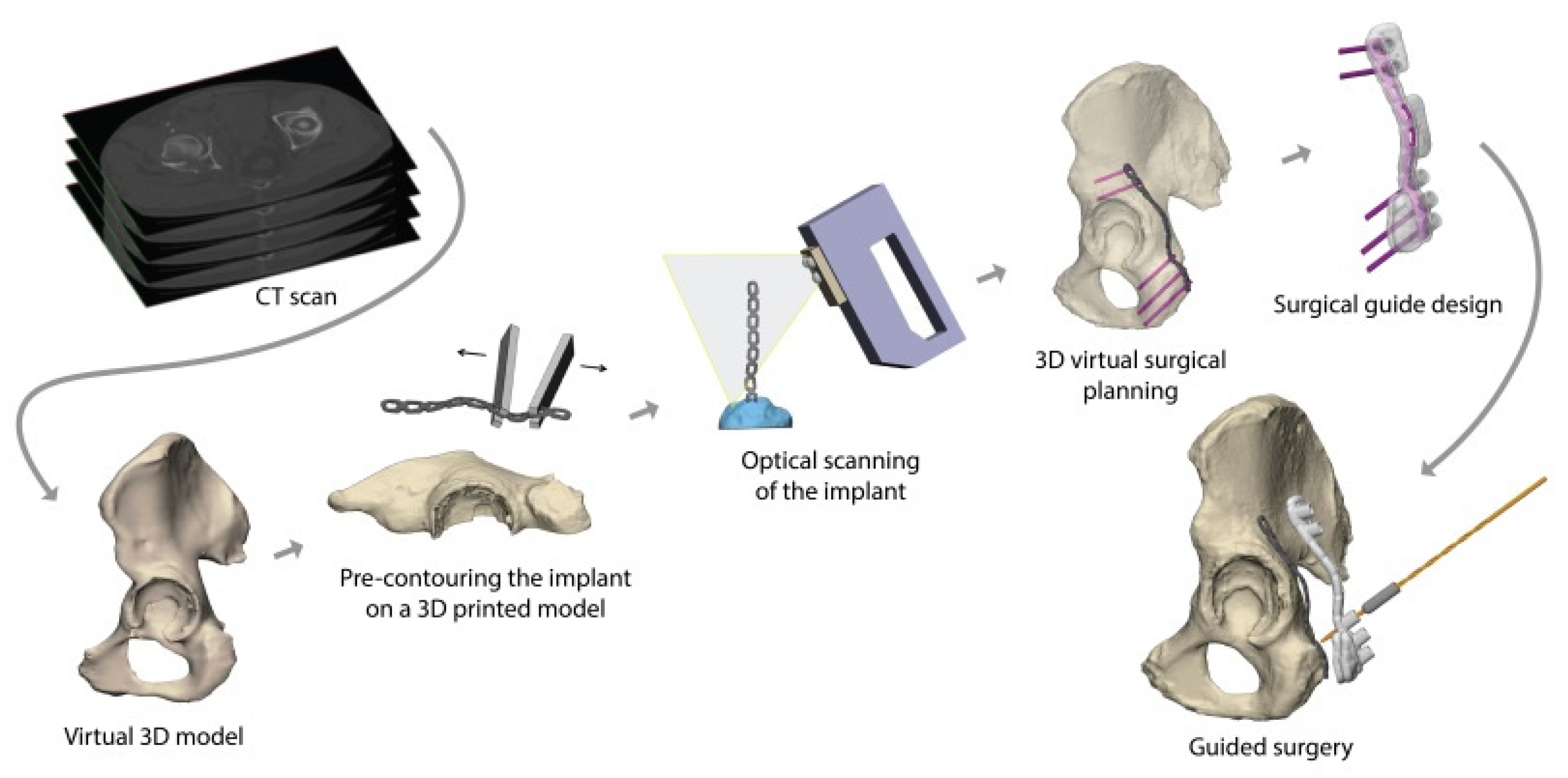
2.2. 3D Surgical Planning
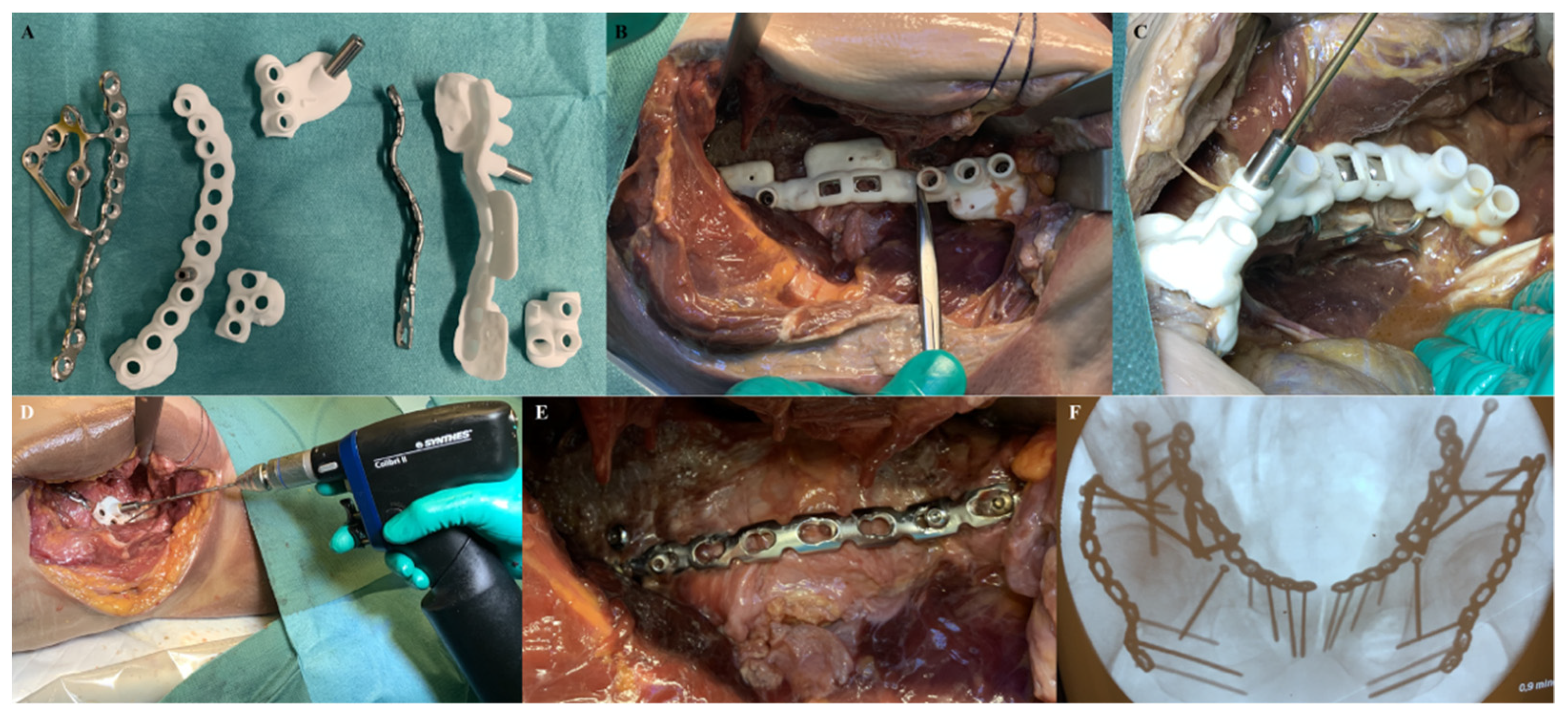
2.3. Surgical Procedure
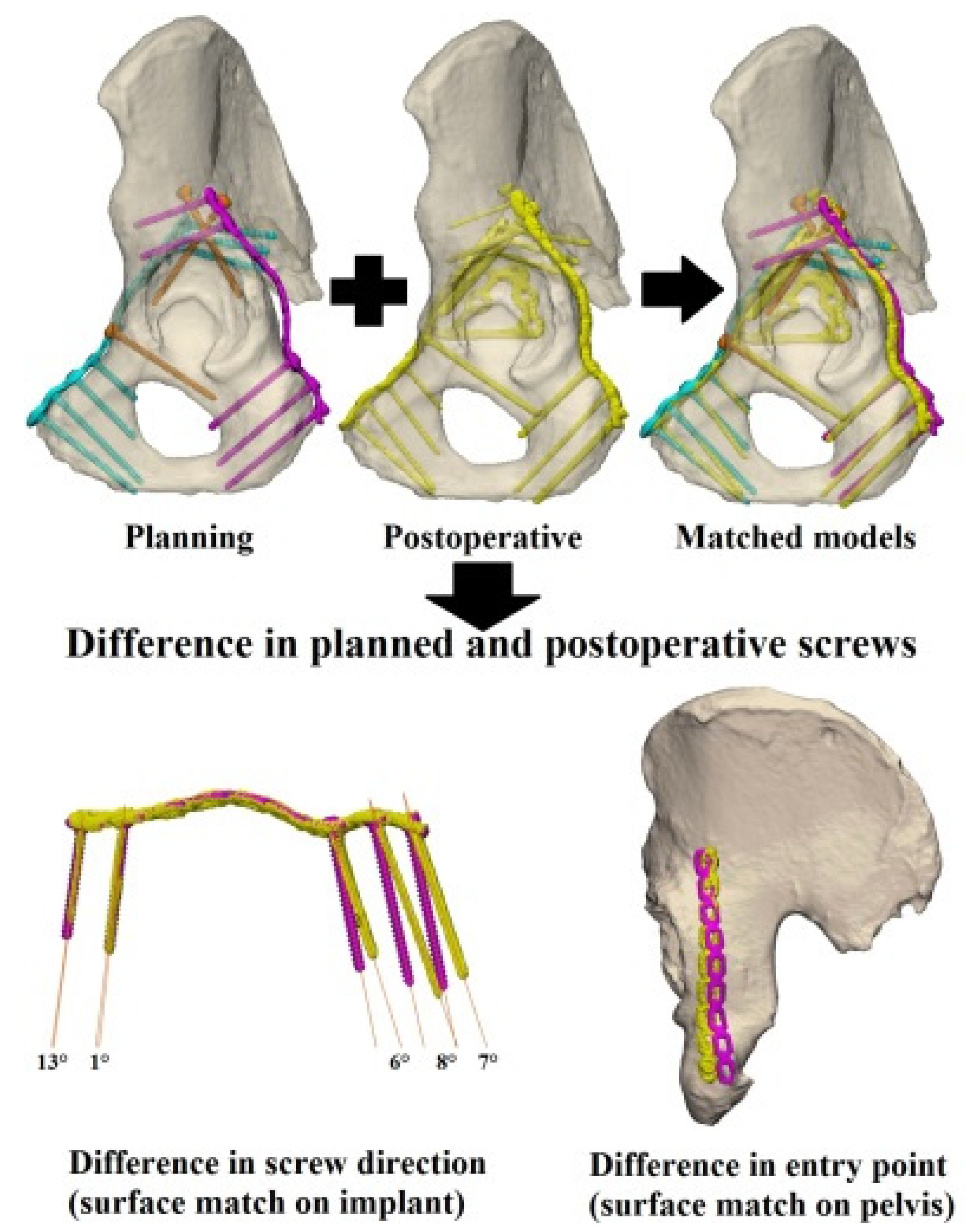
2.4. Postoperative Evaluation–Accuracy of Guided Screw Insertion
3. Results
Postoperative Evaluation—Accuracy of Guided Screw Insertion
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Liu, P.; Wang, G.; Yang, Y.; Dong, J.; Wang, Y.; Zhou, D. Risk Factors of Surgical Site Infection after Acetabular Fracture Surgery. Surg. Infect. 2015, 16, 577–582. [Google Scholar] [CrossRef]
- Yi, C.; Burns, S.; Hak, D.J. Intraoperative fluoroscopic evaluation of screw placement during pelvic and acetabular surgery. J. Orthop. Trauma 2014, 28, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Culemann, U.; Marintschev, I.; Gras, F.; Pohlemann, T. Infra-acetabular corridor-technical tip for an additional screw placement to increase the fixation strength of acetabular fractures. J. Trauma-Inj. Infect. Crit. Care 2011, 70, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Marintschev, I.; Gras, F.; Schwarz, C.E.; Pohlemann, T.; Hofmann, G.O.; Culemann, U. Biomechanical comparison of different acetabular plate systems and constructs—The role of an infra-acetabular screw placement and use of locking plates. Injury 2012, 43, 470–474. [Google Scholar] [CrossRef]
- Gras, F.; Marintschev, I.; Schwarz, C.E.; Hofmann, G.O.; Pohlemann, T.; Culemann, U. Screw-versus plate-fixation strength of acetabular anterior column fractures: A biomechanical study. J. Trauma Acute Care Surg. 2012, 72, 1664–1670. [Google Scholar] [CrossRef]
