
Distinct Phenotypes of Kidney Transplant Recipients in the United States with Limited Functional Status as Identified through Machine Learning Consensus Clustering

 ,
,  , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Methods
2.1. Data Source and Study Population
2.2. Data Collection
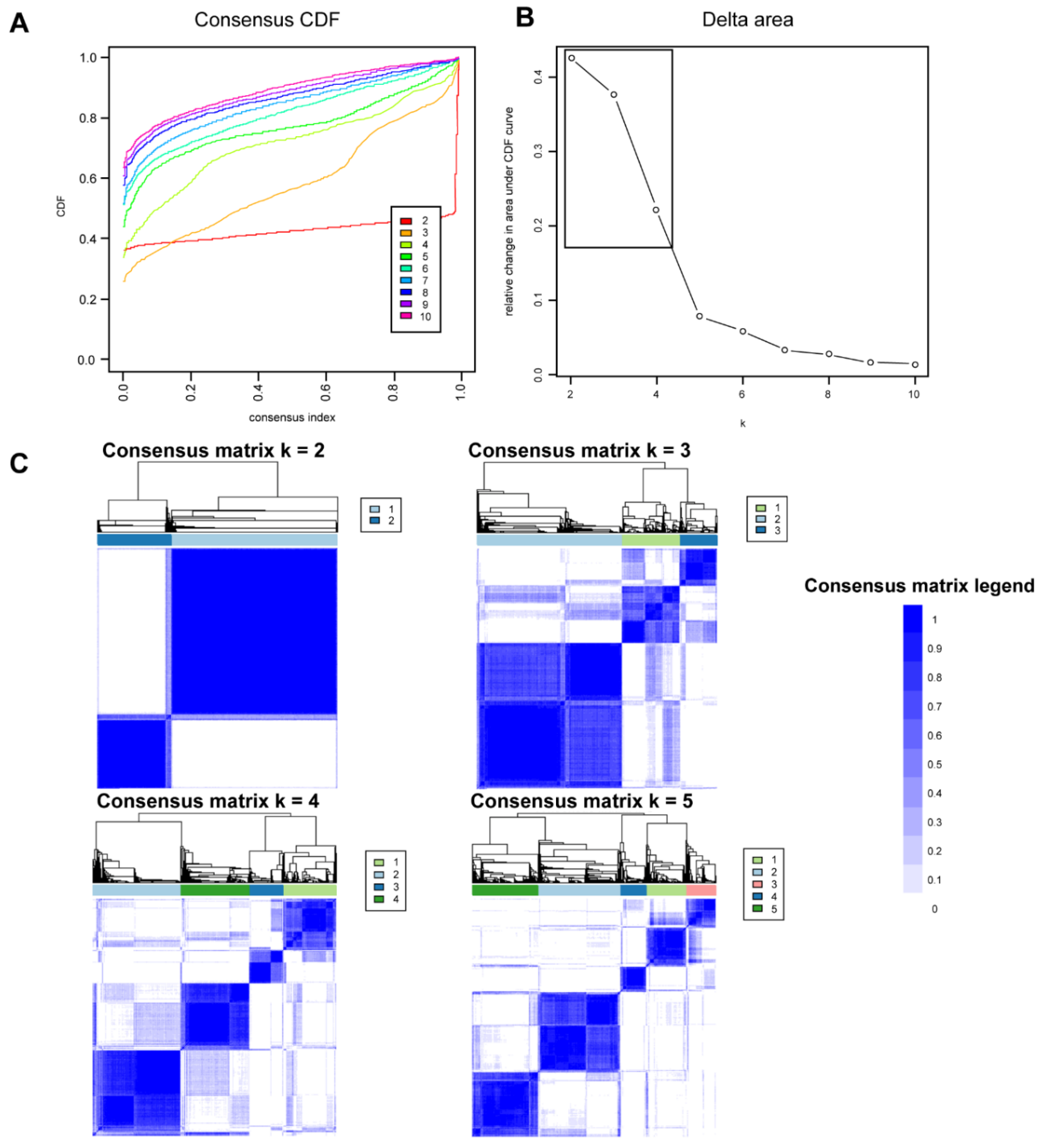
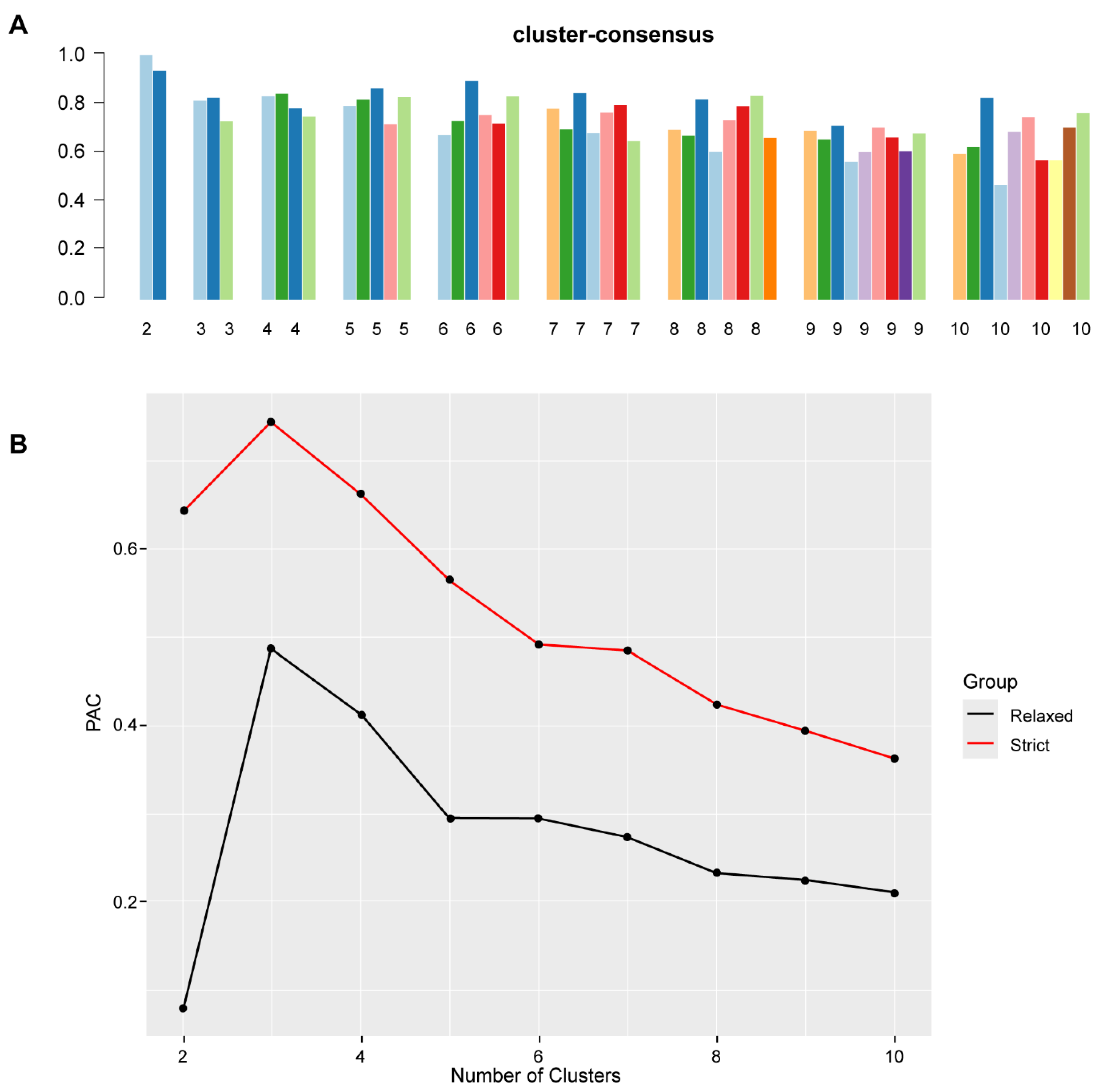
2.3. Clustering Analysis
Outcomes
2.4. Statistical Analysis
3. Results
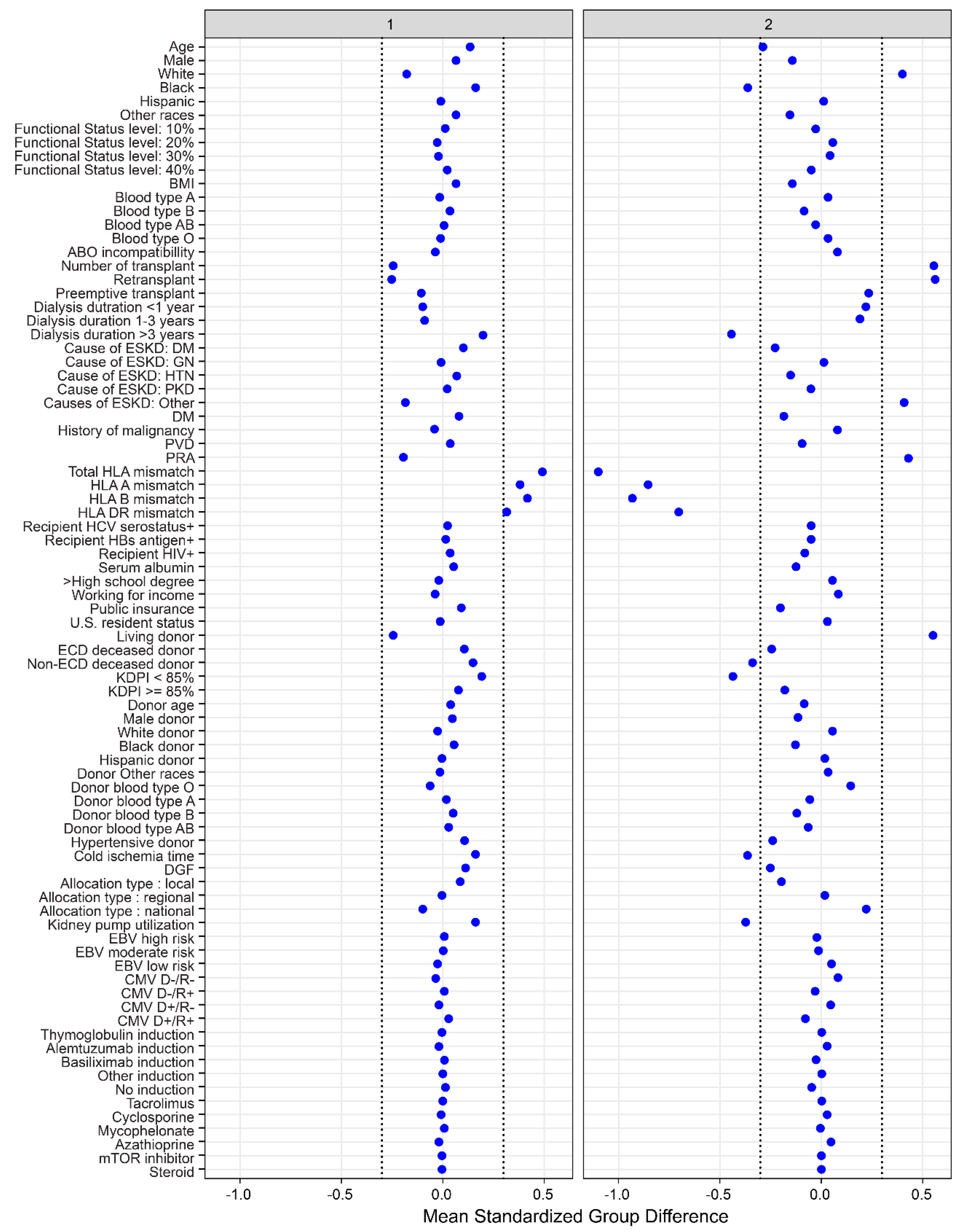
3.1. Clinical Characteristics of Each Functionally Impaired Kidney Transplant Clusters
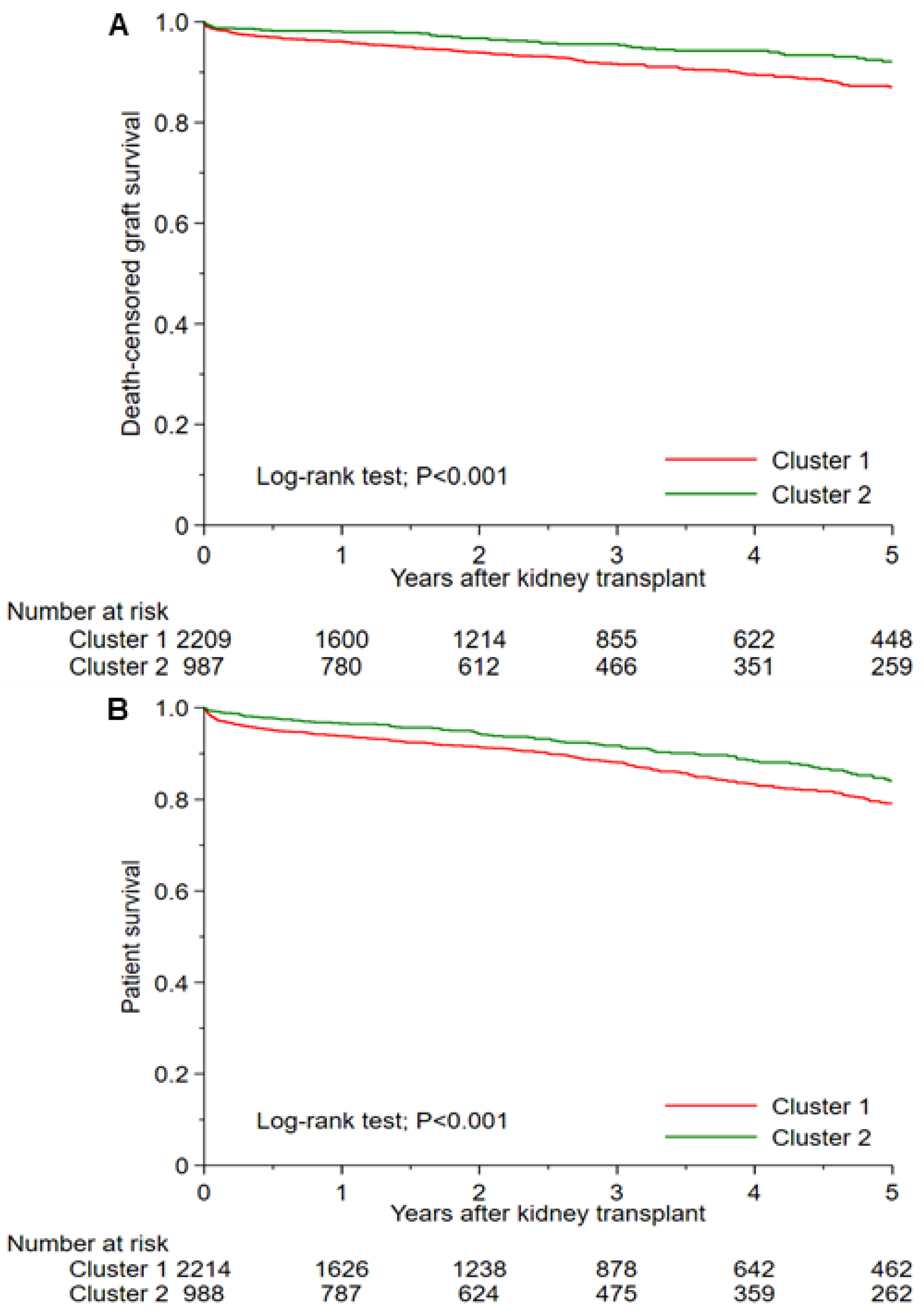
3.2. Posttransplant Outcomes of Each Functionally Disabled Kidney Transplant Cluster
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reese, P.P.; Bloom, R.D.; Shults, J.; Thomasson, A.; Mussell, A.; Rosas, S.E.; Johansen, K.L.; Abt, P.; Levine, M.; Caplan, A.; et al. Functional status and survival after kidney transplantation. Transplantation 2014, 97, 189–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutner, N.G.; Zhang, R.; Bowles, T.; Painter, P. Pretransplant physical functioning and kidney patients’ risk for posttransplantation hospitalization/death: Evidence from a national cohort. Clin. J. Am. Soc. Nephrol. 2006, 1, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Alhamad, T.; Cheungpasitporn, W.; Tan, J.C.; Chang, S.H.; Cooper, M.; Dadhania, D.M.; Axelrod, D.A.; Schnitzler, M.A.; Ouseph, R.; et al. Impact of Functional Status on Outcomes of Simultaneous Pancreas-kidney Transplantation: Risks and Opportunities for Patient Benefit. Transplant. Direct 2020, 6, e599. [Google Scholar] [CrossRef] [PubMed]
- Chu, N.M.; Chen, X.; Bae, S.; Brennan, D.C.; Segev, D.L.; McAdams-DeMarco, M.A. Changes in Functional Status Among Kidney Transplant Recipients: Data From the Scientific Registry of Transplant Recipients. Transplantation 2021, 105, 2104–2111. [Google Scholar] [CrossRef]
- Garonzik-Wang, J.M.; Govindan, P.; Grinnan, J.W.; Liu, M.; Ali, H.M.; Chakraborty, A.; Jain, V.; Ros, R.L.; James, N.T.; Kucirka, L.M.; et al. Frailty and delayed graft function in kidney transplant recipients. Arch. Surg. 2012, 147, 190–193. [Google Scholar] [CrossRef]
