
Development and Assessment of the Validity and Reliability of the Short-Form Life Satisfaction Index (LSI-SF) among the Elderly Population

 , , and
, , and
Abstract
:1. Introduction
1.1. ‘Life Satisfaction’ Measurement in the Elderly
1.2. Research Questions and Purposes
2. Methods
2.1. Study Design and Data Collection
2.2. Measures
2.2.1. Background Characteristics of the Participants
2.2.2. Short-Form Life Satisfaction Index (LSI-SF)
2.2.3. WHO-5 Well-Being Index
2.2.4. Definition of Frailty
2.3. Statistical Analysis
3. Results
3.1. Social–Demographic Status and TLSA-LSI Scores of the Participants
3.2. Reliability
3.3. Validity
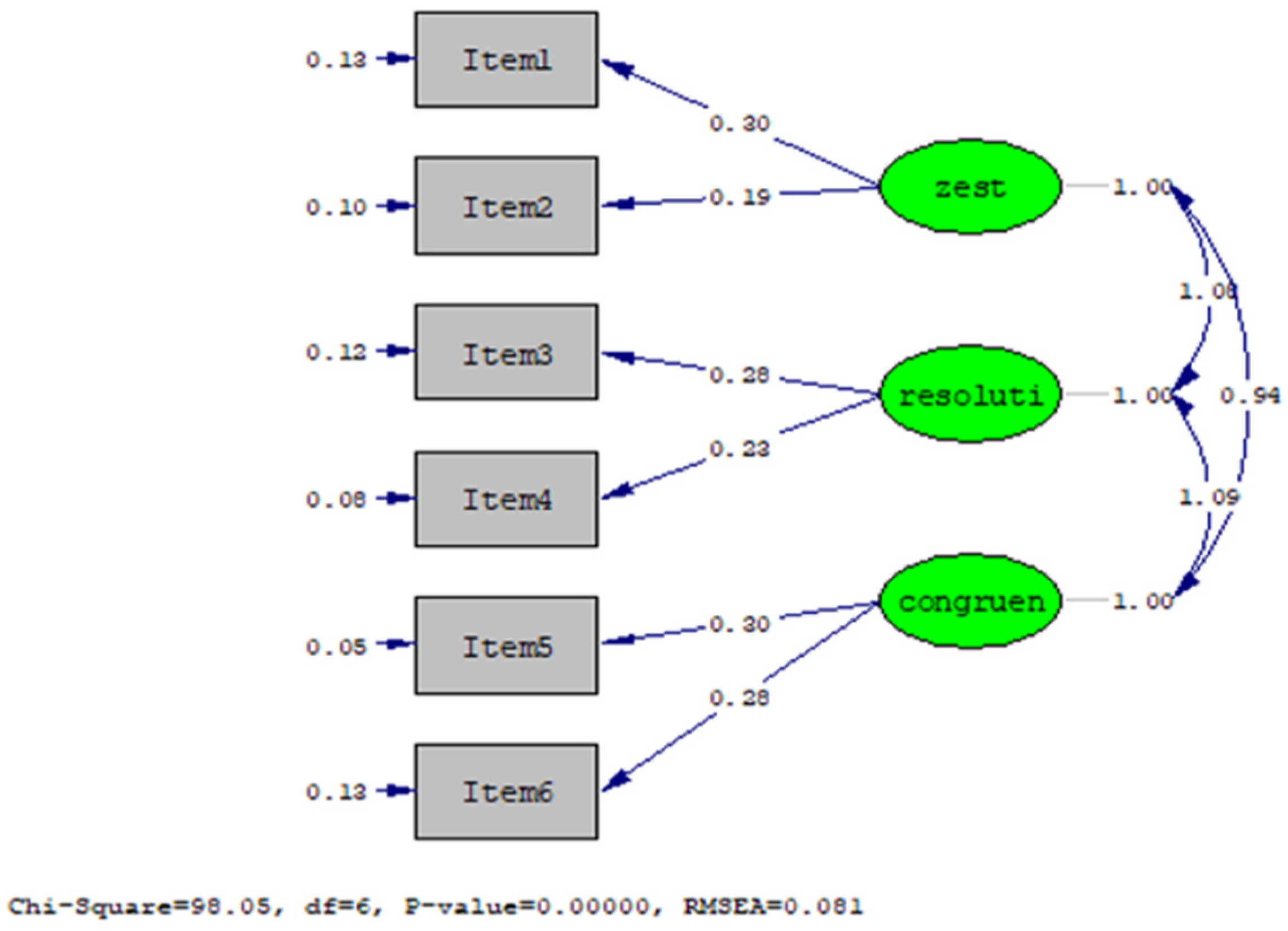
3.3.1. Construct Validity
3.3.2. Criterion-Related Validity
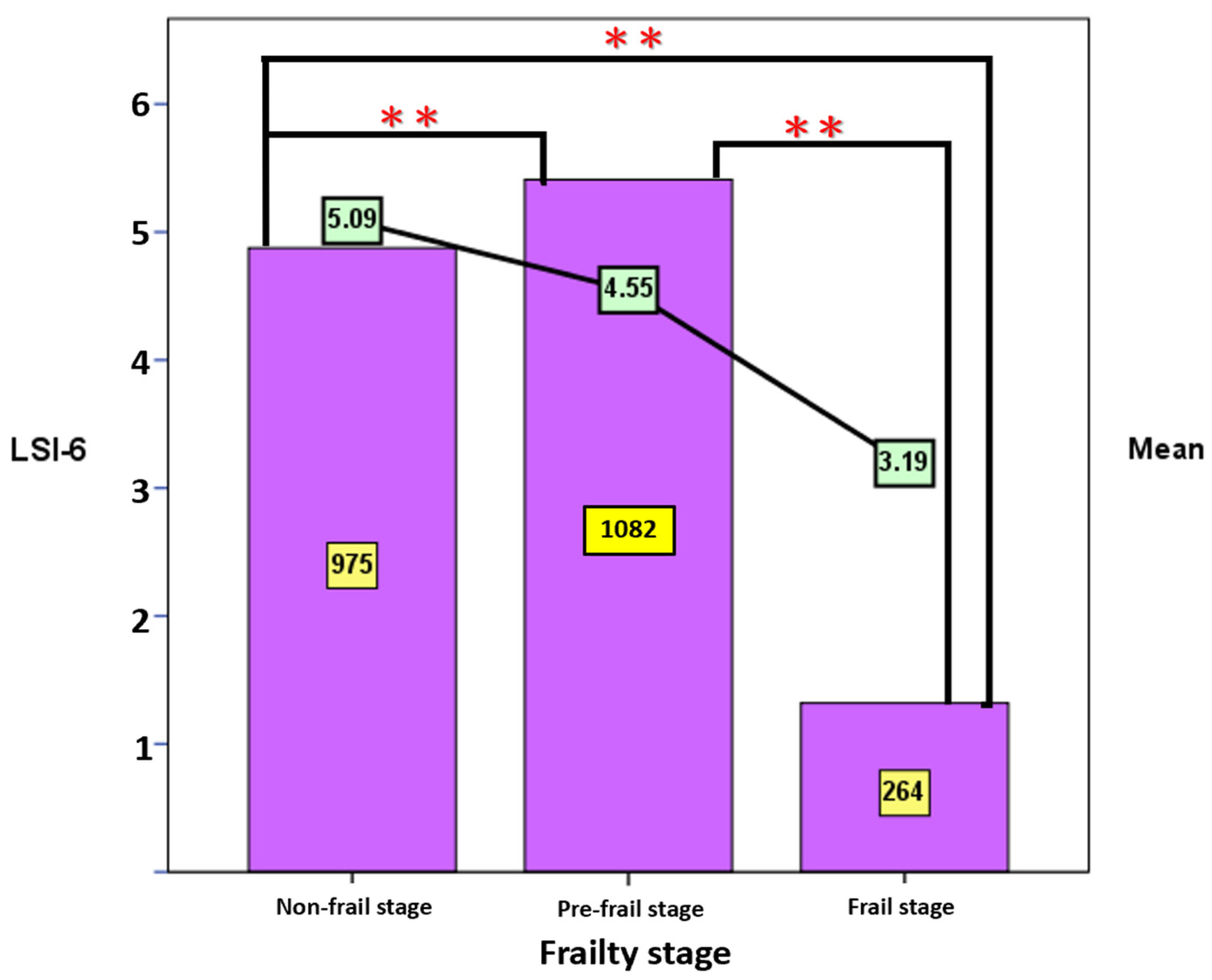
3.3.3. Known-Group Validity
4. Discussion
4.1. Participant Characteristics and LSI-SF
4.2. Reliability of the LSI-SF
4.3. Validity of the Short-Form Life Satisfaction Index
4.3.1. Construct Validity
4.3.2. Criterion-Related Validity
4.3.3. Known-Group Validity
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LSI-SF | Short-Form Life Satisfaction Index |
| CFA | confirmatory factor analysis |
| LS | Life Satisfaction |
| QoL | quality of life |
| LSIA | Life Satisfaction Index-A |
| LSI-11 | Life Satisfaction Index-11 questions |
| LSIZ | Life Satisfaction Index-Z |
| TLSA-LSI | Taiwan Longitudinal Study on Aging-Life Satisfaction Index |
| TLSA | Taiwan Longitudinal Study on Aging |
| KR-20 | Kuder–Richardson 20 value |
| GFI | goodness of fit index |
| AVE | average variance extracted |
| CR | Composite Reliability |
References
