Epidemiology of Acute Injuries in Surfing: Type, Location, Mechanism, Severity, and Incidence: A Systematic Review




Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Critical Appraisal
2.4. Data Extraction
2.5. Data Synthesis/Analysis
3. Results
3.1. Data Search Results
3.2. Critical Appraisal Results
3.3. Geographical Location of Injury Research
3.4. Study Characteristics and Main Findings
3.5. Injury Incidence Rate and Injury Proportion
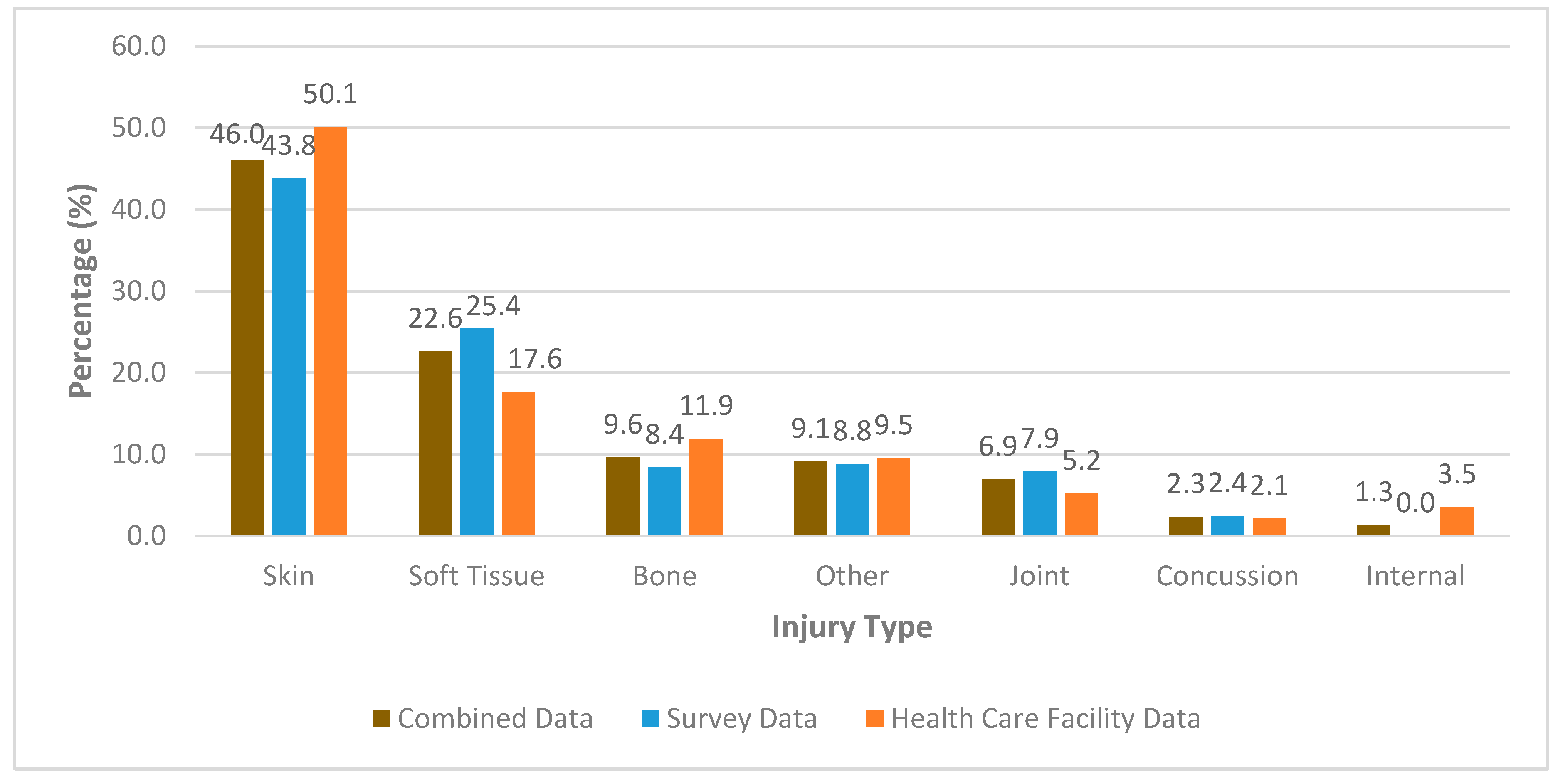
3.6. Type of Injury
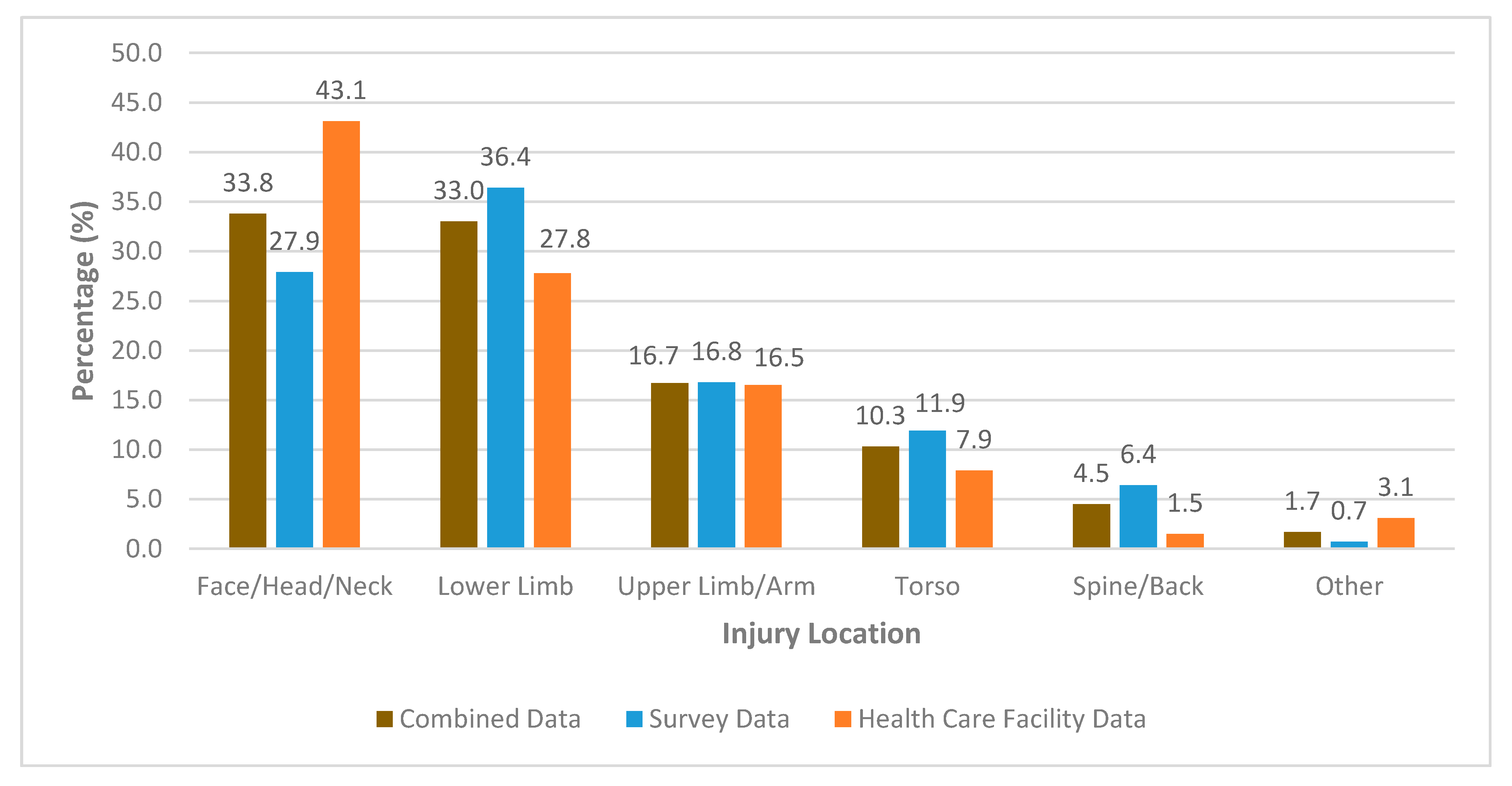
3.7. Location of Injury
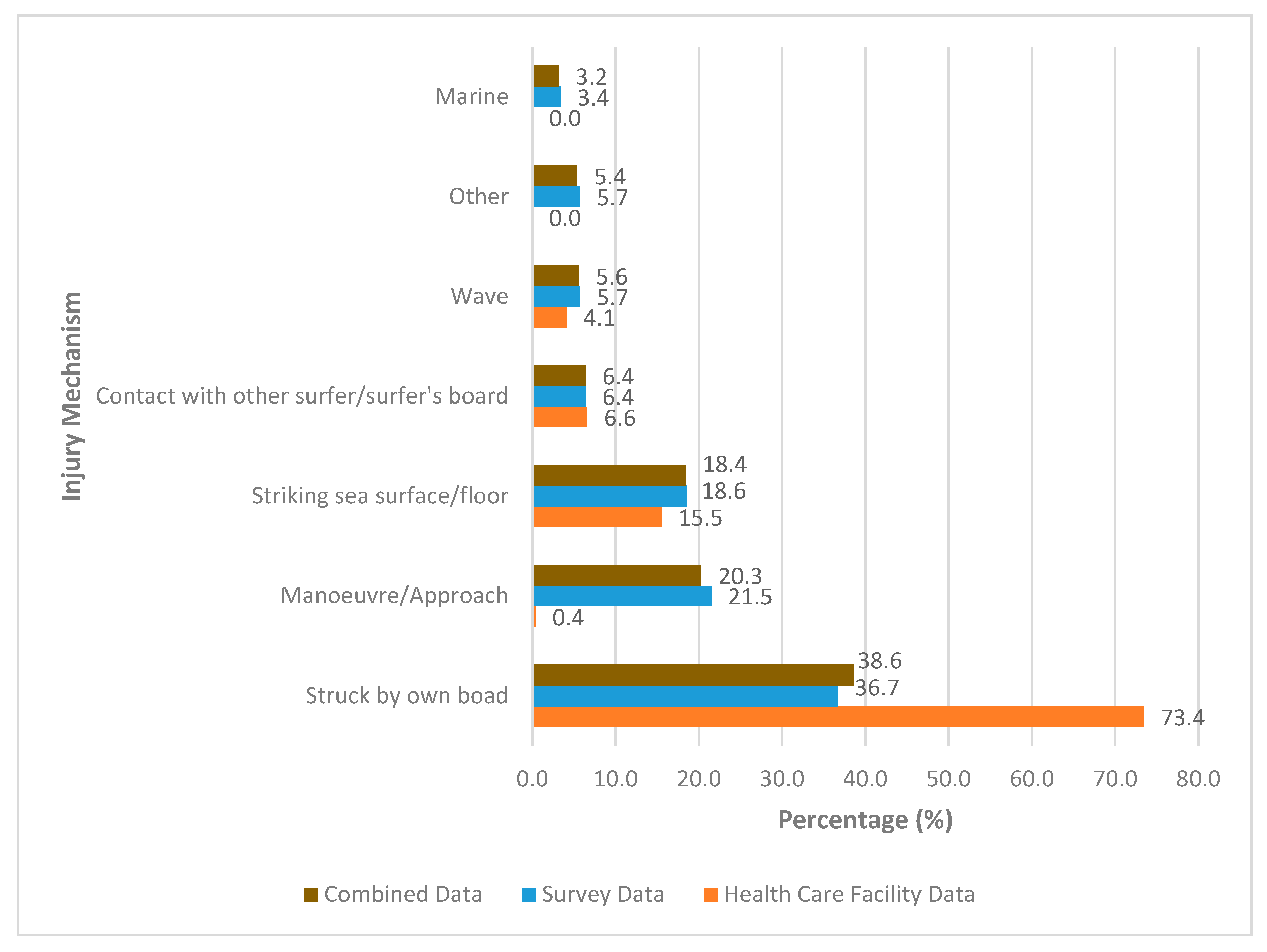
3.8. Mechanism of Injury
4. Discussion
4.1. Injury Incidence Rate and Injury Proportion
4.2. Type of Injury
4.3. Location of Injury
4.4. Mechanism of Injury
4.5. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Yes = 1 (or 2) | No = 0 | Not Applicable (Comment) | |
|---|---|---|---|---|
| Introduction | ||||
| 1 | Were the aims/objectives of the study clear? | √ | ||
| Methods | ||||
| 2 | Was the study design appropriate for the stated aim(s)? | |||
| 3 | Was the sample size justified? | |||
| 4 | Was the target/reference population clearly defined? (Is it clear who the research was about?) | |||
| 5 | Was the sample frame taken from an appropriate population base so that it closely represented the target/reference population under investigation? | |||
| 6 | Was the selection process likely to select subjects/participants that were representative of the target/reference population under investigation? | |||
| 7 | Were measures undertaken to address and categorise non-responders? | |||
| 8 | Were the risk factor and outcome variables measured appropriate to the aims of the study? | |||
| 9 | Were the risk factor and outcome variables measured correctly using instruments/measurements that had been trialled, piloted or published previously? | |||
| 10 | Is it clear what was used to determined statistical significance and/or precision estimates? (e.g. p-values, confidence intervals) | |||
| 11 | Were the methods (including statistical methods) sufficiently described to enable them to be repeated? | |||
| 12 | Was injury classified using body region, type, and stage of injury? (Score = 2) OR was injury classified using one or more of the following: body region, type, and/or stage of injury? (Score = 1) | |||
| 13 | Do the authors define their interpretation of injury? | |||
| 14 | Was an appropriate criteria for injury severity used? | |||
| 15 | Was injury data collected prospectively? (Score = 2) OR was injury data recalled retrospectively? (Score = 1) | |||
| 16 | Was the mechanism of the injury recorded? (Intrinsic and extrinsic factors i.e. seabed, wave height?) | |||
| Results | ||||
| 17 | Were the basic data adequately described? | |||
| 18 | Are there no concerns about non-response bias? | |||
| 19 | If appropriate, was information about non-responders described? | |||
| 20 | Were the results internally consistent? | |||
| 21 | Were the results presented for all the analyses described in the methods? | |||
| Discussion | ||||
| 22 | Were the authors' discussions and conclusions justified by the results? | |||
| 23 | Were the limitations of the study discussed? | |||
| Other | ||||
| 24 | Was there an absence of any funding sources or conflicts of interest that may affect the authors’ interpretation of the results? | |||
| 25 | Was ethical approval or consent of participants obtained? | |||
| Score = | ||||
Appendix B
| Author (Year) | Type | Body Region | Severity | Mechanism |
|---|---|---|---|---|
| Allen et al. (1977) | Fracture (6) 26.1% Laceration (6) 26.1% Contusion (5) 21.7% Other (3) 13% Concussion (1) 4.3% Ligament sprain (1) 4.3% 23 total acute injuries | Head (11) 47.8% Abdomen (5) 21.7% Other (3) 13% Arm (2) 8.7% Knee (1) 4.3% Neck (1) 4.3% | All people were required to admit into hospital with their respective follow-up treatments | Struck by own board (21) 91.3% Striking seafloor (1) 4.3% Manoeuvre (1) 4.3% |