- Arlt, S.; Hofmann, G.O.; Mendel, T.; Noser, H.; Wienke, A.; Radetzki, F. Secure corridor for infraacetabular screws in acetabular fracture fixation-a 3-D radiomorphometric analysis of 124 pelvic CT datasets. J. Orthop. Surg. Res. 2018, 13, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochs, B.G.; Stuby, F.M.; Stoeckle, U.; Gonser, C.E. Virtual mapping of 260 three-dimensional hemipelvises to analyse gender-specific differences in minimally invasive retrograde lag screw placement in the posterior acetabular column using the anterior pelvic and midsagittal plane as reference. BMC Musculoskelet. Disord. 2015, 16, 240. [Google Scholar] [CrossRef] [Green Version]
- Caviglia, H.; Mejai, A.; Landro, M.E.; Vatani, N. Percutaneous fixation of acetabular fractures. EFORT Open Rev. 2018, 3, 326–334. [Google Scholar] [CrossRef]
- Peng, Y.; Zhang, L.; Min, W.; Tang, P. Comparison of anterograde versus retrograde percutaneous screw fixation of anterior column acetabular fractures. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 635–639. [Google Scholar] [CrossRef]
- Bastian, J.D.; Näf, D.R.; Cullmann, J.L.; Keel, M.J.; Giannoudis, P.V. Does increased acetabular depth affect safe infra-acetabular screw placement in acetabular fracture fixation? Eur. J. Trauma Emerg. Surg. 2020. [Google Scholar] [CrossRef]
- San-Millán, M.; Rissech, C.; Turbón, D. Shape variability of the adult human acetabulum and acetabular fossa related to sex and age by geometric morphometrics. Implications for adult age estimation. Forensic Sci. Int. 2017, 272, 50–63. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Cai, H.; Kuong, E.; Chui, E.; Siu, Y.C.; Ji, T.; Drstvenšek, I. Surgical applications of three-dimensional printing in the pelvis and acetabulum: From models and tools to implants. Unfallchirurg 2019, 122, 278–285. [Google Scholar] [CrossRef] [Green Version]
