
Empowered, Yet Vulnerable: Motives for Sport Participation, Health Correlates, and Experience of Sexual Harassment in Female Combat-Sport Athletes

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
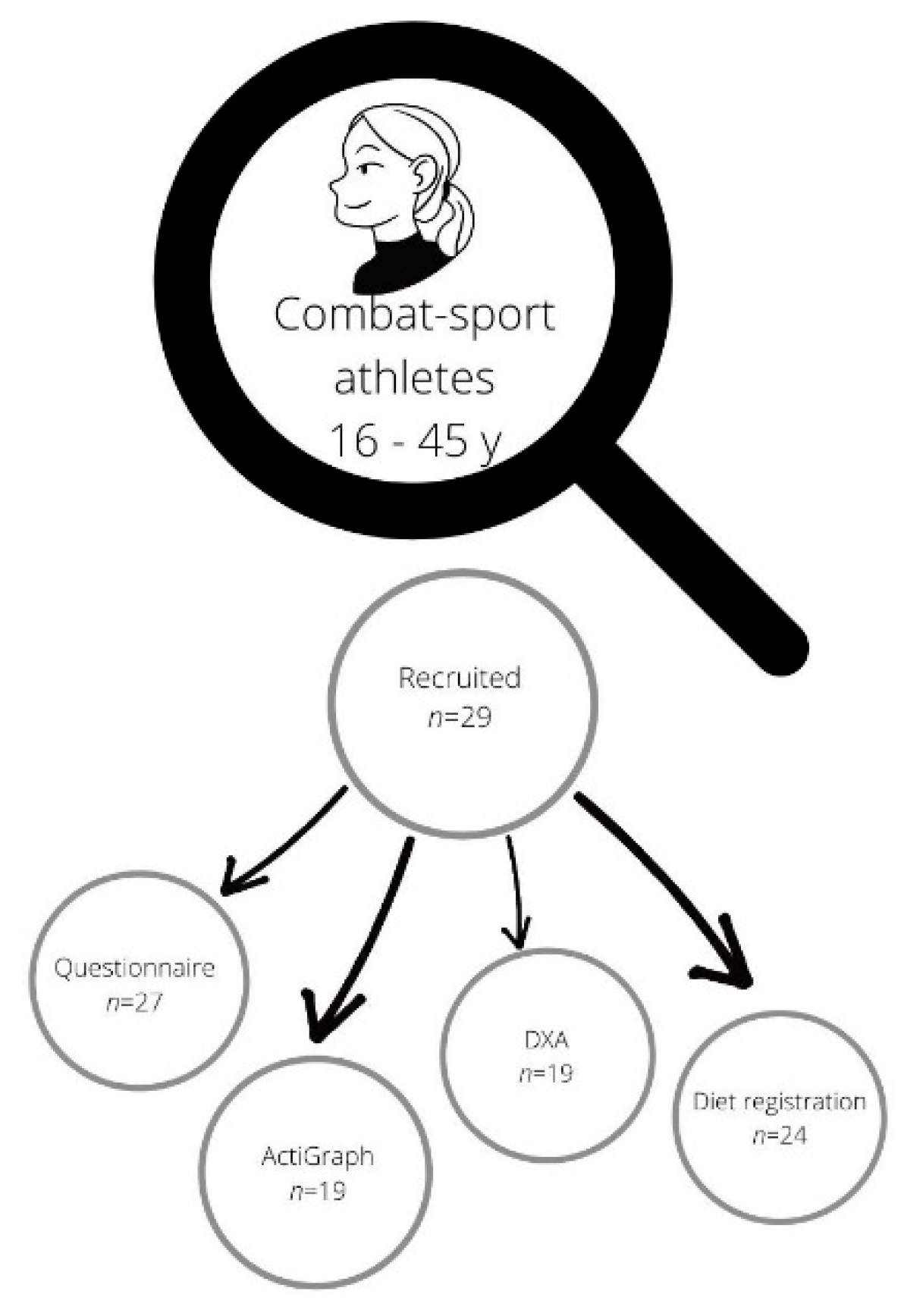
2.2. Participants
2.3. Outcomes
3. Results
3.1. Mental Health
3.2. Physical Health
3.3. Nutritional Intake, Dietary Information
3.4. Weight Regulation
3.5. Sexual Harassment
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matthews, C.R.; Channon, A. Global Perspectives on Women in Combat Sports: Women Warriors around the World; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Jensen, G. Meet the Fearless Athletes Who Are Taking Women’s Combat Sports Mainstream. Huffington Post. 2016. Available online: Huffpost.com (accessed on 2 February 2022).
