Exploring the Impact of Medical Brain Drain on Child Health in 188 Countries over 2000–2015

Interdisciplinary Studies Field Major, University of California Berkeley, Berkeley, CA 94720-2922, USA
Societies 2020, 10(4), 73; https://0-doi-org.brum.beds.ac.uk/10.3390/soc10040073
Submission received: 23 August 2020
/
Revised: 13 September 2020
/
Accepted: 17 September 2020
/
Published: 24 September 2020
Abstract
:Medical brain drain has been a policy concern in recent years when many countries are struggling with health workforce shortages. Some suggest that wealthy countries only exacerbate this problem by recruiting internationally trained health professionals. Little research has considered the impact of medical brain drain on child health in the sending society, and the few empirical analyses that exist find no conclusive evidence. To fill this gap, I test the underlying mechanisms through which medical brain drain may affect child health in scores of countries. I use a panel dataset covering 188 countries over the period 2000–2015. The findings from fixed-effects regression models suggest that medical brain drain negatively affects child health and that there is a curvilinear relationship between the two. The effects on child health are stronger in countries approximately in the middle of the medical brain drain scale, and weaker on both ends. The implications of the findings for policy and future research are highlighted.
1. Introduction
The international migration of doctors and nurses has been a policy concern in recent years when many resource-poor countries are struggling with health workforce shortages [1,2]. Over the past decades, the migration flows have increased in scale from low- and middle-income countries to high-income countries due to market liberalization [3,4]. The current COVID-19 pandemic and economic crisis have worsened resource shortages, including health workforce shortages, globally and, more importantly, in resource-poor countries [5,6]. The World Health Organization (WHO) has estimated that 18 million more doctors, midwives, nurses, and support workers are needed to achieve the sustainable development goal of universal health coverage (UHC) by 2030 in low- and lower-middle-income countries [7]. Using health workforce data from the WHO Global Health Observatory for 165 countries over 1990–2013, a 2017 study has projected that global demand for health workers will rise to 80 million by 2030 with the supply of 65 million health workers over the same period [8]. It argues that due to economic and population growth and aging, the demand for health workers will be highest among upper-middle-income countries, while lower-middle-income countries will face acute shortages because their demand will exceed supply. By contrast, in many low-income countries, demand may stay below projected supply, as they will struggle economically to employ more health workers.
According to the WHO, sub-Saharan Africa, which shares more than 24 percent of the global burden of disease, has access to only 3 percent of health workers. In contrast, the Americas share only 10 percent of the global burden of disease but have 37 percent of the world’s health workers [2]. The WHO claims that the global inequity in health systems arising from health workforce shortages is more pronounced than the inequity in population health between rich and poor countries. Wealthy countries have not done enough to address the global shortage of health workers. Some even suggest that they only exacerbate this problem by recruiting internationally trained health professionals [9]. The failure of rich countries to educate an adequate number of their own health workers to serve in the domestic health systems leads to their reliance on and recruitment of large numbers of health workers from low- and middle-income countries, contributing to the extreme health workforce shortages in these countries [10].
The international migration of health workers may affect health outcomes through its negative effects on health systems in the sending society. Due to the increased rates of emigration, those health workers who remain in the health system with inadequate numbers may experience added stress and greater workloads. Consequently, they are more likely to neglect public sector responsibilities and find work in the private sector [11]. More directly, the migration of health workers may threaten the functioning of the health system by causing a shortage of doctors, nurses, and support workers [12]. Evidence suggests that health suffers when health workers are scarce [13,14]. More specifically, medical brain drain (MBD) is found to increase child mortality [15]. However, there are mixed findings in extant empirical research. For example, a pioneering study by Bhargava, Docquier, and Moullan finds that MBD has no significant effects on infant and child mortality and that mortality rates are negatively associated with the number of doctors per capita after adult literacy rates exceed 60 percent [16]. But the importance of literacy and physicians per capita does not hold for higher DPT and measles vaccination rates. In contrast, some studies find that countries with a higher density of health workers attain higher levels of measles vaccination and antenatal care coverage [17,18].
High vacancy rates inevitably lead to inadequate coverage, causing population health needs to remain unmet. However, many argue that vacancy rates are only one way of demonstrating shortages and may not give a true reflection of the capacity of the health system to absorb all the migrant health workers if they were to return to their home countries [19,20]. The capacity of the public health system is much weaker in low-income countries compared to middle- or high-income countries. Whereas the Americas spend more than 50 percent of the world’s financial resources for health, the African region spends less than 1 percent, even with loans and grants from abroad. Of this 1 percent, a country usually devotes just over 42 percent of total public health expenditure to paying its health workforce [2]. Wages are higher in the private sector, which is estimated by the WHO as 50 percent of the total health expenditure in a typical country. Consequently, health worker density is generally highest in urban centers where there are greater earning opportunities due to the existence of more private health clinics and teaching hospitals, and a population that can afford to pay for health services. Higher wages, training, and earning prospects, among other factors, also pull health professionals from developing countries to developed countries [21,22]. Thus, the maldistribution of doctors and other health workers who are over-represented in urban areas, in the private sector, and in wealthier countries, leave those in rural, poor, and marginalized communities and resource-poor countries underserved.
A growing literature claims that the international migration of health workers may have a positive economic and health impact on sending countries. This impact works mainly through the remittances migrant workers send to their families in their home country. Arguably, remittances may enable receiving families to obtain better healthcare for young children [23]. The brain gain literature also claims that greater migration prospects can provide incentives to current and would-be health professionals to acquire higher qualifications and medical training in the home country [24]. Against this claim, many argue that although remittances provide some compensation for sending countries, it is most probable that those sent by migrant health professionals are not directly reinvested in the training of new medical students and overall human capital development for the health system [25]. A 2011 study estimates that the emigration of health workers from sub-Saharan Africa costs the region, on average, US $2.17 billion annually [26]. Another study in 2006 estimates that the total cost of educating a physician from primary school until earning a medical degree is nearly US $66,000 in Kenya, and the government loses a return on investments worth US $517,000 if the physician leaves the country to practice abroad [27]. These huge costs outweigh the economic benefits of health workers’ emigration [28]. The developing countries that are training health professionals but losing many of them to high-income countries ultimately end up with a net loss of human capital in the health system. This shortage might have negative implications for coverage of and access to healthcare services in the long run.