- Brouwers, L.; Pull ter Gunne, A.F.; de Jongh, M.A.C.; van der Heijden, F.H.W.M.; Leenen, L.P.H.; Spanjersberg, W.R.; van Helden, S.H.; Verbeek, D.O.; Bemelman, M.; Lansink, K.W.W. The Value of 3D Printed Models in Understanding Acetabular Fractures. 3D Print. Addit. Manuf. 2018, 5, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Song, W.; Zhang, Y.; Zhang, Q.; Zhou, D.; Zhou, X.; He, Y. Three-dimensional printing model improves morphological understanding in acetabular fracture learning: A multicenter, randomized, controlled study. PLoS ONE 2018, 13, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Lyu, F.; Sugand, K.; Wong, S.; Lin, Y.; Wang, Q. Learning Acetabular Fracture Classification using a Three-Dimensional Interactive Software: A Randomized Controlled Trial. Anat. Sci. Educ. 2018, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Zhang, S.; Luo, Q.; Fang, J.; Lin, C.; Leung, F.; Chen, B. Definition of a safe zone for antegrade lag screw fixation of fracture of posterior column of the acetabulum by 3D technology. Injury 2016, 47, 702–706. [Google Scholar] [CrossRef]
- Maini, L.; Verma, T.; Sharma, A.; Sharma, A.; Mishra, A.; Jha, S. Evaluation of accuracy of virtual surgical planning for patient-specific pre-contoured plate in acetabular fracture fixation. Arch. Orthop. Trauma Surg. 2018, 138, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.; Xing, W.; Wu, Z.; Huang, H.; Huang, W. A combination of three-dimensional printing and computer-assisted virtual surgical procedure for preoperative planning of acetabular fracture reduction. Injury 2016, 47, 2223–2227. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.-L.; Chou, Y.-C.; Li, Y.-T.; Chen, J.-E.; Hung, C.-C.; Wu, C.-C.; Shen, H.-C.; Yeh, T.-T. Pre-operative virtual simulation and three-dimensional printing techniques for the surgical management of acetabular fractures. Int. Orthop. 2018, 43, 1969–1976. [Google Scholar] [CrossRef]
