
Paucigranulocytic Asthma: Potential Pathogenetic Mechanisms, Clinical Features and Therapeutic Management


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Underlying Mechanisms of PGA
2.1. Low Intensity of Inflammation
2.2. Uncoupling of Airway Remodeling and Hyperresponsiveness from Inflammation
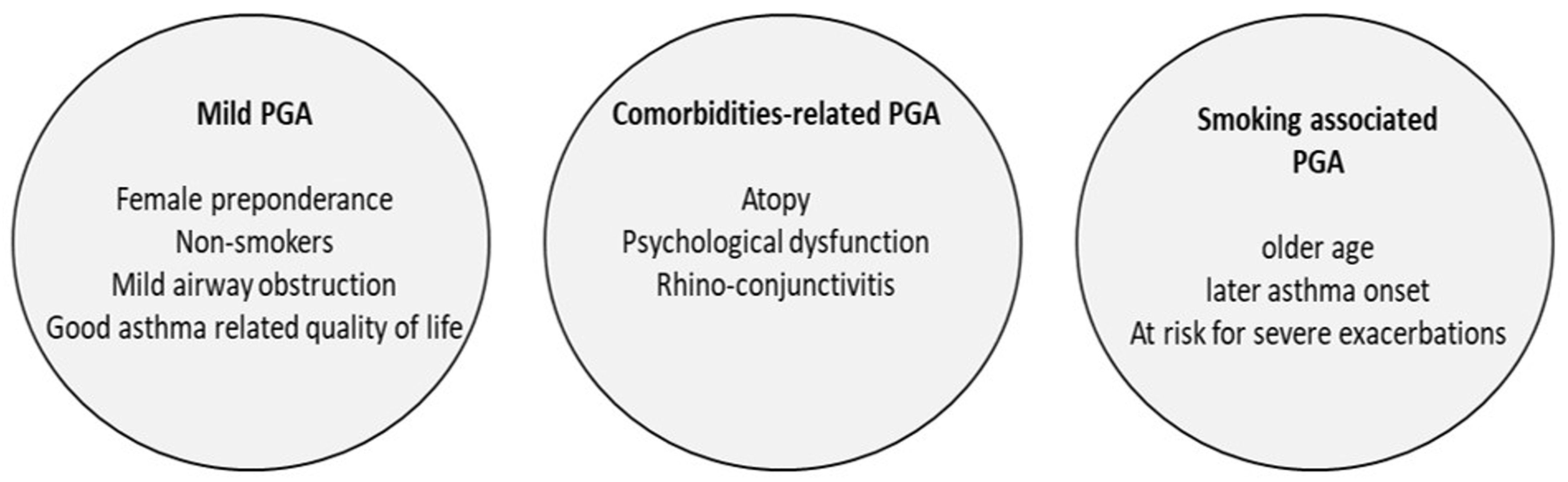
3. Clinical Features of PGA
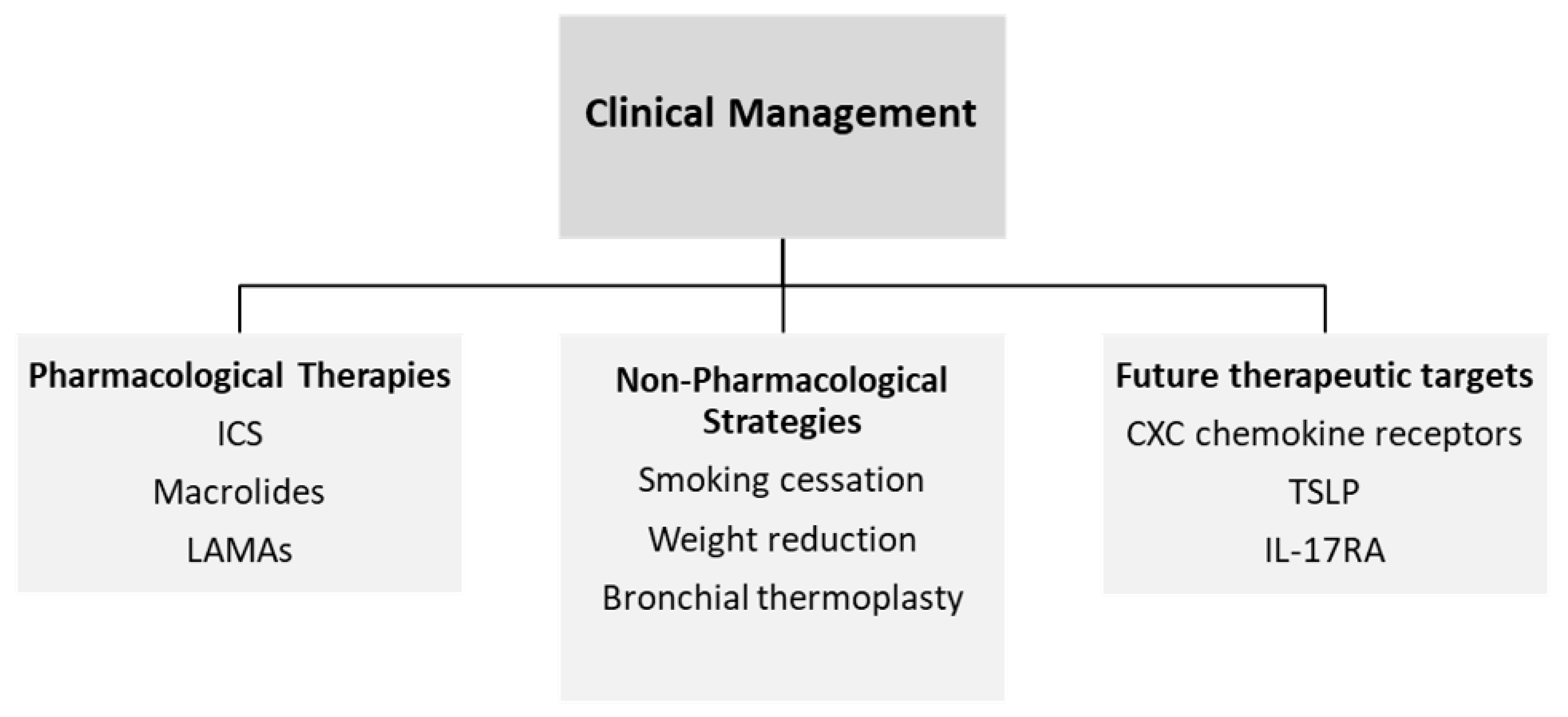
4. Clinical Management of PGA
5. Pharmacological Therapies
5.1. Inhaled Corticosteroids (ICS)
5.2. Macrolides
5.3. LAMAs
6. Non-Pharmacological Strategies
6.1. Smoking Cessation
6.2. Weight Reduction
6.3. Bronchial Thermoplasty
7. Future Therapeutic Targets
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xie, M.; Wenzel, S.E. A global perspective in asthma: From phenotype to endotype. Chin. Med. J. 2013, 1, 166–174. [Google Scholar]
- Turner, A.M.; Tamasi, L.; Schleich, F.; Hoxha, M.; Horvath, I.; Louis, R.; Barnes, N. Clinically relevant subgroups in COPD and asthma. Eur. Respir. Rev. 2015, 136, 283–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, J.L.; Scott, R.; Boyle, M.J.; Gibson, P.G. Inflammatory subtypes in asthma: Assessment and identification using induced sputum. Respirology 2006, 1, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Green, R.H.; Brightling, C.E.; McKenna, S.; Hargadon, B.; Parker, D.; Bradding, P.; Wardlaw, A.J.; Pavord, I.D. Asthma exacerbations and sputum eosinophil counts: A randomised controlled trial. Lancet 2002, 9347, 1715–1721. [Google Scholar] [CrossRef]
- Schleich, F.N.; Seidel, L.; Sele, J.; Manise, M.; Quaedvlieg, V.; Michils, A.; Louis, R. Exhaled nitric oxide thresholds associated with a sputum eosinophil count >/=3% in a cohort of unselected patients with asthma. Thorax 2010, 12, 1039–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, M.; Morgan, A.; Shaw, D.E.; Parker, D.; Green, R.; Brightling, C.; Bradding, P.; Wardlaw, A.J.; Pavord, I.D. Pathological features and inhaled corticosteroid response of eosinophilic and non-eosinophilic asthma. Thorax 2007, 12, 1043–1049. [Google Scholar] [CrossRef] [Green Version]
- Berry, M.A.; Shaw, D.E.; Green, R.H.; Brightling, C.E.; Wardlaw, A.J.; Pavord, I.D. The use of exhaled nitric oxide concentration to identify eosinophilic airway inflammation: An observational study in adults with asthma. Clin. Exp. Allergy 2005, 9, 1175–1179. [Google Scholar] [CrossRef]
- Hargreave, F.E.; Nair, P. Point: Is measuring sputum eosinophils useful in the management of severe asthma? Yes. Chest 2011, 6, 1270–1273. [Google Scholar] [CrossRef] [Green Version]
- Ntontsi, P.; Loukides, S.; Bakakos, P.; Kostikas, K.; Papatheodorou, G.; Papathanassiou, E.; Hillas, G.; Koulouris, N.; Papiris, S.; Papaioannou, A.I. Clinical, functional and inflammatory characteristics in patients with paucigranulocytic stable asthma: Comparison with different sputum phenotypes. Allergy 2017, 11, 1761–1767. [Google Scholar] [CrossRef]
- Baines, K.J.; Simpson, J.L.; Wood, L.G.; Scott, R.J.; Gibson, P.G. Transcriptional phenotypes of asthma defined by gene expression profiling of induced sputum samples. J. Allergy Clin. Immunol. 2011, 1, 153–160, 160 e1-9. [Google Scholar] [CrossRef]