Healthcare migration prospects are not equal for all countries. The demand for migrant health professionals in destination countries depends on several factors, including political factors such as the concerns for security, demographic factors like birth rates and aging population, and economic factors concerning domestic labor market conditions [29,30,31]. Wealthy countries that recruit foreign-trained health workers, such as Australia, Austria, Canada, Denmark, France, Switzerland, the United Kingdom, and the United States, do not recognize educational credentials from all countries. Credential assessment in each country usually takes into consideration the content of foreign education (whether it is relevant to the needs of their labor market), the linguistic ability of the health worker in the recruiting country’s language (most often English or French), and the entry procedures in some trades and professions [32]. Unfamiliarity with foreign degrees and work experience among employers may also play a role [33]. Due to the nonrecognition of or unfamiliarity with foreign credentials by employers and regulatory professional and trade bodies, certain countries represent less than others in the health workforce of a host country [34,35,36,37]. Consequently, it is more likely that medical brain drain rates are higher in countries with recognized credentials, relevant content of education, and the matching linguistic ability of health workers.
Sending countries vary in capacity to provide employment to health workers and deliver health services to all people. Levels of economic development may affect countries’ employment and service delivery capacity in the health sector. Levels of economic development may also affect countries’ capacity to cope with the shortages in the health workforce and effectively deal with the resultant consequences on population health. Studies find that higher levels of economic development have positive effects on population health [38,39]. Although most countries in the past two decades have significantly reduced child mortality rates due to global efforts like the Millennium Development Goals (MDGs) and improvement in socioeconomic status and public health measures, many still face challenges to deliver health services due to health workforce shortages. Specifically, poorer countries lack the infrastructural and financial resources to educate and retain their health workers, as many of them emigrate abroad for higher wages [40]. However, the rates of emigration remain low in poorer countries, since most health workers lack financial resources and a preexisting social network deemed important for migrating to a new destination and settling there [41,42]. In contrast, the rates of emigration are higher in middle-income countries, but they face fewer constraints from healthcare migration because they are better able to fill the loss by training and recruiting more health workers [43,44]. High-income countries also face the challenge of an increased international migration of health workers, both across high-income countries and between developing countries and high-income countries [1]. While high-income countries have the resources to recruit foreign-trained health workers, the situation for the low- and lower-middle-income countries is dire because the emigration rates of health workers in these countries are arguably high and at the same time, they lack resources to fill the shortages in their health workforce [45,46,47]. From this scenario, it can be hypothesized that the relationship between medical brain drain and health is not linear; rather, it can be quadratic, with stronger effects of medical brain drain on health among countries approximately in the middle of the medical brain-drain scale, and weaker effects on both ends.
This study tests the quadratic relationship between doctors’ migration and child health using empirical evidence from 188 countries over 16 years (2000–2015). It also estimates the economic benefits of healthcare migration—the effect of remittances—on child health to assess the claims of medical brain gain proponents. The findings of this study are expected to inform policy on how to better manage healthcare migration nationally and globally.
2. Materials and Methods
I have created a panel dataset using the OECD database on the foreign-trained doctors in OECD countries by their country of origin over 2000–2015 [48]. A major issue with the OECD data is that a large stock of foreign-trained doctors is classified as “Others (not elsewhere classified)”, meaning the country of origin is not known for these doctors. The emigration stock by the country of origin is thus summed up yearly from 29 OECD countries for the foreign-trained doctors whose country of origin is known. This means that the data does not include the stock of foreign-trained doctors in non-OECD countries such as the Middle Eastern countries, where a sizable stock of foreign-trained doctors is present. Accepting this caveat, I calculate the relative measure of medical brain drain rate as defined by Bhargava and Docquier [49]. The relative measure is as follows:
where Mit denotes the stock of doctors from country i working abroad in time t, and Pit denotes the number of doctors working in the home country i during the same period. In addition to the OECD data on the stock of foreign-trained doctors, I have used the WHO data on doctors per thousand people as well as the World Bank data on total population by country and year to calculate medical brain drain [50,51]. Thus, this measure includes only doctors’ emigration from the country of training, but not the emigration of nurses, midwives, dentists, or medical technicians. The values of medical brain drain range from 0 to 1 where 1 means 100 percent.
I have used two measures of child health—infant mortality and under-five child mortality—because the most immediate health effect of medical brain drain should arguably be observed on young children who are the most vulnerable population in any country. Bhargava, Docquier, and Moullan also used these two measures in addition to child vaccination [16]. In most countries, nurses and immunization workers administer child vaccination, so doctors’ emigration may not directly affect the program. For this reason, I did not use child vaccination as a dependent variable. The data on my dependent variables—infant mortality and under-five child mortality per thousand live births—come from the World Development Indicators (WDI) database compiled by the World Bank [51].
I have controlled for several country-level variables that commonly affect child health and are related to healthcare migration. The data on the following control variables come from the World Bank’s WDI database: GDP per capita (PPP adjusted, in 2011 constant international dollars), personal remittances received as a percentage of GDP, primary gross enrollment ratio for both sexes, public spending on health as a percentage of GDP, and total fertility rates. I use the natural logarithm of GDP per capita and primary gross enrollment ratio. Primary gross enrollment ratio is a common measure of a country’s overall literacy status, but it is not an input measure for its medical training capacity. Since medical training capacity is related to the supply of doctors, I have also controlled for the number of medical schools in a country and used the natural logarithm of this variable. As about 12 percent of country-years in the dataset do not have a single medical school, I have added 1 to the number of medical schools to do the log transformation. The data on medical schools come from the World Directory of Medical Schools database [52]. Finally, to account for a country’s levels of economy over time, I have used the World Bank’s income-group classification as low, lower-middle, upper-middle, and high-income countries based on gross national income (GNI) per capita in current US dollars of the previous year [53].
Using this data set in a fixed-effects regression model, first I estimate the effect of medical brain drain (MBD) on the log of the total number of domestically available doctors, and then I estimate the effect of the number of available doctors on child health. After establishing the association between medical brain drain and child health through the mediation of the number of doctors, I test the possible quadratic relationship by using a square term of the 1-year lagged MBD variable. In addition, I analyze the interaction between MBD and levels of economic development. Since the medical brain drain would take some time to have its effect on health, I use a 1-year lag of this variable, as did Bhargava and Docquier [49]. The logarithm of the total number of doctors is used to correct a potential positive skewness. Fixed-effects regression is used to control for the possible characteristics of the countries in the dataset—even without measuring them—so long as those characteristics (e.g., culture, language, and geographies) do not change over time [54].