- Jakovljevic, M.; Westerman, R.; Sharma, T.; Lamnisos, D. Aging and global health. In Handbook of Global Health; Springer: Belgrade, Serbia, 2020; pp. 1–30. [Google Scholar]
- Haber, D. Health Promotion and Aging: Practical Applications for Health Professionals; Springer Publishing Company: New York, NY, USA, 2019. [Google Scholar]
- Kutubaeva, R.Z. Analysis of life satisfaction of the elderly population on the example of Sweden, Austria and Germany. Popul. Econ. 2019, 3, 102–116. [Google Scholar] [CrossRef] [Green Version]
- Prasoon, R.; Chaturvedi, K.R. Life satisfaction: A literature review. Int. J. Manag. Hum. Soc. Sci. 2016, 1, 25–32. [Google Scholar]
- Neugarten, B.L.; Havighurst, R.J.; Tobin, S.S. The measurement of life satisfaction. J. Gerontol. 1961, 16, 134–143. [Google Scholar] [CrossRef]
- Theofilou, P. Quality of life: Definition and measurement. Eur. J. Psychol. 2013, 9, 150–162. [Google Scholar] [CrossRef]
- Papi, S.; Cheraghi, M. Multiple factors associated with life satisfaction in older adults. Menopause Rev. Przegląd Menopauzalny 2021, 20, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Young, D.; Wei, H.; Zhang, Y.; Zheng, Y.; Xiao, S.; Wang, X.; Chen, X. The relationship between objective life status and subjective life satisfaction with quality of life. Behav. Med. 1998, 23, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Rondón García, L.M.; Ramírez Navarrro, J.M. The impact of quality of life on the health of older people from a multidimensional perspective. J. Aging Res. 2018, 2018, 4086294. [Google Scholar] [CrossRef] [Green Version]
- Boggatz, T. Quality of life in old age—A concept analysis. Int. J. Older People Nurs. 2016, 11, 55–69. [Google Scholar] [CrossRef]