- Hamilton, J. Undoing Gender or Overdoing Gender? Women MMA Athletes’ Intimate Partnering and the Relational Maintenance of Femininity. Sociol. Sport J. 2020, 37, 346–354. [Google Scholar] [CrossRef]
- Channon, A.; Jennings, G. The Rules of Engagement: Negotiating Painful and “Intimate” Touch in Mixed-Sex Martial Arts. Sociol. Sport J. 2013, 30, 487–503. [Google Scholar] [CrossRef] [Green Version]
- Bråthen, M.; Øistad, B.S. Sexual Harassment in Working life. Survey among the Members in the Norwegian labor Union Fellesforbundet Employed in Hotels and Restaurants and in Health and Welfare Services, in Sexual Harassment in Working Life. Fafo. 2017. Available online: https://www.fafo.no/zoo-publikasjoner/fafo-rapporter/item/seksuell-trakassering-i-arbeidslivet-3 (accessed on 2 February 2022).
- Norwegian Ministry of Culture. Act Relating to Equality and a Prohibition against Discrimination (Equality and Anti-Discrimination Act); LOV-2017-06-16-2018; Ministry of Justice: Oslo, Norway, 2018. [Google Scholar]
- Pina, A.; Gannon, T.A. An overview of the literature on antecedents, perceptions and behavioural consequences of sexual harassment. J. Sex. Aggress. 2012, 18, 209–232. [Google Scholar] [CrossRef]
- Pina, A.; Gannon, T.A.; Saunders, B. An overview of the literature on sexual harassment: Perpetrator, theory, and treatment issues. Aggress. Violent Behav. 2009, 14, 126–138. [Google Scholar] [CrossRef]
- Murphy, W.F. Investigating the incidence of sexual assault in martial arts coaching using media reports. Digit. Investig. 2019, 30, 90–93. [Google Scholar] [CrossRef]
- Barley, O.R.; Chapman, D.W.; Abbiss, C.R. The Current State of Weight-Cutting in Combat Sports-Weight-Cutting in Combat Sports. Sports 2019, 7, 123. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.K. UFC Vegas 38 Video: Aspen Ladd Misses Weight after Lengthy Struggle on Scale, Fight Cancelled. 2021. Available online: https://www.mmafighting.com/2021/10/1/22704585/ufc-vegas-38-video-aspen-ladd-misses-weight-after-lengthy-struggle-on-scale (accessed on 3 October 2021).
