
Cardiovascular Risk Assessment by SCORE2 Predicts Risk for Colorectal Neoplasia and Tumor-Related Mortality

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Patient Assessment for Risk Factors
2.3. Assessment of Cardiovascular Risk
2.4. Assessment of Colorectal Lesions
2.5. Mortality Data Assessment
2.6. Statistical Analysis
2.7. Ethics Statement
3. Results
3.1. Baseline Demographics in the SCORE2 Strata
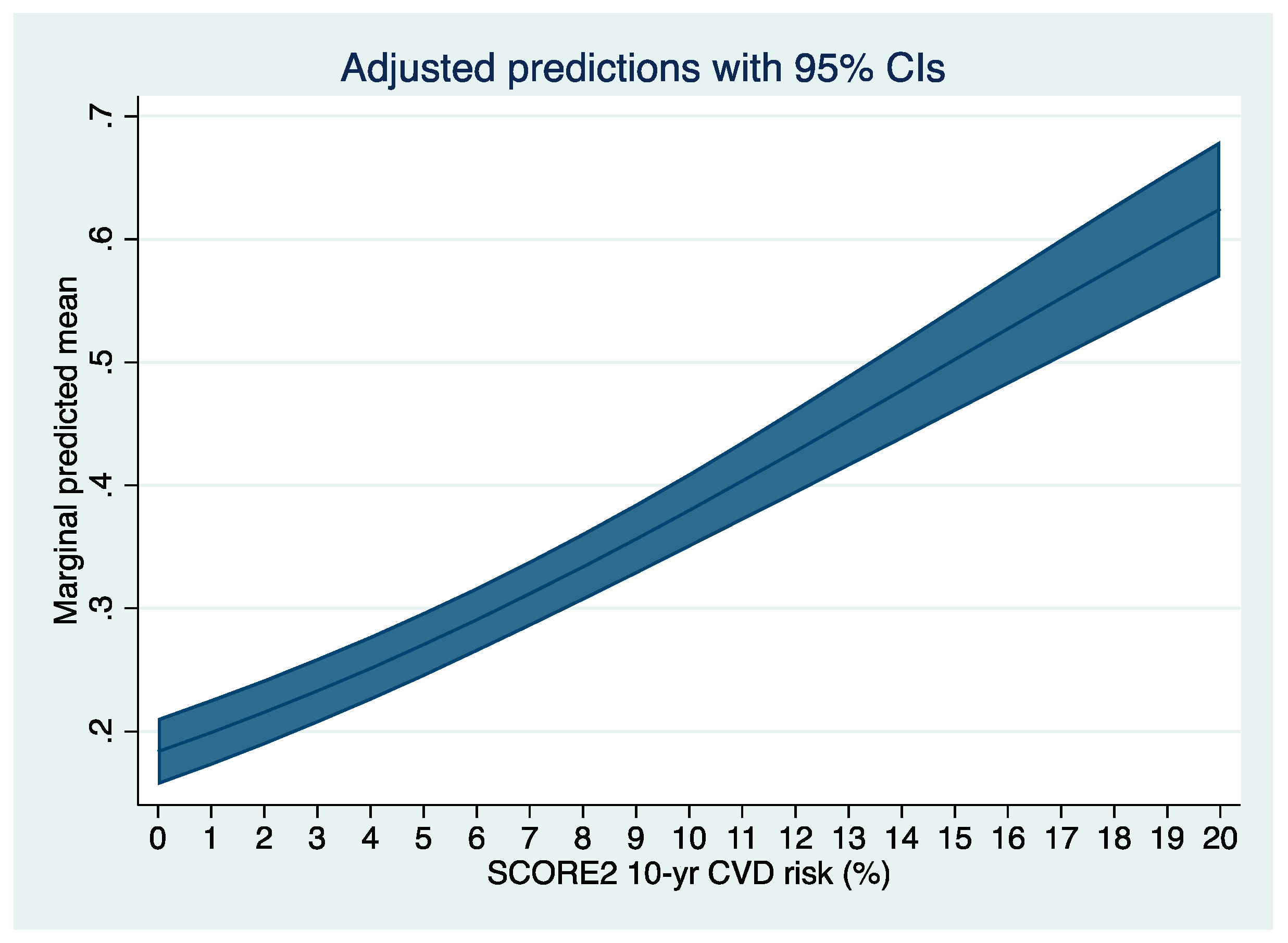
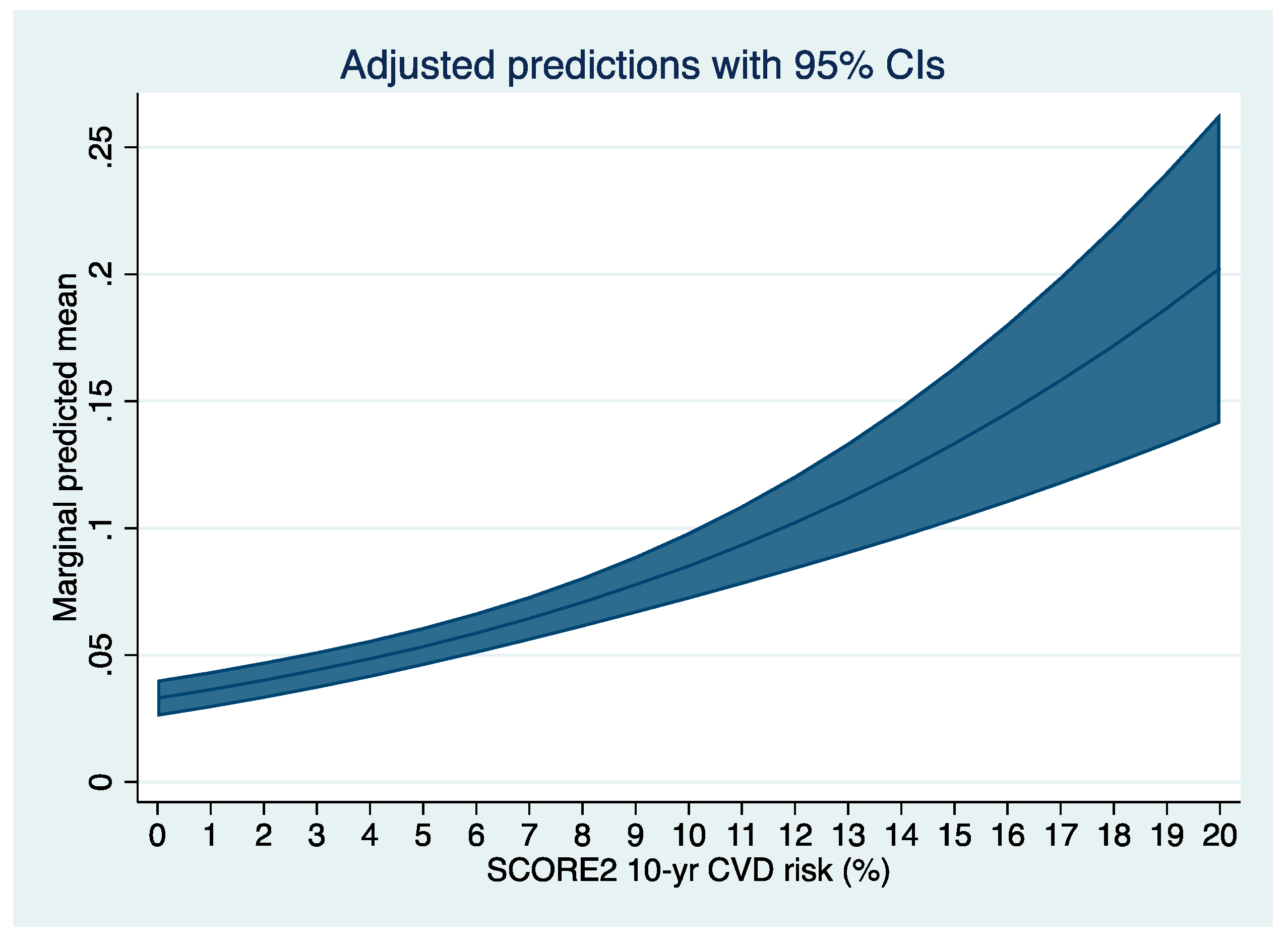
3.2. Association between SCORE2 and Colorectal Adenoma
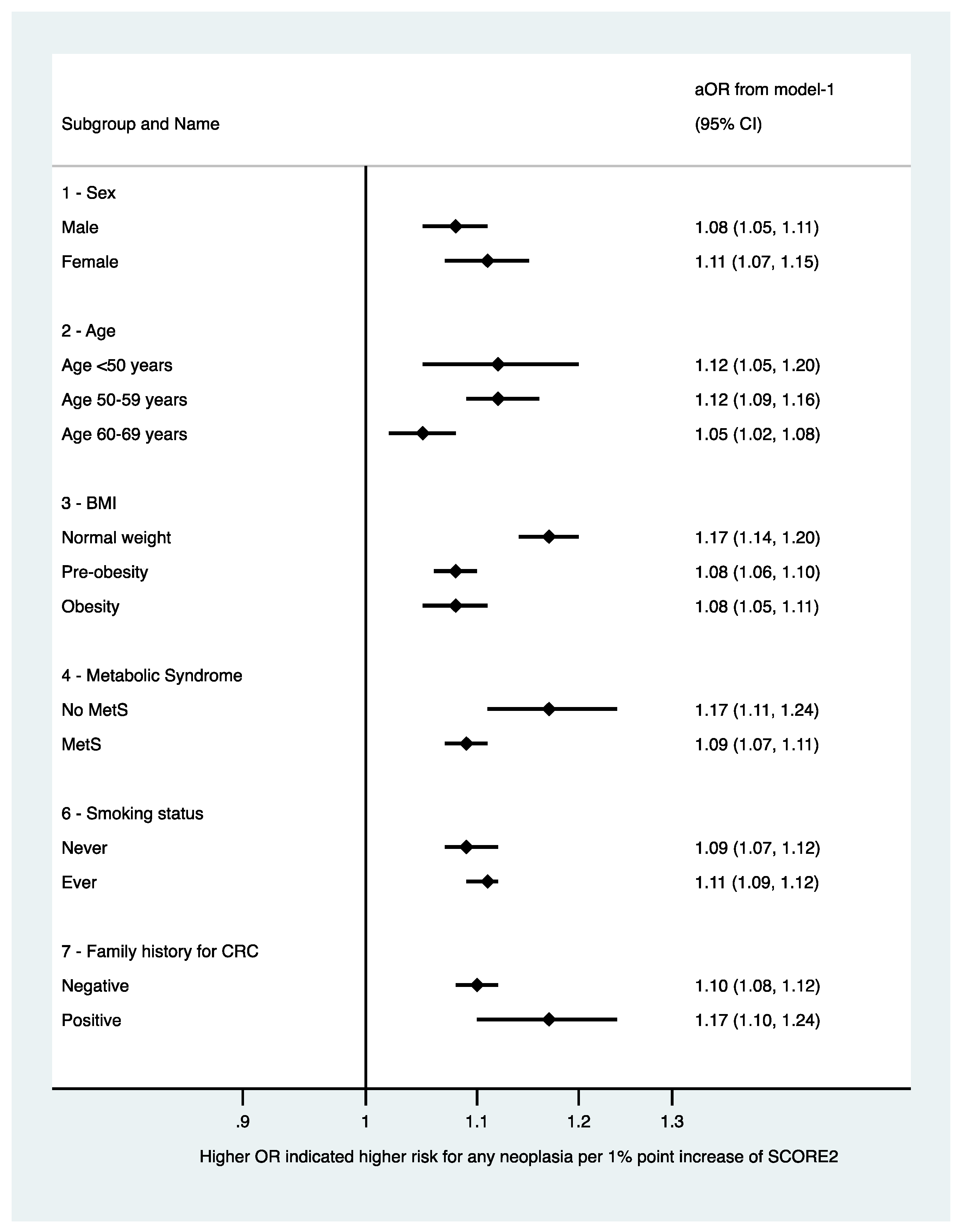
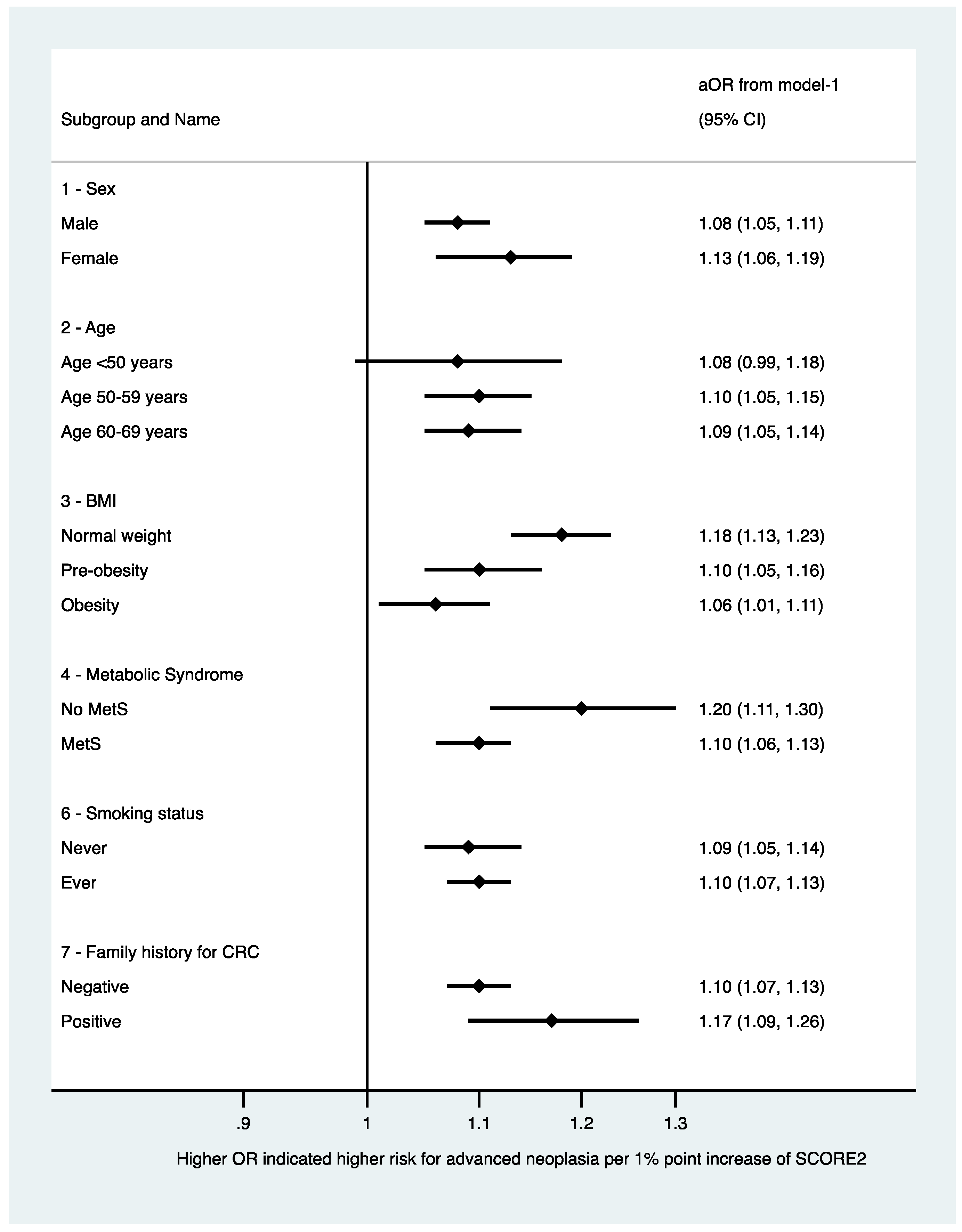
3.3. Sensitivity Analyses
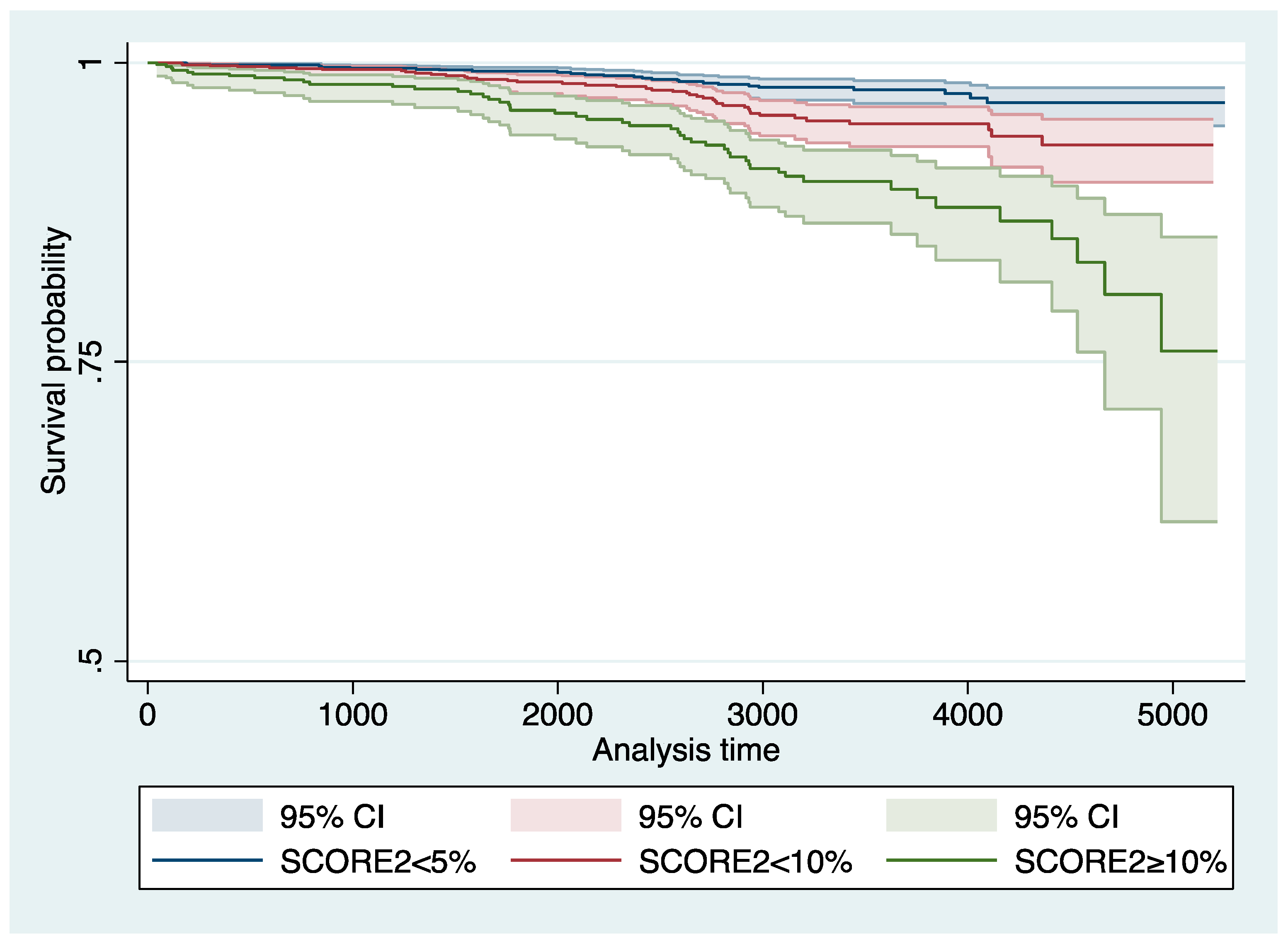
3.4. Association between SCORE2 and Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Demographics Collaborators. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: A comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1160–1203. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, X.; Wang, X.; Liu, Z.; Zhou, H.; Xu, S. Association of Cardiovascular Risk Assessment with Early Colorectal Neoplasia Detection in Asymptomatic Population: A Systematic Review and Meta-Analysis. Clin. Epidemiol. 2020, 12, 865–873. [Google Scholar] [CrossRef] [PubMed]
- Niederseer, D.; Bracher, I.; Stadlmayr, A.; Huber-Schönauer, U.; Plöderl, M.; Obeid, S.; Schmied, C.; Hammerl, S.; Stickel, F.; Lederer, D.; et al. Association between Cardiovascular Risk and Diabetes with Colorectal Neoplasia: A Site-Specific