
The Cut-Off Value for Classifying Active Italian Children Using the Corresponding National Version of the Physical Activity Questionnaire

 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.2.1. Anthropometric Parameters
2.2.2. Triaxial Accelerometry
2.2.3. Physical Activity Questionnaire for Older Children (PAQ-C-It)
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Biddle, S.J.H.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, L.B.; Riddoch, C.; Kriemler, S.; Hills, A.P. Physical activity and cardiovascular risk factors in children. Br. J. Sports Med. 2011, 45, 871–876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Must, A.; Tybor, D.J. Physical activity and sedentary behavior: A review of longitudinal studies of weight and adiposity in youth. Int. J. Obes. 2005, 29, S84–S96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rey-López, J.P.; Vicente-Rodríguez, G.; Biosca, M.; Moreno, L.A. Sedentary behaviour and obesity development in children and adolescents. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Sheikholeslami, S.; Ghanbarian, A.; Azizi, F. The Impact of Physical Activity on Non-Communicable Diseases: Findings from 20 Years of the Tehran Lipid and Glucose Study. Int. J. Endocrinol. Metab. 2018, 16, e84740. [Google Scholar] [PubMed] [Green Version]
- World Health Organization WHO. Guidelines on Physical Activity and Sedentary Behaviour: Web Annex Evidence Profiles. Available online: https://apps.who.int/iris/bitstream/handle/10665/336656/9789240015128-eng.pdf (accessed on 16 November 2021).
- Colley, R.C.; Garriguet, D.; Adamo, K.B.; Carson, V.; Janssen, I.; Timmons, B.W.; Tremblay, M.S. Physical activity and sedentary behavior during the early years in Canada: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 54–59. [Google Scholar] [CrossRef] [Green Version]
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.-P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Gorber, S.C.; et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: An update. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265. [Google Scholar] [CrossRef]
- Konstabel, K.; Veidebaum, T.; Verbestel, V.; Moreno, L.A.; Bammann, K.; Tornaritis, M.; Eiben, G.; Molnár, D.; Siani, A.; Sprengeler, O.; et al. Objectively measured physical activity in European children: The IDEFICS study. Int. J. Obes. 2014, 38, S135–S143. [Google Scholar] [CrossRef] [Green Version]
- Brustio, P.R.; Moisè, P.; Marasso, D.; Alossa, D.; Miglio, F.; Mulasso, A.; Rabaglietti, E.; Rainoldi, A.; Boccia, G. Participation in a school-based walking intervention changes the motivation to undertake physical activity in middle-school students. PLoS ONE 2018, 13, e0204098. [Google Scholar] [CrossRef] [Green Version]