3. Results
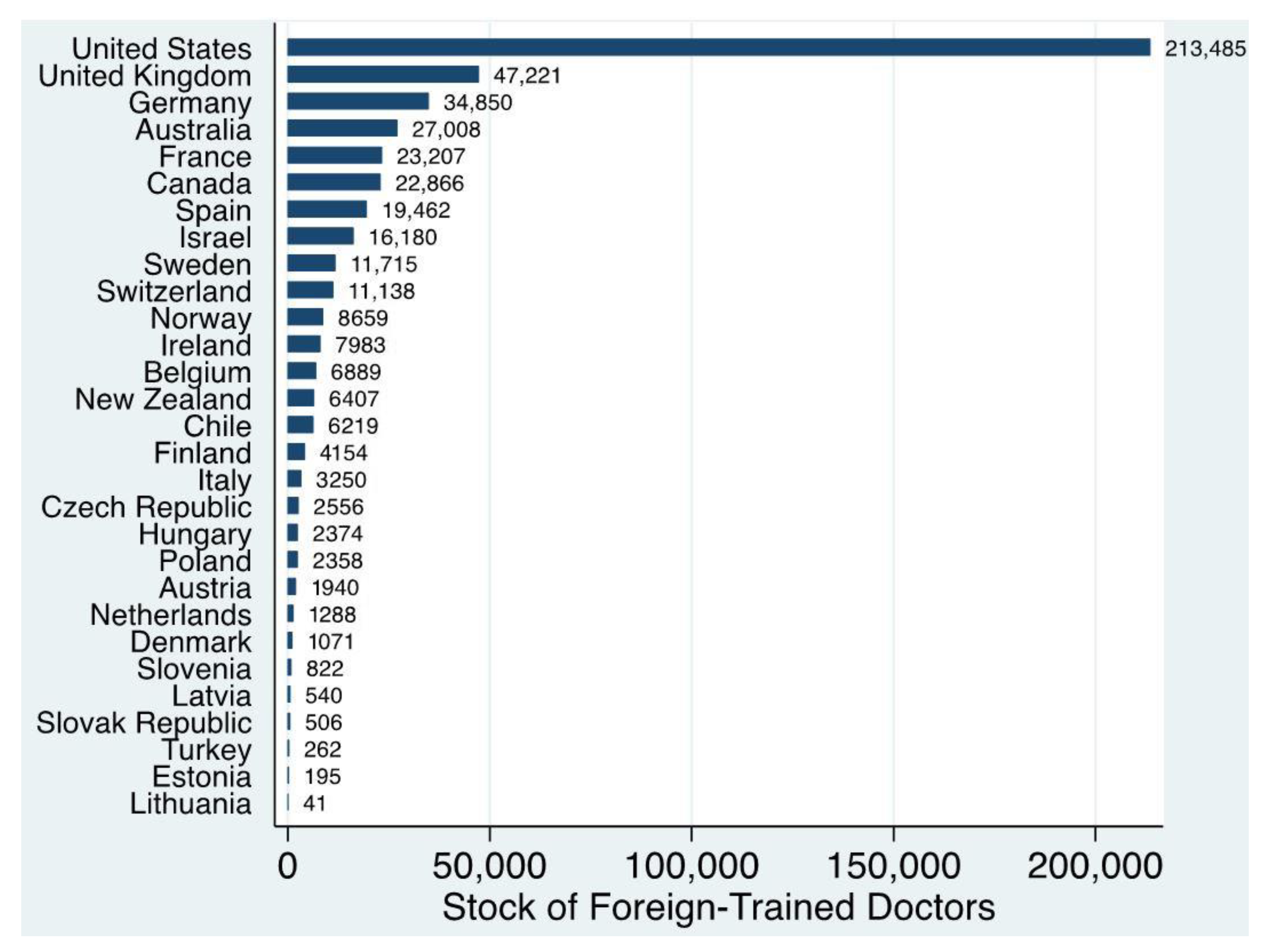
Table 1 provides the descriptive statistics of the variables used in this study. Here, the mean probability of infant mortality is 29.75, and that of U5 child mortality is 41.34 per thousand live births. The mean MBD rate is 5.1 percent. The majority of the country-year observations (94 percent) have an MBD rate between 0 and 20 percent; only 4 percent of them have an MBD rate between 20 and 40 percent; slightly less than one percent have MBD between 40 and 60 percent, while slightly over one percent have MBD between 60 and 100 percent. The total stock of foreign-trained doctors by destination country is presented in Figure 1. It shows that the United States has the most foreign-trained doctors of all destination countries. Since the destination countries are also the countries of origin and training for many doctors working in other countries, these countries are first kept in the analysis and then dropped to see if there is any difference in results. However, no significant difference was found. In addition, no significant multicollinearity issues were found among the variables used in this analysis.
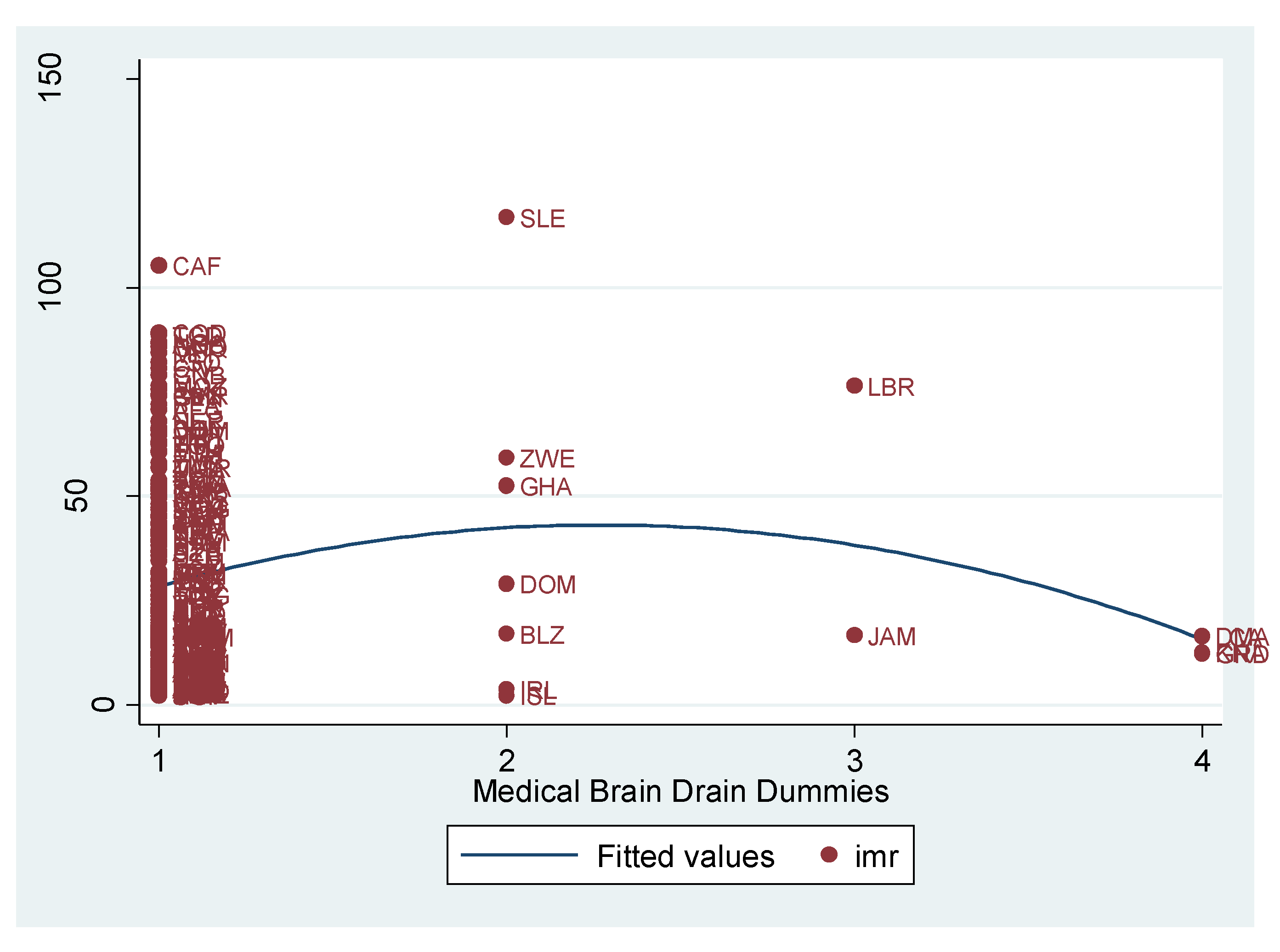
Figure 2 presents the distribution of infant mortality by the levels of MBD in 188 countries in the year 2008, the midpoint of the period 2000–2015. The levels of MBD are measured as 1 = MBD (0–20%), 2 = MBD (20–40%), 3 = MBD (40–60%), and 4 = MBD (60–100%). This distribution gives a sense of my hypothesized quadratic relationship between MBD and child health.