Analysis. J. Clin. Med. 2018, 7, 484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gini, A.; Jansen, E.E.L.; Zielonke, N.; Meester, R.G.S.; Senore, C.; Anttila, A.; Segnan, N.; Mlakar, D.N.; de Koning, H.J.; Lansdorp-Vogelaar, I.; et al. Impact of colorectal cancer screening on cancer-specific mortality in Europe: A systematic review. Eur. J. Cancer 2020, 127, 224–235. [Google Scholar] [CrossRef] [Green Version]
- Quintero, E.; Castells, A.; Bujanda, L.; Cubiella, J.; Salas, D.; Lanas, A.; Andreu, M.; Carballo, F.; Morillas, J.D.; Hernández, C.; et al. Colonoscopy versus Fecal Immunochemical Testing in Colorectal-Cancer Screening. N. Engl. J. Med. 2012, 366, 697–706. [Google Scholar] [CrossRef] [Green Version]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- SCORE2 Working Group; ESC Cardiovascular Risk Collaboration. SCORE2 risk prediction algorithms: New models to estimate 10-year risk of cardiovascular disease in Europe. Eur. Heart J. 2021, 42, ehab309. [Google Scholar]
- Niederseer, D.; Wernly, S.; Bachmayer, S.; Wernly, B.; Bakula, A.; Huber-Schönauer, U.; Semmler, G.; Schmied, C.; Aigner, E.; Datz, C. Diagnosis of Non-Alcoholic Fatty Liver Disease (NAFLD) Is Independently Associated with Cardiovascular Risk in a Large Austrian Screening Cohort. J. Clin. Med. 2020, 9, 1065. [Google Scholar] [CrossRef] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the Metabolic Syndrome. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Bisschops, R.; Areia, M.; Coron, E.; Dobru, D.; Kaskas, B.; Kuvaev, R.; Pech, O.; Ragunath, K.; Weusten, B.; Familiari, P.; et al. Performance measures for lower gastrointestinal endoscopy: A European Society of Gastrointestinal Endoscopy (ESGE) quality improvement initiative. United Eur. Gastroenterol. J. 2017, 5, 309–334. [Google Scholar]
- Bond, J.H. Polyp guideline: Diagnosis, treatment, and surveillance for patients with colorectal polyps. Am. J. Gastroenterol. 2000, 95, 3053–3063. [Google Scholar] [CrossRef] [PubMed]
- Winawer, S.J.; Zauber, A.G. The Advanced Adenoma as the Primary Target of Screening. Gastrointest. Endosc. Clin. N. Am. 2002, 12, 1–9. [Google Scholar] [CrossRef]
- Ferlitsch, M.; Reinhart, K.; Pramhas, S.; Wiener, C.; Gal, O.; Bannert, C.; Hassler, M.; Kozbial, K.; Dunkler, D.; Trauner, M.; et al. Sex-Specific Prevalence of Adenomas, Advanced Adenomas, and Colorectal Cancer in Individuals Undergoing Screening Colonoscopy. JAMA 2011, 306, 1352–1358. [Google Scholar] [CrossRef]
- Wernly, S.; Datz, C.; Wernly, B. RE: Long-Term Colorectal Cancer Incidence and Mortality After Colonoscopy Screening According to Individuals’ Risk Profiles. JNCI J. Natl. Cancer Inst. 2021, 114, 779–780. [Google Scholar] [CrossRef]
- Wernly, S.; Wernly, B.; Semmler, G.; Bachmayer, S.; Niederseer, D.; Stickel, F.; Huber-Schönauer, U.; Aigner, E.; Datz, C. A sex-specific propensity-adjusted analysis of colonic adenoma detection rates in a screening cohort. Sci. Rep. 2021, 11, 17785. [Google Scholar] [CrossRef]
