
Is the Integration of Additional Eccentric, Balance and Core Muscles Exercises into a Typical Soccer Program Effective in Improving Strength and Postural Stability?



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
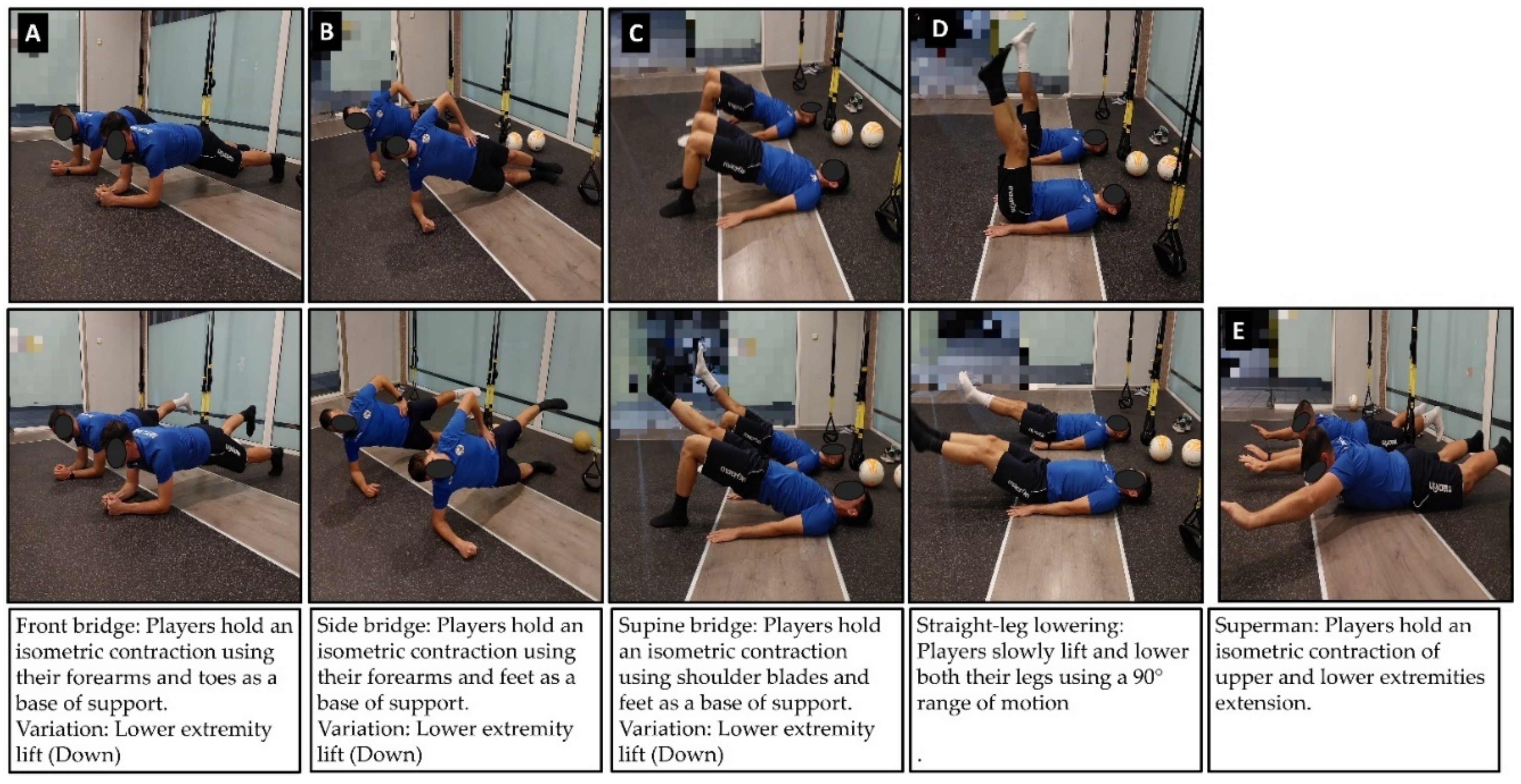
2.3. Intervention
2.4. Statistical Analysis
3. Results
3.1. Hamstring Strength
3.2. Quadriceps Strength
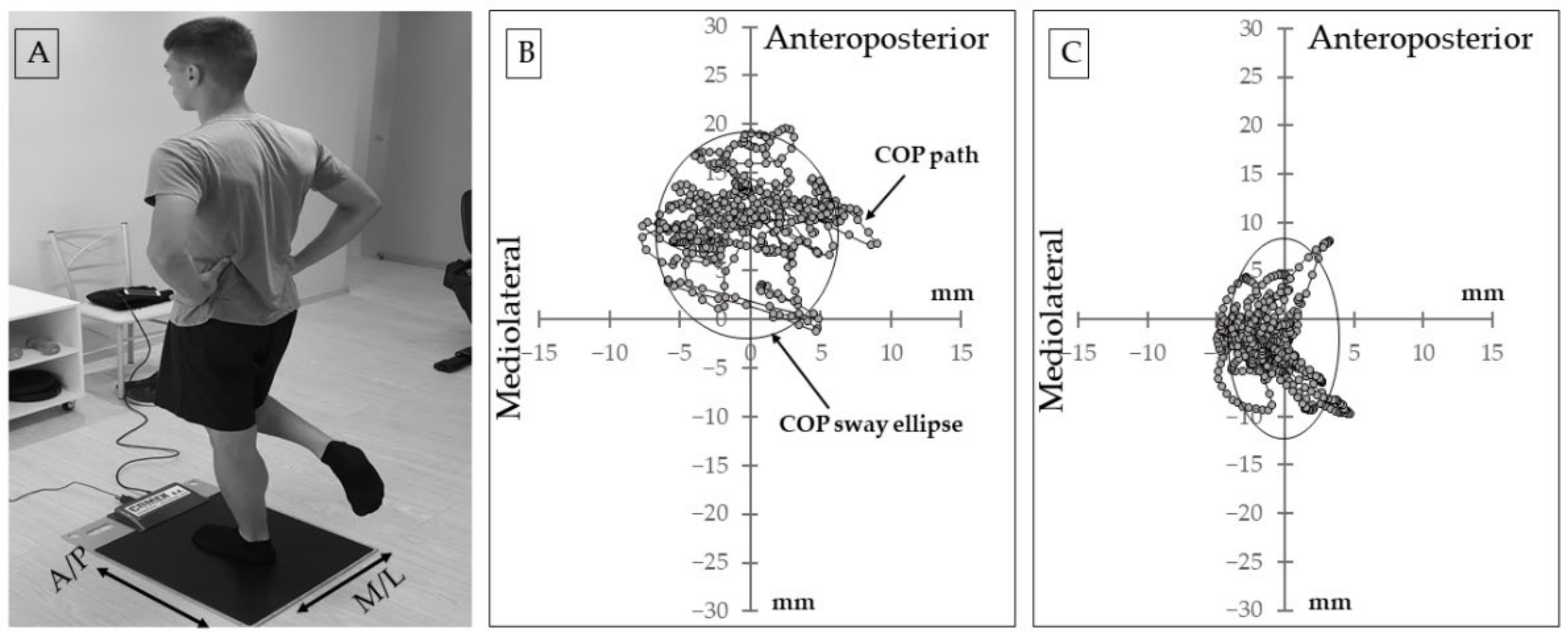
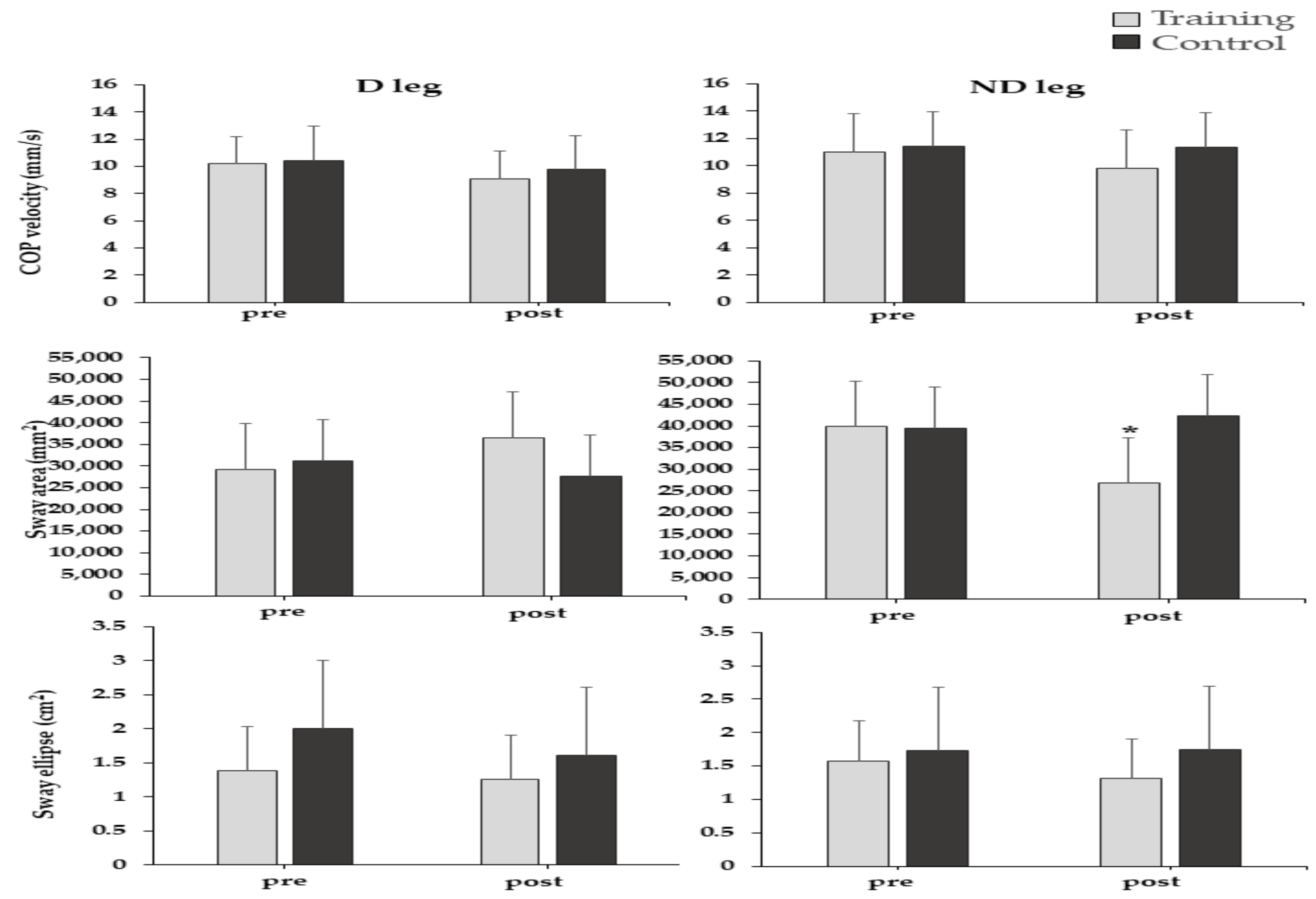
3.3. Single-Leg Balance
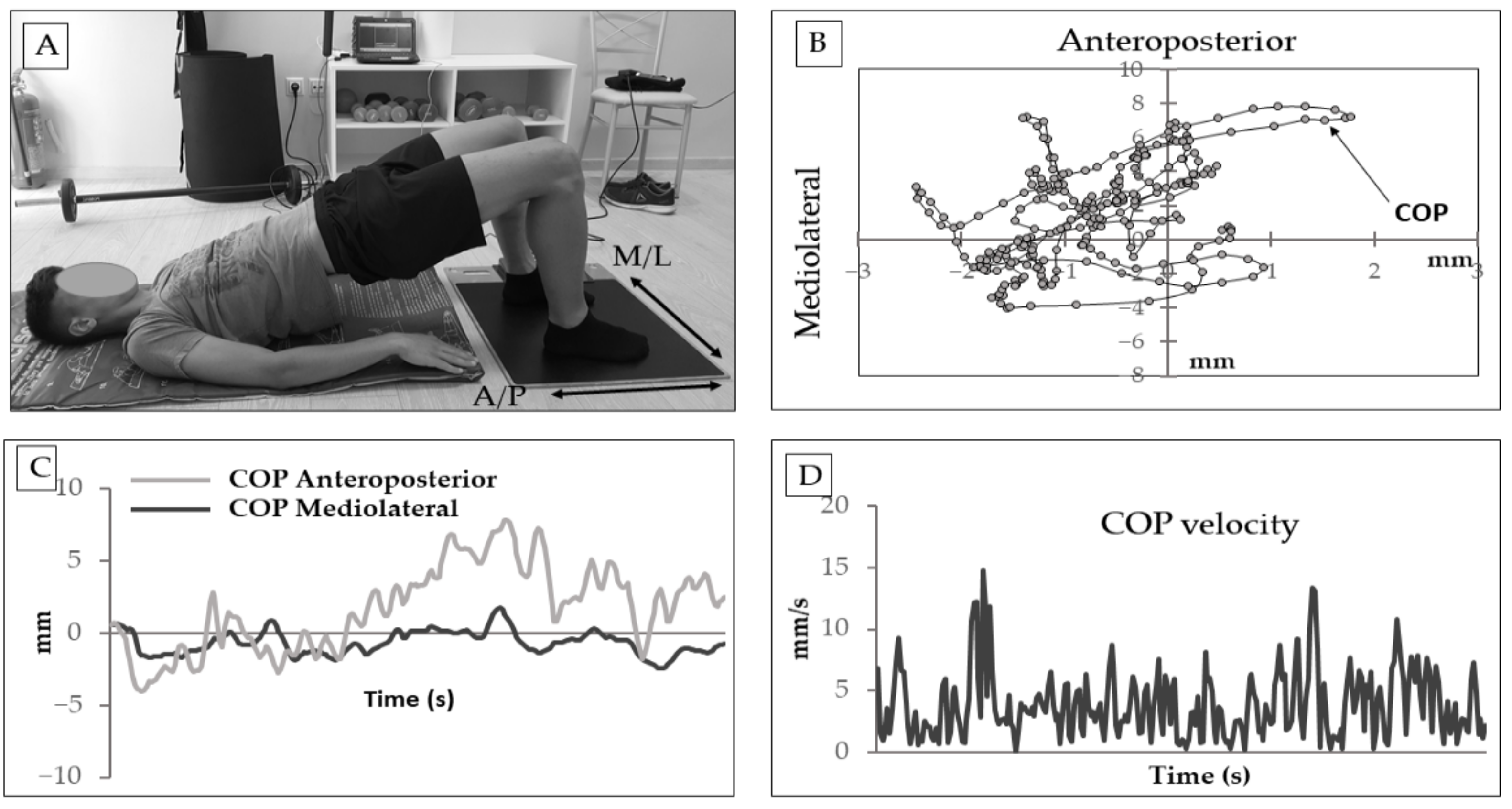
3.4. Bridge Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.A.; Myer, G.D.; Lloyd, R.S. Neuromuscular Risk Factors for Knee and Ankle Ligament Injuries in Male Youth Soccer Players. Sport. Med. 2016, 46, 1059–1066. [Google Scholar] [CrossRef] [Green Version]
- Ekstrand, J.; Krutsch, W.; Spreco, A.; Van Zoest, W.; Roberts, C.; Meyer, T.; Bengtsson, H. Time before return to play for the most common injuries in professional football: A 16-year follow-up of the UEFA Elite Club Injury Study. Br. J. Sports Med. 2019, 54, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Pfirrmann, D.; Herbst, M.; Ingelfinger, P.; Simon, P.; Tug, S. Analysis of injury incidences in male professional adult and elite youth soccer players: A systematic review. J. Athl. Train. 2016, 51, 410–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iga, J.; Fruer, C.S.; Deighan, M.; Croix, M.D.S.; James, D.V.B. Nordic hamstrings exercise—Engagement characteristics and training responses. Int. J. Sports Med. 2012, 33, 1000–1004. [Google Scholar] [CrossRef]
- Mjølsnes, R.; Arnason, A.; Østhagen, T.; Raastad, T.; Bahr, R. A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand. J. Med. Sci. Sport. 2004, 14, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Mendiguchia, J.; Martinez-Ruiz, E.; Morin, J.B.; Samozino, P.; Edouard, P.; Alcaraz, P.E.; Esparza-Ros, F.; Mendez-Villanueva, A. Effects of hamstring-emphasized neuromuscular training on strength and sprinting mechanics in football players. Scand. J. Med. Sci. Sport. 2015, 25, e621–e629. [Google Scholar] [CrossRef]