- Matthews, J.J.; Stanhope, E.; Godwin, M.S.; Holmes, M.E.; Artioli, G.G. The Magnitude of Rapid Weight Loss and Rapid Weight Gain in Combat Sport Athletes Preparing for Competition: A Systematic Review. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 441–452. [Google Scholar] [CrossRef] [Green Version]
- Hillier, M.; Sutton, L.; James, L.; Mojtahedi, D.; Keay, N.; Hind, K. High Prevalence and Magnitude of Rapid Weight Loss in Mixed Martial Arts Athletes. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 512–517. [Google Scholar] [CrossRef]
- Carl, R.L.; Johnson, M.D.; Martin, T.J.; LaBella, C.R.; Brooks, M.A.; Diamond, A.; Hennrikus, W.; LaBotz, M.; Logan, K.; Loud, K.J.; et al. Promotion of Healthy Weight-Control Practices in Young Athletes. Pediatrics 2017, 140, e20171871. [Google Scholar] [CrossRef] [Green Version]
- White, T.; Kirk, C. Pre-competition body mass loss characteristics of Brazilian jiu-jitsu competitors in the United Kingdom. Nutr. Health 2021, 260106020983800. [Google Scholar] [CrossRef]
- Escobar-Molina, R.; Rodríguez-Ruiz, S.; Gutiérrez-García, C.; Franchini, E. Weight Loss and Psychological-Related States in High-Level Judo Athletes. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Sundgot-Borgen, C.; Sundgot-Borgen, J.; Bratland-Sanda, S.; Kolle, E.; Torstveit, M.K.; Svantorp-Tveiten, K.M.E.; Mathisen, T.F. Body appreciation and body appearance pressure in Norwegian university students comparing exercise science students and other students. BMC Public Health 2021, 21, 352. [Google Scholar] [CrossRef] [PubMed]
- Avalos, L.; Tylka, T.L.; Wood-Barcalow, N. The Body Appreciation Scale: Development and psychometric evaluation. Body Image 2005, 2, 285–297. [Google Scholar] [CrossRef]
- Tylka, T.L.; Wood-Barcalow, N.L. The Body Appreciation Scale-2: Item refinement and psychometric evaluation. Body Image 2015, 12, 53–67. [Google Scholar] [CrossRef] [PubMed]
- Melin, A.; Tornberg, Å.B.; Skouby, S.; Faber, J.; Ritz, C.; Sjödin, A.; Sundgot-Borgen, J. The LEAF questionnaire: A screening tool for the identification of female athletes at risk for the female athlete triad. Br. J. Sports Med. 2014, 48, 540–545. [Google Scholar] [CrossRef]
- Rogers, M.A.; Drew, M.K.; Appaneal, R.; Lovell, G.; Lundy, B.; Hughes, D.; Vlahovich, N.; Waddington, G.; Burke, L.M. The Utility of the Low Energy Availability in Females Questionnaire to Detect Markers Consistent with Low Energy Availability-Related Conditions in a Mixed-Sport Cohort. Int. J. Sport Nutr. Exerc. Metab. 2021, 31, 427–437. [Google Scholar] [CrossRef]
- Fairburn, C.; Beglin, S. Eating Disorder Examination Questionnaire (EDE-Q 6.0), in Cognitive Behavior Therapy and Eating Disorders; Fairburn, C., Ed.; Guildford Press: New York, NY, USA, 2008; pp. 309–313. [Google Scholar]
- Nana, A.; Slater, G.; Stewart, A.; Burke, L.M. Methodology Review: Using Dual-Energy X-Ray Absorptiometry (DXA) for the Assessment of Body Composition in Athletes and Active People. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 198–215. [Google Scholar] [CrossRef]
- International Society for Clinical Densitometry. The International Society for Clinical Densitometry, Official Positions 2019—Adult; ISCD: Middletown, CT, USA, 2019; p. 34. Available online: https://iscd.org (accessed on 2 February 2022).
- Tenforde, A.S.; Fredericson, M. Influence of sports participation on bone health in the young athlete: A review of the literature. PMR 2011, 3, 861–867. [Google Scholar] [CrossRef]
