
BMI at Discharge from Treatment Predicts Relapse in Anorexia Nervosa: A Systematic Scoping Review

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction and Synthesis
2.5. Risk of Bias in Individual Studies
3. Results
3.1. Study Search and Selection
3.2. Characteristics and Quality of the Included Studies
3.2.1. Study Design
3.2.2. Sample Size and Considerations for Statistical Analyses
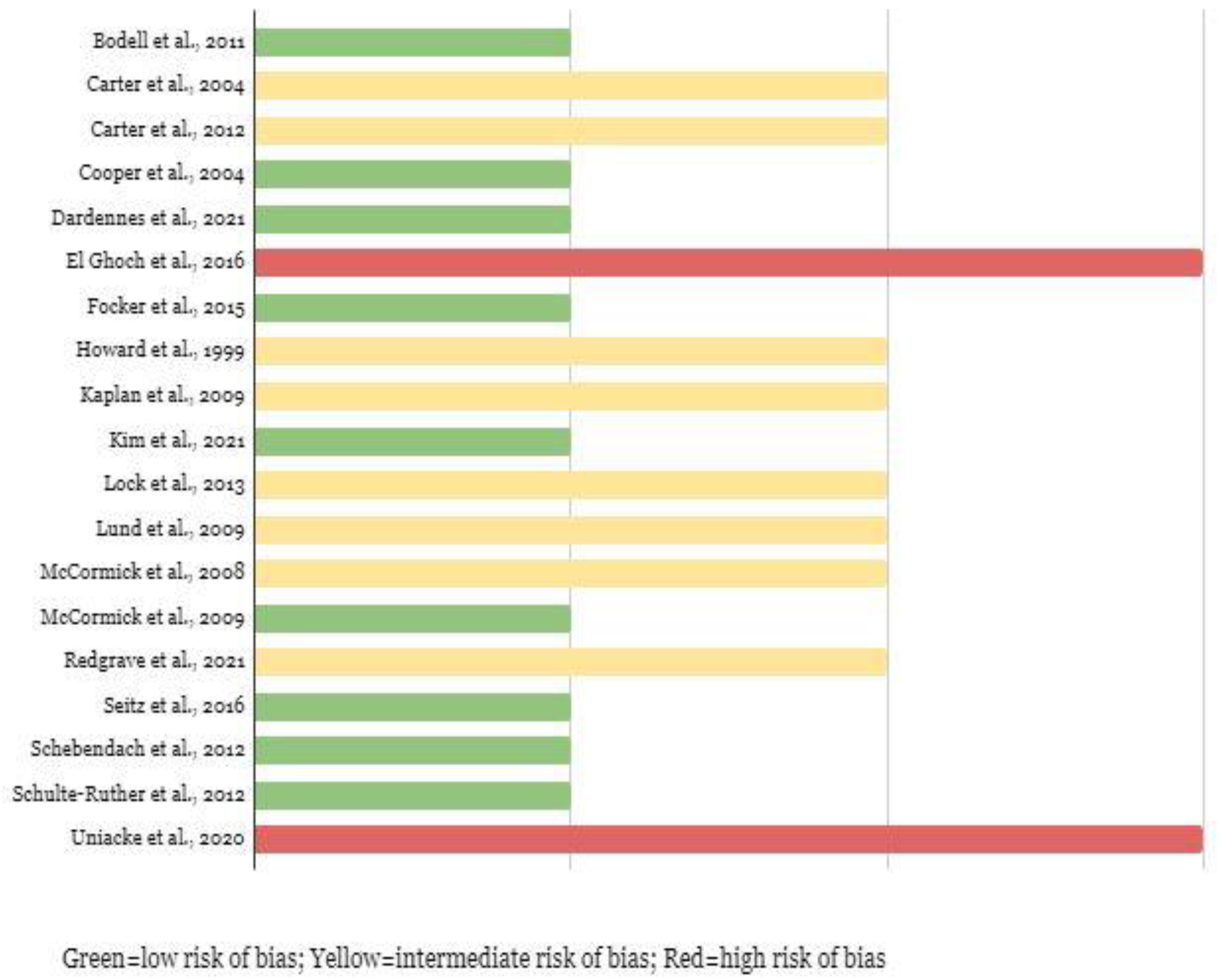
3.2.3. Bias Assessment
3.2.4. Review Question 1: What Is the Time to Relapse?
3.2.5. Review Question 2: Which Are the Predictors of Relapse?
Biological Predictors
Psychological Predictors
ED-Related Predictors
Study Design
3.2.6. Summary of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AN | Anorexia nervosa |
| BMI | Body mass index |
| ED | Eating disorder |
| EDE | Eating Disorder Evaluation |
| HC | Healthy control |
| M ± SD | Mean ± Standard Deviation |
| Mo | months |
| NRCT | Non-randomized control trial |
| n.s. | non-significant |
| PICO | Population, intervention, comparison, outcome |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines |
| PROSPERO | International Prospective Register of Systematic Reviews |
| ROBINS-I | Risk of Bias in Non-randomized Studies–of Interventions |
| QUIPS | Quality in Prognosis Study tool |
| SE-AN | Severe and enduring anorexia nervosa |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Lock, J. Updates on Treatments for Adolescent Anorexia Nervosa. Child Adolesc. Psychiatr. Clin. N. Am. 2019, 28, 523–535. [Google Scholar] [CrossRef] [PubMed]
- Dalle Grave, R.; Sartirana, M.; Sermattei, S.; Calugi, S. Treatment of Eating Disorders in Adults Versus Adolescents: Similarities and Differences. Clin. Ther. 2020, 43, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Eating Disorders: Recognition and treatment. National Institute for Health and Care Excellence, London. 2017. Available online: https://www.nice.org.uk/guidance/ng69 (accessed on 18 May 2020).
- Mitchell, J.E.; Peterson, C.B. Anorexia Nervosa. N. Engl. J. Med. 2020, 382, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Lock, J. Family therapy for eating disorders in youth: Current confusions, advances, and new directions. Curr. Opin. Psychiatry 2018, 31, 431–435. [Google Scholar] [CrossRef]
- Dalle Grave, R.; Calugi, S.; Doll, H.A.; Fairburn, C.G. Enhanced cognitive behaviour therapy for adolescents with anorexia nervosa: An alternative to family therapy? Behav. Res. 2013, 51, R9–R12. [Google Scholar] [CrossRef] [Green Version]
- Linardon, J.; Fairburn, C.G.; Fitzsimmons-Craft, E.E.; Wilfley, D.E.; Brennan, L. The empirical status of the third-wave behaviour therapies for the treatment of eating disorders: A systematic review. Clin. Psychol. Rev. 2017, 58, 125–140. [Google Scholar] [CrossRef]
