Vitamin D Status Differs by Sex, Sport-Season, and Skin Pigmentation among Elite Collegiate Basketball Players


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measurements
2.2.1. Skin Pigmentation
2.2.2. Sun Exposure
2.2.3. Body Composition and Bone Health
2.2.4. Hematology and Blood Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wyon, M.A.; Wolman, R.; Nevill, A.M.; Cloak, R.; Metsios, G.S.; Gould, D.; Ingham, A.; Koutedakis, Y. Acute effects of vitamin D3 supplementation on muscle strength in judoka athletes: A randomized placebo-controlled, double-blind trial. Clin. J. Sports Med. 2016, 26, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Holick, M.F. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am. J. Clin. Nutr. 2004, 80, 1678S–1688S. [Google Scholar] [CrossRef] [PubMed]
- Bartoszewska, M.; Kamboj, M.; Patel, D.R. Vitamin D, Muscle Function, and Exercise Performance. Pediatr. Clin. North Am. 2010, 57, 849–861. [Google Scholar] [CrossRef] [PubMed]
- Cannell, J.J.; Hollis, B.W.; Sorenson, M.B.; Taft, T.N.; Anderson, J.J.B. Athletic performance and Vitamin D. Med. Sci. Sports Exerc. 2009, 41, 1102–1110. [Google Scholar] [CrossRef] [PubMed]
- Barker, T.; Martins, T.B.; Hill, H.R.; Kjeldsberg, C.R.; Trawick, R.H.; Weaver, L.K.; Traber, M.G. Low Vitamin D Impairs Strength Recovery after Anterior Cruciate Ligament Surgery. J. Evid. Based Integr. Med. 2011, 16, 201–209. [Google Scholar] [CrossRef]
- Close, G.; Russell, J.; Cobley, J.; Owens, D.; Wilson, G.; Gregson, W.; Fraser, W.; Morton, J. Assessment of vitamin D concentration in non-supplemented professional athletes and healthy adults during the winter months in the UK: Implications for skeletal muscle function. J. Sports Sci. 2013, 31, 344–353. [Google Scholar] [CrossRef]
- Maroon, J.C.; Mathyssek, C.M.; Bost, J.W.; Amos, A.; Winkelman, R.; Yates, A.P.; Duca, M.A.; Norwig, J.A. Vitamin D Profile in National Football League Players. Am. J. Sports Med. 2015, 43, 1241–1245. [Google Scholar] [CrossRef]
- Wyon, M.A.; Koutedakis, Y.; Wolman, R.; Nevill, A.M.; Allen, N. The influence of winter vitamin D supplementation on muscle function and injury occurrence in elite ballet dancers: A controlled study. J. Sci. Med. Sport 2014, 17, 8–12. [Google Scholar] [CrossRef]