- Meléndez, J.C.; Tomás, J.M.; Oliver, A.; Navarro, E. Psychological and physical dimensions explaining life satisfaction among the elderly: A structural model examination. Arch. Gerontol. Geriatr. 2009, 48, 291–295. [Google Scholar] [CrossRef]
- Lim, H.J.; Min, D.K.; Thorpe, L.; Lee, C.H. Multidimensional construct of life satisfaction in older adults in Korea: A six-year follow-up study. BMC Geriatr. 2016, 16, 197. [Google Scholar] [CrossRef] [Green Version]
- Michalos, A.C. Encyclopedia of Quality of Life and Well-Being Research; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar]
- Vinsalia, T.; Handajani, Y.S. Life satisfaction is the most significant determinant of quality of life in the elderly. Universa Med. 2021, 40, 14–21. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Baji, P.; Farkas, M.; Dobos, Á.; Zrubka, Z.; Gulácsi, L.; Brodszky, V.; Rencz, F.; Péntek, M. Capability of well-being: Validation of the Hungarian version of the ICECAP-A and ICECAP-O questionnaires and population normative data. Qual. Life Res. 2020, 29, 2863–2874. [Google Scholar] [CrossRef] [PubMed]
- Larson, R. Thirty years of research on the subjective well-being of older Americans. J. Gerontol. 1978, 33, 109–125. [Google Scholar] [CrossRef]
- Hoyt, D.R.; Creech, J.C. The Life Satisfaction Index: A methodological and theoretical critique. J. Gerontol. 1983, 38, 111–116. [Google Scholar] [CrossRef]
- Adams, D.L. Analysis of a life satisfaction index. J. Gerontol. 1969, 24, 470–474. [Google Scholar] [CrossRef]
- Lohmann, N. A factor analysis of life satisfaction, adjustment and morale measures with elderly adults. Int. J. Aging Hum. Dev. 1980, 11, 35–43. [Google Scholar] [CrossRef]