- Kobashigawa, J.; Dadhania, D.; Bhorade, S.; Adey, D.; Berger, J.; Bhat, G.; Budev, M.; Duarte-Rojo, A.; Dunn, M.; Hall, S.; et al. Report from the American Society of Transplantation on frailty in solid organ transplantation. Am. J. Transplant. 2019, 19, 984–994. [Google Scholar] [CrossRef]
- McAdams-DeMarco, M.A.; Law, A.; King, E.; Orandi, B.; Salter, M.; Gupta, N.; Chow, E.; Alachkar, N.; Desai, N.; Varadhan, R.; et al. Frailty and mortality in kidney transplant recipients. Am. J. Transplant. 2015, 15, 149–154. [Google Scholar] [CrossRef] [Green Version]
- McAdams-DeMarco, M.A.; Law, A.; Salter, M.L.; Chow, E.; Grams, M.; Walston, J.; Segev, D.L. Frailty and early hospital readmission after kidney transplantation. Am. J. Transplant. 2013, 13, 2091–2095. [Google Scholar] [CrossRef] [Green Version]
- McAdams-DeMarco, M.A.; Law, A.; Tan, J.; Delp, C.; King, E.A.; Orandi, B.; Salter, M.; Alachkar, N.; Desai, N.; Grams, M.; et al. Frailty, mycophenolate reduction, and graft loss in kidney transplant recipients. Transplantation 2015, 99, 805–810. [Google Scholar] [CrossRef] [Green Version]
- Karnofsky, D.A. The clinical evaluation of chemotherapeutic agents in cancer. Eval. Chemother. Agents 1949, 191–205. [Google Scholar]
- Bui, K.; Kilambi, V.; Rodrigue, J.R.; Mehrotra, S. Patient Functional Status at Transplant and Its Impact on Posttransplant Survival of Adult Deceased-donor Kidney Recipients. Transplantation 2019, 103, 1051–1063. [Google Scholar] [CrossRef] [PubMed]
- McAdams-DeMarco, M.A.; Van Pilsum Rasmussen, S.E.; Chu, N.M.; Agoons, D.; Parsons, R.F.; Alhamad, T.; Johansen, K.L.; Tullius, S.G.; Lynch, R.; Harhay, M.N.; et al. Perceptions and Practices Regarding Frailty in Kidney Transplantation: Results of a National Survey. Transplantation 2020, 104, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Mor, V.; Laliberte, L.; Morris, J.N.; Wiemann, M. The Karnofsky Performance Status Scale. An examination of its reliability and validity in a research setting. Cancer 1984, 53, 2002–2007. [Google Scholar] [CrossRef]
- UNOS Transplant Candidate Registration—Kidney. Available online: https://unos.org/wp-content/uploads/Adult-TCR-Kidney.pdf (accessed on 4 December 2021).