- Wang, G.; Baines, K.J.; Fu, J.J.; Wood, L.G.; Simpson, J.L.; McDonald, V.M.; Cowan, D.C.; Taylor, D.R.; Cowan, J.O.; Gibson, P.G. Sputum mast cell subtypes relate to eosinophilia and corticosteroid response in asthma. Eur. Respir. J. 2016, 4, 1123–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demarche, S.; Schleich, F.; Henket, M.; Paulus, V.; Van Hees, T.; Louis, R. Detailed analysis of sputum and systemic inflammation in asthma phenotypes: Are paucigranulocytic asthmatics really non-inflammatory? BMC Pulm. Med. 2016, 16, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, P.G. Inflammatory phenotypes in adult asthma: Clinical applications. Clin. Respir. J. 2009, 4, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Deng, K.; Zhang, X.; Liu, Y.; Zhang, L.; Wang, G.; Feng, M.; Oliver, B.G.; Wang, L.; Hansbro, P.M.; Qin, L.; et al. Heterogeneity of Paucigranulocytic Asthma: A Prospective Cohort Study with Hierarchical Cluster Analysis. J. Allergy Clin. Immunol. Pract. 2021, 6, 2344–2355. [Google Scholar] [CrossRef]
- Simpson, J.L.; Scott, R.J.; Boyle, M.J.; Gibson, P.G. Differential proteolytic enzyme activity in eosinophilic and neutrophilic asthma. Am. J. Respir. Crit. Care Med. 2005, 5, 559–565. [Google Scholar] [CrossRef]
- Steinke, J.W.; Lawrence, M.G.; Teague, W.G.; Braciale, T.J.; Patrie, J.T.; Borish, L. Bronchoalveolar lavage cytokine patterns in children with severe neutrophilic and paucigranulocytic asthma. J. Allergy Clin. Immunol. 2021, 2, 686–693 e3. [Google Scholar] [CrossRef]
- Tliba, O.; Panettieri, R.A., Jr. Paucigranulocytic asthma: Uncoupling of airway obstruction from inflammation. J. Allergy Clin. Immunol. 2019, 4, 1287–1294. [Google Scholar] [CrossRef] [Green Version]
- Hudey, S.N.; Ledford, D.K.; Cardet, J.C. Mechanisms of non-type 2 asthma. Curr. Opin. Immunol. 2020, 66, 123–128. [Google Scholar] [CrossRef]
- Panettieri, R.A., Jr. Neutrophilic and Pauci-immune Phenotypes in Severe Asthma. Immunol. Allergy Clin N. Am. 2016, 3, 569–579. [Google Scholar] [CrossRef]
- Damera, G.; Panettieri, R.A., Jr. Does airway smooth muscle express an inflammatory phenotype in asthma? Br. J. Pharmacol. 2011, 1, 68–80. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Zhu, W.; Wang, C.; Zheng, Y.; Sun, S.; Fang, Y.; Luo, Z. Weighted gene co-expression network analysis to identify key modules and hub genes associated with paucigranulocytic asthma. BMC Pulm. Med. 2021, 1, 343. [Google Scholar] [CrossRef] [PubMed]
- Kambayashi, T.; Wallin, R.P.; Ljunggren, H.G. cAMP-elevating agents suppress dendritic cell function. J. Leukoc. Biol. 2001, 6, 903–910. [Google Scholar]
- Chang, H.C.; Huang, P.H.; Syu, F.S.; Hsieh, C.H.; Chang, S.L.; Lu, J.; Chen, H.C. Critical involvement of atypical chemokine receptor CXCR7 in allergic airway inflammation. Immunology 2018, 2, 274–284. [Google Scholar] [CrossRef] [PubMed]
- De Filippo, K.; Dudeck, A.; Hasenberg, M.; Nye, E.; van Rooijen, N.; Hartmann, K.; Gunzer, M.; Roers, A.; Hogg, N. Mast cell and macrophage chemokines CXCL1/CXCL2 control the early stage of neutrophil recruitment during tissue inflammation. Blood 2013, 24, 4930–4937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irukayama-Tomobe, Y.; Tanaka, H.; Yokomizo, T.; Hashidate-Yoshida, T.; Yanagisawa, M.; Sakurai, T. Aromatic D-amino acids act as chemoattractant factors for human leukocytes through a G protein-coupled receptor, GPR109B. Proc. Natl. Acad. Sci. USA 2009, 10, 3930–3934. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, A.; Damera, G.; Bhandare, R.; Gu, S.; Lopez-Boado, Y.S.; Panettieri, R.A., Jr.; Tliba, O. Vitamin D and glucocorticoids differentially modulate chemokine expression in human airway smooth muscle cells. Br. J. Pharmacol. 2008, 1, 84–92. [Google Scholar] [CrossRef] [Green Version]
- Black, J.L.; Panettieri, R.A.; Banerjee, A.; Berger, P. Airway smooth muscle in asthma: Just a target for bronchodilation? Clin. Chest Med. 2012, 3, 543–558. [Google Scholar] [CrossRef] [Green Version]