- Tai, C.J.; Tseng, T.G.; Hsiao, Y.H.; Kuo, T.A.; Huang, C.Y.; Yang, Y.H.; Lee, M.C. Effects of hearing impairment and hearing aid use on the incidence of cognitive impairment among community-dwelling older adults: Evidence from the Taiwan Longitudinal Study on Aging (TLSA). BMC Geriatr. 2021, 21, 76. [Google Scholar] [CrossRef]
- Liang, J. Dimensions of the Life Satisfaction Index A: A structural formulation. J. Gerontol. 1984, 39, 613–622. [Google Scholar] [CrossRef]
- Rawat, P.S. Patriarchal beliefs, women’s empowerment, and general well-being. Vikalpa 2014, 39, 43–56. [Google Scholar] [CrossRef]
- Voros, V.; Martin Gutierrez, D.; Alvarez, F.; Boda-Jorg, A.; Kovacs, A.; Tenyi, T.; Fekete, S.; Osvath, P. The impact of depressive mood and cognitive impairment on quality of life of the elderly. Psychogeriatrics 2020, 20, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Bureau of Health Promotion Department of Health Taiwan. Survey of the Elderly in Taiwan 1989. 2021. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=240&pid=1281 (accessed on 1 March 2022).
- Chen, M.F.; Tsai, C.C. The Effectiveness of a Thanks, Sorry, Love, and Farewell Board Game in Older People in Taiwan: A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2022, 19, 3146. [Google Scholar] [CrossRef] [PubMed]
- Lobello, S.G.; Underhill, A.T.; Fine, P.R. The reliability and validity of the Life Satisfaction Index-A with survivors of traumatic brain injury. Brain Inj. 2004, 18, 1127–1134. [Google Scholar] [CrossRef]
- World Health Organization. WHO-Five Well-Being Index—Background Information 1998. Available online: http://www.who-5.org/ (accessed on 1 March 2022).