- Askling, C.; Karlsson, J.; Thorstensson, A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand. J. Med. Sci. Sport. 2003, 13, 244–250. [Google Scholar] [CrossRef]
- Padulo, J.; Laffaye, G.; Ardigò, L.P.; Chamari, K. Concentric and Eccentric: Muscle Contraction or Exercise? J. Hum. Kinet. 2013, 37, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croisier, J.-L.L.; Ganteaume, S.; Binet, J.; Genty, M.; Ferret, J.-M.M. Strength imbalances and prevention of hamstring injury in professional soccer players: A prospective study. Am. J. Sports Med. 2008, 36, 1469–1475. [Google Scholar] [CrossRef]
- Soligard, T.; Nilstad, A.; Steffen, K.; Myklebust, G.; Holme, I.; Dvorak, J.; Bahr, R.; Andersen, T.E. Compliance with a comprehensive warm-up programme to prevent injuries in youth football. Br. J. Sports Med. 2010, 44, 787–793. [Google Scholar] [CrossRef]
- McCall, A.; Carling, C.; Davison, M.; Nedelec, M.; Le Gall, F.; Berthoin, S.; Dupont, G. Injury risk factors, screening tests and preventative strategies: A systematic review of the evidence that underpins the perceptions and practices of 44 football (soccer) teams from various premier leagues. Br. J. Sports Med. 2015, 49, 583–589. [Google Scholar] [CrossRef]
- Huxel Bliven, K.C.; Anderson, B.E. Core Stability Training for Injury Prevention. Sports Health 2013, 5, 514–522. [Google Scholar] [CrossRef] [Green Version]