- Davies, D.E. Epithelial barrier function and immunity in asthma. Ann. Am. Thorac Soc. 2014, 11 (Suppl. 5), S244–S251. [Google Scholar] [CrossRef]
- Ammit, A.J.; Lazaar, A.L.; Irani, C.; O’Neill, G.M.; Gordon, N.D.; Amrani, Y.; Penn, R.B.; Panettieri, R.A., Jr. Tumor necrosis factor-alpha-induced secretion of RANTES and interleukin-6 from human airway smooth muscle cells: Modulation by glucocorticoids and beta-agonists. Am. J. Respir. Cell Mol. Biol. 2002, 4, 465–474. [Google Scholar] [CrossRef]
- Amrani, Y.; Lazaar, A.L.; Panettieri, R.A., Jr. Up-regulation of ICAM-1 by cytokines in human tracheal smooth muscle cells involves an NF-kappa B-dependent signaling pathway that is only partially sensitive to dexamethasone. J. Immunol. 1999, 4, 2128–2134. [Google Scholar]
- Bhandare, R.; Damera, G.; Banerjee, A.; Flammer, J.R.; Keslacy, S.; Rogatsky, I.; Panettieri, R.A.; Amrani, Y.; Tliba, O. Glucocorticoid receptor interacting protein-1 restores glucocorticoid responsiveness in steroid-resistant airway structural cells. Am. J. Respir. Cell Mol. Biol. 2010, 1, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tliba, O.; Panettieri, R.A.; Tliba, S.; Walseth, T.F.; Amrani, Y. Tumor necrosis factor-alpha differentially regulates the expression of proinflammatory genes in human airway smooth muscle cells by activation of interferon-beta-dependent CD38 pathway. Mol. Pharmacol. 2004, 2, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Tliba, O.; Tliba, S.; Da Huang, C.; Hoffman, R.K.; DeLong, P.; Panettieri, R.A.; Amrani, Y. Tumor necrosis factor alpha modulates airway smooth muscle function via the autocrine action of interferon beta. J. Biol. Chem. 2003, 50, 50615–50623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frossard, N.; Freund, V.; Advenier, C. Nerve growth factor and its receptors in asthma and inflammation. Eur. J. Pharmacol. 2004, 500, 453–465. [Google Scholar] [CrossRef]
- Braun, A.; Quarcoo, D.; Schulte-Herbrüggen, O.; Lommatzsch, M.; Hoyle, G.; Renz, H. Nerve growth factor induces airway hyperresponsiveness in mice. Int. Arch. Allergy Immunol. 2001, 124, 205–207. [Google Scholar] [CrossRef]
- Balenga, N.A.; Jester, W.; Jiang, M.; Panettieri, R.A., Jr.; Druey, K.M. Loss of regulator of G protein signaling 5 promotes airway hyperresponsiveness in the absence of allergic inflammation. J. Allergy Clin. Immunol. 2014, 2, 451–459. [Google Scholar] [CrossRef] [Green Version]
- Gabehart, K.E.; Royce, S.G.; Maselli, D.J.; Miyasato, S.K.; Davis, E.C.; Tang, M.L.; Jourdan Le Saux, C. Airway hyperresponsiveness is associated with airway remodeling but not inflammation in aging Cav1-/- mice. Respir. Res. 2013, 1, 110. [Google Scholar] [CrossRef] [Green Version]
- Kramer, E.L.; Mushaben, E.M.; Pastura, P.A.; Acciani, T.H.; Deutsch, G.H.; Khurana Hershey, G.K.; Korfhagen, T.R.; Hardie, W.D.; Whitsett, J.A.; Le Cras, T.D. Early growth response-1 suppresses epidermal growth factor receptor-mediated airway hyperresponsiveness and lung remodeling in mice. Am. J. Respir. Cell Mol. Biol. 2009, 4, 415–425. [Google Scholar] [CrossRef]
- Miller, M.; Rosenthal, P.; Beppu, A.; Mueller, J.L.; Hoffman, H.M.; Tam, A.B.; Doherty, T.A.; McGeough, M.D.; Pena, C.A.; Suzukawa, M.; et al. ORMDL3 transgenic mice have increased airway remodeling and airway responsiveness characteristic of asthma. J. Immunol. 2014, 8, 3475–3487. [Google Scholar] [CrossRef] [Green Version]