- Wonderlich, S.A.; Bulik, C.M.; Schmidt, U.; Steiger, H.; Hoek, H.W. Severe and enduring anorexia nervosa: Update and observations about the current clinical reality. Int. J. Eat. Disord. 2020, 53, 1303–1312. [Google Scholar] [CrossRef]
- Khalsa, S.S.; Portnoff, L.C.; McCurdy-McKinnon, D.; Feusner, J.D. What happens after treatment? A systematic review of relapse, remission, and recovery in anorexia nervosa. J. Eat. Disord. 2017, 5, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Couturier, J.; Lock, J. What is recovery in adolescent anorexia nervosa? Int. J. Eat Disord. 2006, 39, 550–555. [Google Scholar] [CrossRef]
- Carter, J.C.; Mercer-Lynn, K.B.; Norwood, S.J.; Bewell-Weiss, C.V.; Crosby, R.D.; Woodside, D.B.; Olmsted, M.P. A prospective study of predictors of relapse in anorexia nervosa: Implications for relapse prevention. Psychiatry Res. 2012, 200, 518–523. [Google Scholar] [CrossRef]
- Keel, P.K.; Dorer, D.J.; Franko, D.L.; Jackson, S.C.; Herzog, D.B. Postremission Predictors of Relapse in Women with Eating Disorders. Am. J. Psychiatry 2005, 162, 2263–2268. [Google Scholar] [CrossRef] [PubMed]
- Walsh, B.T.; Kaplan, A.S.; Attia, E.; Olmsted, M.; Parides, M.; Carter, J.C.; Pike, K.M.; Devlin, M.J.; Woodside, B.; Roberto, C.A.; et al. Fluoxetine after weight restoration in anorexia nervosa: A randomized controlled trial. JAMA 2006, 295, 2605–2612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pike, K.M.; Walsh, B.T.; Vitousek, K.; Wilson, G.T.; Bauer, J. Cognitive Behavior Therapy in the Posthospitalization Treatment of Anorexia Nervosa. Am. J. Psychiatry 2003, 160, 2046–2049. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.C.; Blackmore, E.; Sutandar-Pinnock, K.; Woodside, D.B. Relapse in anorexia nervosa: A survival analysis. Psychol. Med. 2004, 34, 671–679. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Engelhardt, C.; Föcker, M.; Bühren, K.; Dahmen, B.; Becker, K.; Weber, L.; Correll, C.U.; Egberts, K.M.; Ehrlich, S.; Roessner, V.; et al. Age dependency of body mass index distribution in childhood and adolescent inpatients with anorexia nervosa with a focus on DSM-5 and ICD-11 weight criteria and severity specifiers. Eur. Child Adolesc. Psychiatry 2020, 30, 1081–1094. [Google Scholar] [CrossRef]
- Golden, N.H.; Jacobson, M.S.; Sterling, W.M.; Hertz, S. Treatment goal weight in adolescents with anorexia nervosa: Use of BMI percentiles. Int. J. Eat. Disord. 2008, 41, 301–306. [Google Scholar] [CrossRef]