- Brustio, P.R.; Moisè, P.; Marasso, D.; Miglio, F.; Rainoldi, A.; Boccia, G. Feasibility of implementing an outdoor walking break in Italian middle schools. PLoS ONE 2018, 13, e0202091. [Google Scholar] [CrossRef]
- Brustio, P.R.; Mulasso, A.; Marasso, D.; Ruffa, C.; Ballatore, A.; Moisè, P.; Lupo, C.; Rainoldi, A.; Boccia, G. The Daily Mile: 15 Minutes Running Improves the Physical Fitness of Italian Primary School Children. Int. J. Environ. Res. Public Health 2019, 16, 3921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brustio, P.R.; Mulasso, A.; Lupo, C.; Massasso, A.; Rainoldi, A.; Boccia, G. The Daily Mile Is Able to Improve Cardiorespiratory Fitness When Practiced Three Times a Week. Int. J. Environ. Res. Public Health 2020, 17, 2095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marasso, D.; Lupo, C.; Collura, S.; Rainoldi, A.; Brustio, P.R. Subjective versus Objective Measure of Physical Activity: A Systematic Review and Meta-Analysis of the Convergent Validity of the Physical Activity Questionnaire for Children (PAQ-C). Int. J. Environ. Res. Public Health 2021, 18, 3413. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, N.; Welsman, J.R. The Physical Activity Patterns of European Youth with Reference to Methods of Assessment. Sports Med. 2006, 36, 1067–1086. [Google Scholar] [CrossRef]
- Ekelund, U.; Sjöström, M.; Yngve, A.; Poortvliet, E.; Nilsson, A.; Froberg, K.; Wedderkopp, N.; Westerterp, K. Physical activity assessed by activity monitor and doubly labeled water in children. Med. Sci. Sports Exerc. 2001, 33, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Slootmaker, S.M.; Paw, M.J.M.C.A.; Schuit, A.J.; Van Mechelen, W.; Koppes, L.L.J. Concurrent validity of the PAM accelerometer relative to the MTI Actigraph using oxygen consumption as a reference. Scand. J. Med. Sci. Sports 2009, 19, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Hendelman, D.; Miller, K.; Baggett, C.; DeBold, E.; Freedson, P. Validity of accelerometry for the assessment of moderate intensity physical activity in the field. Med. Sci. Sports Exerc. 2000, 32, S442–S449. [Google Scholar] [CrossRef] [Green Version]
- Welk, G.J.; Blair, S.N.; Wood, K.; Jones, S.; Thompson, R.W. A comparative evaluation of three accelerometry-based physical activity monitors. Med. Sci. Sports Exerc. 2000, 32, S489–S497. [Google Scholar] [CrossRef]
- Chinapaw, M.J.M.; Mokkink, L.B.; Van Poppel, M.N.M.; Van Mechelen, W.; Terwee, C.B. Physical Activity Questionnaires for Youth: A Systematic Review of Measurement Properties. Sport. Med. 2010, 40, 2317–2346. [Google Scholar] [CrossRef]