- Levin, T.R.; Corley, D.A.; Jensen, C.D.; Schottinger, J.E.; Quinn, V.P.; Zauber, A.G.; Lee, J.K.; Zhao, W.K.; Udaltsova, N.; Ghai, N.R.; et al. Effects of Organized Colorectal Cancer Screening on Cancer Incidence and Mortality in a Large Community-Based Population. Gastroenterology 2018, 155, 1383–1391.e5. [Google Scholar] [CrossRef]
- Damen, J.A.A.G.; Hooft, L.; Schuit, E.; Debray, T.P.A.; Collins, G.S.; Tzoulaki, I.; Lassale, C.M.; Siontis, G.C.M.; Chiocchia, V.; Roberts, C.; et al. Prediction models for cardiovascular disease risk in the general population: Systematic review. BMJ 2016, 353, i2416. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.W.F.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of Coronary Heart Disease Using Risk Factor Categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef] [Green Version]
- Brindle, P.; Jonathan, E.; Lampe, F.; Walker, M.; Whincup, P.; Fahey, T.; Ebrahim, S. Predictive accuracy of the Framingham coronary risk score in British men:prospective cohort study. BMJ 2003, 327, 1267. [Google Scholar] [CrossRef] [Green Version]
- Goff, D.C.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk. Circulation 2014, 129, S49–S73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Borhani, N.O.; Enright, P.; Furberg, C.D.; Gardin, J.M.; Kronmal, R.A.; Kuller, L.H.; Manolio, T.A.; Mittelmark, M.B.; Newman, A.; et al. The cardiovascular health study: Design and rationale. Ann. Epidemiol. 1991, 1, 263–276. [Google Scholar] [CrossRef]