- Lock, J.; Le Grange, D.; Agras, W.S.; Moye, A.; Bryson, S.W.; Jo, B. Randomized Clinical Trial Comparing Family-Based Treatment with Adolescent-Focused Individual Therapy for Adolescents With Anorexia Nervosa. Arch. Gen. Psychiatry 2010, 67, 1025–1032. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Grooten, W.J.A.; Tseli, E.; Äng, B.O.; Boersma, K.; Stålnacke, B.-M.; Gerdle, B.; Enthoven, P. Elaborating on the assessment of the risk of bias in prognostic studies in pain rehabilitation using QUIPS—Aspects of interrater agreement. Diagn. Progn. Res. 2019, 3, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Schulte-Rüther, M.; Mainz, V.; Fink, G.R.; Herpertz-Dahlmann, B.; Konrad, K. Theory of Mind and the Brain in Anorexia Nervosa: Relation to Treatment Outcome. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 832–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howard, W.T.; Evans, K.K.; Quintero-Howard, C.V.; A Bowers, W.; E Andersen, A. Predictors of success or failure of transition to day hospital treatment for inpatients with anorexia nervosa. Am. J. Psychiatry 1999, 156, 1697–1702. [Google Scholar] [CrossRef] [PubMed]
- Seitz, J.; Bühren, K.; Biemann, R.; Timmesfeld, N.; Dempfle, A.; Winter, S.M.; Egberts, K.; Fleischhaker, C.; Wewetzer, C.; Herpertz-Dahlmann, B.; et al. Leptin levels in patients with anorexia nervosa following day/inpatient treatment do not predict weight 1 year post-referral. Eur. Child Adolesc. Psychiatry 2016, 25, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Dardennes, R.; Tolle, V.; Lavoisy, G.; Grouselle, D.; Alanbar, N.; Duriez, P.; Gorwood, P.; Ramoz, N.; Epelbaum, J. Lower leptin level at discharge in acute anorexia nervosa is associated with early weight-loss. Eur. Eat. Disord. Rev. 2021, 29, 634–644. [Google Scholar] [CrossRef]
- Cooper, M.; Guarda, A.S.; Petterway, F.; Schreyer, C.C. Change in normative eating self-efficacy is associated with six-month weight restoration following inpatient treatment for anorexia nervosa. Eat. Behav. 2021, 42, 101518. [Google Scholar] [CrossRef]
- Redgrave, G.W.; Schreyer, C.C.; Coughlin, J.W.; Fischer, L.K.; Pletch, A.; Guarda, A.S. Discharge Body Mass Index, Not Illness Chronicity, Predicts 6-Month Weight Outcome in Patients Hospitalized With Anorexia Nervosa. Front. Psychiatry 2021, 12, 641861. [Google Scholar] [CrossRef]
- Carter, J.C.; McFarlane, T.L.; Bewell, C.; Olmsted, M.P.; Woodside, D.B.; Kaplan, A.S.; Crosby, R.D. Maintenance treatment for anorexia nervosa: A comparison of cognitive behavior therapy and treatment as usual. Int. J. Eat. Disord. 2009, 42, 202–207. [Google Scholar] [CrossRef]
- El Ghoch, M.; Calugi, S.; Chignola, E.; Bazzani, P.V.; Dalle Grave, R. Body mass index, body fat and risk factor of relapse in anorexia nervosa. Eur. J. Clin. Nutr. 2016, 70, 194–198. [Google Scholar] [CrossRef]
- Föcker, M.; Bühren, K.; Timmesfeld, N.; Dempfle, A.; Knoll, S.; Schwarte, R.; Egberts, K.M.; Pfeiffer, E.; Fleischhaker, C.; Wewetzer, C.; et al. The relationship between premorbid body weight and weight at referral, at discharge and at 1-year follow-up in anorexia nervosa. Eur. Child Adolesc. Psychiatry 2014, 24, 537–544. [Google Scholar] [CrossRef]