- Fehling, P.; Alekel, L.; Clasey, J.; Rector, A.; Stillman, R. A comparison of bone mineral densities among female athletes in impact loading and active loading sports. Bone 1995, 17, 205–210. [Google Scholar] [CrossRef]
- Taaffe, D.; Snow-Harter, C.; Connolly, D.A.; Robinson, T.L.; Brown, M.D.; Marcus, R. Differential effects of swimming versus weight-bearing activity on bone mineral status of eumenorrheic athletes. J. Bone Miner. Res. 1995, 10, 586–593. [Google Scholar] [CrossRef]
- Jonvik, K.L.; Torstveit, M.K.; Sundgot-Borgen, J.K.; Mathisen, T.F. Do we need to change the guideline values for determining low bone mineral density in athletes? J. Appl. Physiol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Helsedirektoratet. Anbefalinger om Kosthold Ernæring og Fysisk Aktivitet; Helsedirektoratet: Oslo, Norway, 2013; p. 28. [Google Scholar]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American college of Sports Medicine, Nutrition and Athletic Performance. Med. Sci. Sports Exerc. 2016, 48, 543–568. [Google Scholar] [PubMed]
- Janiszewska, K.; Przybyłowicz, K.E. Pre-Competition Weight Loss Models in Taekwondo: Identification, Characteristics and Risk of Dehydration. Nutrients 2020, 12, 2793. [Google Scholar] [CrossRef] [PubMed]
- Sundgot-Borgen, J.; Garthe, I. Elite athletes in aesthetic and Olympic weight-class sports and the challenge of body weight and body compositions. J. Sports Sci. 2011, 29 (Suppl. S1), S101–S114. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, S.; Ekström, M.P.; Berg, C. Practices of Weight Regulation Among Elite Athletes in Combat Sports: A Matter of Mental Advantage? J. Athl. Train. 2013, 48, 99–108. [Google Scholar] [CrossRef] [Green Version]
- Berkovich, B.-E.; Stark, A.; Eliakim, A.; Nemet, D.; Sinai, T. Rapid Weight Loss in Competitive Judo and Taekwondo Athletes: Attitudes and Practices of Coaches and Trainers. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 532–538. [Google Scholar] [CrossRef]
- Rouveix, M.; Bouget, M.; Pannafieux, C.; Champely, S.; Filaire, E. Eating Attitudes, Body Esteem, Perfectionism and Anxiety of Judo Athletes and Nonathletes. Int. J. Sports Med. 2007, 28, 340–345. [Google Scholar] [CrossRef]
- Mathisen, T.F.; Aambø, J.; Bratland-Sanda, S.; Sundgot-Borgen, C.; Svantorp-Tveiten, K.; Sundgot-Borgen, J. Body Figure Idealization and Body Appearance Pressure in Fitness Instructors. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- Mathisen, T.F.F.; Sundgot-Borgen, C.; Anstensrud, B. Mental health, eating behaviour and injuries in professional dance students. Res. Dance Educ. 2022, 23, 108–125. [Google Scholar]
- Taylor, B.C. Weight and Shape Concern and Body Image as Risk Factors for Eating Disorders. In Encyclopedia of Feeding and Eating Disorders; Wade, T., Ed.; Springer: Singapore, 2016; pp. 1–5. [Google Scholar]
- Levine, M.P.; Smolak, L. The role of protective factors in the prevention of negative body image and disordered eating. Eat. Disord. 2016, 24, 39–46. [Google Scholar] [CrossRef]
- Kotarska, K.; Nowak, L.; Szark-Eckardt, M.; Nowak, M.A. Intensity of Health Behaviors in People Who Practice Combat Sports and Martial Arts. Int. J. Environ. Res. Public Health 2019, 16, 2463. [Google Scholar] [CrossRef] [Green Version]
- Hansen, B.H.; Anderssen, S.A.; Steene-Johannessen, J.; Ekelund, U.; Nilsen, A.K.; Andersen, I.D.; Dalene, K.E.; Kolle, E. Fysisk Aktivitet og Sedat Tid Blant Voksne og Eldre i Norge—Nasjonal Kartlegging 2014–2015; Norwegian Directorate of Health: Oslo, Norway, 2015; p. 154. [Google Scholar]