- Reese, P.P.; Shults, J.; Bloom, R.D.; Mussell, A.; Harhay, M.N.; Abt, P.; Levine, M.; Johansen, K.L.; Karlawish, J.T.; Feldman, H.I. Functional status, time to transplantation, and survival benefit of kidney transplantation among wait-listed candidates. Am. J. Kidney Dis. 2015, 66, 837–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veasey, T.M.; Fleming, J.N.; Strout, S.E.; Miller, R.; Pilch, N.A.; Meadows, H.B.; Mardis, C.R.; Mardis, B.A.; Shenvi, S.; McGillicuddy, J.; et al. Morbid obesity and functional status as predictors of surgical complication after renal transplantation. Am. J. Surg. 2018, 215, 663–668. [Google Scholar] [CrossRef]
- Bardonnaud, N.; Pillot, P.; Lillaz, J.; Delorme, G.; Chabannes, E.; Bernardini, S.; Guichard, G.; Bittard, H.; Kleinclauss, F. Outcomes of renal transplantation in obese recipients. Transplant. Proc. 2012, 44, 2787–2791. [Google Scholar] [CrossRef] [PubMed]
- Kampaktsis, P.N.; Tzani, A.; Doulamis, I.P.; Moustakidis, S.; Drosou, A.; Diakos, N.; Drakos, S.G.; Briasoulis, A. State-of-the-art machine learning algorithms for the prediction of outcomes after contemporary heart transplantation: Results from the UNOS database. Clin. Transplant. 2021, 35, e14388. [Google Scholar] [CrossRef]
- Killian, M.O.; Payrovnaziri, S.N.; Gupta, D.; Desai, D.; He, Z. Machine learning-based prediction of health outcomes in pediatric organ transplantation recipients. JAMIA Open 2021, 4, ooab008. [Google Scholar] [CrossRef]
- Ershoff, B.D.; Lee, C.K.; Wray, C.L.; Agopian, V.G.; Urban, G.; Baldi, P.; Cannesson, M. Training and Validation of Deep Neural Networks for the Prediction of 90-Day Post-Liver Transplant Mortality Using UNOS Registry Data. Transplant. Proc. 2020, 52, 246–258. [Google Scholar] [CrossRef]
- Wadhwani, S.I.; Hsu, E.K.; Shaffer, M.L.; Anand, R.; Ng, V.L.; Bucuvalas, J.C. Predicting ideal outcome after pediatric liver transplantation: An exploratory study using machine learning analyses to leverage Studies of Pediatric Liver Transplantation Data. Pediatric Transplant. 2019, 23, e13554. [Google Scholar] [CrossRef]