| Base et al. (2007) | Cut-contusion (38) 33.9% Sprain (29) 25.9% Contusion (16) 14.3% Muscular strain (14) 12.5% Burn (9) 8.0% Fracture (6) 5.4% 112 total acute injuries | Lower limbs (64) 57.6% Head (23) 20.7% Upper limbs (13) 11.7% Chest (12) 10.8% | No severity data | Struck by own board (53) 51.4% Manoeuvre (42) 40.7% Striking seafloor (8) 7.7% Mechanism not specified (9) |
| Bazanella et al. (2017) | Skin (83) 46.6% Muscle (50) 28.1% Ligament (26) 14.6% Other (11) 6.2% Joint (6) 3.4% Fracture (2) 1.1% 178 total acute injuries | Lower limbs (80) 44.9% Upper limbs (36) 20.2% Head (33) 18.5% Upper body (29) 16.3% | No severity data | Struck by own board and/or the seabed (72) 40.4% Manoeuvres (50) 28.1% Paddling/duck diving (35) 19.7% Jellyfish * (21) 11.8% |
| Burgess et al. (2018) | Abrasion (48) 16.5% Laceration (46) 15.8% Cramping (38) 13.1% Muscle strain (30) 10.3% Ear infection (27) 9.3% Haematoma (25) 8.6% Joint sprain (17) 5.8% Bone injury (13) 4.5% Tendonitis (7) 2.4% Fracture (6) 2.1% Dislocation (6) 2.1% Concussion (6) 2.1% Tendon rupture (5) 1.7% Peripheral nerve injury (4) 1.4% Cartilage injury (4) 1.4% Dental injury (4) 1.4% Bursitis (3) 1.1% Spinal cord injury (2) 0.7% 291 total acute injuries | Lower back (36) 15.6% Foot (27) 11.7% Knee (27) 11.7% Ankle (25) 10.8% Head (20) 8.7% Hand (7) 8.7% Shoulder (16) 6.9% Wrist (15) 6.5% Hip/groin (15) 6.5% Neck (8) 3.5% Thigh (8) 3.5% Leg (7) 3.0% Chest (6) 2.5% Pelvis (4) 1.7% Elbow (4) 1.7% Arm (2) 0.9% Forearm (2) 0.9% Abdomen (2) 0.9% 231 injuries total | No severity data | Struck by own board (45) 21.5% Underwater turbulence (28) 13.4% Striking seafloor (24) 11.5% Fin chop (18) 8.6% Cut back (17) 8.1% Barrel (14) 6.7% Contact with other surfer (13) 6.2% Leg rope (13) 6.2% Walking on beach/rock/reef (13) 6.2% Arm rope (8) 3.8% Aerial (7) 3.3% Floater (6) 3.0% Marine (3) 1.55% 209 injuries total |
| De Moraes et al. (2007) | Contusion (112) 29% Laceration (89) 23% Burn (89) 23% Others (89) 23% Sprain (35) 9% Dislocation (15) 4% Fracture (0) 0% 387 total acute injuries | Legs (101) 26% Arms (85) 22% Feet (77) 20% Head (62) 16% Torso (58) 15% | Period of absence from sport after injury: None 35% 1 to 6 days 17% 1 to 3 weeks 20% 1 to 3 months 24% 4 to 6 months 5% 7 to 9 months 3% >10 months 2% No answer 5% | Struck by own board (201) 52% Manoeuvres (182) 47% Marine animals * (104) 27% Other injuries * (67) 18% Overtraining * (66) 17% |
| Dimmick et al. (2018) | No injury type data 248 total acute injuries | Head (115) 46.4% Lower limb (69) 27.8% Upper limb (27) 10.9% Spine (21) 8.5% Chest (8) 3.2% Abdomen (8) 3.2% | No severity data | Struck by own board (178) 71.8% Striking seafloor (41) 16.5% Struck by other person’s board (18) 7.3% Wave turbulence (11) 4.4% |
| Furness et al. (2015) | Muscular (288) 31.3% Joint (264) 28.7% Skin (178) 17.2% Bone (113) Nerve (63) 6.9% Marine (27) Other (22) 4% 739 total acute major injuries | Shoulder (121) 16.4% Ankle (108) 14.6% Head (98) 13.3% Knee (95) 10.7% Lower back (70) 9.5% Neck (68) 9.2% Hip (61) 8.4% Ribs/sternum (39) 5.3% Upper back (29) 3.9% Shin/calf (27) 2.8% Wrist/hand (19) 2.6% Elbow (18) 2.4% | Major injuries-required 1 day or more off work and/or surfing and/or the participant required treatment from a health professional Minor injuries-did not interfere with work or surfing, or involve treatment from a health professional | Striking seafloor (124) 16.5% Struck by own board (121) 16.1% Paddling (82) 10.9% Striking surface of sea (80) 10.6% Tube riding (67) 8.9% Take off (55) 7.3% Duck diving (35) 4.6% Aerial (35) 4.6% Struck by others board (30) 4% Re-entry (28) 3.7% Top turn (26) 3.5% Riding face of wave (21) 2.8% Bottom turn (19) 2.5% Cut back (18) 2.4% Floater (12) 1.6% |
| Hay et al. (2009) | Laceration (73) 38.6% Sprain (40) 21.2% Contusion (26) 13.8% Fracture (26) 13.8% Dislocation (24) 12.7% 189 total acute injuries | Head (79) 41.8% Lower limb (35) 18.5% Upper limb (23) 12.2% Shoulder (20) 10.6% Neck (17) 9% Chest/ribs (7) 3.7% Miscellaneous (5) 2.6% Back (4) 2.1% | Minor/moderate injuries - 90% of injuries defined as minor/moderate or allowed for discharge after treatment Major injuries - 10% of injuries required hospitalisation (fractures of the LL and CxSp) | No mechanism of injury data |