- Fahrenholtz, I.L.; Sjödin, A.; Benardot, D.; Tornberg, Å.B.; Skouby, S.O.; Faber, J.; Sundgot-Borgen, J.K.; Melin, A. Within-day energy deficiency and reproductive function in female endurance athletes. Scand. J. Med. Sci. Sports 2018, 28, 1139–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torstveit, M.K.; Fahrenholtz, I.; Stenqvist, T.B.; Sylta, Ø.; Melin, A. Within-Day Energy Deficiency and Metabolic Perturbation in Male Endurance Athletes. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 419–427. [Google Scholar] [CrossRef] [PubMed]
- De Quel, M.; Óscar, M.; Ara, I.; Izquierdo, M.; Ayán, C. Does Physical Fitness Predict Future Karate Success? A Study in Young Female Karatekas. Int. J. Sports Physiol. Perform. 2020, 15, 868–873. [Google Scholar] [CrossRef] [PubMed]
- Reale, R.; Burke, L.M.; Cox, G.R.; Slater, G. Body composition of elite Olympic combat sport athletes. Eur. J. Sport Sci. 2020, 20, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Agostinete, R.R.; Vlachopoulos, D.; Werneck, A.O.; Vanegas, S.M.; Lynch, K.R.; Naughton, G.; Fernandes, R.A. Bone accrual over 18 months of participation in different loading sports during adolescence. Arch. Osteoporos. 2020, 15, 64. [Google Scholar] [CrossRef]
- Maillane-Vanegas, S.; Agostinete, R.R.; Lynch, K.R.; Ito, I.H.; de Marco, R.L.; Rodrigues-Junior, M.A.; Turi-Lynch, B.C.; Fernandes, R.A. Bone Mineral Density and Sports Participation. J. Clin. Densitom. 2020, 23, 294–302. [Google Scholar] [CrossRef]
- Nattiv, A.; Loucks, A.B.; Manore, M.M.; Sanborn, C.F.; Sundgot-Borgen, J.; Warren, M.P. American College of Sports Medicine the Female Athlete Triad. Med. Sci. Sports Exerc. 2007, 39, 1867–1882. [Google Scholar]
- Solmi, M.; Veronese, N.; Correll, C.U.; Favaro, A.; Santonastaso, P.; Caregaro, L.; Vancampfort, D.; Luchini, C.; De Hert, M.; Stubbs, B. Bone mineral density, osteoporosis, and fractures among people with eating disorders: A systematic review and meta-analysis. Acta Psychiatr. Scand. 2016, 133, 341–351. [Google Scholar] [CrossRef]
- Mountjoy, M.; Sundgot-Borgen, J.; Burke, L.M.; Ackerman, K.E.; Blauwet, C.; Constantini, N.; Lebrun, C.; Lundy, B.; Melin, A.; Meyer, N.; et al. International Olympic Committee (IOC) Consensus Statement on Relative Energy Deficiency in Sport (RED-S): 2018 Update. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 316–331. [Google Scholar] [CrossRef] [Green Version]
- Mountjoy, M.; Brackenridge, C.; Arrington, M.; Blauwet, C.; Carska-Sheppard, A.; Fasting, K.; Kirby, S.; Leahy, T.; Marks, S.; Martin, K.; et al. International Olympic Committee consensus statement: Harassment and abuse (non-accidental violence) in sport. Br. J. Sports Med. 2016, 50, 1019–1029. [Google Scholar] [CrossRef]
- Sundgot-Borgen, J.; Fasting, K.; Brackenridge, C.; Torstveit, M.K.; Berglund, B. Sexual harassment and eating disorders in female elite athletes—A controlled study. Scand. J. Med. Sci. Sports 2003, 13, 330–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fasting, K.; Chroni, S.; Hervik, S.E.; Knorre, N. Sexual harassment in sport toward females in three European countries. Int. Rev. Sociol. Sport 2011, 46, 76–89. [Google Scholar] [CrossRef] [Green Version]
- Ohlert, J.; Rau, T.; Rulofs, B.; Allroggen, M. Comparison of elite athletes’ sexual violence experiences in and outside sport. Ger. J. Exerc. Sport Res. 2020, 50, 435–443. [Google Scholar] [CrossRef]