- Halliday, T.M.; Peterson, N.J.; Thomas, J.J.; Kleppinger, K.; Hollis, B.W.; Larson-Meyer, D.E. Vitamin D Status Relative to Diet, Lifestyle, Injury, and Illness in College Athletes. Med. Sci. Sports Exerc. 2011, 43, 335–343. [Google Scholar] [CrossRef]
- Hildebrand, R.A.; Miller, B.; Warren, A.; Hildebrand, D.; Smith, B.J. Compromised Vitamin D Status Negatively Affects Muscular Strength and Power of Collegiate Athletes. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Forney, L.A.; Earnest, C.P.; Henagan, T.M.; Johnson, L.E.; Castleberry, T.J.; Stewart, L.K. Vitamin D Status, Body Composition, and Fitness Measures in College-Aged Students. J. Strength Cond. Res. 2014, 28, 814–824. [Google Scholar] [CrossRef] [PubMed]
- Fishman, M.P.; Lombardo, S.J.; Kharrazi, F.D. Vitamin D Deficiency among Professional Basketball Players. Orthop. J. Sports Med. 2016, 4. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.S.; Assar, S.; Harnpanich, D.; Bouillon, R.; Lambrechts, D.; Prentice, A.; Schoenmakers, I. 25(OH)D2 half-life is shorter than 25(OH)D3 half-life and is influenced by DBP concentration and genotype. J. Clin. Endocrinol. Metab. 2014, 99, 3373–3381. [Google Scholar] [CrossRef]
- Gallo, S.; Phan, A.; Vanstone, C.A.; Rodd, C.; Weiler, H.A. The change in plasma 25-Hydroxyvitamin D did not differ between breast-fed infants that received a daily supplement of Ergocalciferol or Cholecalciferol for 3 months. J. Nutr. 2013, 143, 148–153. [Google Scholar] [CrossRef]
- Hanwell, H.; Vieth, R.; Cole, D.; Scillitani, A.; Modoni, S.G.; Frusciante, V.; Ritrovato, G.; Chiodini, I.; Minisola, S.; Carnevale, V.; et al. Sun exposure questionnaire predicts circulating 25-hydroxyvitamin D concentrations in Caucasian hospital workers in southern Italy. J. Steroid Biochem. Mol. Biol. 2010, 121, 334–337. [Google Scholar] [CrossRef]
- The International Society for Clinical Densitometry. Indications for Bone Mineral Density Testing; The International Society for Clinical Densitometry: West Hartford, CT, USA, 2015. [Google Scholar]
- Rice, M.E.; Harris, G.T. Comparing effect sizes in follow-up studies: ROC Area, Cohen’s d, and r. Law Hum. Behav. 2005, 29, 615–620. [Google Scholar] [CrossRef]