- Janz, K.F.; Lutuchy, E.M.; Wenthe, P.; Levy, S.M. Measuring Activity in Children and Adolescents Using Self-Report: PAQ-C and PAQ-A. Med. Sci. Sports Exerc. 2008, 40, 767–772. [Google Scholar] [CrossRef]
- Crocker, P.R.E.; Bailey, D.A.; Faulkner, R.A.; Kowalski, K.C.; McGRATH, R. Measuring general levels of physical activity: Preliminary evidence for the Physical Activity Questionnaire for Older Children. Med. Sci. Sports Exerc. 1997, 29, 1344–1349. [Google Scholar] [CrossRef] [PubMed]
- Sabia, S.; Van Hees, V.T.; Shipley, M.J.; Trenell, M.; Hagger-Johnson, G.; Elbaz, A.; Kivimaki, M.; Singh-Manoux, A. Association Between Questionnaire- and Accelerometer-Assessed Physical Activity: The Role of Sociodemographic Factors. Am. J. Epidemiol. 2014, 179, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Venetsanou, F.; Emmanouilidou, K.; Soutos, K.; Sotiriou, S.A.; Bastida, L.; Moya, A.; Kambas, A. Towards a Functional Approach to the Assessment of Daily Life Physical Activity in Children: Are the PAQ-C and Fitbit Flex-2 Technically Adequate? Int. J. Environ. Res. Public Health 2020, 17, 8503. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, E.; Elliot, C.; Varnier, M.; Carraro, A. Psychometric Properties of the Physical Activity Questionnaire for Older Children in Italy: Testing the Validity among a General and Clinical Pediatric Population. PLoS ONE 2016, 11, e0156354. [Google Scholar] [CrossRef]
- Voss, C.; Harris, K.C. Physical activity evaluation in children with congenital heart disease. Heart 2017, 103, 1408–1412. [Google Scholar] [CrossRef]
- Wang, J.J.; Baranowski, T.; Lau, W.P.; Chen, T.A.; Pitkethly, A.J. Validation of the Physical Activity Questionnaire for Older Children (PAQ-C) among Chinese Children. Biomed. Environ. Sci. 2016, 29, 163–164. [Google Scholar] [CrossRef]
- Wang, J.-J.; Baranowski, T.; Lau, P.W.C.; Chen, T.-A.; Zhang, S. Psychological Correlates of Self-Reported and Objectively Measured Physical Activity among Chinese Children—Psychological Correlates of PA. Int. J. Environ. Res. Public Health 2016, 13, 1006. [Google Scholar] [CrossRef] [Green Version]
- Benítez-Porres, J.; López-Fernández, I.; Raya, J.F.; Carnero, S.; Alvero-Cruz, J.R.; Carnero, E. Reliability and Validity of the PAQ-C Questionnaire to Assess Physical Activity in Children. J. Sch. Health 2016, 86, 677–685. [Google Scholar] [CrossRef]
- Benítez-Porres, J.; Alvero-Cruz, J.R.; Sardinha, L.; López-Fernández, I.; Carnero, E.A. Cut-off values for classifying active children and adolescentes using the Physical Activity Questionnaire: PAQ-C and PAQ-A. Nutr. Hosp. 2016, 33, 564. [Google Scholar] [CrossRef]
- Chan, C.H.S.; Ha, A.S.C.; Ng, J.Y.Y.; Lubans, D.R. Associations between fundamental movement skill competence, physical activity and psycho-social determinants in Hong Kong Chinese children. J. Sports Sci. 2019, 37, 229–236. [Google Scholar] [CrossRef]