- Gioftsidou, A.; Malliou, P.; Pafis, G.; Beneka, A.; Godolias, G.; Maganaris, C.N. The effects of soccer training and timing of balance training on balance ability. Eur. J. Appl. Physiol. 2006, 96, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Sebastia-Amat, S.; Ardigò, L.P.; Jimenez-Olmedo, J.M.; Pueo, B.; Penichet-Tomas, A. The Effect of Balance and Sand Training on Postural Control in Elite Beach Volleyball Players. Int. J. Environ. Res. Public Health 2020, 17, 8981. [Google Scholar] [CrossRef]
- Kraemer, R.; Knobloch, K. A soccer-specific balance training program for hamstring muscle and patellar and achilles tendon injuries: An intervention study in premier league female soccer. Am. J. Sports Med. 2009, 37, 1384–1393. [Google Scholar] [CrossRef]
- Hrysomallis, C. Relationship between balance ability, training and sports injury risk. Sport. Med. 2007, 37, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Daneshjoo, A.; Mokhtar, A.H.; Rahnama, N.; Yusof, A. The Effects of Comprehensive Warm-Up Programs on Proprioception, Static and Dynamic Balance on Male Soccer Players. PLoS ONE 2012, 7, e51568. [Google Scholar] [CrossRef]
- Whyte, E.F.; Heneghan, B.; Feely, K.; Moran, K.A.; O’Connor, S. The Effect of Hip Extension and Nordic Hamstring Exercise Protocols on Hamstring Strength. J. Strength Cond. Res. 2019. [Google Scholar] [CrossRef]
- Kouvelioti, V.; Kellis, E.; Kofotolis, N.; Amiridis, I. Reliability of single-leg and double-leg balance tests in subjects with anterior cruciate ligament reconstruction and controls. Res. Sport. Med. 2015, 23, 151–166. [Google Scholar] [CrossRef]
- Santos, T.R.T.; de Andrade, J.A.; da Silva, B.L.; Garcia, A.F.A.; Persichini Filho, J.G.W.; de Ocarino, J.M.; Silva, P.L. Active control stabilization of pelvic position in the transverse plane: An evaluation of soccer players’ performance. Phys. Ther. Sport 2014, 15, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Butowicz, C.M.; Ebaugh, D.D.; Noehren, B.; Silfies, S.P. VALIDATION OF TWO CLINICAL MEASURES OF CORE STABILITY. Int. J. Sports Phys. Ther. 2016, 11, 15–23. [Google Scholar] [PubMed]