- Schwantes, I.R.; Axelrod, D.A. Technology-Enabled Care and Artificial Intelligence in Kidney Transplantation. Curr. Transplant. Rep. 2021, 8, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Connor, K.L.; O’Sullivan, E.D.; Marson, L.P.; Wigmore, S.J.; Harrison, E.M. The Future Role of Machine Learning in Clinical Transplantation. Transplantation 2021, 105, 723–735. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Vaitla, P.; Jadlowiec, C.C.; Leeaphorn, N.; Mao, S.A.; Mao, M.A.; Pattharanitima, P.; Bruminhent, J.; Khoury, N.J.; Garovic, V.D.; et al. Use of Machine Learning Consensus Clustering to Identify Distinct Subtypes of Black Kidney Transplant Recipients and Associated Outcomes. JAMA Surg. 2022, e221286. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Mao, M.A.; Kattah, A.G.; Keddis, M.T.; Pattharanitima, P.; Erickson, S.B.; Dillon, J.J.; Garovic, V.D.; Cheungpasitporn, W. Subtyping hospitalized patients with hypokalemia by machine learning consensus clustering and associated mortality risks. Clin. Kidney J. 2022, 15, 253–261. [Google Scholar] [CrossRef]
- MacEachern, S.J.; Forkert, N.D. Machine learning for precision medicine. Genome 2021, 64, 416–425. [Google Scholar] [CrossRef]
- Alyousef, A.A.; Nihtyanova, S.; Denton, C.; Bosoni, P.; Bellazzi, R.; Tucker, A. Nearest Consensus Clustering Classification to Identify Subclasses and Predict Disease. J. Healthc. Inform. Res. 2018, 2, 402–422. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Z.; Waikar, S.S.; Schmidt, I.M.; Landis, J.R.; Hsu, C.Y.; Shafi, T.; Feldman, H.I.; Anderson, A.H.; Wilson, F.P.; Chen, J.; et al. Subtyping CKD Patients by Consensus Clustering: The Chronic Renal Insufficiency Cohort (CRIC) Study. J. Am. Soc. Nephrol. 2021, 32, 639–653. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Kattah, A.G.; Mao, M.A.; Keddis, M.T.; Pattharanitima, P.; Vallabhajosyula, S.; Nissaisorakarn, V.; Erickson, S.B.; Dillon, J.J.; Garovic, V.D.; et al. Distinct Phenotypes of Hospitalized Patients with Hyperkalemia by Machine Learning Consensus Clustering and Associated Mortality Risks. QJM—Int. J. Med. 2021, hcab194. [Google Scholar] [CrossRef]