- Kaplan, A.S.; Walsh, B.T.; Olmsted, M.; Attia, E.; Carter, J.C.; Devlin, M.J.; Pike, K.M.; Woodside, B.; Rockert, W.; Roberto, C.A.; et al. The slippery slope: Prediction of successful weight maintenance in anorexia nervosa. Psychol. Med. 2008, 39, 1037–1045. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Hersch, J.; Bodell, L.P.; Schebendach, J.; Hildebrandt, T.; Walsh, B.T.; Mayer, L.E.S. The association between leptin and weight maintenance outcome in anorexia nervosa. Int. J. Eat. Disord. 2020, 54, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Lund, B.C.; Hernandez, E.R.; Yates, W.R.; Mitchell, J.R.; McKee, P.A.; Johnson, C.L. Rate of inpatient weight restoration predicts outcome in anorexia nervosa. Int. J. Eat. Disord. 2008, 42, 301–305. [Google Scholar] [CrossRef] [PubMed]
- McCormick, L.M.; Keel, P.K.; Bs, M.C.B.; Bowers, W.; Swayze, V.; Andersen, A.; Andreasen, N. Implications of starvation-induced change in right dorsal anterior cingulate volume in anorexia nervosa. Int. J. Eat. Disord. 2008, 41, 602–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormick, L.M.; Keel, P.K.; Brumm, M.C.; Watson, D.B.; Forman-Hoffman, V.L.; Bowers, W.A. A pilot study of personality pathology in patients with anorexia nervosa: Modifiable factors related to outcome after hospitalization. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2009, 14, e113–e120. [Google Scholar] [CrossRef]
- Schebendach, J.E.; Mayer, L.E.; Devlin, M.J.; Attia, E.; Contento, I.R.; Wolf, R.L.; Walsh, B.T. Dietary energy density and diet variety as predictors of outcome in anorexia nervosa. Am. J. Clin. Nutr. 2008, 87, 810–816. [Google Scholar] [CrossRef] [Green Version]
- Bodell, L.P.; Mayer, L.E. Percent body fat is a risk factor for relapse in Anorexia Nervosa: A replication study. Int. J. Eat. Disord. 2010, 44, 118–123. [Google Scholar] [CrossRef]
- Uniacke, B.; Attia, E.; Kaplan, A.; Walsh, B.T. Weight suppression and weight maintenance following treatment of anorexia nervosa. Int. J. Eat. Disord. 2020, 53, 1002–1006. [Google Scholar] [CrossRef]
- Lock, J.; Agras, W.S.; Le Grange, D.; Couturier, J.; Safer, D.; Bryson, S.W. Do end of treatment assessments predict outcome at follow-up in eating disorders? Int. J. Eat. Disord. 2013, 46, 771–778. [Google Scholar] [CrossRef] [Green Version]
- Berends, T.; Boonstra, N.; van Elburg, A. Relapse in anorexia nervosa: A systematic review and meta-analysis. Curr. Opin. Psychiatry 2018, 31, 445–455. [Google Scholar] [CrossRef]
- Goldman-Rakic, P.S. The prefrontal landscape: Implications of functional architecture for understanding human mentation and the central executive. Philos. Trans. R. Soc. B Biol. Sci. 1996, 351, 1445–1453. [Google Scholar] [CrossRef]