- Malliaropoulos, N.; Panagiotis, T.; Jurdan, M.; Vasilis, K.; Debasish, P.; Peter, M.; Tsapralis, K. Muscle and intensity based hamstring exercise classification in elite female track and field athletes: Implications for exercise selection during rehabilitation. Open Access J. Sport. Med. 2015, 6, 209. [Google Scholar] [CrossRef] [Green Version]
- Martuscello, J.M.; Nuzzo, J.L.; Ashley, C.D.; Campbell, B.I.; Orriola, J.J.; Mayer, J.M. Systematic Review of Core Muscle Activity During Physical Fitness Exercises. J. Strength Cond. Res. 2013, 27, 1684–1698. [Google Scholar] [CrossRef] [PubMed]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [Green Version]
- Delextrat, A.; Bateman, J.; Ross, C.; Harman, J.; Davis, L.; Vanrenterghem, J.; Cohen, D.D. Changes in Torque-Angle Profiles of the Hamstrings and Hamstrings-to-Quadriceps Ratio After Two Hamstring Strengthening Exercise Interventions in Female Hockey Players. J. Strength Cond. Res. 2020, 34, 396–405. [Google Scholar] [CrossRef]
- Brughelli, M.; Cronin, J. Altering the Length-Tension Relationship with Eccentric Exercise Implications for Performance and Injury. Sports Med. 2007, 37, 807–826. [Google Scholar] [CrossRef]
- Brito, J.; Figueiredo, P.; Fernandes, L.; Seabra, A.; Soares, J.M.; Krustrup, P.; Rebelo, A. Isokinetic strength effects of FIFA’s “the 11+” injury prevention training programme. Isokinet. Exerc. Sci. 2010, 18, 211–215. [Google Scholar] [CrossRef]
- Douglas, J.; Pearson, S.; Ross, A.; McGuigan, M. Chronic Adaptations to Eccentric Training: A Systematic Review. Sport. Med. 2017, 47, 917–941. [Google Scholar] [CrossRef]