- Van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Monti, S.; Tamayo, P.; Mesirov, J.; Golub, T. Consensus clustering: A resampling-based method for class discovery and visualization of gene expression microarray data. Mach. Learn. 2003, 52, 91–118. [Google Scholar] [CrossRef]
- Wilkerson, M.D.; Hayes, D.N. ConsensusClusterPlus: A class discovery tool with confidence assessments and item tracking. Bioinformatics 2010, 26, 1572–1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Șenbabaoğlu, Y.; Michailidis, G.; Li, J.Z. Critical limitations of consensus clustering in class discovery. Sci. Rep. 2014, 4, 6207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, B.J.; Dahhou, M.; Zhang, X.; Platt, R.W.; Smith, J.M.; Hanley, J.A. Impact of HLA mismatch at first kidney transplant on lifetime with graft function in young recipients. Am. J. Transplant. 2014, 14, 876–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez, D.; Vazquez, T.; Alonso-Titos, J.; Leon, M.; Caballero, A.; Cobo, M.A.; Sola, E.; Lopez, V.; Ruiz-Esteban, P.; Cruzado, J.M.; et al. Impact of HLA Mismatching on Early Subclinical Inflammation in Low-Immunological-Risk Kidney Transplant Recipients. J. Clin. Med. 2021, 10, 1934. [Google Scholar] [CrossRef]
- Mjoen, G.; Reisaeter, A.V.; Dahle, D.O. HLA Mismatch and Allograft Survival. Transplantation 2016, 100, e52. [Google Scholar] [CrossRef]
- Kouwenhoven, E.A.; de Bruin, R.W.; Bajema, I.M.; Marquet, R.L.; Ijzermans, J.N. Cold ischemia augments allogeneic-mediated injury in rat kidney allografts. Kidney Int. 2001, 59, 1142–1148. [Google Scholar] [CrossRef] [Green Version]
- Mikhalski, D.; Wissing, K.M.; Ghisdal, L.; Broeders, N.; Touly, M.; Hoang, A.D.; Loi, P.; Mboti, F.; Donckier, V.; Vereerstraeten, P.; et al. Cold ischemia is a major determinant of acute rejection and renal graft survival in the modern era of immunosuppression. Transplantation 2008, 85, S3–S9. [Google Scholar] [CrossRef]
- Bryan, C.F.; Luger, A.M.; Martinez, J.; Muruve, N.; Nelson, P.W.; Pierce, G.E.; Ross, G.; Shield, C.F., III; Warady, B.A.; Aeder, M.I.; et al. Cold ischemia time: An independent predictor of increased HLA class I antibody production after rejection of a primary cadaveric renal allograft. Transplantation 2001, 71, 875–879. [Google Scholar] [CrossRef]