- Das, S.; Miller, M.; Beppu, A.K.; Mueller, J.; McGeough, M.D.; Vuong, C.; Karta, M.R.; Rosenthal, P.; Chouiali, F.; Doherty, T.A.; et al. GSDMB induces an asthma phenotype characterized by increased airway responsiveness and remodeling without lung inflammation. Proc. Natl. Acad. Sci. USA 2016, 46, 13132–13137. [Google Scholar] [CrossRef] [Green Version]
- Amrani, Y.; Tliba, O.; Deshpande, D.A.; Walseth, T.F.; Kannan, M.S.; Panettieri, R.A., Jr. Bronchial hyperresponsiveness: Insights into new signaling molecules. Curr. Opin. Pharmacol. 2004, 3, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Elliot, J.G.; Noble, P.B.; Mauad, T.; Bai, T.R.; Abramson, M.J.; McKay, K.O.; Green, F.H.; James, A.L. Inflammation-dependent and independent airway remodelling in asthma. Respirology 2018, 12, 1138–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, W.; Han, G.J.; Zhu, Y.J.; Mao, D.; Hu, H. Clinical characteristics and biomarkers analysis of asthma inflammatory phenotypes. Biomark Med. 2020, 3, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Ricciardolo, F.L.M.; Carriero, V.; Bertolini, F. Which Therapy for Non-Type(T)2/T2-Low Asthma. J. Pers Med. 2021, 12, 10. [Google Scholar] [CrossRef] [PubMed]
- Svenningsen, S.; Nair, P. Asthma Endotypes and an Overview of Targeted Therapy for Asthma. Front. Med. 2017, 4, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, N.C. Recent Developments In Bronchial Thermoplasty For Severe Asthma. J. Asthma Allergy 2019, 12, 375–387. [Google Scholar] [CrossRef] [Green Version]
- McGrath, K.W.; Icitovic, N.; Boushey, H.A.; Lazarus, S.C.; Sutherland, E.R.; Chinchilli, V.M.; Fahy, J.V. A large subgroup of mild-to-moderate asthma is persistently noneosinophilic. Am. J. Respir. Crit. Care Med. 2012, 6, 612–619. [Google Scholar] [CrossRef]
- Good, J.T.; Rollins, D.R.; Jr Martin, R.J. Macrolides in the treatment of asthma. Curr. Opin. Pulm. Med. 2012, 1, 76–84. [Google Scholar] [CrossRef] [Green Version]
- Simpson, J.L.; Powell, H.; Boyle, M.J.; Scott, R.J.; Gibson, P.G. Clarithromycin targets neutrophilic airway inflammation in refractory asthma. Am. J. Respir. Crit. Care Med. 2008, 2, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Brusselle, G.G.; VanderStichele, C.; Jordens, P.; Deman, R.; Slabbynck, H.; Ringoet, V.; Verleden, G.; Demedts, I.K.; Verhamme, K.; Delporte, A.; et al. Azithromycin for prevention of exacerbations in severe asthma (AZISAST): A multicentre randomised double-blind placebo-controlled trial. Thorax 2013, 4, 322–329. [Google Scholar] [CrossRef] [Green Version]
- Gibson, P.G.; Yang, I.A.; Upham, J.W.; Reynolds, P.N.; Hodge, S.; James, A.L.; Jenkins, C.; Peters, M.J.; Marks, G.B.; Baraket, M.; et al. Effect of azithromycin on asthma exacerbations and quality of life in adults with persistent uncontrolled asthma (AMAZES): A randomised, double-blind, placebo-controlled trial. Lancet 2017, 10095, 659–668. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.L.; Leong, L.E.; Mobegi, F.M.; Choo, J.M.; Wesselingh, S.; Yang, I.A.; Upham, J.W.; Reynolds, P.N.; Hodge, S.; James, A.L.; et al. Long-Term Azithromycin Reduces Haemophilus influenzae and Increases Antibiotic Resistance in Severe Asthma. Am. J. Respir. Crit. Care Med. 2019, 3, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2014, 2, 343–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Initiative for Asthma. GINA Workshop Report, Global Strategy for Asthma Management and Prevention. Revised 2021. Available online: http://www.ginasthma.org (accessed on 9 April 2022).