- Li, Y.T.; Hung, C.C.; Chou, Y.C.; Chen, J.E.; Wu, C.C.; Shen, H.C.; Yeh, T. Te Surgical treatment for posterior dislocation of hip combined with acetabular fractures using preoperative virtual simulation and three-dimensional printing model-assisted precontoured plate fixation techniques. Biomed Res. Int. 2019, 2019, 3971571. [Google Scholar] [CrossRef] [Green Version]
- Upex, P.; Jouffroy, P.; Riouallon, G. Application of 3D printing for treating fractures of both columns of the acetabulum: Benefit of pre-contouring plates on the mirrored healthy pelvis. Orthop. Traumatol. Surg. Res. 2017, 103, 331–334. [Google Scholar] [CrossRef]
- Hung, C.C.; Li, Y.T.; Chou, Y.C.; Chen, J.E.; Wu, C.C.; Shen, H.C.; Yeh, T. Te Conventional plate fixation method versus pre-operative virtual simulation and three-dimensional printing-assisted contoured plate fixation method in the treatment of anterior pelvic ring fracture. Int. Orthop. 2019, 43, 425–431. [Google Scholar] [CrossRef] [PubMed]
- IJpma, F.F.A.; Meesters, A.M.L.; Merema, B.B.J.; Duis, K.; De Vries, J.P.M.; Banierink, H.; Wendt, K.W.; Kraeima, J.; Witjes, M.J.H. Feasibility of Imaging-Based 3-Dimensional Models to Design Patient-Specific Osteosynthesis Plates and Drilling Guides. JAMA Netw. Open 2021, 4, 1–13. [Google Scholar] [CrossRef]
- Thiel, W. The preservation of the whole corpse with natural color. Ann. Anat. 1992, 174, 185–195. [Google Scholar] [CrossRef]
- Chen, X.; Chen, X.; Zhang, G.; Lin, H.; Yu, Z.; Wu, C.; Li, X.; Lin, Y.; Huang, W. Accurate fixation of plates and screws for the treatment of acetabular fractures using 3D-printed guiding templates: An experimental study. Injury 2017, 48, 1147–1154. [Google Scholar] [CrossRef]
- Chen, H.; Wang, G.; Li, R.; Sun, Y.; Wang, F.; Zhao, H.; Zhang, P.; Zhang, X. A Novel Navigation Template for Fixation of Acetabular Posterior Column Fractures with Antegrade Lag Screws: Design and Application. Int. Orthop. 2016, 40, 827–834. [Google Scholar] [CrossRef]