- Hall, T.; Krahn, G.L.; Horner-Johnson, W.; Lamb, G. Examining functional content in widely used Health-Related Quality of Life scales. Rehabil Psychol. 2011, 56, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Romero-Ortuno, R.; Walsh, C.D.; Lawlor, B.A.; Kenny, R.A. A frailty instrument for primary care: Findings from the Survey of Health, Ageing and Retirement in Europe (SHARE). BMC Geriatr. 2010, 10, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos-Eggimann, B.; Cuénoud, P.; Spagnoli, J.; Junod, J. Prevalence of frailty in middle-aged and older community-dwelling Europeans living in 10 countries. J. Gerontol. Ser. A 2009, 64, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.Y.; Wu, S.C.; Chen, L.J.; Lue, B.H. The prevalence of subjective frailty and factors associated with frailty in Taiwan. Arch. Gerontol. Geriatr. 2010, 50, 43–47. [Google Scholar] [CrossRef]
- Lee, W.J.; Chen, L.K.; Peng, L.N.; Chiou, S.T.; Chou, P. Personal mastery attenuates the adverse effect of frailty on declines in physical function of older people: A 6-year population-based cohort study. Medicine 2016, 95, e4661. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, 146–157. [Google Scholar] [CrossRef]
- Chu, W.M.; Ho, H.E.; Yeh, C.J.; Hsiao, Y.H.; Hsu, P.S.; Lee, S.H.; Lee, M.C. Self-rated health trajectory and frailty among community-dwelling older adults: Evidence from the Taiwan Longitudinal Study on Aging (TLSA). BMJ Open 2021, 11, e049795. [Google Scholar] [CrossRef]
- Chu, W.M.; Ho, H.E.; Yeh, C.J.; Tsan, Y.T.; Lee, S.H.; Lee, M.C. Late-career unemployment and risk of frailty among older adults in Taiwan: An 8-year population-based cohort study. Geriatr. Gerontol. Int. 2021, 21, 353–358. [Google Scholar] [CrossRef]
- An, H.Y.; Chen, W.; Wang, C.W.; Yang, H.F.; Huang, W.T.; Fan, S.Y. The Relationships between Physical Activity and Life Satisfaction and Happiness among Young, Middle-Aged, and Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 4817. [Google Scholar] [CrossRef] [PubMed]
- Elmståhl, S.; Berglund, J.S.; Fagerström, C.; Ekström, H. The life satisfaction index-a (LSI-A): Normative data for a general swedish population aged 60 to 93 years. Clin. Interv. Aging 2020, 15, 2031. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.J.; Min, D.K.; Thorpe, L.; Lee, C.H. Trajectories of Life Satisfaction and their Predictors among Korean Older Adults. BMC Geriatr. 2017, 17, 89. [Google Scholar] [CrossRef] [Green Version]
- Rodgers, V.; Neville, S.; La Grow, S. Health, functional ability and life satisfaction among older people 65 years and over: A cross-sectional study. Contemp. Nurse 2017, 53, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Tavares, A.I. Health and life satisfaction factors of Portuguese older adults. Arch. Gerontol. Geriatr. 2021, 99, 104600. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Braun, K.L.; Wu, Y.Y. The educational, racial and gender crossovers in life satisfaction: Findings from the longitudinal Health and Retirement Study. Arch. Gerontol. Geriatr. 2017, 73, 60–68. [Google Scholar] [CrossRef] [Green Version]