- Kerstjens, H.A.; Disse, B.; Schröder-Babo, W.; Bantje, T.A.; Gahlemann, M.; Sigmund, R.; Engel, M.; van Noord, J.A. Tiotropium improves lung function in patients with severe uncontrolled asthma: A randomized controlled trial. J. Allergy Clin. Immunol. 2011, 2, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, S.C.; Krishnan, J.A.; King, T.S.; Lang, J.E.; Blake, K.V.; Covar, R.; Lugogo, N.; Wenzel, S.; Chinchilli, V.M.; Mauger, D.T.; et al. Mometasone or Tiotropium in Mild Asthma with a Low Sputum Eosinophil Level. N. Engl. J. Med. 2019, 21, 2009–2019. [Google Scholar] [CrossRef] [PubMed]
- Casale, T.B.; Bateman, E.D.; Vandewalker, M.; Virchow, J.C.; Schmidt, H.; Engel, M.; Moroni-Zentgraf, P.; Kerstjens, H.A. Tiotropium Respimat Add-on Is Efficacious in Symptomatic Asthma, Independent of T2 Phenotype. J. Allergy Clin. Immunol. Pract. 2018, 3, 923–935 e9. [Google Scholar] [CrossRef]
- Lee, L.A.; Bailes, Z.; Barnes, N.; Boulet, L.P.; Edwards, D.; Fowler, A.; Hanania, N.A.; Kerstjens, H.A.; Kerwin, E.; Nathan, R.; et al. Efficacy and safety of once-daily single-inhaler triple therapy (FF/UMEC/VI) versus FF/VI in patients with inadequately controlled asthma (CAPTAIN): A double-blind, randomised, phase 3A trial. Lancet Respir. Med. 2021, 1, 69–84. [Google Scholar] [CrossRef]
- Stapleton, M.; Howard-Thompson, A.; George, C.; Hoover, R.M.; Self, T.H. Smoking and asthma. J. Am. Board Fam. Med. 2011, 3, 313–322. [Google Scholar] [CrossRef]
- Thomson, N.C.; Chaudhuri, R.; Livingston, E. Asthma and cigarette smoking. Eur. Respir. J. 2004, 5, 822–833. [Google Scholar] [CrossRef] [Green Version]
- Henderson, I.; Caiazzo, E.; McSharry, C.; Guzik, T.J.; Maffia, P. Why do some asthma patients respond poorly to glucocorticoid therapy? Pharmacol. Res. 2020, 160, 105189. [Google Scholar] [CrossRef]
- Bel, E.H. Smoking: A neglected cause of glucocorticoid resistance in asthma. Am. J. Respir. Crit. Care Med. 2003, 11, 1265–1266. [Google Scholar] [CrossRef] [PubMed]
- Ramamoorthy, S.; Cidlowski, J.A. Ligand-induced repression of the glucocorticoid receptor gene is mediated by an NCoR1 repression complex formed by long-range chromatin interactions with intragenic glucocorticoid response elements. Mol. Cell Biol. 2013, 9, 1711–1722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, K.; Lim, S.; Caramori, G.; Chung, K.F.; Barnes, P.J.; Adcock, I.M. Cigarette smoking reduces histone deacetylase 2 expression, enhances cytokine expression, and inhibits glucocorticoid actions in alveolar macrophages. FASEB J. 2001, 6, 1110–1112. [Google Scholar] [CrossRef] [Green Version]
- Adcock, I.M.; Barnes, P.J. Molecular mechanisms of corticosteroid resistance. Chest 2008, 2, 394–401. [Google Scholar] [CrossRef] [Green Version]
- Barnes, P.J. Corticosteroid resistance in patients with asthma and chronic obstructive pulmonary disease. J. Allergy Clin. Immunol. 2013, 3, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Carr, T.F. Treatment approaches for the patient with T2 low asthma. Ann. Allergy Asthma Immunol. 2021, 5, 530–535. [Google Scholar] [CrossRef]
- Chaudhuri, R.; Livingston, E.; McMahon, A.D.; Lafferty, J.; Fraser, I.; Spears, M.; McSharry, C.P.; Thomson, N.C. Effects of smoking cessation on lung function and airway inflammation in smokers with asthma. Am. J. Respir. Crit. Care Med. 2006, 2, 127–133. [Google Scholar] [CrossRef]
- Rayens, M.K.; Burkhart, P.V.; Zhang, M.; Lee, S.; Moser, D.K.; Mannino, D.; Hahn, E.J. Reduction in asthma-related emergency department visits after implementation of a smoke-free law. J. Allergy Clin. Immunol. 2008, 3, 537–541 e3. [Google Scholar] [CrossRef]