- Sert, I.; Colak, H.; Tugmen, C.; Dogan, S.M.; Karaca, C. The effect of cold ischemia time on delayed graft function and acute rejection in kidney transplantation. Saudi J. Kidney Dis. Transplant. 2014, 25, 960–966. [Google Scholar] [CrossRef]
- McAdams-DeMarco, M.A.; Isaacs, K.; Darko, L.; Salter, M.L.; Gupta, N.; King, E.A.; Walston, J.; Segev, D.L. Changes in Frailty After Kidney Transplantation. J. Am. Geriatr. Soc. 2015, 63, 2152–2157. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 3205) | Cluster 1 (n = 2216) | Cluster 2 (n = 989) | p-Value | |
|---|---|---|---|---|
| Recipient Age (year) | 51.0 ± 13.4 | 52.8 ± 12.7 | 47.2 ± 14.2 | <0.001 |
| Recipient male sex | 1957 (61) | 1422 (64) | 535 (54) | <0.001 |
| Recipient race | <0.001 | |||
| 1521 (48) | 854 (39) | 667 (67) | |
| 935 (29) | 807 (36) | 128 (13) | |
| 446 (14) | 302 (14) | 144 (15) | |
| 303 (9) | 253 (11) | 50 (5) | |
| ABO blood group | 0.02 | |||
| 1176 (37) | 798 (36) | 378 (38) | |
| 432 (13) | 325 (15) | 107 (11) | |
| 170 (5) | 123 (5) | 47 (5) | |
| 1427 (45) | 970 (44) | 457 (46) | |
| Body mass index (kg/m2) | 28.4 ± 5.8 | 28.7 ± 5.7 | 27.5 ± 5.9 | <0.001 |
| Kidney retransplant | 392 (12) | 89 (4) | 303 (31) | <0.001 |
| Dialysis duration | <0.001 | |||
| 275 (9) | 124 (6) | 151 (15) | |
| 331 (10) | 162 (7) | 169 (17) | |
| 1860 (58) | 1500 (68) | 360 (36) | |
| 739 (23) | 430 (19) | 309 (31) | |
| Cause of end-stage kidney disease | <0.001 | |||
| 1018 (32) | 809 (36) | 209 (21) | |
| 643 (20) | 506 (23) | 137 (14) | |
| 585 (18) | 399 (18) | 186 (19) | |
| 192 (6.0) | 145 (7) | 47 (5) | |
| 767 (24) | 357 (16) | 410 (41) | |
| Comorbidity | ||||
| 1258 (39) | 958 (43) | 300 (30) | <0.001 |
| 285 (9) | 174 (8) | 111 (11) | 0.002 |
| 485 (15) | 368 (17) | 117 (12) | <0.001 |
| PRA (%), median (Q25, Q75) | 0 (0, 41) | 0 (0, 17) | 15 (0, 88) | <0.001 |
| Positive HCV serostatus | 158 (5) | 120 (5) | 38 (4) | 0.06 |
| Positive HBs antigen | 68 (2) | 53 (2) | 15 (2) | 0.11 |
| Positive HIV serostatus | 27 (1) | 26 (1) | 1 (0) | 0.002 |
| Functional status | 0.04 | |||