- English, K.L.; Loehr, J.A.; Lee, S.M.C.; Smith, S.M. Early-phase musculoskeletal adaptations to different levels of eccentric resistance after 8 weeks of lower body training. Eur. J. Appl. Physiol. 2014, 114, 2263–2280. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.; Bryant, A.; Culgan, J.P.; Hartley, B. The effects of eccentric hamstring strength training on dynamic jumping performance and isokinetic strength parameters: A pilot study on the implications for the prevention of hamstring injuries. Phys. Ther. Sport 2005, 6, 67–73. [Google Scholar] [CrossRef]
- Heleno, L.R.; da Silva, R.A.; Shigaki, L.; Araújo, C.G.A.; Coelho Candido, C.R.; Okazaki, V.H.A.; Frisseli, A.; Macedo, C. de S.G. Five-week sensory motor training program improves functional performance and postural control in young male soccer players—A blind randomized clinical trial. Phys. Ther. Sport 2016, 22, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Barone, R. Soccer players have a better standing balance in nondominant one-legged stance. Open Access J. Sport. Med. 2010, 2, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pau, M.; Loi, A.; Pezzotta, M.C. Does sensorimotor training improve the static balance of young volleyball players? Sport. Biomech. 2012, 11, 97–107. [Google Scholar] [CrossRef]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35 (Suppl. 2), ii7–ii11. [Google Scholar] [CrossRef] [Green Version]
- Konrad, P.; Schmitz, K.; Denner, A. Neuromuscular Evaluation of Trunk-Training Exercises. J. Athl. Train. 2001, 36, 109–118. [Google Scholar] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concentric Peak Torque | Eccentric Peak Torque | |||||
|---|---|---|---|---|---|---|
| Before | After | Before | After | |||
| Group | x ± SD | x ± SD | x ± SD | x ± SD | ||
| 240°/s, Dominant Leg | % change | 240°/s, Dominant Leg | % change | |||
| Training | 90.77 ± 15.03 | 95.39 ± 16.14 | 5.09 ± 7.38 | 185.22 ± 35.88 | 197.02 ± 25.05 | 6.37 ± 30.18 |