- Bermon, S.; Adami, P.E.; Dahlström, O.; Fagher, K.; Hautala, J.; Ek, A.; Anderson, C.; Jacobsson, J.; Svedin, C.G.; Timpka, T. Lifetime Prevalence of Verbal, Physical, and Sexual Abuses in Young Elite Athletics Athletes. Front. Sports Act. Living 2021, 3. [Google Scholar] [CrossRef]
- Gavilanes, J.M.R. Low sample size and regression: A Monte Carlo approach. J. Appl. Econ. Sci. 2020, 15, 22–44. [Google Scholar]
- Herrera-Valenzuela, T.; Vargas, J.J.N.; Merlo, R.; Valdés-Badilla, P.A.; Pardo-Tamayo, C.; Franchini, E. Effect of the COVID-19 quarantine on body weight among combat sports athletes. Nutr. Hosp. 2020, 37, 1186–1189. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Female Combat-Sport Athletes | |
|---|---|
| Age, years # | 23.5 (6.3) |
| BMI, kg × h−2 | 22.7 (1.7) |
| Combat sport exercise volume, hours per week | 6.3 (1.8) |
| Age of combat-sport specialization, years # | 16.0 (11.0) |
| Exercise volume, other sports, hours per week | 4.3 (1.8) |
| CPM * | 457.3 (204.2) |
| Educational level ≥ BSc, n (%) | 17 (59) |
| Female Combat-Sport Athletes | |
|---|---|
| Eating disorders, n (%) | 9 (33) |
| EDE-q global score # | 1.1 (2.1) |
| EDE-q weight concern # | 1.6 (3.0) |
| EDE-q shape concern # | 1.9 (2.8) |
| EDE-q eating concern # | 0.2 (1.0) |
| EDE-q eating restriction # | 1.2 (1.6) |
| BAS-2 total score | 3.8 (0.6) |
| Female Combat-Sport Athletes | |
|---|---|
| Body weight, kg | 62.1 (6.4) |
| Maximal adult BW difference, kg | 10.5 (6.0) |
| Competitive BW, kg | 61.5 (7.8) |
| Body fat percentage (%) | 25.4 (5.2) |
| BMD total body, gram × cm−2 | 1.23 (0.1) |
| BMD Z-score total body | 1.5 (1.1) |
| BMD proximal femur, gram × cm−2 | 1.1 (0.1) |
| BMD Z-score proximal femur | 0.8 (1.0) |
| BMD lumbar spine, gram × cm−2 | 1.3 (0.2) |
| BMD Z-score lumbar spine | 0.9 (1.2) |
| Female Combat-Sport Athletes | Recommendations | |
|---|---|---|
| Energy intake, kcal | 1770.9 (467.9) | |
| Energy intake, kcal × kg BW−2 | 29.8 (10.7) | ≥40 kcal × kg LBM−2 (sr) |
| Protein intake | 76.0 (42.0) | |
| Protein intake, kcal × kg BW−2 | 1.4 (0.6) | 1.2–2.0 g × kg BW−2 (sr) |
| Carbohydrate intake | 201.7 (54.2) | |
| Carbohydrate intake, kcal × kg BW−2 | 3.4 (1.3) | 5–7 g × kg BW−2 (sr) |
| Dietary fiber intake, gram per day | 24.6 (10.7) | 25 35 g × day−2 (na) |
| Fat intake, percent of energy intake (%) | 36.9 (5.7) | 25–40 E% (na) |
| Vitamin D, µg per day | 4.4 (5.9) | 10 µg (na) |
| Calcium, gram per day | 776.5 (329.8) | 800 mg (na) |
| Iron, mg per day | 9.5 (5.7) | 15 mg (na) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathisen, T.F.; Kumar, R.S.; Svantorp-Tveiten, K.M.E.; Sundgot-Borgen, J. Empowered, Yet Vulnerable: Motives for Sport Participation, Health Correlates, and Experience of Sexual Harassment in Female Combat-Sport Athletes. Sports 2022, 10, 68. https://0-doi-org.brum.beds.ac.uk/10.3390/sports10050068
Mathisen TF, Kumar RS, Svantorp-Tveiten KME, Sundgot-Borgen J. Empowered, Yet Vulnerable: Motives for Sport Participation, Health Correlates, and Experience of Sexual Harassment in Female Combat-Sport Athletes. Sports. 2022; 10(5):68. https://0-doi-org.brum.beds.ac.uk/10.3390/sports10050068
Chicago/Turabian StyleMathisen, Therese Fostervold, Radhika Singh Kumar, Kethe M. E. Svantorp-Tveiten, and Jorunn Sundgot-Borgen. 2022. "Empowered, Yet Vulnerable: Motives for Sport Participation, Health Correlates, and Experience of Sexual Harassment in Female Combat-Sport Athletes" Sports 10, no. 5: 68. https://0-doi-org.brum.beds.ac.uk/10.3390/sports10050068