| Hohn et al. (2018) | Ligament sprain (63) 38.7% Subluxation (16) 9.8% Other (14) 8.6% Muscle strain (13) 8% Joint (41) 5.8% Tendon tear (7) 4.3% Fracture (6) 3.7% Tendonitis (3) 1.8% 163 total acute injuries | Knee (45) 28% Ankle (36) 22% Shoulder (31) 19% Other * (22) 13% Hip (16) 10% Back (16) 10% | No severity data | No mechanism of injury data |
| Inada et al. (2018) | Ligament (23) Laceration (23) Miscellaneous (12) Fracture (5) Subluxation (3) Meniscal injury (1) 65 total acute injuries | Foot and Ankle (26) 40% Knee (23) 35% Shoulder (4) 6% Head (3) 5% Neck (2) 3% Thigh (2) 3% Lumber spine (1) 2% Abdomen (1) 2% Elbow (1) 2% Finger (1) 2% | No severity data | No mechanism of injury data |
| Klick et al. (2016) | Laceration (844) 40.7% Sprain (299) 14.4% Contusion (267) 12.9% Fracture (246) 11.9% Other (170) 8.2% Internal injury (97) 4.7% Dislocation (93) 4.5% Concussion (56) 2.7% | Lower limb (537) 25.9% Face (478) 23.1% Head/neck (470) 22.7% Upper limb (345) 16.7% Trunk (178) 8.6% Other * (64) 3.1% | No severity data | No mechanism of injury data |
| Lowdon et al. (1983) | Lacerations (138) 41% Sprains/dislocations/strains (119) 35% Fracture (50) 15% Ear perforations (19) 6% Contusions (11) 3% 337 total acute injuries | Head (105) 37% Foot (44) 13.1% Spine (37) 11% Shoulder (21) 6.2% Ear (19) 5.6% Knee (18) 5.3% Lower leg (18) 5.3% Ribs (16) 4.8% Thigh (10) 3% Abdomen (8) 2.4% Groin (8) 2.4% Arm/hand (4) 1.2% | Moderate to severe injuries receiving medical attention or days lost from surfing Surfing days lost: 1 to 3 (n = 92) 4 to 14 (n = 85) 15 to 60 (n = 30) >60 (n = 6) | Struck by own board (153) 45.4% Manoeuvre (50) 14.8% Striking rocks (43) 12.8% Struck by other person’s board (31) 9.2% Paddling (26) 7.7% Other * (13) 3.9% 7.5% of stated injuries were second to surfboard recoil from the leash |
| Lowdon et al. (1987) | Lacerations (84) 45% Sprains/strains (69) 37% Fractures (16) 9% Contusions (8) 4% Ear perforations (6) 3% Dislocations (4) 2% 187 total acute injuries | Head (47) 29% Spine (27) 14.4% Knee (19) 10.2% Arm/elbow/hand (15) 8% Foot (10) 5.3% Leg (8) 4.3% Other * (8) 4.3% Ankle (7) 3.7% Ribs (3) 1.6% Abdomen (3) 1.6% | Moderate to severe receiving medical attention or days lost from surfing) Surfing days lost: 1 to 3 (n = 48) 4 to 14 (n = 69) 15 to 60 (n = 34) >60 (n = 6) | Struck by own board (67) 35.8% Manoeuvre (30) 16% Striking rocks (20) 10.7% Other * (16) 8.6% Struck by other person’s board (13) 7% |
| Minghelli et al. (2017) | Laceration (93) 23.5% Joint injury (86) 21.8% Muscle injury (66) 16.7% Low back pain (51) 12.9% Tendinitis (40) 10.1% Fracture (35) 8.9% Neck pain (21) 5.3%. Others (3) 0.8% 395 total acute injuries | Knee/leg (66) 16.7% Shoulder/arm (61) 15.4% Head (59) 14.9% Lumbar spine (59) 14.9% Ankle (31) 7.8% Cervical spine (27) 6.8% Foot/toes (27) 6.8% Pelvis/thigh (23) 5.8% Wrist/hand/fingers (19) 4.8% Thorax/chest/ribs (12) 3.2% Elbow/forearm (11) 2.9% | No severity data | Struck by own board (107) 27.1% Paddling (71) 17.9% Striking seafloor (67) 17% Manoeuvre (66) 10.6% Cannot answer (42) 10.6% During take-off (19) 4.8% During the wave output 9 (2.3%) Struck by another surfer (8) 2% Duck diving (6) 1.5% |
| Nathanson et al. (2007) | Sprain/strain (45) 39% Laceration (35) 30% Fracture/dislocation (11) 9% Contusion (10) 9% Other (9) 8%. Abrasion (6) 5% 116 total acute injuries | Lower extremity (45) 39% Head/neck (29) 25% Upper extremity (29) 25% Torso (13) 11% | Significant injury - unable to continue surfing, required sutures, or were trans- ported to a hospital (n = 45) | Struck by own board (34) 29% Striking seafloor (28) 24% Paddling/Duck diving/Take off/Manoeuvre (19) 16%, Turbulence of wave (14) 12% |
| Nathanson et al. (2002) | Lacerations (523) 42% Other (236) 19%. Contusions (160) 13% Sprain (180) 12% Fracture (101) 8% Concussion (73) 6%, 1237 total acute injuries | Head/neck (453) 37% Lower extremity (453) 37% Trunk (162) 13% Upper extremity (156) 13% Systemic-hypothermia + near-drowning (13) 1% Other (other 13). | Minor injury – person able to continue surfing after injury Significant injury – person sought medical attention, unable to surf/work/or attend school for >1 day, or was hospitalized | Struck by own board (680) 55%. Striking seafloor (210) 17%. Strunk by other person’s board (148) 12%. Wave turbulence (87) 7%. Manoeuvres (62) 5%. Marine animals (37) 3%. * 62% of all injuries occurred while riding a wave, * 16% unsuccessful take offs, * 16% turning manoeuvres, * 10% getting tubed |