- Westergaard, C.G.; Porsbjerg, C.; Backer, V. The effect of smoking cessation on airway inflammation in young asthma patients. Clin. Exp. Allergy 2014, 3, 353–361. [Google Scholar] [CrossRef]
- Marijsse, G.S.; Seys, S.F.; Schelpe, A.S.; Dilissen, E.; Goeminne, P.; Dupont, L.J.; Ceuppens, J.L.; Bullens, D.M. Obese individuals with asthma preferentially have a high IL-5/IL-17A/IL-25 sputum inflammatory pattern. Am. J. Respir. Crit. Care Med. 2014, 10, 1284–1285. [Google Scholar] [CrossRef]
- Rastogi, D. Pediatric obesity-related asthma: A prototype of pediatric severe non-T2 asthma. Pediatr. Pulmonol. 2020, 3, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Todd, D.C.; Armstrong, S.; D’silva, L.; Allen, C.J.; Hargreave, F.E.; Parameswaran, K. Effect of obesity on airway inflammation: A cross-sectional analysis of body mass index and sputum cell counts. Clin. Exp. Allergy 2007, 7, 1049–1054. [Google Scholar] [CrossRef] [PubMed]
- Pakhale, S.; Baron, J.; Dent, R.; Vandemheen, K.; Aaron, S.D. Effects of weight loss on airway responsiveness in obese adults with asthma: Does weight loss lead to reversibility of asthma? Chest 2015, 6, 1582–1590. [Google Scholar] [CrossRef] [PubMed]
- Charron, C.B.; Pakhalé, S. The role of airway hyperresponsiveness measured by methacholine challenge test in defining asthma severity in asthma-obesity syndrome. Curr. Opin. Allergy Clin. Immunol. 2016, 3, 218–223. [Google Scholar] [CrossRef]
- Simard, B.; Turcotte, H.; Cockcroft, D.W.; Davis, B.E.; Boulay, M.È.; Boulet, L.P. Deep inspiration avoidance and methacholine response in normal subjects and patients with asthma. Chest 2005, 1, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Boulet, L.P.; Turcotte, H.; Boulet, G.; Simard, B.; Robichaud, P. Deep inspiration avoidance and airway response to methacholine: Influence of body mass index. Can. Respir. J. 2005, 7, 371–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulet, L.P.; Hamid, Q. Symposium on obesity and asthma—November 2, 2006. Can. Respir. J. 2007, 4, 201–208. [Google Scholar] [CrossRef] [Green Version]
- Boulet, L.P.; Des Cormiers, A. The link between obesity and asthma: A Canadian perspective. Can. Respir. J. 2007, 4, 217–220. [Google Scholar] [CrossRef]
- Boulet, L.P. Influence of obesity on the prevalence and clinical features of asthma. Clin. Investig. Med. 2008, 6, E386–E390. [Google Scholar] [CrossRef] [Green Version]
- Nair, P.; Radford, K.; Fanat, A.; Janssen, L.J.; Peters-Golden, M.; Cox, P.G. The effects of leptin on airway smooth muscle responses. Am. J. Respir. Cell Mol. Biol. 2008, 4, 475–481. [Google Scholar] [CrossRef]
- Cardet, J.C.; Ash, S.; Kusa, T.; Camargo, C.A.; Israel, E. Insulin resistance modifies the association between obesity and current asthma in adults. Eur. Respir. J. 2016, 2, 403–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.C.; Tu, Y.K.; Huang, K.C.; Chen, P.C.; Chu, D.C.; Lee, Y.L. Pathway from central obesity to childhood asthma. Physical fitness and sedentary time are leading factors. Am. J. Respir. Crit. Care Med. 2014, 10, 1194–1203. [Google Scholar] [CrossRef] [PubMed]
- Dias-Júnior, S.A.; Reis, M.; de Carvalho-Pinto, R.M.; Stelmach, R.; Halpern, A.; Cukier, A. Effects of weight loss on asthma control in obese patients with severe asthma. Eur. Respir. J. 2014, 5, 1368–1377. [Google Scholar] [CrossRef] [Green Version]
- van Huisstede, A.; Rudolphus, A.; Cabezas, M.C.; Biter, L.U.; van de Geijn, G.J.; Taube, C.; Hiemstra, P.S.; Braunstahl, G.J. Effect of bariatric surgery on asthma control, lung function and bronchial and systemic inflammation in morbidly obese subjects with asthma. Thorax 2015, 7, 659–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasegawa, K.; Tsugawa, Y.; Chang, Y.; Camargo, C.A., Jr. Risk of an asthma exacerbation after bariatric surgery in adults. J. Allergy Clin. Immunol. 2015, 2, 288–294 e8. [Google Scholar] [CrossRef] [PubMed]