- Barcal, J.N.; Thomas, J.T.; Hollis, B.W.; Austin, K.J.; Alexander, B.M.; Larson-Meyer, D.E. Vitamin D and Weight Cycling: Impact on Injury, Illness, and Inflammation in Collegiate Wrestlers. Nutrients 2016, 8, 775. [Google Scholar] [CrossRef]
- Lovell, G. Vitamin D Status of Females in an Elite Gymnastics Program. Clin. J. Sport Med. 2008, 18, 159–161. [Google Scholar] [CrossRef]
- Pollock, N.; Dijkstra, P.; Chakraverty, R.; Hamilton, B. Low 25(OH) vitamin D concentrations in international UK track and field athletes. South Afr. J. Sports Med. 2012, 24, 55–59. [Google Scholar] [CrossRef]
- Willis, K.S.; Smith, D.T.; Broughton, K.S.; Larson-Meyer, D.E. Vitamin D status and biomarkers of inflammation in runners. Open Access J. Sports Med. 2012, 3, 35–42. [Google Scholar] [PubMed]
- Heller, J.E.; Thomas, J.J.; Hollis, B.W.; Larson-Meyer, D.E. Relation between Vitamin D Status and Body Composition in Collegiate Athletes. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Villacis, D.; Yi, A.; Jahn, R.; Kephart, C.J.; Charlton, T.; Gamradt, S.C.; Romano, R.; Tibone, J.E.; Hatch, G.F.R. Prevalence of Abnormal Vitamin D Levels among Division I NCAA Athletes. Sports Health 2014, 6, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Maruyama-Nagao, A.; Sakuraba, K.; Suzuki, Y. Seasonal variations in vitamin D status in indoor and outdoor female athletes. Biomed. Rep. 2016, 5, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Morton, J.P.; Iqbal, Z.; Drust, B.; Burgess, D.; Close, G.L.; Brukner, P.D. Seasonal variation in vitamin D status in professional soccer players of the English Premier League. Appl. Physiol. Nutr. Metab. 2012, 37, 798–802. [Google Scholar] [CrossRef]
- Krzywanski, J.; Mikulski, T.; Krysztofiak, H.; Mlynczak, M.; Gaczynska, E.; Ziemba, A. Seasonal Vitamin D Status in Polish Elite Athletes in Relation to Sun Exposure and Oral Supplementation. PLoS ONE 2016, 11, e0164395. [Google Scholar] [CrossRef]
- Kopeć, A.; Solarz, K.; Majda, F.; Słowińska-Lisowska, M.; Mędraś, M. An Evaluation of the Levels of Vitamin D and Bone Turnover Markers after the Summer and Winter Periods in Polish Professional Soccer Players. J. Hum. Kinet. 2013, 38, 135–140. [Google Scholar] [CrossRef]