| Taylor et al. (2004) | Survey data Laceration (78) 46.4% Sprain (48) 28.6% Dislocation (18) 10.7% Fracture (15) 8.9% Other (9) 5.4% 165 total acute injuries ED data Laceration (126) 47.2% Other (64) 24% Fracture (38) 14.2% Sprain (33) 12.4% Dislocation (6) 2.2% 267 total acute injuries | Survey data Foot/ankle (30) 17.9% Face (28) 16.7% Leg (24) 14.3% Knee/patella (23) 13.7% Head (16) 9.5% Shoulder (13) 7.7% Back (11) 6.6% Trunk (10) 6% Neck (5) 3% Arm/elbow (4) 2.4% Hand/wrist (4) 2.4% ED data Face (71) 26.6% Head (41) 15.4% Foot/ankle (34) 12.7% Hand/wrist (24) 9% Leg (22) 8.2% Thorax/pelvis (15) 5.6% Shoulder (12) 4.5% Neck (8) 3% Arm/elbow (7) 2.6% Knee (5) 1.9% Back (3) 1.1% | Significant injury - requiring medical attention or time off surfing/work. In the survey group, 113 (67.3%) injuries necessitated time off from either work or surfing | Survey data Struck by board (76) 46.1% Wiping out (61) 37% Striking seafloor (30) 18.2% Jellyfish (1) 0.6% |
| Ulkestad et al. (2013) | Lacerations/abrasions (128) 30.4% Contusions (89) 21.1% Sprains/strains (88) 20.9% Other (65) 15.4% Fractures (42) 10% Concussions (27) 6% Hypothermia (13) 3% Dislocation (9) 2.1% 421 total acute injuries | Head/neck (182) 43% Lower limb not specified (64) 15.2% Torso (54) 13% Foot (30) 7% Knee (27) 6.4% Shoulder (27) 6.4% Hand (19) 4.5% Upper limb not specified (17) 4% | No severity data | Strunk by own board (155) 36.8% Striking seafloor (103) 24.5% Manoeuvres (60) 14.3% Struck by other person’s board (35) 8.4% Wave turbulence (34) 8.1% Low temperature/climate (16) 3.8% Other (12) 2.9% Contact with own leash (7) 1.6% |
| Woodacre, T. et al. (2014) | Cuts/lacerations (104) 31% Contusions and peri-orbital ecchymoses (80.4) 24% Joint/ligament sprains (50) 15% Muscle or tendon rupture/tear (30) 9% Concussion (17) 5% Fractures (10) 3% Teeth injury (3) 1% 335 total injuries | Head/face (81) 24% Neck (15) 4% Back (32) 10% Trunk (22) 7% Hand/wrist (31) 9% Elbow/shoulder (24) 7% Genitalia (11) 3% Hip (13) 4% Knee (44) 13% Ankle/foot (62) 19% | 90% of injuries sustained did not require professional medical attention | Strunk by own board (86) 31% Striking rocks/coral (42) 15% Striking the water (31) 11% Strunk by other person’s board (31) 11% Striking seafloor (19) 7% Strunk by another water vessel (6) 2% Injury by litter (1 injury) Mechanism not specified * (57) 17% |
References
- Warshaw, M. The History of Surfing; Chronicle Books: San Francisco, CA, USA, 2011. [Google Scholar]
- Moran, K.; Webber, J. Surfing Injuries Requiring First Aid in New Zealand, 2007–2012. Int. J. Aquat. Res. Educ. 2013, 7, 192–203. [Google Scholar] [CrossRef] [Green Version]
- Stark, A. Surfing Australia: Annual Report 2013; Surfing Australia: Coolangatta, QLD, 2013. [Google Scholar]
- ISA. International Olympic Committee and ISA Confirm Qualification Process for Surfing Competition at Tokyo 2020; ISA: La Joll, CA, USA, 2018. [Google Scholar]
- Base, L.H.; Alves, M.A.F.; Martins, E.O.; da Costa, R.F. Injuries among professional surfers. Rev. Bras. Med. do Esporte 2007, 13, 251–253. [Google Scholar] [CrossRef] [Green Version]
- Dimmick, S.; Gillett, M.; Buchan, C.; Sheehan, P.; Franks, M.; Ratchford, A.; Porges, K.; Day, R.; Milne, T.; Anderson, S. Prospective analysis of surfing and bodyboard injuries. Trauma 2019, 21, 113–120. [Google Scholar] [CrossRef]
- Bazanella, N.V.; Garrett, J.G.Z.D.A.; Gomes, A.R.S.; Novack, L.F.; Osiecki, R.; Korelo, R.I.G. Influence of practice time on surfing injuries. Fisioter. em Mov. 2017, 30, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Lowdon, B.J.; Pateman, N.A.; Pitman, A.J. Surfboard-riding injuries. Med. J. Aust. 1983, 2, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Ulkestad, G.-E.; Drogset, J.O. Surfing Injuries in Norwegian Arctic Waters. Open Sports Sci. J. 2016, 9, 153–161. [Google Scholar] [CrossRef]