| 94 (3) | 69 (3) | 25 (2) | |
| 92 (3) | 54 (3) | 38 (4) | |
| 122 (4) | 76 (3) | 46 (5) | |
| 2897 (90) | 2017 (91) | 880 (89) | |
| Working income | 267 (8) | 161 (7) | 106 (11) | 0.001 |
| Public insurance | 2641 (82) | 1902 (86) | 739 (75) | <0.001 |
| US resident | 3192 (99) | 2205 (99) | 987 (99) | 0.23 |
| Undergraduate education or above | 1433 (45) | 965 (43) | 468 (47) | 0.04 |
| Serum albumin (g/dL) | 3.8 ± 0.6 | 3.8 ± 0.6 | 3.7 ± 0.6 | <0.001 |
| Kidney donor status | <0.001 | |||
| 2067 (64) | 1587 (72) | 480 (49) | |
| 373 (12) | 334 (15) | 39 (4) | |
| 765 (24) | 295 (13) | 470 (47) | |
| ABO incompatibility | 5 (0) | 0 (0) | 5 (1) | 0.003 |
| Donor age (year) | 39.8 ± 15.1 | 40.3 ± 15.5 | 38.6 ± 14.0 | 0.004 |
| Donor male sex | 1753 (55) | 1265 (57) | 488 (49) | <0.001 |
| Donor race | <0.001 | |||
| 2289 (71) | 1555 (70) | 734 (74) | |
| 419 (13) | 330 (15) | 89 (9) | |
| 382 (12) | 258 (12) | 124 (13) | |
| 115 (4) | 73 (3) | 42 (4) | |
| History of hypertension in donor | 710 (22) | 588 (27) | 122 (12) | <0.001 |
| KDPI | <0.001 | |||
| 765 (24) | 295 (13) | 470 (48) | |
| 2267 (71) | 1762 (80) | 505 (51) | |
| 173 (5) | 159 (7) | 14 (1) | |
| HLA mismatch, median (Q25, Q75) | 4 (3, 5) | 5 (4, 5) | 2 (1, 3) | <0.001 |
| Cold ischemia time (hours) | 13.8 ± 9.8 | 15.3 ± 9.5 | 10.3 ± 9.5 | <0.001 |
| Kidney on pump | 1271 (40) | 1059 (48) | 212 (21) | <0.001 |
| Delay graft function | 742 (23) | 616 (28) | 126 (13) | <0.001 |
| Allocation type | <0.001 | |||
| 2703 (84) | 1937 (87) | 766 (77) | |
| 226 (7) | 150 (7) | 76 (8) | |
| 276 (9) | 129 (6) | 147 (15) | |
| EBV status | 0.08 | |||
| 79 (3) | 46 (2) | 33 (3) | |
| 2782 (87) | 1926 (87) | 856 (87) | |
| 344 (11) | 244 (11) | 100 (10) | |
| CMV status | 0.001 | |||
| 540 (17) | 342 (15) | 198 (20) | |
| 863 (27) | 608 (27) | 255 (26) | |
| 1251 (39) | 903 (41) | 348 (35) | |
| 551 (17) | 363 (16) | 188 (19) | |
| Induction immunosuppression | ||||
| 1893 (59) | 1306 (59) | 587 (59) | 0.82 |
| 346 (11) | 230 (10) | 116 (12) | 0.26 |
| 631 (20) | 446 (20) | 185 (19) | 0.35 |
| 82 (3) | 56 (3) | 26 (3) | 0.87 |
| 326 (10) | 238 (11) | 88 (9) | 0.11 |
| Maintenance Immunosuppression | ||||