Since the mechanism through which MBD may affect child health works through the number of available doctors, we want to see if MBD has a negative effect on the latter. Table 2 presents the results from the fixed-effects regression of MBD (1-year lagged) on the number of available doctors (logged). The results show that MBD negatively affects the number of available doctors over time, even after controlling for factors like GDP per capita, remittances, public spending on health, primary gross enrollment ratio, TFR, number of medical schools, and country-income groups. All these factors are significant in the expected direction except for health expenditures and medical schools.
Table 3 presents the results from the fixed-effects regression of the number of available doctors on infant mortality. The results show that the number of available doctors is associated with fewer infant deaths per thousand live births. A Sobel test (following Baron and Kenny [55]; Sobel [56]) is performed on the first models from Table 2 and Table 3 to determine if the effect of medical brain drain on infant mortality is significantly mediated by the number of available doctors. The test confirms the mediation effect. The effect of the number of doctors on infant mortality per 1000 live births (IMR) is significant across all models in Table 3.
Now, I test the hypothesized quadratic relationship between MBD and child health. Table 4 presents the results from the fixed-effects regression of MBD on IMR in 188 countries over 2000–2015. The first model with MBD (1-year lagged) only shows a beneficial effect of MBD on IMR, but as I add the MBD-squared term in models 2 to 4, the effect turns to be detrimental. All the control variables are significant in the expected direction. Notably, remittances have a beneficial effect on IMR, and so do GDP per capita, health expenditures, primary gross enrollment ratio, and medical schools. Total fertility rate has an unfavorable effect on IMR. Both low- and lower-middle-income countries have higher IMR compared to high-income countries, the reference category.
Medical brain drain has the same unfavorable quadratic relationship with U5 mortality per 1000 live births (U5MR). Results in Table 5 show that the beneficial effect of MBD turns unfavorable when a square term of the variable is added to the model. As in Table 4, GDP per capita, remittances, public spending on health, and primary education have beneficial effects on U5MR, while TFR is associated with increased child mortality. Unlike Table 4, the number of medical schools (logged) is not related to U5MR.
To analyze if MBD affects child health in interaction with the levels of economy, I added several interaction terms to the final models of Table 4 and Table 5. The interaction term for MBD and GDP per capita has an unfavorable effect on IMR (Table 6) and U5MR (Table 7). The interaction term for MBD and low-income countries has a beneficial effect on both IMR and U5MR, but the interaction term for MBD and upper-middle-income countries has an unfavorable effect. The interaction term for MBD and lower-middle-income countries is not significant.
Finally, Table 8 replicates the full models from Table 4 and Table 5, excluding the destinations countries from which the data on the stock of foreign-trained doctors were compiled (see Figure 1 above). In addition, I have also excluded Saudi Arabia, the United Arab Emirates, and Qatar, as these countries have a sizable stock of foreign-trained doctors. As the full set of countries, the results are similar and suggest that the relationship between MBD and child health is curvilinear.
4. Discussion
This study finds strong evidence supporting a quadratic relationship between medical brain drain and child health. The results show that higher medical brain drain rates are associated with higher infant and child mortality rates among countries approximately in the middle of the medical brain drain scale. This relationship is weaker among countries on both ends of the scale. Moreover, the effect is detrimental for upper-middle-income countries but beneficial for low-income countries. These findings, based on more recent data on 188 countries over a span of 16 years, add to the extant literature on both medical brain drain and medical brain gain. These findings also have important implications for policy and future research.
Firstly, the high-income countries’ policy of attracting and recruiting foreign-trained healthcare professionals, especially doctors, should be informed by empirical evidence. When doctors emigrate, the number of available doctors in the sending society decreases. The health systems in many countries are already crippled by workforce shortages. If they fail to replenish the human capital loss due to the increasing emigration of doctors and other health professionals, their health systems may collapse [1]. Under the United Nations framework on Sustainable Development Goals (SDGs), rich countries have obligations to support developing countries for achieving universal health coverage by 2030. Providing financial assistance is an important way to help them, but adjusting their immigration and recruitment policy is perhaps more important to address the health workforce shortages in developing countries.
Secondly, rich countries may have to treat foreign-trained doctors and nurses differently and practice “medical exceptionalism” in their immigration and recruitment policy, as suggested by Alkire and Chen [57]. This is a moral call, and can be tied to The WHO Global Code of Practice on the International Recruitment of Health Personnel [58]. However, the implementation of the Code is obstructed due to the complexity of the patterns and effects of healthcare migration. The empirical basis for policy decisions about recruiting internationally trained health workers is very weak since only a few empirical studies exist. Further empirical research and the monitoring of the recruitment of foreign-trained health personnel at the international level are constrained by data availability. Most sending countries do not regularly report healthcare migration data to the WHO. Most of them do not have a good system of recording migration data. In contrast, receiving countries in OECD more systematically record migration flows and are the main sources of healthcare migration data. Lacking appropriate data, solid empirical evidence cannot be produced. The WHO in partnership with its member countries and other public and private organizations must ensure regular data collection on healthcare migration and monitor factors affecting migration flows and health workforce shortages in sending countries. Data availability would facilitate and expedite future research on this topic as well. Future research projects should also focus on data collection, especially through surveys. Survey data can importantly help multilevel analysis by looking at individual-level factors contributing to healthcare migration and health. Ecological studies, including this one, miss the individual-level dynamics that may affect the relationships between healthcare migration and health outcomes.