- Taylor, D.M.; Bennett, D.; Carter, M.; Garewal, D.; Finch, C.F. Acute injury and chronic disability resulting from surfboard riding. J. Sci. Med. Sport 2004, 7, 429–437. [Google Scholar] [CrossRef]
- Verhagen, E.; Van Mechelen, W. Sports Injury Research; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- Allen, R.H.; Eiseman, B.; Straehley, C.J.; Orloff, B.G. Surfing injuries at Waikiki. J. Am. Med. Assoc. 1977, 237, 668–670. [Google Scholar] [CrossRef]
- Burgess, A.; Swain, M.S.; Lystad, R.P. An Australian survey on health and injuries in adult competitive surfing. J. Sports Med. Phys. Fit. 2019, 59, 462–468. [Google Scholar] [CrossRef]
- Hohn, E.; Robinson, S.; Merriman, J.; Parrish, R.; Kramer, W. Orthopedic Injuries in Professional Surfers: A Retrospective Study at a Single Orthopedic Center. Clin. J. Sport Med. 2018. [Google Scholar] [CrossRef]
- Inada, K.; Matsumoto, Y.; Kihara, T.; Tsuji, N.; Netsu, M.; Kanari, S.; Yakame, K.; Arima, S. Acute injuries and chronic disorders in competitive surfing: From the survey of professional surfers in Japan. Sports Orthop. Traumatol. 2018, 34, 256–260. [Google Scholar] [CrossRef]
- Bizzini, M.; Dvorak, J. FIFA 11+: An effective programme to prevent football injuries in various player groups worldwide—A narrative review. Br. J. Sports Med. 2015, 49, 577–579. [Google Scholar] [CrossRef] [PubMed]
- de Moraes, G.C.; Guimaraes, A.T.; Gomes, A.R. Analysis of injuries’ prevalence in surfers from Parana seacoast. Acta Ortop. Bras. 2013, 21, 213–218. [Google Scholar]
- Furness, J.; Hing, W.; Walsh, J.; Abbott, A.; Sheppard, J.M.; Climstein, M. Acute injuries in recreational and competitive surfers: Incidence, severity, location, type, and mechanism. Am. J. Sports Med. 2015, 43, 1246–1254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hay, C.S.; Barton, S.; Sulkin, T. Recreational surfing injuries in Cornwall, United Kingdom. Wilderness Environ. Med. 2009, 20, 335–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klick, C.; Jones, C.M.C.; Adler, D. Surfing USA: An epidemiological study of surfing injuries presenting to US EDs 2002 to 2013. Am. J. Emerg. Med. 2016, 34, 1491–1496. [Google Scholar] [CrossRef] [PubMed]
- Lam, T.; Noonan, V.K.; Eng, J.J. A systematic review of functional ambulation outcome measures in spinal cord injury. Spinal Cord 2008, 46, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions. Ann. Intern. Med. 2009, 151, W65. [Google Scholar] [CrossRef] [Green Version]
- Lowdon, B.J.; Pitman, A.J.; Pateman, N.A.; Ross, K. Injuries to international competitive surfboard riders. J. Sports Med. Phys. Fit. 1987, 27, 57–63. [Google Scholar]
- Minghelli, B.; Nunes, C.; Oliveira, R. Injuries in recreational and competitive surfers: A nationwide study in Portugal. J. Sports Med. Phys. Fit. 2017, 58, 1831–1838. [Google Scholar] [CrossRef]
- Nathanson, A.; Haynes, P.; Galanis, D. Surfing injuries. Am. J. Emerg. Med. 2002, 20, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Woodacre, T.; Waydia, S.E.; Wienand-Barnett, S. Aetiology of injuries and the need for protective equipment for surfers in the UK. Injury 2015, 46, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Nathanson, A.; Bird, S.; Dao, L.; Tam-Sing, K. Competitive Surfing Injuries A Prospective Study of Surfing-Related Injuries Among Contest Surfers. Am. J. Sports Med. 2007, 35, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Donoša, K.; Cabral, A. Injuries in surf athletes and the use of safety equipments. Head/Neck 2015, 43, 3. [Google Scholar]
- Nathanson, A.T. Surfing Injuries; Springer: London, UK, 2013. [Google Scholar]
- Jahan, N.; Naveed, S.; Zeshan, M.; Tahir, M.A. How to conduct a systematic review: A narrative literature review. Cureus 2016, 8, e864. [Google Scholar] [CrossRef] [Green Version]
- Furness, J.; Hing, W.; Abbott, A.; Walsh, J.; Climstein, M.; Sheppard, J.M. Retrospective analysis of chronic injuries in recreational and competitive surfers: Injury location, type, and mechanism. Int. J. Aquat. Res. Educ. 2014, 8, 277–287. [Google Scholar] [CrossRef] [Green Version]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open. 2016, 6, e011458. [Google Scholar] [CrossRef] [Green Version]