- Mesulam, M.-M. Large-scale neurocognitive networks and distributed processing for attention, language, and memory. Ann. Neurol. 1990, 28, 597–613. [Google Scholar] [CrossRef] [PubMed]
- Waterhouse, E.G.; Xu, B. New insights into the role of brain-derived neurotrophic factor in synaptic plasticity. Mol. Cell. Neurosci. 2009, 42, 81–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eskild-Jensen, M.; Støving, R.K.; Flindt, C.F.; Sjogren, M. Comorbid depression as a negative predictor of weight gain during treatment of anorexia nervosa: A systematic scoping review. Eur. Eat. Disord. Rev. 2020, 28, 605–619. [Google Scholar] [CrossRef] [PubMed]
- Cooper, M.; Turner, H. Underlying assumptions and core beliefs in anorexia nervosa and dieting. Br. J. Clin. Psychol. 2000, 39, 215–218. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| First Author, Year | Study Design | Sample Size and Diagnosis | Age, Duration, Severity *, Gender and Country | Intervention and Follow-Up Duration | Definition of Relapse, and Results | Key Findings (Predictors of Relapse Bolded) |
|---|---|---|---|---|---|---|
| Bodell and Mayer, 2011 | Observational-Prospective | n = 21 (AN) | M ± SD = 26.6 (5.5) D: NA S: NA F = 100%; M = 0% USA | Structured behavioral program (weight and eating behavior normalization) FU: 6–9 mo | Def: MROS TTR: NA Relapse rate: 52% |
|
| Carter et al., 2004 | Observational-Prospective | n = 51 (AN) | M ± SD = 26.9 (9.0) D: 6.2 ± 6.8 years S: BMI = 15.1 ± 2.1 F = 100%; M = 0% Canada | Intensive group therapy program (weight and eating behavior normalization) FU: 15 mo | Def: BMI < 17.5 for 3 mo. TTR: M ± SD = 17.0 (4.1) mo Relapse rate: 35% |
|
| Carter et al., 2012 | Observational-Prospective | n = 100 (AN) | M ± SD = 25.4 (7.7) D: 6.3 ± 7.2 years S: BMI = 15.1 ± 1.9 F = 95%; M = 5% Canada | Multidisciplinary:
| Def: BMI < 17.5 for 3 mo. TTR: 4–9 mo Relapse rate = 41% |
|
| Cooper et al., 2021 | Observational-Prospective | n = 146 (AN) | M ± SD = 30.1 (14.39) D: 10.2 ± 11.2 years S: BMI = 15.6 ± 1.8 F = 92.5%; M = 7.5% USA | Behavioral meal-based protocol to help patients interrupt unhealthy eating and weight control behaviors FU: 6 mo | Def: BMI < 19 at FU. TTR: 6 mo Relapse rate: 23% non-responders: 18% |
|
| Dardennes et al., 2021 | Observational-Prospective | n = 26 (AN) | M ± SD = 26.5 (4.3) D: Fair outcome group: 7.6 ± 5.5 years, poor outcome group: 9.1 ± 3.7 years S: BMI = 14.5 ± 1.6 F = 100%; M = 0% France | Behavioral nutritional rehabilitation and weight restoration program FU: 2 mo | Def: BMI < 18 at 2 months FU. TTR: NA Relapse rate: 27% |
|