- Ben Jemaa, H.; Mankaï, A.; Mahjoub, F.; Kortobi, B.; Khlifi, S.; Draoui, J.; Minaoui, R.; Karmous, I.; Ben Hmad, H.; Ben Slama, F.; et al. Physical Activity Level Assessed by Accelerometer and PAQ-C in Tunisian Children. Ann. Nutr. Metab. 2018, 73, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Welk, G.J.; Mcclain, J.; Ainsworth, B.E. Protocols for Evaluating Equivalency of Accelerometry-Based Activity Monitors. Med. Sci. Sports Exerc. 2012, 44, S39–S49. [Google Scholar] [CrossRef] [PubMed]
- Corder, K.; Ekelund, U.; Steele, R.M.; Wareham, N.J.; Brage, S. Assessment of physical activity in youth. J. Appl. Physiol. 2008, 105, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Bailey, D.A.; Mckay, H.A.; Mirwald, R.L.; Crocker, P.R.E.; Faulkner, R.A. A Six-Year Longitudinal Study of the Relationship of Physical Activity to Bone Mineral Accrual in Growing Children: The University of Saskatchewan Bone Mineral Accrual Study. J. Bone Miner. Res. 1999, 14, 1672–1679. [Google Scholar] [CrossRef]
- Chen, S.-R.; Lee, Y.-J.; Chiu, H.-W.; Jeng, C. Impact of physical activity on heart rate variability in children with type 1 diabetes. Child’s Nerv. Syst. 2008, 24, 741–747. [Google Scholar] [CrossRef]
- Ogunleye, A.A.; Voss, C.; Sandercock, G.R. Prevalence of high screen time in English youth: Association with deprivation and physical activity. J. Public Health 2011, 34, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Voss, C.; Ogunleye, A.A.; Sandercock, G.R. Physical Activity Questionnaire for children and adolescents: English norms and cut-off points. Pediatr. Int. 2013, 55, 498–507. [Google Scholar] [CrossRef]
- Bingham, D.D.; Costa, S.; Hinkley, T.; Shire, K.A.; Clemes, S.A.; Barber, S.E. Physical Activity During the Early Years: A Systematic Review of Correlates and Determinants. Am. J. Prev. Med. 2016, 51, 384–402. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, J.E.; John, D.; Freedson, P.S. Validation and comparison of ActiGraph activity monitors. J. Sci. Med. Sport 2011, 14, 411–416. [Google Scholar] [CrossRef]
- Leppänen, M.H.; Nyström, C.D.; Henriksson, P.; Pomeroy, J.; Ruiz, J.R.; Ortega, F.B.; Cadenas-Sánchez, C.; Löf, M. Physical activity intensity, sedentary behavior, body composition and physical fitness in 4-year-old children: Results from the ministop trial. Int. J. Obes. 2016, 40, 1126–1133. [Google Scholar] [CrossRef]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Mâsse, L.C.; Tilert, T.; Mcdowell, M. Physical Activity in the United States Measured by Accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, M.; Verloigne, M.; De