- Lyons, K.; Radburn, C.; Orr, R.; Pope, R. A profile of injuries sustained by law enforcement officers: A critical review. Int. J. Environ. Res. Public Health 2017, 14, 142. [Google Scholar] [CrossRef] [Green Version]
- Hassan, E. Recall bias can be a threat to retrospective and prospective research designs. Internet J. Epidemiol. 2006, 3, 339–412. [Google Scholar]
- Handler, A.; Kennelly, J. Reducing Racial/Ethnic Disparities in Reproductive and Perinatal Outcomes: The Evidence from Population-Based Interventions; Springer: Boston, MA, USA, 2011. [Google Scholar]
- Rew, L. The systematic review of literature: Synthesizing evidence for practice. J. Spec. Pediatric Nurs. 2011, 16, 64–69. [Google Scholar] [CrossRef]
- Kaminskyj, A.; Frazier, M.; Johnstone, K.; Gleberzon, B.J. Chiropractic care for patients with asthma: A systematic review of the literature. J. Can. Chiropr. Assoc. 2010, 54, 24. [Google Scholar] [PubMed]






| Inclusion Criteria | Example/s |
| Peer-reviewed journal articles | Retrieved from a scholarly journal |
| Surf board riding injury incidence | Studies documenting injury epidemiology: specific to injury incidence, location, types and mechanisms as a direct result of surfing |
| Studies documenting acute injury epidemiology | Injuries definable by a sudden onset of sharp pain or sudden impact |
| Musculoskeletal injury | Laceration, contusion, fracture, sprain/strain, dislocation |
| Exclusion Criteria | Example/s |
| Full text not available | Abstract |
| Full text not available in English | French, Spanish, German |
| Injuries that were not initially sustained whilst-surf board riding | Injuries initially sustained during any activity other than surfing |
| Non-musculoskeletal related injury or illness | Submersion, ocular trauma, exostosis etc. |
| Data from surfing injuries cannot be interpreted independently from other surf-sport injury data | Injury data from surfing and body surfing grouped and inseparable |
| Case series | A study documenting the incidence of surfing related head injuries only |
| Author (Year) | Title | Study Design (Data Source) | Level of Evidence * | Modified AXIS | Percentage | Quality Rating |
|---|---|---|---|---|---|---|
| Final | % | |||||
| Allen et al. (1977) | Surfing injuries at Waikiki | Cross-sectional Retrospective cohort (medical records) | III-2 | 13/24 | 54.2% | Fair |
| Base et al. (2007) | Injuries among professional surfers | Cross-sectional Retrospective cohort (questionnaire) | III-2 | 18/27 | 66.7% | Fair |
| Bazanella et al. (2017) | Influence of practice time on surfing injuries | Cross-sectional Retrospective cohort (questionnaire) | III-2 | 17/27 | 63.0% | Fair |
| Burgess et al. (2018) | An Australian survey on health and injuries in adult competitive surfing | Cross-sectional Retrospective cohort (online survey) | III-2 | 20/27 | 74.1% | Good |
| De Moraes et al. (2007) | Analysis of injuries’ prevalence in surfers from Parana seacoast | Cross-sectional Retrospective cohort (questionnaire) | III-2 | 18/27 | 66.7% | Fair |
| Dimmick et al. (2018) | Prospective analysis of surfing and bodyboard injuries | Cross-sectional Prospective cohort (ED questionnaire) | II | 16/27 | 59.3% | Fair |
| Furness et al. (2015) | Acute injuries in recreational and competitive surfers: incidence, severity, location, type, and mechanism | Cross-sectional Retrospective cohort (online survey) | III-2 | 23/27 | 85.2% | Good |
| Hay et al. (2009) | Recreational surfing injuries in Cornwall, United Kingdom | Cross-sectional Retrospective cohort (ED questionnaire) | III-2 | 17/27 | 63.0% | Fair |
| Hohn et al. (2018) | Orthopedic Injuries in Professional Surfers: A Retrospective Study at a Single Orthopedic Center | Cross-sectional Retrospective cohort (Medical records – WSL) | III-2 | 20/24 | 83.3% | Good |
| Inada et al. (2018) | Acute injuries and chronic disorders in competitive surfing: From the survey of professional surfers in Japan | Cross-sectional Retrospective cohort (Medical records) | III-2 | 15/24 | 62.5% | Fair |