| El Ghoch et al., 2016 | Observational-Prospective | n = 54 (AN) | M ± SD = 25.3 (7.4) D: 7.9 ± 6.3 years S: BMI: 15.6 ± 1.7 and 14.8 ± 1.6 in treatment success (TS) versus treatment failure (TF) group F = 100%; M = 0% Italy | Inpatient CBT-E and day care before discharge FU: 12 mo | Def: MROS TTR: 12 mo Relapse rate: 52% |
|
| Focker et al., 2015 | Observational- Prospective | n = 161 (AN) | M ± SD = 15.2 (1.5) D: 1.0 ± 0.7 years S: BMI = 15.1 ± 1.3 F = 100%; M = 0% Germany | Day patient treatment after short inpatient care or inpatient Treatment FU: 12 mo | Def: Readmission to inpatient treatment. TTR: 12 mo Relapse rate: 20% | BMI-percentile at discharge significantly predicts BMI percentile at 1-year follow up. |
| Howard et al., 1999 | Observational-retrospective | n = 59 (AN) | M ± SD = 24.8 (8.7) D: 5.0 ± 6.1 years S: 16.0 ± 2.0 F = 100%; M = 0% USA | Transferred from inpatient treatment to a day hospital program FU: NA | Def: Readmission to inpatient treatment. TTR: NA Relapse rate: 24% | At the time of day, hospital admission BMI below 19 significantly predicted day hospital treatment failure. |
| Kaplan et al., 2009 | Observational-Prospective (from RCT) | n = 93 (AN) | M ± SD = 23.3 (4.6) D: 4.5 ± 3.6 years S: NA F = 100%; M = 0% Canada and USA | Behavioral weight restoration program FU: 12 mo | Def: BMI < 18.5 TTR: 6 months Relapse rate: 57% TTR: 12 mo Relapse rate: 72% |
|
| Kim et al., 2020 | Observational-retrospective | n = 41 (AN) | M ± SD = 25 (5.3) D: 7.4 ± 6.1 years S: NA F = 100%; M = 0% USA | Inpatient treatment (weight restoration and reduction of psychological distress) Involved medical management, psychotherapy, and dietary intervention. FU: 12 mo | Def: BMI < 18.5 TTR: 12 mo Relapse rate: 51% |
|
| Lock et al., 2013 | Observational- retrospective (from 5 RCT) | n = 111 AN 83 adolescents 28 adults | M ± SD = 20.2 ± 4.0 D: NA S: BMI adolescents = 16.1 ± 1.1, BMI adults = 18 ± 2.1 F = 100%; M = 0% USA and Canada |
| Def: BMI ≤ 19 TTR: NA Relapse rate: NA |
|
| Lund et al., 2009 | Observational-prospective | n = 79 (AN) | M ± SD = 21.6 ± 7.7 D: 4.8 ± 6.3 years S: BMI = 16.3 ± 1.7 F = 100%; M = 0% USA | Inpatient treatment (weight restoration and reduction of psychological distress) Involved medical management, psychotherapy, and dietary intervention. FU: 12 mo | Def: Increase in CGI-S during the 1-year FU. TTR: 12 mo Relapse rate: 41% |
|
| McCormick et al., 2008 | Observational- retrospective (from NRCT) | n = 18 (AN) n = 10 data on follow up | M ± SD = 25.6 (7.24) D: 6.5 ± 5.3 years S: BMI = 13.5 ± 2.1 F = 66.7%; M = 33.3% USA | Inpatient treatment FU: 12 mo | Def: BMI < 18 TTR: 12 mo Relapse rate: 70% |
|
| McCormick et al., 2009 | Observational-retrospective | n = 20 (AN) | M ± SD = 27.6 (9.45) D: 10.5 ± 8.5 years S: BMI = 16 ± 2.3 F = 100%; M = 0% USA | Inpatient treatment FU: 12 mo | Def: Readmission to a partial or inpatient unit and/or BMI < 17.5 TTR: 12 mo Relapse rate: 35% Unknown: 25% |