| Control | 88.42 ± 15.27 | 87.04 ± 20.61 | −1.56 ± 34.97 | 187.24 ± 30.01 | 186.41 ± 30.55 | −0.42 ± 1.79 |
| 240°/s, Non-dominant Leg | 240°/s, Non-dominant Leg | |||||
| Training | 87.14 ± 21.57 | 88.49 ± 13.76 | 1.55 ± 36.20 | 173.51 ± 39.57 | 187.04 ± 19.39 | 7.80 ± 50.99 |
| Control | 84.12 ± 11.04 | 86.77 ± 13.97 | 3.15 ± 26.53 | 171.60 ± 24.51 | 179.77 ± 40.70 | 4.76 ± 63.19 |
| 180°/s, Dominant Leg | 180°/s, Dominant Leg | |||||
| Training | 101.37 ± 19.67 | 103.39 ± 18.45 | 1.99 ± 6.20 | 180.73 ± 31.80 | 189.45 ± 40.01 | 4.82 ± 25.81 |
| Control | 107.21 ± 25.32 | 101.3 ± 16.79 | −5.51 ± 33.68 | 186.94 ± 39.43 | 183.28 ± 41.20 | −1.96 ± 4.48 |
| 180°/s, Non-dominant Leg | 180°/s, Non-dominant Leg | |||||
| Training | 96.61 ± 19.43 | 101.72 ± 18.47 | 5.29 ± 4.94 | 176.51 ± 38.46 | 195.81 ± 31.81 | 10.93 ± 17.29 |
| Control | 113.63 ± 27.28 | 109.85 ± 30.44 | −3.33 ± 11.58 | 174.94 ± 28.37 | 178.75 ± 34.2 | 2.18 ± 20.54 |
| 30°/s, Dominant Leg | 30°/s, Dominant Leg | |||||
| Training | 153.80 ± 51.86 | 149.62 ± 43.95 | −2.72 ± 14.95 | 199.88 ± 45.40 | 210.15 ± 39.50 | 5.14 ± 12.99 |
| Control | 157.78 ± 32.99 | 144.56 ± 36.37 | −8.38 ± 10.24 | 214.65 ± 39.61 | 211.66 ± 48.81 | −1.39 ± 23.22 |
| 30°/s, Non-dominant Leg | 30°/s, Non-dominant Leg | |||||
| Training | 139.55 ± 34.24 | 177.57 ± 58.56 * | 27.24 ± 71.02 | 188.31 ± 39.96 | 198.90 ± 39.01 | 5.62 ± 2.37 |
| Control | 148.3 ± 37.15 | 127.94 ± 50.97 | −13.33 ± 37.20 | 188.98 ± 29.13 | 181.4 5± 47.30 | −3.98 ± 62.37 |
| Concentric Peak Torque | Eccentric Peak Torque | |||||
|---|---|---|---|---|---|---|
| Before | After | Before | After | |||
| Group | x ± SD | x ± SD | x ± SD | x ± SD | ||
| 240°/s, Dominant Leg | % change | 240°/s, Dominant Leg | % change | |||