| Klick et al. (2016) | Surfing USA: an epidemiological study of surfing injuries presenting to US Eds 2002 to 2013 | Cross-sectional Retrospective cohort (Medical records–NEISS) | III-2 | 16/24 | 66.7% | Fair |
| Lowdon et al. (1983) | Surfboard-riding injuries | Cross-sectional Retrospective cohort (Reply-paid questionnaire) | III-2 | 17/27 | 63.0% | Fair |
| Lowdon et al. (1987) | Injuries to international competitive surfboard riders | Cross-sectional Retrospective cohort(interviewed questionnaire) | III-2 | 18/27 | 66.7% | Fair |
| Minghelli et al. (2017) | Injuries in recreational and competitive surfers–a nationwide study in Portugal | Cross-sectional Retrospective cohort (interview questionnaire) | III-2 | 22/27 | 81.5% | Good |
| Nathanson et al. (2002) | Surfing injuries | Cross-sectional Retrospective cohort (online survey) | III-2 | 23/24 | 95.8% | Good |
| Nathanson et al. (2007) | Competitive surfing injuries: a prospective study of surfing-related injuries among contest surfers | Cross-sectional Prospective cohort (medical records) | II | 19/27 | 70.4% | Good |
| Taylor et al. (2004) | Acute injury and chronic disability resulting from surfboard riding | Cross-sectional Retrospective cohort (interview questionnaire) | III-2 | 24/27 | 88.9% | Good |
| Ulkestad et al. (2016) | Surfing injuries in Norwegian arctic waters | Cross-sectional Retrospective cohort (online survey) | III-2 | 20/27 | 74.1% | Good |
| Woodacre et al. (2015) | Aetiology of injuries and the need for protective equipment for surfers in the UK | Cross-sectional Retrospective cohort (online survey) | III-2 | 20/27 | 74.1% | Good |
| k = 1.000 | Mean = 75.1% (SD ± 11%) | |||||
| Author (Year) | Data Collection Method | Data Collection Setting | Population Demographics | |||
|---|---|---|---|---|---|---|
| Number of Participants (N=) | Sex (♂/♀) | Competitive Level | ||||
| Allen et al. (1977) | Medical records | Waikiki Kaiser Foundation Hospital (1969–1975) | 24 | 20 years | 33/2 | Recreational surfers |
| Base et al. (2007) | Researcher administered questionnaire | One phase of the Brazilian Professional Surfing Championship (25–26 June 2005) | 32 | 26.5 ± 5.11 years | 32/0 | Professional surfers |
| Bazanella et al. (2017) | Researcher administered questionnaire | Subjects from Paraná coast. | 66 | 26.16 ± 0.72 years | Unspecified | Recreational and professional surfers (min 6 months experience) |
| Burgess et al. (2018) | Online survey | Registered participants of Australian Surfing Titles 2014 in Coffs Harbour (1–18 August) | 227 | 35.0 ± 13.2 years | 77%/23% | Recreational surfers |
| De Moraes et al. (2007) | Paper back survey | Conducted on the beaches of the seacoast cities of Paraná | 60 | 27 ± 6 years | 60/0 | Recreational (surfers with min. 2 years’ experience) |
| Dimmick et al. (2018) | ED – triage questionnaire (prospective) | Six hospitals in South East Queensland, Australia (over 18 months) | 252 | 34 ± 12 years | 89%/11% | Recreational surfers |
| Furness et al. (2015) | Online survey | Advertised to Australian surf websites and local surf clubs (25 October 2012, and 25 March 2013) | 1348 | 35.8 ± 13.1 years | 93.1%/6.9% | Recreational (min. 12 months of experience) |
| Hay et al. (2009) | ED – triage questionnaire | ED (September 2004 to August 2016). | 212 | 27 years | 80%/20% | Unspecified |
| Hohn et al. (2018) | Medical records | Data from the medical director of the WSL(1999 to 2016) | 86 | 28.5 years | 92.6%/7.4% | Professional surfers. |
| Inada et al. (2018) | Medical records | 50 contests of Japan Pro Surfing Tour (2009 to 2016) and professional surfing outpatient clinic (2010 to 2016) | 65 | Unspecified | Unspecified | Professional surfers. |
| Klick et al. (2016) | Medical records | 100 hospital EDs in USA (NEISS injury database; 1 January 2002 to 31 December 2013) | 2072 | 27 years | 81.9%/18.1% | Recreational surfers |
| Lowdon et al. (1983) | Reply-paid questionnaire | Members of the Victorian Branch of the Australian Surfriders Association (March 1982) | 346 | 21.8 ± 5.7 years | Unspecified | Recreational surfers |
| Lowdon et al. (1987) | Questionnaire by interview | International surfing competitors | 86 | 22.4 ± 3.7 years | 89%/11% | Professional surfers |