- Nyenhuis, S.M.; Dixon, A.E.; Ma, J. Impact of Lifestyle Interventions Targeting Healthy Diet, Physical Activity, and Weight Loss on Asthma in Adults: What Is the Evidence? J. Allergy Clin. Immunol. Pract. 2018, 3, 751–763. [Google Scholar] [CrossRef]
- Pretolani, M.; Bergqvist, A.; Thabut, G.; Dombret, M.C.; Knapp, D.; Hamidi, F.; Alavoine, L.; Taillé, C.; Chanez, P.; Erjefält, J.S.; et al. Effectiveness of bronchial thermoplasty in patients with severe refractory asthma: Clinical and histopathologic correlations. J. Allergy Clin. Immunol. 2017, 4, 1176–1185. [Google Scholar] [CrossRef] [Green Version]
- Facciolongo, N.; Di Stefano, A.; Pietrini, V.; Galeone, C.; Bellanova, F.; Menzella, F.; Scichilone, N.; Piro, R.; Bajocchi, G.L.; Balbi, B.; et al. Nerve ablation after bronchial thermoplasty and sustained improvement in severe asthma. BMC Pulm. Med. 2018, 1, 29. [Google Scholar] [CrossRef]
- Papakonstantinou, E.; Koletsa, T.; Zhou, L.; Fang, L.; Roth, M.; Karakioulaki, M.; Savic, S.; Grize, L.; Tamm, M.; Stolz, D. Bronchial thermoplasty in asthma: An exploratory histopathological evaluation in distinct asthma endotypes/phenotypes. Respir. Res. 2021, 1, 186. [Google Scholar] [CrossRef]
- Cox, G.; Thomson, N.C.; Rubin, A.S.; Niven, R.M.; Corris, P.A.; Siersted, H.C.; Olivenstein, R.; Pavord, I.D.; McCormack, D.; Chaudhuri, R.; et al. Asthma control during the year after bronchial thermoplasty. N. Engl. J. Med. 2007, 13, 1327–1337. [Google Scholar] [CrossRef] [Green Version]
- Pavord, I.D.; Cox, G.; Thomson, N.C.; Rubin, A.S.; Corris, P.A.; Niven, R.M.; Chung, K.F.; Laviolette, M.; RISA Trial Study Group. Safety and efficacy of bronchial thermoplasty in symptomatic, severe asthma. Am. J. Respir. Crit. Care Med. 2007, 12, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.; Rubin, A.S.; Laviolette, M.; Fiterman, J.; De Andrade Lima, M.; Shah, P.L.; Fiss, E.; Olivenstein, R.; Thomson, N.C.; Niven, R.M.; et al. Effectiveness and safety of bronchial thermoplasty in the treatment of severe asthma: A multicenter, randomized, double-blind, sham-controlled clinical trial. Am. J. Respir. Crit. Care Med. 2010, 2, 116–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goorsenberg, A.W.; d’Hooghe, J.N.; Srikanthan, K.; Ten Hacken, N.H.; Weersink, E.J.; Roelofs, J.J.; Kemp, S.V.; Bel, E.H.; Shah, P.L.; Annema, J.T.; et al. Bronchial Thermoplasty Induced Airway Smooth Muscle Reduction and Clinical Response in Severe Asthma. The TASMA Randomized Trial. Am. J. Respir. Crit. Care Med. 2021, 2, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Vaselli, M.; Wijsman, P.C.; Willemse, J.; Goorsenberg, A.W.; Feroldi, F.; d’Hooghe, J.N.; Annema, J.T.; de Boer, J.F.; Bonta, P.I. Polarization Sensitive Optical Coherence Tomography for Bronchoscopic Airway Smooth Muscle Detection in Bronchial Thermoplasty-Treated Patients with Asthma. Chest 2021, 2, 432–435. [Google Scholar] [CrossRef]
- Chaudhuri, R.; Rubin, A.; Sumino, K.; e Silva, J.R.; Niven, R.; Siddiqui, S.; Klooster, K.; McEvoy, C.; Shah, P.L.; Simoff, M.; et al. Safety and effectiveness of bronchial thermoplasty after 10 years in patients with persistent asthma (BT10+): A follow-up of three randomised controlled trials. Lancet Respir. Med. 2021, 5, 457–466. [Google Scholar] [CrossRef]