| 2967 (93) | 2050 (93) | 917 (93) | 0.83 |
| 38 (1) | 23 (1) | 15 (2) | 0.25 |
| 2909 (91) | 2012 (91) | 897 (91) | 0.93 |
| 25 (1) | 13 (1) | 12 (1) | 0.06 |
| 18 (1) | 12 (1) | 6 (1) | 0.82 |
| 1987 (62) | 1372 (62) | 615 (62) | 0.88 |
| Cluster 1 | Cluster 2 | |
|---|---|---|
| 1-year death-censored graft failure | 4.1% | 2.1% |
| HR for 1-year death-censored graft failure | 1.92 (1.21–3.22) | 1 (ref) |
| 5-year death-censored graft failure | 13.1% | 8.1% |
| HR for 5-year death-censored graft failure | 1.75 (1.28–2.40) | 1 (ref) |
| 1-year death | 6.3% | 3.5% |
| HR for 1-year death | 1.82 (1.26–2.72) | 1 (ref) |
| 5-year death | 20.9% | 16.1% |
| HR for 5-year death | 1.45 (1.15–1.82) | 1 (ref) |
| 1-year acute rejection | 6.7% | 3.8% |
| OR for 1-year acute rejection | 1.80 (1.25–2.60) | 1 (ref) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongprayoon, C.; Jadlowiec, C.C.; Kaewput, W.; Vaitla, P.; Mao, S.A.; Mao, M.A.; Leeaphorn, N.; Qureshi, F.; Pattharanitima, P.; Qureshi, F.; et al. Distinct Phenotypes of Kidney Transplant Recipients in the United States with Limited Functional Status as Identified through Machine Learning Consensus Clustering. J. Pers. Med. 2022, 12, 859. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12060859
Thongprayoon C, Jadlowiec CC, Kaewput W, Vaitla P, Mao SA, Mao MA, Leeaphorn N, Qureshi F, Pattharanitima P, Qureshi F, et al. Distinct Phenotypes of Kidney Transplant Recipients in the United States with Limited Functional Status as Identified through Machine Learning Consensus Clustering. Journal of Personalized Medicine. 2022; 12(6):859. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12060859
Chicago/Turabian StyleThongprayoon, Charat, Caroline C. Jadlowiec, Wisit Kaewput, Pradeep Vaitla, Shennen A. Mao, Michael A. Mao, Napat Leeaphorn, Fawad Qureshi, Pattharawin Pattharanitima, Fahad Qureshi, and et al. 2022. "Distinct Phenotypes of Kidney Transplant Recipients in the United States with Limited Functional Status as Identified through Machine Learning Consensus Clustering" Journal of Personalized Medicine 12, no. 6: 859. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12060859