- Backx, E.; Van Der Avoort, C.; Tieland, M.; Maase, K.; Kies, A.; Van Loon, L.J.; De Groot, L.; Mensink, M. Seasonal Variation in Vitamin D Status in Elite Athletes: A Longitudinal Study. Int. J. Sport Nutr. Exerc. Metab. 2017, 27, 6–10. [Google Scholar] [CrossRef]
- Arunabh, S.; Pollack, S.; Yeh, J.; Aloia, J.F. Body Fat Content and 25-Hydroxyvitamin D Levels in Healthy Women. J. Clin. Endocrinol. Metab. 2003, 88, 157–161. [Google Scholar] [CrossRef]
- Kremer, R.; Campbell, P.P.; Reinhardt, T.; Gilsanz, V. Vitamin D Status and its Relationship to Body Fat, Final Height, and Peak Bone Mass in Young Women. J. Clin. Endocrinol. Metab. 2009, 94, 67–73. [Google Scholar] [CrossRef]
- Yeum, K.-J.; Dawson-Hughes, B.; Joo, N.-S. Fat Mass Is Associated with Serum 25-Hydroxyvitamin D Concentration Regardless of Body Size in Men. Nutrients 2018, 10, 850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parikh, S.J.; Edelman, M.; Uwaifo, G.I.; Freedman, R.J.; Semega-Janneh, M.; Reynolds, J.; Yanovski, J.A. The Relationship between Obesity and Serum 1,25-Dihydroxy Vitamin D Concentrations in Healthy Adults. J. Clin. Endocrinol. Metab. 2004, 89, 1196–1199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laird, E.; Ward, M.; McSorley, E.; Strain, J.; Wallace, J. Vitamin D and Bone Health; Potential Mechanisms. Nutrients 2010, 2, 693–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allison, R.J.; Farooq, A.; Hamilton, B.; Close, G.L.; Wilson, M.G. No Association between Vitamin D Deficiency and Markers of Bone Health in Athletes. Med. Sci. Sports Exerc. 2015, 47, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Cassity, E.P.; Redzic, M.; Teager, C.R.; Thomas, D.T. The effect of body composition and BMI on 25(OH)D response in vitamin D-supplemented athletes. Eur. J. Sport Sci. 2016, 16, 773–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCabe, M.P.; Smyth, M.P.; Richardson, D.R. Current concept review: Vitamin D and stress fractures. Foot Ankle Int. 2012, 33, 526–533. [Google Scholar] [CrossRef]
- Mudd, L.M.; Fornetti, W.; Pivarnik, J.M. Bone Mineral Density in Collegiate Female Athletes: Comparisons among Sports. J. Athl. Train. 2007, 42, 403–408. [Google Scholar]
- Prelack, K.; Dwyer, J.; Ziegler, P.; Kehayias, J.J. Bone mineral density in elite adolescent female figure skaters. J. Int. Soc. Sports Nutr. 2012, 9, 57. [Google Scholar] [CrossRef] [Green Version]