- Huang, H.; Hsieh, M.F.; Zhang, G.; Ouyang, H.; Zeng, C.; Yan, B.; Xu, J.; Yang, Y.; Wu, Z.; Huang, W. Improved accuracy of 3D-printed navigational template during complicated tibial plateau fracture surgery. Australas. Phys. Eng. Sci. Med. 2015, 38, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Pijpker, P.; Kraeima, J.; Witjes, M.; Oterdoom, D.; Coppes, M.; Groen, R.; Kuijlen, J. Accuracy assessment of pedicle and lateral mass screw insertion assisted by customized 3D-printed drill guides: A human cadaver study. Oper. Neurosurg. 2019, 16, 94–102. [Google Scholar] [CrossRef]
- Ead, M.S.; Duke, K.K.; Jaremko, J.L.; Westover, L. Investigation of pelvic symmetry using CAD software. Med. Biol. Eng. Comput. 2020, 58, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Meynen, A.; Matthews, H.; Nauwelaers, N.; Claes, P.; Mulier, M.; Scheys, L. Accurate reconstructions of pelvic defects and discontinuities using statistical shape models. Comput. Methods Biomech. Biomed. Engin. 2020, 23, 1026–1033. [Google Scholar] [CrossRef]
- Ead, M.S.; Palizi, M.; Jaremko, J.L.; Westover, L.; Duke, K.K. Development and application of the average pelvic shape in virtual pelvic fracture reconstruction. Int. J. Med. Robot. Comput. Assist. Surg. 2021, 17, 1–16. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Anterior In-Plate Screws | Posterior In-Plate Screws | |||||
|---|---|---|---|---|---|---|
| Case | N | ∆ Entry Point (IQR) | ∆ Direction (IQR) | N | ∆ Entry Point (IQR) | ∆ Direction (IQR) |
| 1 | 16 | 3.6 (3–4) mm | 5.0 (3–7)° | 11 | 7.1 (5–10) mm | 3.3 (3–5)° |
| 2 | 16 | 2.1 (2–3) mm | 6.3 (5–8)° | 10 | 3.6 (3–4) mm | 5.4 (4–8)° |
| 3 | 8 | 2.5 (2–3) mm | 5.0 (4–6)° | 12 | 5.2 (4–6) mm | 6.3 (5–7)° |