- Kannel, W.B.; Feinleib, M.; MCnamara, P.M.; Garrison, R.J.; Castelli, W.P. An Investigation Of Coronary Heart Disease In Families. Am. J. Epidemiol. 1979, 110, 281–290. [Google Scholar] [CrossRef]
- Dawber, T.R.; Kannel, W.B.; Lyell, L.P. An Approach To Longitudinal Studies In A Community: The Framingham Study. Ann. N. Y. Acad. Sci. 1963, 107, 539–556. [Google Scholar] [CrossRef] [PubMed]
- The Atherosclerosis Risk in Communities (ARIC) Study: Design and objectives. The ARIC investigators. Am. J. Epidemiol. 1989, 129, 687–702. [Google Scholar]
- Friedman, G.D.; Cutter, G.R.; Donahue, R.P.; Hughes, G.H.; Hulley, S.B.; Jacobs, D.R.; Liu, K.; Savage, P.J. Cardia: Study design, recruitment, and some characteristics of the examined subjects. J. Clin. Epidemiol. 1988, 41, 1105–1116. [Google Scholar] [CrossRef]
- Conroy, R.M.; Pyörälä, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetière, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef]
- Lau, E.S.; Paniagua, S.M.; Liu, E.; Jovani, M.; Li, S.X.; Takvorian, K.; Suthahar, N.; Cheng, S.; Splansky, G.L.; Januzzi, J.L.; et al. Cardiovascular Risk Factors Are Associated With Future Cancer. JACC CardioOncology 2021, 3, 48–58. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Addoh, O. Predictive Validity of the American College of Cardiology/American Heart Association Pooled Cohort Equations in Predicting All-Cause and Cardiovascular Disease–Specific Mortality in a National Prospective Cohort Study of Adults in the United States. Mayo Clin. Proc. 2016, 91, 763–769. [Google Scholar] [CrossRef]