Thirdly, rich countries need to decrease their dependency on low- and middle-income countries for recruiting health workers. A significant portion of high-income countries’ health workers is foreign-trained. For example, percentage-wise, Israel has the highest foreign-trained doctors of all OECD countries—58.5 percent of their total doctors were foreign-trained in 2015, a 6.2 percentage point drop from 2000 [48]. In the same period, the medical graduate production in Israel remained constant at 5.5 per 100,000 inhabitants. For all OECD countries, there is a huge gap in health personnel production and their consumption, and this gap is filled in by recruiting foreign-trained doctors. From a cost-benefit analysis, this approach is justified. But from a health justice point of view, this only exacerbates the gap between developed and developing countries. This gap can be minimized if high-income countries train their own medical graduates and/or invest in medical schooling in low- and middle-income countries. Given the growing demand of health professionals worldwide, more investment in medical graduate production is necessary. According to the World Directory of Medical Schools database, high-income countries did not see any significant increase in medical schools between 2000 and 2015, whereas there was almost 2.5 times increase in medical schools in middle-income countries over the same period [52].
A fourth policy implication of my findings relates to the recruitment and retention policy in the health sector of sending countries. To ensure basic health service delivery to people and achieve the UHC goal, sending countries must take steps to retain their trained health workforce. Wide gaps in wages in relative terms between sending and receiving countries make emigration decisions easier for many health professionals, given the high demand for their job in the international market. Lack of governance in the health sector is another important contributing factor for physician emigration [59]. In many developing countries, health professionals do not serve in their posts largely because of the poor working conditions at the facility [60]. Working conditions are even worse in rural facilities than those in urban areas, contributing to internal rural–urban migration of health workers who may also leave the public sector for better earning potentials and working conditions in the private sector. Authorities in these developing countries need to address the wage gap, working conditions, and governance issues in the health sector to retain their health professionals.
Finally, this study finds that remittances have a favorable effect on child health. This may explain why the interaction term for MBD and low-income country dummy has a favorable effect on child health as well. Although data are not available on what percentage of the total remittances is sent by health workers, the emigration of more health workers from low-income countries should reasonably contribute to more remittance revenues. Evidence suggests that workers’ remittances bear great importance for economic development especially in low-income countries [61]. Some studies find that remittance earning opportunities encourage greater production of health workers in Africa [62]. However, the favorable effect of remittances should not be taken as evidence for medical brain gain in the long run. The employability of health workers in the international market depends on factors like economic recessions, changes in immigration policy in destination countries, the recognition of academic credentials from certain sending countries, and uncertainties arising from situations like the COVID-19 pandemic. The experience of some countries like the Philippines suggests that the dependence on remittances by exporting health workers can end up in an “emigration trap” [63]. Moreover, the focus on training health workers for the international market can ignore the domestic need and create pressure on medical schools due to competition, as evidenced in the Philippines. In some other countries like India, Malaysia, Singapore, and Thailand, modern private hospitals recruit both domestic and foreign-trained health professionals to attract “medical tourists” from all over the world. While this effort can be viewed as a means to reduce medical brain drain, it obviously creates health disparities between the rich and the poor [64]. In the long run, the positive incentive effect of migration prospects on medical training can turn to be too small to generate a net brain gain and ultimately lead to a reduction in the number of health workers in developing countries, as warned by a seminal study [16].
It should also be noted that remittance data has major problems. The most important problem is estimating remittance data from informal flows. Many countries do not report data on remittance flows in the IMF balance of payments statistics, which is the main source of official remittance data. Additionally, those countries that report data on remittances leave out flows from money transfer operators and informal channels which indeed handle most remittance flows [65]. Household surveys often collect information on personal remittances, but these surveys are not conducted in all countries on a regular basis. Future research can see how to improve remittance data and gather information on the specific contribution to remittance flows made by migrant health workers.
Reliable data on the international migration of health professionals as well as remittances are vital to make evidence-based policy for better managing healthcare migration and addressing the medical brain drain problem at both national and international levels. Efforts should be made to record migration data by professions (e.g., doctors, nurses, medical technicians, etc.), levels of education, degrees, gender, country of training, and country of birth to help further research and policymaking on healthcare migration. It is important to note that, lacking appropriate data, my results are more likely to under-estimate the impact of medical brain drain, as this variable measures only the stock of foreign-trained doctors in some destination countries; it does not include the stock of other foreign-trained medical professionals such as nurses, midwives, dentists, ophthalmologists, and medical technicians. If the stock of all the foreign-trained health professionals is calculated, the impact of medical brain drain can be much bigger.
Funding
This research received no external funding.
Acknowledgment
The author thanks three anonymous reviewers for their comments and suggestions. He also thanks Matthew Lange, Professor of Sociology, McGill University, for his comments on the first draft of the paper.
Conflicts of Interest
The author declares no conflict of interest.
References
- OECD. The Looming Crisis in the Health Workforce: How Can OECD Countries Respond? Organisation for Economic Co-Operation and Development (OECD): Paris, France, 2008. [Google Scholar]
- WHO. The World Health Report 2006: Working Together for Health; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Clark, P.F.; Stewart, J.B.; Clark, D.A. The globalization of the labour market for health-care professionals. Int. Labour Rev. 2006, 145, 37–64. [Google Scholar] [CrossRef]
- Clemens, M.A.; Pettersson, G. New data on African health professionals abroad. Hum. Resour. Health 2008, 6, 1. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, S.; Sperling, P.; Poulsen, M.S.; Emmersen, J.; Andersen, S. Medical students for health-care staff shortages during the COVID-19 pandemic. Lancet 2020, 395, e79–e80. [Google Scholar] [CrossRef]
- McMahon, D.E.; Peters, G.A.; Ivers, L.C.; Freeman, E.E. Global resource shortages during COVID-19: Bad news for low-income countries. PLoS Negl. Trop. Dis. 2020, 14, e0008412. [Google Scholar] [CrossRef]
- WHO. Health Workforce. Available online: https://www.who.int/health-topics/health-workforce#tab=tab_1. (accessed on 22 August 2020).