| Minghelli et al. (2017) | Questionnaire by interview | Unspecified | 1016 | 24.43 ± 11.98 years | 84%/16% | Recreational and professional surfers |
| Nathanson et al. (2002) | Online survey | Advertised in periodicals and websites (May 1998 to August 1999) | 1348 | 28.6 ± 10.6 years | 90%/10% | Recreational and professional surfers. |
| Nathanson et al. (2007) | Medical records (prospective) | 32 surf contests; 10 amateur and 22 pro contests worldwide (1999 to 2005) | 116 | 23.6 ± 7 years | Unspecified | Recreational and professional surfers |
| Taylor et al. (2004) | Questionnaire by interview | Recruited beachside in Victoria (2003) and Victorian Emergency Minimum Database (VEMD) | Survey: 646 VEMD: 276 | Survey: 28.2 ± 7.9 years VEMD: Unspecified | Survey: 90.2%/9.8% VEMD: 83.1%/16.9% | Survey: Unspecified VEMD: Unspecified |
| Ulkestad et al. (2016) | Online survey | Advertised on surfing websites and invitations to members from surfing-Facebook groups | 974 | Unspecified | 71%/29% | Unspecified |
| Woodacre et al. (2015) | Online survey | Distributed to 50 surf clubs across the UK (May 2012 to November 2012);– | 130 | 28 years | 85/45 | Recreational and professional surfers |
| Author (Year) | Total Injuries (N=) | Type (% of Total Injuries) | Body Region (% of Total Injuries) | Mechanism (% of Total Injuries) |
|---|---|---|---|---|
| Allen et al. (1977) | 23 | Laceration (26.1%) | Head (47.8%) | Struck by own board (91.3%) |
| Fracture (26.1%) | - | - | ||
| Base et al. (2007) | 112 | Cut/contusion (33.9%) | Lower limbs (57.6%) | Struck by own board (51.4%) |
| Bazanella et al. (2017) | 178 | Skin (46.6%) | Lower limbs (44.9%) | Struck by own board and/or seabed (40.4%) |
| Burgess et al. (2018) | 291 | Abrasion (16.5%) | Lower back (15.6%) | Struck by own board (21.5%) |
| De Moraes et al. (2007) | 387 | Contusion (29%) | Legs (26%) | Struck by own board (52%) |
| * Dimmick et al. (2018) | 248 | - | Head (46.4%) | Struck by own board (71.8%) |
| Furness et al. (2015) | 512 | Muscular (31.3%) | Shoulder (16.4%) | Striking seafloor (16.5%) |
| Hay et al. (2009) | 189 | Laceration (38.6%) | Head (41.8%) | none given |
| Hohn et al. (2018) | 163 | Ligament sprain (38.7%) | Knee (28%) | none given |
| Inada et al. (2018) | 65 | Ligament (35.1%) | Foot/ankle (40%) | none given |
| Laceration (35.1%) | - | - | ||
| Klick et al. (2016) | 2072 | Laceration (40.7%) | Lower limbs (25.9%) | none given |
| Lowdon et al. (1983) | 337 | Laceration (41%) | Head (37%) | Struck by own board (45.4%) |
| Lowdon et al. (1987) | 187 | Laceration (45%) | Head (29%) | Struck by own board (35.8%) |
| Minghelli et al. (2017) | 395 | Laceration (23.5%) | Knee/leg (16.7%) | Struck by own board (27.2%) |
| * Nathanson et al. (2007) | 116 | Sprain/strain (39%) | Lower extremity (39%) | Struck by own board (29%) |
| Nathanson et al. (2002) | 1237 | Laceration (42%) | Head/neck (37%) | Struck by own board |
| - | Lower extremity (37%) | - | ||
| Taylor et al. (2004) | 165 | Laceration (46.4%) | Foot/ankle (survey) (17.9%) | Struck by own board (46.1%) |
| 267 | Laceration (47.2%) | Face (ED) (26.6%) | - | |
| Ulkestad et al. (2013) | 421 | Lacerations/abrasions (30.4%) | Head/neck (43%) | Struck by own board (36.8%) |
| Woodacre et al. (2014) | 335 | Cuts/laceration (31%) | Head/face (24.2%) | Struck by own board (25.7%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McArthur, K.; Jorgensen, D.; Climstein, M.; Furness, J. Epidemiology of Acute Injuries in Surfing: Type, Location, Mechanism, Severity, and Incidence: A Systematic Review. Sports 2020, 8, 25. https://0-doi-org.brum.beds.ac.uk/10.3390/sports8020025
McArthur K, Jorgensen D, Climstein M, Furness J. Epidemiology of Acute Injuries in Surfing: Type, Location, Mechanism, Severity, and Incidence: A Systematic Review. Sports. 2020; 8(2):25. https://0-doi-org.brum.beds.ac.uk/10.3390/sports8020025
Chicago/Turabian StyleMcArthur, Katherine, Darcy Jorgensen, Mike Climstein, and James Furness. 2020. "Epidemiology of Acute Injuries in Surfing: Type, Location, Mechanism, Severity, and Incidence: A Systematic Review" Sports 8, no. 2: 25. https://0-doi-org.brum.beds.ac.uk/10.3390/sports8020025