- Niederseer, D.; Stadlmayr, A.; Huber-Schönauer, U.; Plöderl, M.; Schmied, C.; Lederer, D.; Patsch, W.; Aigner, E.; Datz, C. Cardiovascular Risk and Known Coronary Artery Disease Are Associated With Colorectal Adenoma and Advanced Neoplasia. J. Am. Coll. Cardiol. 2017, 69, 2348–2350. [Google Scholar] [CrossRef]
- Godos, J.; Biondi, A.; Galvano, F.; Basile, F.; Sciacca, S.; Giovannucci, E.L.; Grosso, G. Markers of systemic inflammation and colorectal adenoma risk: Meta-analysis of observational studies. World J. Gastroenterol. 2017, 23, 1909–1919. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SCORE2 < 5% | SCORE2 5–9.9% | SCORE2 ≥ 10% | p-Value | |
|---|---|---|---|---|
| N = 1537 | N = 1235 | N = 636 | ||
| Sex | <0.001 | |||
| Male, % (n) | 34% (527) | 65% (803) | 78% (496) | |
| Female, % (n) | 66% (1010) | 35% (432) | 22% (140) | |
| Age (years) | 52 (5) | 58 (6) | 62 (6) | <0.001 |
| Age categories | <0.001 | |||
| Age < 50 years, % (n) | 28% (435) | 7% (88) | 3% (17) | |
| Age 50–59 years, % (n) | 64% (976) | 52% (641) | 30% (180) | |
| Age 60–69 years, % (n) | 8% (126) | 41% (497) | 68% (412) | |
| BMI | 26 (5) | 28 (4) | 29 (5) | <0.001 |
| BMI categories | <0.001 | |||
| Underweight, % (n) | 1% (16) | 0% (4) | 0% (1) | |
| Normal weight, % (n) | 50% (765) | 28% (344) | 20% (126) | |
| Pre–obesity, % (n) | 34% (523) | 47% (586) | 44% (278) | |
| Obesity, % (n) | 15% (233) | 24% (301) | 36% (231) | |