- Liu, J.; Goryakin, Y.; Maeda, A.; Bruckner, T.A.; Scheffler, R.M. Global health workforce labor market projections for 2030. Hum. Resour. Health 2017, 15, 11. [Google Scholar] [CrossRef] [Green Version]
- Aluttis, C.; Bishaw, T.; Frank, M.W. The workforce for health in a globalized context—Global shortages and international migration. Glob. Health Action 2014, 7. [Google Scholar] [CrossRef]
- O’Brien, P.; Gostin, L.O. Health worker shortages and inequalities: The reform of United States policy. Glob. Health Gov. 2009, 2, 1. [Google Scholar]
- Crisp, N.; Chen, L.C. Global supply of health professionals. N. Engl. J. Med. 2014, 370, 950–957. [Google Scholar] [CrossRef] [Green Version]
- Sewankambo, N.K. Strengthening health capacity in sub-Saharan Africa: A millennium development challenge. In Africa’s Health Challenges: Sovereignty, Mobility of People and Healthcare Governance; Cooper, A.F., Besada, H., Eds.; Routledge: London, UK, 2016. [Google Scholar]
- Anand, S.; Bärnighausen, T. Human resources and health outcomes: Cross-country econometric study. Lancet 2004, 364, 1603–1609. [Google Scholar] [CrossRef]
- Tandon, A.; Sousa, A.; Prasad, A.; Evans, D.B. Human resources and health outcomes in Brazil and Viet Nam: A comparative perspective. In The World Health Report 2006: Working Together for Health; WHO, Ed.; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Chauvet, L.; Gubert, F.; Mesplé-Somps, S. Aid, remittances, medical brain drain and child mortality: Evidence using inter and intra-country data. J. Dev. Stud. 2013, 49, 801–818. [Google Scholar] [CrossRef]
- Bhargava, A.; Docquier, F.; Moullan, Y. Modeling the effects of physician emigration on human development. Econ. Hum. Biol. 2011, 9, 172–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.C.; Evans, T.; Anand, S.; Boufford, J.I.; Brown, H.; Chowdhury, M.; Cueto, M.; Dare, L.; Dussault, G.; Elzinga, G.; et al. Human resources for health: Overcoming the crisis. Lancet 2004, 364, 1984–1990. [Google Scholar] [CrossRef]
- Speybroeck, N.; Kinfu, Y.; Dal Poz, M.R.; Evans, D.B. Reassessing the relationship between human resources for health, intervention coverage and health outcomes. In The World Health Report 2006: Working Together for Health; WHO, Ed.; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Lehmann, U.; Dieleman, M.; Martineau, T. Staffing remote rural areas in middle- and low-income countries: A literature review of attraction and retention. BMC Health Serv. Res. 2008, 8, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vujicic, M.; Zurn, P.; Diallo, K.; Adams, O.; Poz, M.R.D. The role of wages in the migration of health care professionals from developing countries. Hum. Resour. Health 2004, 2, 3. [Google Scholar] [CrossRef] [Green Version]
- Docquier, F.; Rapoport, H. Globalization, brain drain, and development. J. Econ. Lit. 2012, 50, 681–730. [Google Scholar] [CrossRef] [Green Version]
- Okeke, E.N. Brain drain: Do economic conditions “push” doctors out of developing countries? Soc. Sci. Med. 2013, 98, 169–178. [Google Scholar] [CrossRef]
- Acosta, P.A.; Fajnzylber, P.; Lopez, H. The Impact of Remittances on Poverty and Human Capital: Evidence from Latin American Household Surveys; Technical Report No. WPS4247; World Bank Group: Washington, DC, USA, 2007. [Google Scholar] [CrossRef]
- Docquier, F.; Faye, O.; Pestieau, P. Is migration a good substitute for education subsidies? J. Dev. Econ. 2008, 86, 263–276. [Google Scholar] [CrossRef] [Green Version]
- Stilwell, B.; Diallo, K.; Zurn, P.; Poz, M.R.D.; Adams, O.; Buchan, J. Developing evidence-based ethical policies on the migration of health workers: Conceptual and practical challenges. Hum. Resour. Health 2003, 1, 8. [Google Scholar] [CrossRef] [Green Version]
- Mills, E.J.; Kanters, S.; Hagopian, A.; Bansback, N.; Nachega, J.; Alberton, M.; Au-Yeung, C.G.; Mtambo, A.; Bourgeault, I.L.; Luboga, S.; et al. The financial cost of doctors emigrating from sub-Saharan Africa: Human capital analysis. BMJ 2011, 343, d7031. [Google Scholar] [CrossRef] [Green Version]
- Kirigia, J.M.; Gbary, A.R.; Muthuri, L.H.K.; Nyoni, J.; Seddoh, A. The cost of health professionals’ brain drain in Kenya. BMC Health Serv. Res. 2006, 6, 89. [Google Scholar] [CrossRef] [Green Version]
- Karan, D.D.A. Medical “Brain drain” and health care worker shortages: How should international training programs respond? AMA J. Ethics 2016, 18, 665–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, X.; Hatton, T.; Williamson, J. Where Do Us Immigrants Come From and Why? Working Paper No. 8998; National Bureau of Economic Research: Cambridge, MA, USA, 2002; Available online: http://www.nber.org/papers/w8998 (accessed on 12 January 2017).
- Hatton, T.; Williamson, J. What Fundamentals Drive World Migration? Working Paper 9159; National Bureau of Economic Research: Cambridge, MA, USA, 2002; Available online: http://www.nber.org/papers/w9159 (accessed on 29 April 2017).
- Kassar, H.; Marzouk, D.; Anwar, W.A.; Lakhoua, C.; Hemminki, K.; Khyatti, M. Emigration flows from North Africa to Europe. Eur. J. Public Health 2014, 24, 2–5. [Google Scholar] [CrossRef] [Green Version]
- Houle, R.; Yssaad, L. Recognition of newcomers’ foreign credentials and work experience. Perspect. Lab. Income 2010, 22, 18–33. [Google Scholar]
- Mata, F. The Non-Accreditation of Immigrant Professionals in Canada: Societal Dimensions of the Problem; Metropolis: Ottawa, ON, Canada, 1999. [Google Scholar]
- Boyd, M.; Schellenberg, G. Re-accreditation and occupations of immigrant doctors and engineers. Canadian Soc. Trends 2007. Available online: https://www150.statcan.gc.ca/n1/pub/11-008-x/2007004/10312-eng.htm (accessed on 29 April 2017).
- Boyd, M.; Thomas, D. Match or mismatch? The employment of immigrant engineers in Canada’s labor force. Popul. Res. Policy Rev. 2001, 20, 107–133. [Google Scholar] [CrossRef]
- Boyd, M.; Thomas, D. Skilled immigrant labour: Country of origin and the occupational locations of male engineers. Can. Stud. Popul. 2002, 29, 71–99. [Google Scholar] [CrossRef] [Green Version]
- Wayland, S.V. Unsettled: Legal and Policy Barriers for Newcomers to CANADA; A Joint Initiative of Community Foundations of Canada and the Law Commission of Canada: Ottawa, ON, Canada, 2018; Available online: http://www.cfc-fcc.ca/doc/LegalPolicyBarriers.pdf. (accessed on 10 August 2018).