| Training | 128.89 ± 31.66 | 146.07 ± 22.63 * | 13.32 ± 28.52 | 328.74 ± 59.31 | 292.64 ± 115.41 | 10.97 ± 93.89 |
| Control | 137.99 ± 21.31 | 132.48 ± 14.35 | −3.99 ± 32.66 | 306.16 ± 70.35 | 295.41 ± 81.67 | 3.59 ± 16.15 |
| 240°/s, Non-dominant Leg | 240°/s, Non-dominant Leg | |||||
| Training | 135.81 ± 24.14 | 146.46 ± 21.55 | 7.84 ± 10.72 | 309.70 ± 81.58 | 320.43 ± 77.51 | 3.55 ± 4.93 |
| Control | 129.4 ± 20.20 | 127.01 ± 23.29 | −1.85 ± 15.29 | 312.21 ± 66.19 | 298.06 ± 69.73 | 4.48 ± 4.54 |
| 180°/s, Dominant Leg | 180°/s, Dominant Leg | |||||
| Training | 160.16 ± 28.98 | 174.33 ± 27.17 | 8.84 ± 6.24 | 312.56 ± 69.22 | 298.04 ± 89.38 | 4.64 ± 28.98 |
| Control | 163.19 ± 22.16 | 160.68 ± 18.99 | −1.53 ± 14.3 | 289.92 ± 80.84 | 286.77 ± 93.50 | 1.03 ± 16.25 |
| 180°/s, Non-dominant Leg | 180°/s, Non-dominant Leg | |||||
| Training | 162.01 ± 18.35 | 169.38 ± 24.06 | 4.54 ± 31.11 | 309.85 ± 67.64 | 290.88 ± 69.35 | 6.14 ± 2.98 |
| Control | 156.45 ± 20.87 | 156.07 ± 21.93 | −0.24 ± 5.08 | 303.53 ± 67.44 | 290.49 ± 77.56 | 4.29 ± 14.92 |
| 30°/s, Dominant Leg | 30°/s, Dominant Leg | |||||
| Training | 276.77 ± 54.06 | 273.20 ± 42.68 | −1.28 ± 21.05 | 369.86 ± 47.55 | 373.4 ± 33.12 | 1.08 ± 29.78 |
| Control | 263.71 ± 39.35 | 253.55 ± 50.20 | −3.85 ± 25.65 | 333.91 ± 54.27 | 329.02 ± 83.33 | 1.20 ± 53.53 |
| 30°/s, Non-dominant Leg | 30°/s, Non-dominant Leg | |||||
| Training | 277.52 ± 46.11 | 277.94 ± 38.37 | 0.15 ± 16.78 | 365.15 ± 41.71 | 372.62±50.48 | 1.91 ± 21.95 |
| Control | 256.57 ± 33.45 | 244.89 ± 43.57 | −4.55 ± 30.25 | 352.96 ± 60.59 | 334.98 ± 62.10 * | 5.11 ± 3.33 |
| Before | After | Group × Time Interaction | ||
|---|---|---|---|---|
| Group | x ± SD | x ± SD | ||
| TCOP (mm), Dominant Leg | % change | |||
| Training | 305.61 ± 89.80 | 272.91 ± 60.97 | −10.7 ± 32.10 | NS |