| Systolic BP (mmHg) | 124 (15) | 135 (16) | 147 (20) | <0.001 |
| Diastolic BP (mmHg) | 78 (9) | 82 (9) | 85 (11) | <0.001 |
| Arterial hypertension, % (n) | 32% (493) | 62% (762) | 83% (527) | <0.001 |
| Current smoker, % (n) | 16% (253) | 33% (403) | 45% (289) | <0.001 |
| Ever smoker, % (n) | 62% (952) | 72% (885) | 76% (483) | <0.001 |
| Cholesterol, (mg/dL) | 222 (39) | 229 (44) | 223 (49) | <0.001 |
| LDL (mg/dL) | 140 (36) | 150 (40) | 147 (43) | <0.001 |
| HDL (mg/dL) | 64 (17) | 55 (14) | 50 (13) | <0.001 |
| Triglycerides (mg/dL) | 105 (54) | 141 (100) | 171 (137) | <0.001 |
| CRP (mg/dL) | 0.3 (0.7) | 0.3 (0.5) | 0.4 (0.8) | <0.001 |
| HbA1c (%) | 5.4 (0.4) | 5.5 (0.4) | 5.9 (0.8) | <0.001 |
| Fasting glucose (mg/dL) | 94 (10) | 101 (20) | 118 (43) | <0.001 |
| Metabolic syndrome, % (n) | 64% (980) | 84% (1042) | 93% (594) | <0.001 |
| SCORE2 < 5% | SCORE2 5–9.9% | SCORE2 ≥ 10% | p-Value | |
|---|---|---|---|---|
| N = 1537 | N = 1235 | N = 636 | ||
| Any neoplasia | 20% (313) | 37% (463) | 44% (281) | <0.001 |
| NNS | 5 | 3 | 2 | |
| Mean adenoma detection rate | 0.28 (0.67) | 0.60 (0.97) | 0.96 (1.61) | <0.001 |
| Number of neoplasia | <0.001 | |||
| 0 | 80% (1224) | 63% (772) | 56% (355) | |
| 1 | 15% (233) | 23% (283) | 22% (143) | |
| 2 | 3% (52) | 9% (115) | 8% (51) | |
| 3 | 1% (19) | 4% (44) | 7% (43) | |
| 4 | 0% (6) | 1% (12) | 3% (22) | |
| 5 | 0% (2) | 0% (6) | 1% (8) | |
| 6 | 0% (0) | 0% (2) | 1% (5) | |
| 7 | 0% (1) | 0% (1) | 0% (1) | |
| 8 | 0% (0) | 0% (0) | 1% (5) | |