- Del Bino, S.; Sok, J.; Bessac, E.; Bernerd, F. Relationship between skin response to ultraviolet exposure and skin color type. Pigment. Cell Res. 2006, 19, 606–614. [Google Scholar] [CrossRef]
- Binkley, N.; Novotny, R.; Krueger, D.; Kawahara, T.; Daida, Y.G.; Lensmeyer, G.; Hollis, B.W.; Drezner, M.K. Low Vitamin D Status despite Abundant Sun Exposure. J. Clin. Endocrinol. Metab. 2007, 92, 2130–2135. [Google Scholar] [CrossRef] [Green Version]
- Gebreegziabher, T.; Stoecker, B.J. Vitamin D insufficiency in a sunshine-sufficient area: Southern Ethiopia. Food Nutr. Bull. 2014, 34, 429–433. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
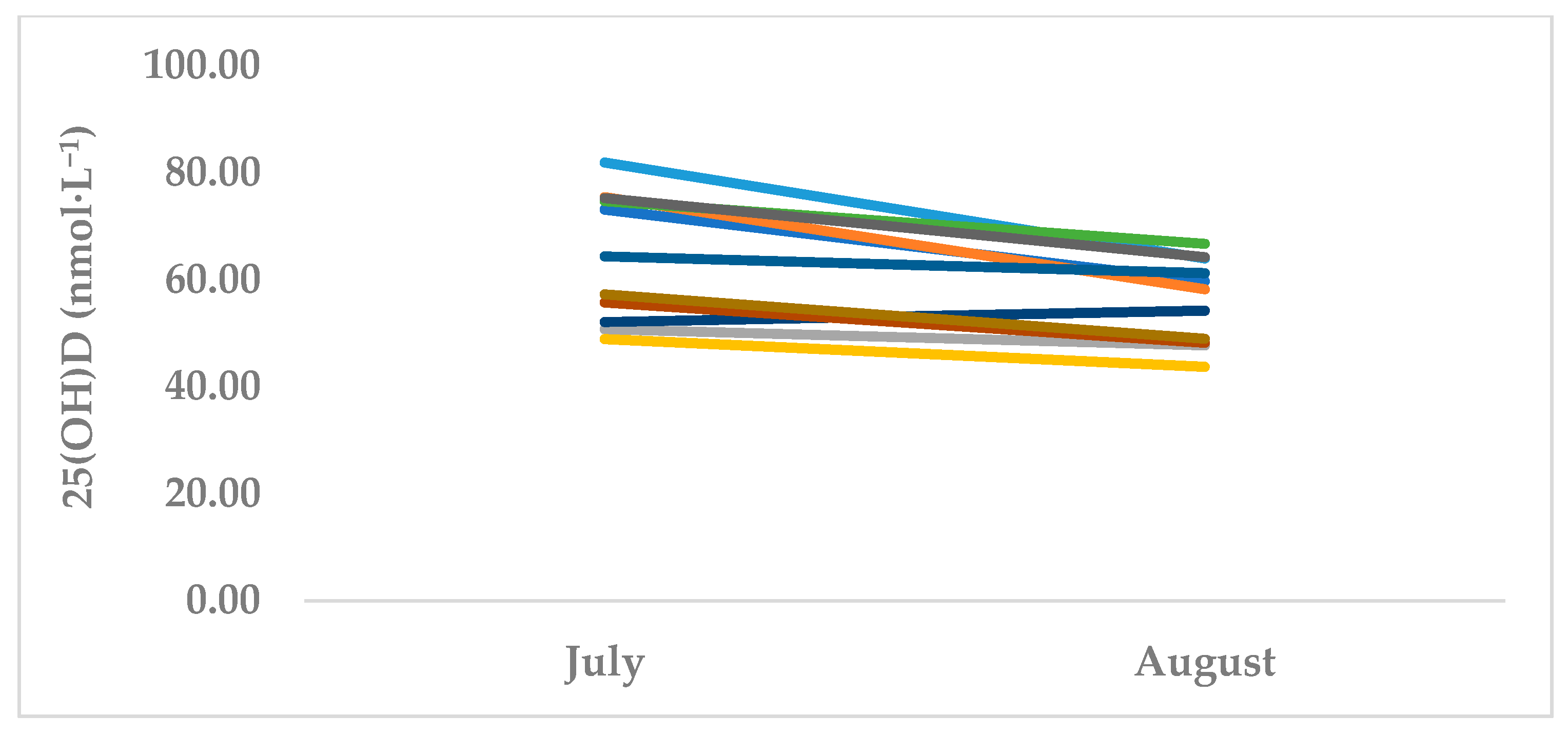
| Characteristics | T1 (Summer Off-season, July) Mean ± SD | T2 (Autumn Pre-season, October) Mean ± SD |
|---|---|---|
| 25(OH)D (nmol·L−1) | 64.5 ± 11.9 | 56.1 ± 7.9 * |
| <50 nmol·L−1 | 1 (11.1%) | 4 (36.3%) |
| 50–75 nmol·L−1 | 7 (63.6%) | 7 (63.6%) |
| >75 nmol·L−1 | 3 (27.2%) | 0 (0%) |
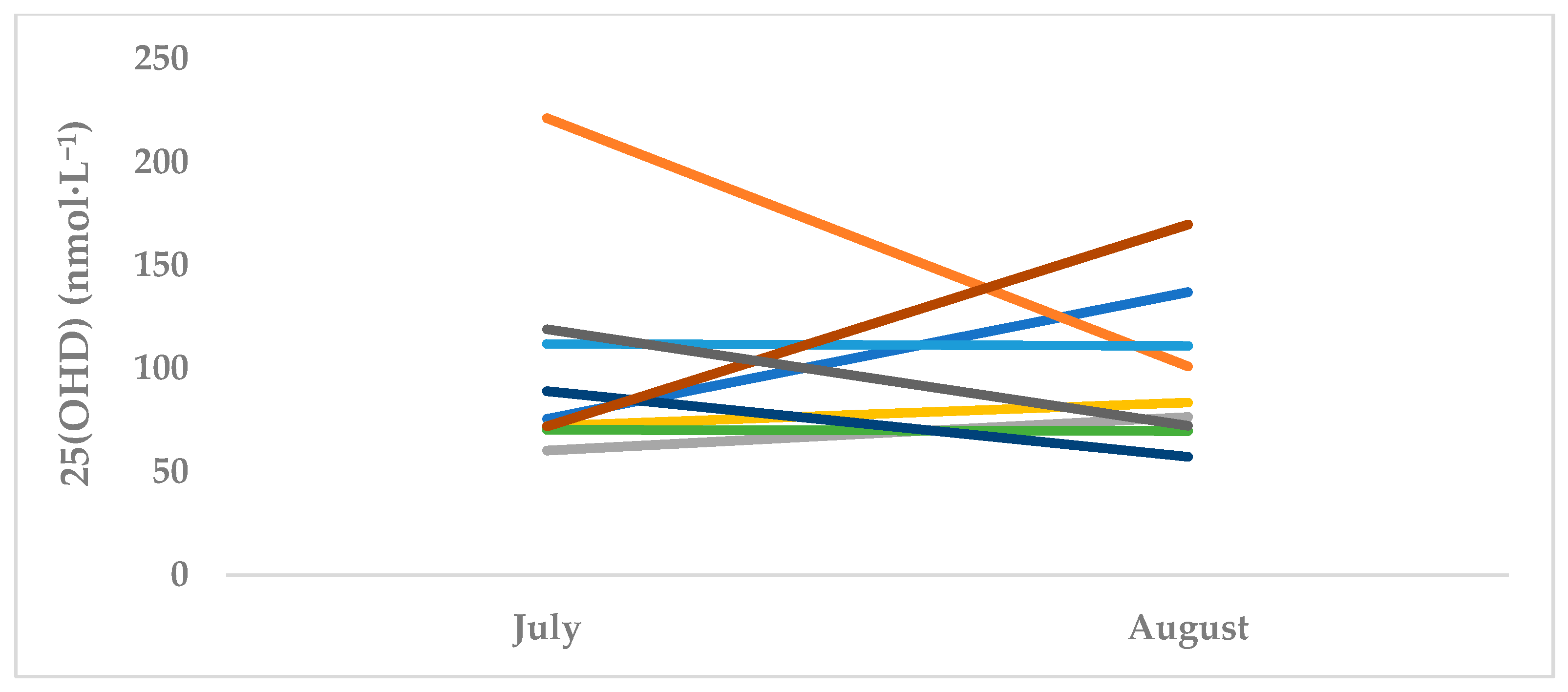
| Characteristics | T1 (Summer Off-season, July) Mean ± SD | T2 (Autumn Pre-season, October) Mean ± SD |
|---|---|---|
| 25(OH)D (nmol·L−1) | 99.1 ± 49.9 | 97.6 ± 36.5 |
| <50 nmol·L−1 | 0 (0%) | 0 (0%) |
| 50–75 nmol·L−1 | 4 (44.4%) | 3 (33.3%) |
| >75 nmol·L−1 | 5 (55.5%) | 6 (66.6%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fields, J.B.; Payne, D.C.; Gallo, S.; Busteed, D.R.; Jones, M.T. Vitamin D Status Differs by Sex, Sport-Season, and Skin Pigmentation among Elite Collegiate Basketball Players. Sports 2019, 7, 239. https://0-doi-org.brum.beds.ac.uk/10.3390/sports7110239
Fields JB, Payne DC, Gallo S, Busteed DR, Jones MT. Vitamin D Status Differs by Sex, Sport-Season, and Skin Pigmentation among Elite Collegiate Basketball Players. Sports. 2019; 7(11):239. https://0-doi-org.brum.beds.ac.uk/10.3390/sports7110239
Chicago/Turabian StyleFields, Jennifer B., Daniel C. Payne, Sina Gallo, Deanna R. Busteed, and Margaret T. Jones. 2019. "Vitamin D Status Differs by Sex, Sport-Season, and Skin Pigmentation among Elite Collegiate Basketball Players" Sports 7, no. 11: 239. https://0-doi-org.brum.beds.ac.uk/10.3390/sports7110239