- Pan, Y.; Chan, S.H.; Xu, Y.; Yeung, K.C. Determinants of life satisfaction and self-perception of ageing among elderly people in China: An exploratory study in comparison between physical and social functioning. Arch. Gerontol. Geriatr. 2019, 84, 103910. [Google Scholar] [CrossRef]
- Friedman, S.M.; Mulhausen, P.; Cleveland, M.L.; Coll, P.P.; Daniel, K.M.; Hayward, A.D.; Shah, K.; Skudlarska, A.B.; White, H.K. Healthy aging: American Geriatrics Society white paper executive summary. J. Am. Geriatr. Soc. 2019, 67, 17–20. [Google Scholar] [CrossRef] [Green Version]
- Adisa, T.A.; Abdulraheem, I.; Isiaka, S.B. Patriarchal hegemony: Investigating the impact of patriarchy on women’s work-life balance. Gend. Manag. Int. J. 2019, 34, 19–33. [Google Scholar] [CrossRef] [Green Version]
- Bratt, A.S.; Stenström, U.; Rennemark, M. Effects on life satisfaction of older adults after child and spouse bereavement. Aging Ment. Health 2017, 21, 602–608. [Google Scholar] [CrossRef]
- Qin, W.; Xu, L.; Sun, L.; Li, J.; Ding, G.; Wang, Q.; Zhang, J.; Shao, H. Association between frailty and life satisfaction among older people in Shandong, China: The differences in age and general self-efficacy. Psychogeriatrics 2020, 20, 172–179. [Google Scholar] [CrossRef]
- Enkvist, Å.; Ekström, H.; Elmståhl, S. Associations between functional ability and life satisfaction in the oldest old: Results from the longitudinal population study Good Aging in Skåne. Clin. Interv. Aging 2012, 7, 313. [Google Scholar] [CrossRef] [Green Version]
- Wylie, M.L. Life satisfaction as a program impact criterion. J. Gerontol. 1970, 25, 36–40. [Google Scholar] [CrossRef]
- Abraham, I.L. Longitudinal reliability of the life satisfaction index (short form) with nursing home residents: A cautionary note. Perceptual and motor skills 1992, 75, 665–666. [Google Scholar] [CrossRef]
- McDowell, I. Measures of self-perceived well-being. J. Psychosom. Res. 2010, 69, 69–79. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Structural Equation Models with Unobservable Variables and Measurement Error: Algebra and Statistics. J. Mark. Res. 1981, 18, 382–388. [Google Scholar]
- Şahin, D.S.; Özer, Ö.; Yanardağ, M.Z. Perceived social support, quality of life and satisfaction with life in elderly people. Educ. Gerontol. 2019, 45, 69–77. [Google Scholar] [CrossRef]
- St John, P.D.; Tyas, S.L.; Montgomery, P.R. Montgomery, Life satisfaction and frailty in community-based older adults: Cross-sectional and prospective analyses. Int. Psychogeriatr. 2013, 25, 1709–1716. [Google Scholar] [CrossRef]
- Wilhelmson, K.; Fritzell, E.; Eklund, K.; Dahlin-Ivanoff, S. Life satisfaction and frailty among older adults. Health Psychol. Res. 2013, 1, e32. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Dimension | Item |
|---|---|
| Zest vs. Apathy | 1. These are the best years of my life. |
| 2. Most of the things I do are boring or monotonous. | |
| Resolution and Fortitude | 3. As I grow older, things seem better than I thought they would be. |
| 4. The things I do are as interesting to me as they ever were. | |
| Congruence Between Desired and Achieved Goals | 5. As I look back on my life, I am fairly well satisfied. |
| 6. I’ve gotten pretty much what I expected out of life. |
| Total | LSI-SF | ||||
|---|---|---|---|---|---|