- Preston, S.H. The changing relation between mortality and level of economic development. Popul. Stud. 1975, 29, 231–248. [Google Scholar] [CrossRef]
- Pritchett, L.; Summers, L.H. Wealthier is Healthier. J. Hum. Resour. 1996, 31, 841. [Google Scholar] [CrossRef]
- Smith, R.D.; Chanda, R.; Tangcharoensathien, V. Trade in health-related services. Lancet 2009, 373, 593–601. [Google Scholar] [CrossRef]
- Bach, S. International migration of health workers: Labour and social issues. In Sectoral Activities Program Working Paper, WP.209; International Labour Office: Geneva, Switzerland, 2003. [Google Scholar]
- Docquier, F.; Lodigiani, E. Skilled migration and business networks. Open Econ. Rev. 2010, 21, 565–588. [Google Scholar] [CrossRef] [Green Version]
- Frenk, J.; Bobadilla, J.L.; Sepuúlveda, J.; Cervantes, M.L. Health transition in middle-income countries: New challenges for health care. Health Policy Plan. 1989, 4, 29–39. [Google Scholar] [CrossRef]
- Skeldon, R. International migration as a tool in development policy: A passing phase? Popul. Dev. Rev. 2008, 34, 1–18. [Google Scholar] [CrossRef]
- Buchan, J. Migration of health workers in Europe: Policy problem or policy solution. In Human Resources for Health in Europe; Dubois, C.-A., McKee, M., Nolte, E., Eds.; Open University Press: Berkshire, UK, 2006; pp. 41–62. [Google Scholar]
- Hagopian, A.; Thompson, M.J.; Fordyce, M.; Johnson, K.E.; Hart, L.G. The migration of physicians from sub-Saharan Africa to the United States of America: Measures of the African brain drain. Hum. Resour. Health 2004, 2, 17. [Google Scholar] [CrossRef] [PubMed]
- Pond, B.; McPake, B. The health migration crisis: The role of four Organisation for Economic Cooperation and Development countries. Lancet 2006, 367, 1448–1455. [Google Scholar] [CrossRef]
- OECD. Health Resources Data. Available online: https://stats.oecd.org (accessed on 10 December 2018).
- Bhargava, A.; Docquier, F. AIDS pandemic, medical brain drain and economic development in sub-Saharan Africa. World Bank Econ. Rev. 2008, 22, 345–366. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global Health Workforce Statistics. Available online: https://www.who.int/hrh/statistics/hwfstats/en/ (accessed on 10 December 2018).
- World Bank. World Development Indicators. Available online: http://data.worldbank.org. (accessed on 9 December 2018).
- World Directory of Medical Schools. World Medical School Database. 2018. Available online: https://search.wdoms.org/ (accessed on 10 December 2018).
- World Bank. Country Classification Data. 2018. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519 (accessed on 10 December 2018).
- Allison, P.D. Fixed Effects Regression Methods for Longitudinal Data Using SAS®; SAS Institute Inc.: Cary, NC, USA, 2005. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Sobel, M.E. Asymptotic intervals for indirect effects in structural equations models. In Sociological Methodology; Leinhart, S., Ed.; Jossey-Bass: San Francisco, CA, USA, 1982; pp. 290–312. [Google Scholar]
- Alkire, S.; Chen, L. Medical exceptionalism in international migration: Should doctors and nurses be treated differently. In Globalizing Migration Regimes; Tomas, K., Palme, J., Eds.; Ashgate: Aldershot, UK, 2006. [Google Scholar]
- WHO. The WHO Global Code of Practice on the International Recruitment of Health Personnel; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Quamruzzaman, A. Infrastructure provisioning and health service utilization in Africa: Does governance explain the gap? Sociol. Dev. 2017, 3, 47–69. [Google Scholar] [CrossRef]
- Chaudhury, N.; Hammer, J.; Kremer, M.; Muralidharan, K.; Rogers, F.H. Missing in action: Teacher and health worker absence in developing countries. J. Econ. Perspect. 2006, 20, 91–116. [Google Scholar] [CrossRef] [Green Version]
- Neyapti, B. Trends in workers’ remittances: A worldwide overview. Emerg. Mark. Finance Trade 2004, 40, 83–90. [Google Scholar] [CrossRef]
- Clemens, M.A. Do Visas Kill? Health Effects of African Health Professional Emigration; Working Paper 114; Center for Global Development: Washington, DC, USA, 2007. [Google Scholar]
- Ortiga, Y.Y. Emigration, Employability and Higher Education in the Philippines; Routledge: London, UK, 2017. [Google Scholar]
- Connell, J. Medical tourism: Sea, sun, sand and … surgery. Tour. Manag. 2006, 27, 1093–1100. [Google Scholar] [CrossRef]
- Ratha, D.; Xu, Z. Migration and Remittances Factbook 2008; The World Bank: Washington, DC, USA, 2008. [Google Scholar]
Figure 1.
Stock of foreign-trained doctors in 29 destination countries in 2015 (or nearest year). Data source: OECD [48]. Foreign-trained is defined based on the place of training for all countries except Germany, where it is based on nationality, and Spain, where it is based on place of birth.
Figure 1.
Stock of foreign-trained doctors in 29 destination countries in 2015 (or nearest year). Data source: OECD [48]. Foreign-trained is defined based on the place of training for all countries except Germany, where it is based on nationality, and Spain, where it is based on place of birth.

Figure 2.
Distribution of infant mortality by the levels of MBD in 188 countries in 2008.


{kind=link}
{kind=link}
Table 1.
Descriptive statistics.