| 9 | 0% (0) | 0% (0) | 0% (1) | |
| ≥10 | 0% (0) | 0% (0) | 0% (2) | |
| Neoplasia in proximal colon, % (n) | 12% (189) | 23% (289) | 30% (192) | <0.001 |
| Neoplasia in distal colon, % (n) | 8% (128) | 17% (210) | 21% (135) | <0.001 |
| Neoplasia in rectum, % (n) | 3% (48) | 5% (63) | 7% (41) | 0.001 |
| Advanced neoplasia, % (n) | 4% (59) | 7% (86) | 13% (80) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wernly, S.; Semmler, G.; Völkerer, A.; Rezar, R.; Datz, L.; Radzikowski, K.; Stickel, F.; Aigner, E.; Niederseer, D.; Wernly, B.; et al. Cardiovascular Risk Assessment by SCORE2 Predicts Risk for Colorectal Neoplasia and Tumor-Related Mortality. J. Pers. Med. 2022, 12, 848. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050848
Wernly S, Semmler G, Völkerer A, Rezar R, Datz L, Radzikowski K, Stickel F, Aigner E, Niederseer D, Wernly B, et al. Cardiovascular Risk Assessment by SCORE2 Predicts Risk for Colorectal Neoplasia and Tumor-Related Mortality. Journal of Personalized Medicine. 2022; 12(5):848. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050848
Chicago/Turabian StyleWernly, Sarah, Georg Semmler, Andreas Völkerer, Richard Rezar, Leonora Datz, Konrad Radzikowski, Felix Stickel, Elmar Aigner, David Niederseer, Bernhard Wernly, and et al. 2022. "Cardiovascular Risk Assessment by SCORE2 Predicts Risk for Colorectal Neoplasia and Tumor-Related Mortality" Journal of Personalized Medicine 12, no. 5: 848. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050848