|
| Redgrave et al., 2021 | Observational- Prospective | n = 191 (AN or OSFED) -follow up data for n= 99 n = 166 (AN) n = 25 (OSFED) | M ± SD = 32.55 (12.29) D: 13.2 ± 11.6 years S: BMI = 16.2 ± 2.1 F = 100%; M = 0% USA | Behavioral weight restoration program FU: 6 mo | Def: Sustain BMI < 19 for 6 months FU. TTR: NA Relapse rate long-term ill: 21% Relapse rate short-term ill: 31% |
|
| Schebendach et al., 2012 | Observational-Prospective | n = 19 (AN) (16 in the analysis) | M ± SD = 25.8 ± 3.8 D: 6.3 ± 2.9 and 4.0 ± 2.5 years for treatment success (TS) versus treatment failure (TF) group, respectively S: 15.5 ± 1.4 versus 14.6 ± 1.4 for TS versus TF groups F = 100%; M = 0% USA | Multidisciplinary:
| Def: MROS TTR: 9–12 mo Relapse rate: 50% |
|
| Schulte-Ruther et al, 2012 | NRCT | n = 19 (AN) n = 21 (HC) | M ± SD = 15.7 ± 1.5 D: 1.0 ± 0.7 years S: BMI = 15.3 ± 1.5 F = 100%; M = 0% Germany | Multimodal treatment program:
| Def: MROS TTR: NA Relapse rate: NA |
|
| Seitz et al., 2016 | Observational-Prospective (from RCT) | n =121 (AN) | M ± SD = 15.6 (1.5) D: 0.9 ± 0.7 years S: BMI: 15 ± 1.3 F = 100%; M = 0% Germany | Stepped care program of stabilizing inpatient treatment Randomized to inpatient or day-patient care FU: 12 mo | Def: Readmission to hospital following inpatient treatment discharge. TTR: NA Relapse rate: 17% |
|
| Uniacke et al., 2020 | Observational- Retrospective (from RCT) | n = 93 (AN) | M ± SD = 23.3 (4.6) D: 4.7 ± 3.7 years S: BMI = 15.4 ± 1.8 F = 100%; M = 0% USA and Canada | Behavioral weight restoration program FU: 12 mo | Def: Weight maintenance: the BMI never fell below 18.5 kg/m2 for four consecutive weeks TTR: 6 mo: Relapse rate: 57% TTR: 12 mo: Relapse rate: 72% |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frostad, S.; Rozakou-Soumalia, N.; Dârvariu, Ş.; Foruzesh, B.; Azkia, H.; Larsen, M.P.; Rowshandel, E.; Sjögren, J.M. BMI at Discharge from Treatment Predicts Relapse in Anorexia Nervosa: A Systematic Scoping Review. J. Pers. Med. 2022, 12, 836. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050836
Frostad S, Rozakou-Soumalia N, Dârvariu Ş, Foruzesh B, Azkia H, Larsen MP, Rowshandel E, Sjögren JM. BMI at Discharge from Treatment Predicts Relapse in Anorexia Nervosa: A Systematic Scoping Review. Journal of Personalized Medicine. 2022; 12(5):836. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050836
Chicago/Turabian StyleFrostad, Stein, Natalia Rozakou-Soumalia, Ştefana Dârvariu, Bahareh Foruzesh, Helia Azkia, Malina Ploug Larsen, Ehsan Rowshandel, and Jan Magnus Sjögren. 2022. "BMI at Discharge from Treatment Predicts Relapse in Anorexia Nervosa: A Systematic Scoping Review" Journal of Personalized Medicine 12, no. 5: 836. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050836