Bourdeaudhuij, I.; Androutsos, O.; Manios, Y.; Felső, R.; Kovács, É.; Doessegger, A.; Bringolf-Isler, B.; Velde, S.J.T.; et al. Study protocol of physical activity and sedentary behaviour measurement among schoolchildren by accelerometry—Cross-sectional survey as part of the ENERGY-project. BMC Public Health 2011, 11, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandler, J.L.; Brazendale, K.; Beets, M.W.; Mealing, B.A. Classification of physical activity intensities using a wrist-worn accelerometer in 8-12-year-old children. Pediatr. Obes. 2015, 11, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: New York, NY, USA, 1988; ISBN 0805802835. [Google Scholar]
- Ruiz, J.R.; Ortega, F.B.; Rizzo, N.S.; Villa, I.; Hurtig-Wennlöf, A.; Oja, L.; Sjöström, M. High Cardiovascular Fitness Is Associated with Low Metabolic Risk Score in Children: The European Youth Heart Study. Pediatr. Res. 2007, 61, 350–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metz, C.E. Basic Principles of ROC Analysis. Available online: http://gim.unmc.edu/dxtests/ROC1.htm (accessed on 4 May 2018).
- Fairclough, S.J.; Noonan, R.; Rowlands, A.V.; VAN Hees, V.; Knowles, Z.; Boddy, L.M. Wear Compliance and Activity in Children Wearing Wrist- and Hip-Mounted Accelerometers. Med. Sci. Sports Exerc. 2016, 48, 245–253. [Google Scholar] [CrossRef]
- Clevenger, K.A.; Pfeiffer, K.A.; Mackintosh, K.A.; McNarry, M.; Brønd, J.C.; Arvidsson, D.; Montoye, A.H.K. Effect of sampling rate on acceleration and counts of hip- and wrist-worn ActiGraph accelerometers in children. Physiol. Meas. 2019, 40, 095008. [Google Scholar] [CrossRef]
- Alonso-Fernández, N.; Garcia, R.J.; Alonso-Fernández, L.; Hernandez-Barrera, V.; Palacios-Ceña, D. Health factors related to physical activity among children and adolescents: Results from Spanish National Health Surveys 2006 and 2011/12. J. Spéc. Pediatr. Nurs. 2015, 20, 193–202. [Google Scholar] [CrossRef]
- Chesham, R.; Booth, J.N.; Sweeney, E.; Ryde, G.C.; Gorely, T.; Brooks, N.; Moran, C.N. The Daily Mile makes primary school children more active, less sedentary and improves their fitness and body composition: A quasi-experimental pilot study. BMC Med. 2018, 16, 64. [Google Scholar] [CrossRef]


{kind=link}
| All (n = 126) | Girls (n = 60) | Boys (n = 66) | |
|---|---|---|---|
| Age (years) | 9.9 (0.4) | 9.9 (0.3) | 9.9 (0.4) |
| Height (cm) | 140.0 (6.5) | 139.7 (5.8) | 140.3 (7.0) |
| Weight (kg) | 35.9 (7.7) | 34.8 (7.6) | 37.0 (7.6) |
| Waist circumference (cm) | 63.5 (9.4) | 60.3 (10.1) | 66.2 (7.9) |
| BMI (kg·m−2) | 18.2 (3.0) | 17.7 (2.9) | 18.7 (3.0) |
| PAQ-C-It score | 2.81 (0.66) | 2.77 (0.66) | 2.83 (0.68) |
| MVPA (min/day) | 64.4 (20.3) | 68.8 (19.3) * | 60.4 (20.6) |