| Control | 313.04 ± 95.26 | 287.9 ± 66.73 | −8.03 ± 29.94 | |
| TCOP (mm), Non-dominant Leg | ||||
| Training | 330.09 ± 71.01 | 292.56 ± 102.64 | −11.6 ± 44.54 | NS |
| Control | 342.74 ± 74.18 | 339.55 ± 91.77 | −1.07 ± 23.71 | |
| SDa (mm), Dominant Leg | ||||
| Training | 0.41 ± 0.10 | 0.34 ± 0.11 | −17.07 ± 11.13 | NS |
| Control | 0.36 ± 0.08 | 0.34 ± 0.05 | −5.55 ± 37.5 | |
| SDa (mm), Non-dominant Leg | ||||
| Training | 0.39 ± 0.10 | 0.35 ± 0.14 | −10.25 ± 10.40 | NS |
| Control | 0.40 ± 0.08 | 0.39 ± 0.09 | −2.50 ± 12.50 | |
| SDm (mm), Dominant Leg | ||||
| Training | 0.29 ± 0.11 | 0.23 ± 0.09 | −20.68 ± 18.18 | NS |
| Control | 0.36 ± 0.38 | 0.22 ± 0.06 | −38.88 ± 54.21 | |
| SDm (mm), Non-dominant Leg | ||||
| Training | 0.30 ± 0.07 | 0.23 ± 0.07 | −23.33 ± 10.31 | NS |
| Control | 0.31 ± 0.09 | 0.25 ± 0.07 | −19.35 ± 22.22 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dafkou, K.; Sahinis, C.; Ellinoudis, A.; Kellis, E. Is the Integration of Additional Eccentric, Balance and Core Muscles Exercises into a Typical Soccer Program Effective in Improving Strength and Postural Stability? Sports 2021, 9, 147. https://0-doi-org.brum.beds.ac.uk/10.3390/sports9110147
Dafkou K, Sahinis C, Ellinoudis A, Kellis E. Is the Integration of Additional Eccentric, Balance and Core Muscles Exercises into a Typical Soccer Program Effective in Improving Strength and Postural Stability? Sports. 2021; 9(11):147. https://0-doi-org.brum.beds.ac.uk/10.3390/sports9110147
Chicago/Turabian StyleDafkou, Konstantinos, Chrysostomos Sahinis, Athanasios Ellinoudis, and Eleftherios Kellis. 2021. "Is the Integration of Additional Eccentric, Balance and Core Muscles Exercises into a Typical Soccer Program Effective in Improving Strength and Postural Stability?" Sports 9, no. 11: 147. https://0-doi-org.brum.beds.ac.uk/10.3390/sports9110147