- Nair, P.; Gaga, M.; Zervas, E.; Alagha, K.; Hargreave, F.E.; O’byrne, P.M.; Stryszak, P.; Gann, L.; Sadeh, J.; Chanez, P.; et al. Safety and efficacy of a CXCR2 antagonist in patients with severe asthma and sputum neutrophils: A randomized, placebo-controlled clinical trial. Clin. Exp. Allergy 2012, 7, 1097–1103. [Google Scholar] [CrossRef]
- O’Byrne, P.M.; Metev, H.; Puu, M.; Richter, K.; Keen, C.; Uddin, M.; Larsson, B.; Cullberg, M.; Nair, P. Efficacy and safety of a CXCR2 antagonist, AZD5069, in patients with uncontrolled persistent asthma: A randomised, double-blind, placebo-controlled trial. Lancet Respir. Med. 2016, 10, 797–806. [Google Scholar] [CrossRef]
- Mitchell, P.D.; O’Byrne, P.M. Epithelial-Derived Cytokines in Asthma. Chest 2017, 6, 1338–1344. [Google Scholar] [CrossRef]
- Porsbjerg, C.M.; Sverrild, A.; Lloyd, C.M.; Menzies-Gow, A.N.; Bel, E.H. Anti-alarmins in asthma: Targeting the airway epithelium with next-generation biologics. Eur. Respir. J. 2020, 56, 2000260. [Google Scholar] [CrossRef]
- Corren, J.; Parnes, J.R.; Wang, L.; Mo, M.; Roseti, S.L.; Griffiths, J.M.; van der Merwe, R. Tezepelumab in Adults with Uncontrolled Asthma. N. Engl. J. Med. 2017, 10, 936–946. [Google Scholar] [CrossRef]
- Menzies-Gow, A.; Corren, J.; Bourdin, A.; Chupp, G.; Israel, E.; Wechsler, M.E.; Brightling, C.E.; Griffiths, J.M.; Hellqvist, Å.; Bowen, K.; et al. Tezepelumab in Adults and Adolescents with Severe, Uncontrolled Asthma. N. Engl. J. Med. 2021, 19, 1800–1809. [Google Scholar] [CrossRef] [PubMed]
- Busse, W.W.; Holgate, S.; Kerwin, E.; Chon, Y.; Feng, J.; Lin, J.; Lin, S.L. Randomized, double-blind, placebo-controlled study of brodalumab, a human anti-IL-17 receptor monoclonal antibody, in moderate to severe asthma. Am. J. Respir. Crit. Care Med. 2013, 11, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Novartis Pharmaceuticals. Study to Assess the Efficacy and Safety of CJM112 in Patients with Inadequately Controlled Severe Asthma. Available online: https://clinicaltrials.gov/ct2/show/NCT03299686/ (accessed on 8 October 2021).
- Shaw, D.E.; Sousa, A.R.; Fowler, S.J.; Fleming, L.J.; Roberts, G.; Corfield, J.; Pandis, I.; Bansal, A.T.; Bel, E.H.; Auffray, C.; et al. Clinical and inflammatory characteristics of the European U-BIOPRED adult severe asthma cohort. Eur. Respir. J. 2015, 46, 1308–1321. [Google Scholar] [CrossRef] [Green Version]
- Heaney, L.G.; Djukanovic, R.; Woodcock, A.; Walker, S.; Matthews, J.G.; Pavord, I.D.; Bradding, P.; Niven, R.; Brightling, C.E.; Chaudhuri, R.; et al. Research in progress: Medical Research Council United Kingdom Refractory Asthma Stratification Programme (RASP-UK). Thorax 2016, 2, 187–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papaioannou, A.I.; Fouka, E.; Ntontsi, P.; Stratakos, G.; Papiris, S. Paucigranulocytic Asthma: Potential Pathogenetic Mechanisms, Clinical Features and Therapeutic Management. J. Pers. Med. 2022, 12, 850. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050850
Papaioannou AI, Fouka E, Ntontsi P, Stratakos G, Papiris S. Paucigranulocytic Asthma: Potential Pathogenetic Mechanisms, Clinical Features and Therapeutic Management. Journal of Personalized Medicine. 2022; 12(5):850. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050850
Chicago/Turabian StylePapaioannou, Andriana I., Evangelia Fouka, Polyxeni Ntontsi, Grigoris Stratakos, and Spyridon Papiris. 2022. "Paucigranulocytic Asthma: Potential Pathogenetic Mechanisms, Clinical Features and Therapeutic Management" Journal of Personalized Medicine 12, no. 5: 850. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050850