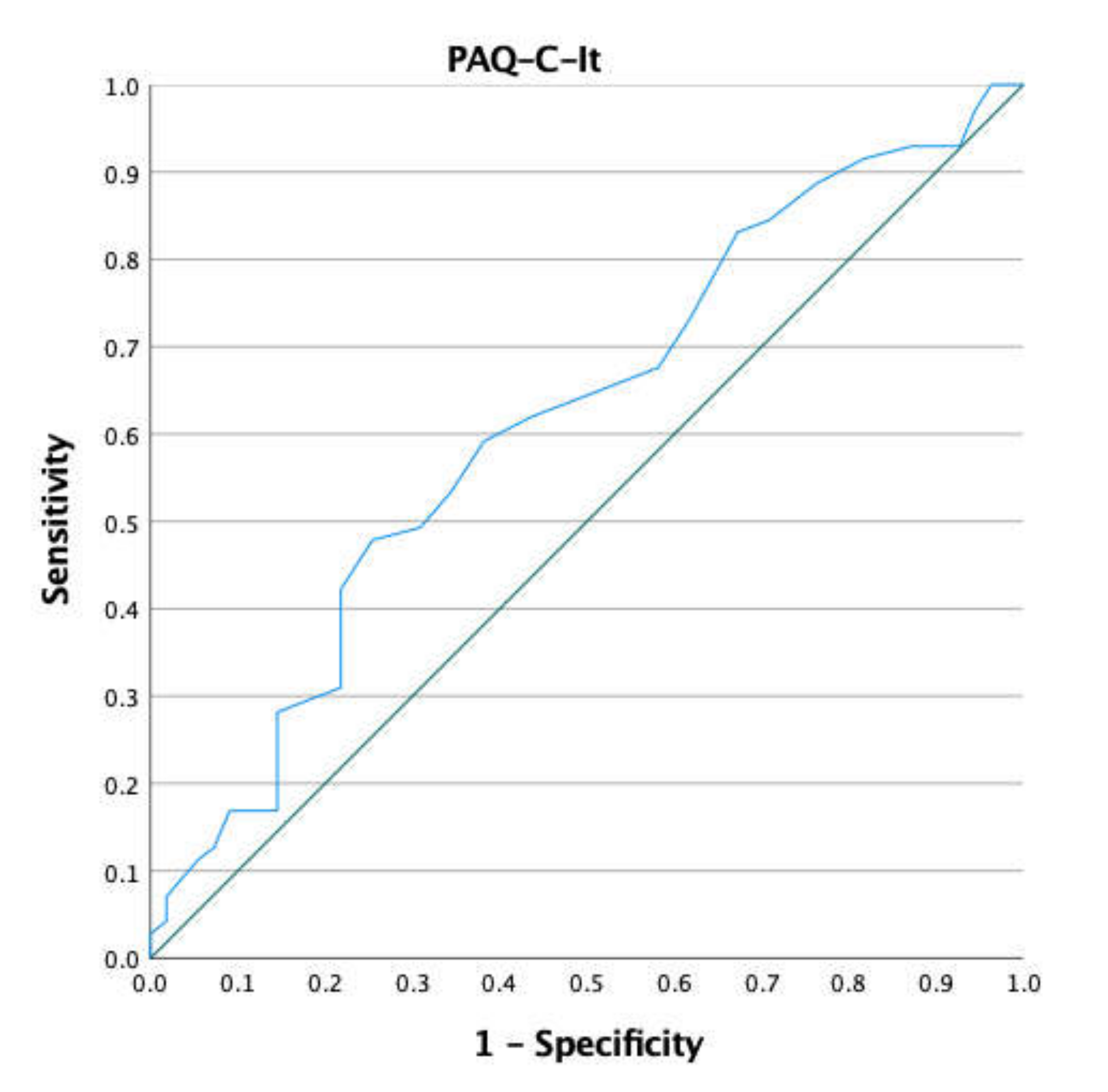
| Positive if Greater Than | Sensibility | 1-Specificity | Youden Index |
|---|---|---|---|
| 0.1 | 1 | 1 | 0 |
| 1.65 | 1 | 0.964 | 0.03 |
| 1.75 | 0.972 | 0.945 | 0.02 |
| 1.85 | 0.93 | 0.927 | 0.00 |
| 1.95 | 0.93 | 0.873 | 0.05 |
| 2.05 | 0.915 | 0.818 | 0.09 |
| 2.15 | 0.887 | 0.764 | 0.12 |
| 2.25 | 0.845 | 0.709 | 0.13 |
| 2.35 | 0.831 | 0.673 | 0.15 |
| 2.45 | 0.732 | 0.618 | 0.11 |
| 2.55 | 0.676 | 0.582 | 0.09 |
| 2.65 | 0.62 | 0.436 | 0.18 |
| 2.75 | 0.592 | 0.382 | 0.21 |
| 2.79 | 0.535 | 0.345 | 0.19 |
| 2.85 | 0.493 | 0.309 | 0.18 |
| 2.95 | 0.479 | 0.255 | 0.22 |
| 3.05 | 0.423 | 0.218 | 0.20 |
| 3.15 | 0.366 | 0.218 | 0.14 |
| 3.25 | 0.31 | 0.218 | 0.09 |
| 3.35 | 0.282 | 0.145 | 0.13 |
| 3.45 | 0.225 | 0.145 | 0.08 |
| 3.55 | 0.169 | 0.145 | 0.02 |
| 3.65 | 0.169 | 0.091 | 0.07 |
| 3.75 | 0.127 | 0.073 | 0.05 |
| 3.85 | 0.113 | 0.055 | 0.05 |
| 3.95 | 0.07 | 0.018 | 0.05 |
| 4.05 | 0.042 | 0.018 | 0.02 |
| 4.15 | 0.028 | 0 | 0.02 |
| 4.3 | 0.014 | 0 | 0.01 |
| 5.4 | 0 | 0 | 0 |
| PAQ-C-It Score for MVPA (60-min) | |
|---|---|
| AUC (95% CI) | 0.62 (0.52 to 0.72) |
| Standard Error | 0.05 |
| p | 0.025 |
| Youden Index | 0.21 |
| Cut-off point | >2.75 |
| Sensitivity (95% CI) | 0.592 (0.47 to 0.71) |
| Specificity (95% CI) | 0.382 (0.25 to 0.51) |
| Positive likelihood ratio (95% CI) | 1.55 (1.05 to 2.28) |
| Negative likelihood ratio (95% CI) | 0.66 (0.46 to 0.93) |
| Positive predictive values (95% CI) | 66% (55% to 78%) |
| Negative predictive values (95% CI) | 54% (41% to 66%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lupo, C.; Boccia, G.; Ungureanu, A.N.; Mulasso, A.; De Pasquale, P.; Mancini, A.; Buono, P.; Rainoldi, A.; Brustio, P.R. The Cut-Off Value for Classifying Active Italian Children Using the Corresponding National Version of the Physical Activity Questionnaire. Sports 2022, 10, 61. https://0-doi-org.brum.beds.ac.uk/10.3390/sports10040061
Lupo C, Boccia G, Ungureanu AN, Mulasso A, De Pasquale P, Mancini A, Buono P, Rainoldi A, Brustio PR. The Cut-Off Value for Classifying Active Italian Children Using the Corresponding National Version of the Physical Activity Questionnaire. Sports. 2022; 10(4):61. https://0-doi-org.brum.beds.ac.uk/10.3390/sports10040061
Chicago/Turabian StyleLupo, Corrado, Gennaro Boccia, Alexandru Nicolae Ungureanu, Anna Mulasso, Paolo De Pasquale, Annamaria Mancini, Pasqualina Buono, Alberto Rainoldi, and Paolo Riccardo Brustio. 2022. "The Cut-Off Value for Classifying Active Italian Children Using the Corresponding National Version of the Physical Activity Questionnaire" Sports 10, no. 4: 61. https://0-doi-org.brum.beds.ac.uk/10.3390/sports10040061