| 4 | 14 | 3.0 (2–3) mm | 8.2 (5–9)° | 10 | 3.9 (4–5) mm | 4.5 (4–7)° |
| Median (IQR) | 2.9 (2–4) mm | 6.1 (4–9)° | 4.4 (3–6) mm | 5.2 (3–7)° | ||
| Infra-Acetabular Screws | Anterior Column Screws | Posterior Column Screws | ||||
|---|---|---|---|---|---|---|
| Case | ∆ P | ∆ D | ∆ P | ∆ D | ∆ P | ∆ D |
| 1 | 3.0 mm | 8.4° | N/A | N/A | N/A | N/A |
| 4.0 mm | 6.3° | |||||
| 2 | 1.7 mm | 6.6° | N/A | N/A | N/A | N/A |
| 2.1 mm | 8.9° | |||||
| 3 | N/A | N/A | 3.6 mm | 10.6° | 3.0 mm | 8.9° |
| 1.0 mm | 1.4° | 1.0 mm | 10.2° | |||
| 4 | 3.3 mm | 11.8° | 7.0 mm | 2.4° | 2.2 mm | 6.7° |
| 1.5 mm | 4.1° | 2.1 mm | 5.7° | 12.4 mm | 16.5° | |
| Median (IQR) | 2.6 (2–3) mm | 7.5 (6–9)° | 2.8 (2–4) mm | 4.1 (2–7)° | 2.6 (2–5) mm | 9.6 (8–12)° |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meesters, A.M.L.; Assink, N.; ten Duis, K.; Fennema, E.M.; Kraeima, J.; Witjes, M.J.H.; de Vries, J.-P.P.M.; Stirler, V.M.A.; IJpma, F.F.A. Accuracy of Patient-Specific Drilling Guides in Acetabular Fracture Surgery: A Human Cadaver Study. J. Pers. Med. 2021, 11, 763. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080763
Meesters AML, Assink N, ten Duis K, Fennema EM, Kraeima J, Witjes MJH, de Vries J-PPM, Stirler VMA, IJpma FFA. Accuracy of Patient-Specific Drilling Guides in Acetabular Fracture Surgery: A Human Cadaver Study. Journal of Personalized Medicine. 2021; 11(8):763. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080763
Chicago/Turabian StyleMeesters, Anne M. L., Nick Assink, Kaj ten Duis, Eelco M. Fennema, Joep Kraeima, Max J. H. Witjes, Jean-Paul P. M. de Vries, Vincent M. A. Stirler, and Frank F. A. IJpma. 2021. "Accuracy of Patient-Specific Drilling Guides in Acetabular Fracture Surgery: A Human Cadaver Study" Journal of Personalized Medicine 11, no. 8: 763. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080763