| N | % | Mean | SD | F/t | |
| Age | 2.93 ** | ||||
| 60–64 | 528 | 22.70 | 4.77 | 1.65 | |
| 65–69 | 592 | 25.50 | 4.76 | 1.67 | |
| 70–74 | 393 | 16.90 | 4.63 | 1.71 | |
| 75–79 | 326 | 14.00 | 4.36 | 2.06 | |
| 80–84 | 217 | 9.30 | 4.46 | 1.85 | |
| ≥85 | 265 | 11.40 | 4.46 | 1.82 | |
| Gender | 1.29 ** | ||||
| male | 1154 | 49.70 | 4.67 | 1.72 | |
| female | 1167 | 50.30 | 4.57 | 1.82 | |
| Education | 11.11 ** | ||||
| primary school | 1493 | 64.30 | 4.48 | 1.86 | |
| middle school | 264 | 11.40 | 4.64 | 1.73 | |
| high school | 420 | 18.10 | 4.97 | 1.47 | |
| university | 144 | 6.20 | 5.02 | 1.50 | |
| Spousal status | 8.28 ** | ||||
| with a spouse | 1660 | 71.50 | 4.81 | 1.64 | |
| without a spouse | 661 | 28.50 | 4.15 | 1.98 | |
| Frailty status | 134.89 ** | ||||
| non-frailty stage | 975 | 42.00 | 5.09 | 1.39 | |
| pre-frailty stage | 1082 | 46.60 | 4.55 | 1.77 | |
| frailty stage | 264 | 11.40 | 3.19 | 2.18 | |
| Maximum Likelihood with Correlated Factors | Outcome | Criterion | |
|---|---|---|---|
| Absolute Fit Measures | χ2 | 98.58 | smaller is better |
| RMSEA | 0.08 | <0.10 | |
| GFI | 0.99 | >0.90 | |
| AGFI | 0.95 | >0.90 | |
| Incremental Fit Measures | NFI | 0.98 | >0.90 |
| CFI | 0.98 | >0.90 | |
| Parsimonious Fit Measures | CN | 396.67 | ≥200 |
| One-Order CFA Factor | Unstandardized Estimate | S.E. | t/p | Standardized Estimate | Factor Loadings | R2 | AVE | CR |
|---|---|---|---|---|---|---|---|---|
| 1. Zest | 0.43 | 0.601 | ||||||
| Item 1 | 0.30 | 0.01 | 26.16 ** | 0.63 | 0.71 | 0.40 | ||
| Item 2 | 0.19 | 0.01 | 22.16 ** | 0.51 | 0.60 | 0.26 | ||
| 2. Resolution | 0.54 | 0.701 | ||||||
| Item 3 | 0.28 | 0.01 | 29.24 ** | 0.62 | 0.72 | 0.39 | ||
| Item 4 | 0.23 | 0.01 | 29.77 ** | 0.63 | 0.75 | 0.40 | ||
| 3. Congruence | 0.58 | 0.733 | ||||||
| Item 5 | 0.30 | 0.01 | 39.52 ** | 0.80 | 0.82 | 0.64 | ||
| Item 6 | 0.28 | 0.01 | 29.92 ** | 0.61 | 0.70 | 0.38 | ||
| criteria | >0.60 | >0.20 | >0.50 | >0.50 |
| Dimension | Zest vs. Apathy | Resolution and Fortitude |
|---|---|---|
| Resolution and Fortitude | 1.08 (33.25 *) [1.02, 1.78] | |
| Congruence Between Desired and Achieved Goals | 0.94 (33.77 *) [0.88, 0.99] | 1.09 (48.95 *) [1.05, 1.13] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, P.-S.; Hsieh, C.-J.; Tallutondok, E.B.; Shih, Y.-L.; Liu, C.-Y. Development and Assessment of the Validity and Reliability of the Short-Form Life Satisfaction Index (LSI-SF) among the Elderly Population. J. Pers. Med. 2022, 12, 709. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050709
Li P-S, Hsieh C-J, Tallutondok EB, Shih Y-L, Liu C-Y. Development and Assessment of the Validity and Reliability of the Short-Form Life Satisfaction Index (LSI-SF) among the Elderly Population. Journal of Personalized Medicine. 2022; 12(5):709. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050709
Chicago/Turabian StyleLi, Pei-Shan, Chia-Jung Hsieh, Eva Berthy Tallutondok, Ya-Ling Shih, and Chieh-Yu Liu. 2022. "Development and Assessment of the Validity and Reliability of the Short-Form Life Satisfaction Index (LSI-SF) among the Elderly Population" Journal of Personalized Medicine 12, no. 5: 709. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050709