| Variables | Obs. | Mean | Std. Dev. | Min. | Max. |
|---|---|---|---|---|---|
| Infant Mortality per 1000 Live Births (IMR) | 3008 | 29.747 | 27.294 | 1.700 | 142 |
| U5 Mortality per 1000 Live Births (U5MR) | 3008 | 41.341 | 43.485 | 2.200 | 234 |
| Total Doctors | 3008 | 49,698.130 | 168,276.800 | 0.066 | 2,484,651 |
| Medical Brain Drain (MBD) | 3008 | 0.051 | 0.123 | 0 | 0.998 |
| MBD (1-year lagged) | 2820 | 0.048 | 0.118 | 0 | 0.998 |
| MBD Dummy (0–20%) | 3008 | 0.940 | 0.237 | 0 | 1 |
| MBD Dummy (20–40%) | 3008 | 0.040 | 0.195 | 0 | 1 |
| MBD Dummy (40–60%) | 3008 | 0.008 | 0.089 | 0 | 1 |
| MBD Dummy (60% +) | 3008 | 0.012 | 0.110 | 0 | 1 |
| GDP per Capita (PPP, 2011 int. dollars) | 3008 | 16,467.910 | 19,546.030 | 545.680 | 129,349.900 |
| Remittances Received (personal, % of GDP) | 3008 | 4.193 | 6.778 | 0 | 53.826 |
| Health Expenditure (public, % of GDP) | 3005 | 3.862 | 2.535 | 0.045 | 21.654 |
| Primary Gross Enrollment Ratio (PGER) | 3008 | 104.259 | 17.321 | 21.720 | 150.786 |
| Total Fertility Rate (TFR) | 3008 | 2.995 | 1.552 | 1.076 | 7.679 |
| Medical Schools | 3008 | 12.850 | 32.756 | 0 | 403 |
| Low-Income Countries Dummy | 3008 | 0.240 | 0.427 | 0 | 1 |
| Lower-Middle-Income Dummy | 3008 | 0.273 | 0.445 | 0 | 1 |
| Upper-Middle-Income Dummy | 3008 | 0.235 | 0.424 | 0 | 1 |
| High-Income Dummy (Reference Category) | 3008 | 0.253 | 0.435 | 0 | 1 |
Table 2.
Fixed-effects regression of MBD (1-year lagged) on total number of doctors (logged) in 188 countries over 2000–2015.
Table 2.
Fixed-effects regression of MBD (1-year lagged) on total number of doctors (logged) in 188 countries over 2000–2015.
| Models | (1) | (2) | (3) |
|---|---|---|---|
| Variables | Log total doctors | Log total doctors | Log total doctors |
| MBD (1-year lagged) | −0.720 *** | −1.080 *** | −1.114 *** |
| (0.101) | (0.102) | (0.103) | |
| Log GDP per Capita | 0.308 *** | 0.245 *** | |
| (0.047) | (0.051) | ||
| Remittances | −0.009 ** | −0.008 * | |
| (0.003) | (0.003) | ||
| Health Expenditures | 0.019 | 0.015 | |
| (0.010) | (0.010) | ||
| Log PGER | 0.321 *** | 0.310 *** | |
| (0.084) | (0.084) | ||
| TFR | −0.335 *** | −0.343 *** | |
| (0.039) | (0.039) | ||
| Log Medical Schools | −0.008 | −0.023 | |
| (0.032) | (0.033) | ||
| Low-income | −0.294 *** | ||
| (0.081) | |||
| Lower-middle Income | −0.221 *** | ||
| (0.066) | |||
| Upper-middle Income | −0.152 ** | ||
| (0.051) | |||
| Constant | 8.436 *** | 5.156 *** | 6.000 *** |
| (0.009) | (0.622) | (0.670) | |
| Observations | 2818 | 2818 | 2818 |
| R-squared | 0.019 | 0.103 | 0.107 |
| Number of Countries | 188 | 188 | 188 |
Standard Errors in Parentheses; *** p < 0.001, ** p < 0.01, * p < 0.05.
Table 3.
Fixed-effects regression of total number of doctors (logged) on IMR in 188 countries over 2000–2015.
Table 3.
Fixed-effects regression of total number of doctors (logged) on IMR in 188 countries over 2000–2015.
| Models | (1) | (2) | (3) |
|---|---|---|---|
| Variables | IMR | IMR | IMR |
| Log Number of Doctors | −3.432 *** | −0.609 ** | −0.494 * |
| (0.300) | (0.198) | (0.192) | |
| Log GDP per Capita | −10.603 *** | −8.279 *** | |
| (0.486) | (0.511) | ||
| Remittances | −0.199 *** | −0.229 *** | |
| (0.032) | (0.031) | ||
| Health Expenditures | −0.930 *** | −0.808 *** | |
| (0.102) | (0.100) | ||
| Log PGER | −12.669 *** | −11.827 *** | |
| (0.873) | (0.848) | ||
| TFR | 12.895 *** | 12.672 *** | |
| (0.405) | (0.396) | ||
| Log Medical Schools | −1.636 *** | −1.094 *** | |
| (0.332) | (0.325) | ||
| Low-income | 7.853 *** | ||
| (0.814) | |||
| Lower-middle Income | 2.808 *** | ||
| (0.660) | |||
| Upper-middle Income | −0.051 | ||
| (0.515) | |||
| Constant | 58.012 *** | 157.750 *** | 128.690 *** |
| (2.521) | (6.524) | (6.818) | |
| Observations | 2818 | 2818 | 2818 |
| R-squared | 0.048 | 0.610 | 0.636 |
| Number of Countries | 188 | 188 | 188 |
Standard Errors in Parentheses; *** p < 0.001, ** p < 0.01, * p < 0.05.
Table 4.
Fixed-effects regression of MBD (1-year lagged) on IMR in 188 countries over 2000–2015.
| Models | (1) | (2) | (3) | (4) |
|---|---|---|---|---|
| Variables | IMR | IMR | IMR | IMR |
| MBD (1-year lagged) | −15.391 *** | −199.693 *** | −57.433 *** | −54.118 *** |
| (1.577) | (11.692) | (8.212) | (7.975) | |
| MBD (squared) | 67.026 *** | 20.853 *** | 19.555 *** | |
| (4.217) | (2.928) | (2.841) | ||
| Log GDP per capita | −10.354 *** | −8.079 *** | ||
| (0.483) | (0.508) | |||
| Remittances | −0.191 *** | −0.221 *** | ||
| (0.031) | (0.031) | |||
| Health Expenditures | −0.839 *** | −0.726 *** | ||
| (0.103) | (0.101) | |||
| Log PGER | −12.605 *** | −11.743 *** | ||
| (0.866) | (0.842) | |||
| TFR | 12.859 *** | 12.587 *** | ||
| (0.402) | (0.394) | |||
| Log Medical Schools | −1.421 *** | −0.894 ** | ||
| (0.335) | (0.327) | |||
| Low-income | 7.644 *** | |||
| (0.810) | ||||
| Lower-middle Income | 2.583 *** | |||
| (0.660) | ||||
| Upper-middle Income | −0.133 | |||
| (0.514) | ||||
| Constant | 29.919 *** | −35.770 *** | 129.013 *** | 102.883 *** |
| (0.144) | (4.135) | (7.343) | (7.468) | |
| Observations | 2818 | 2818 | 2818 | 2818 |
| R-squared | 0.035 | 0.120 | 0.616 | 0.641 |
| Number of Countries | 188 | 188 | 188 | 188 |
Standard Errors in Parentheses; *** p < 0.001, ** p < 0.01.
Table 5.
Fixed-effects regression of MBD (1-year lagged) on U5MR in 188 countries over 2000–2015.
| Models | (1) | (2) | (3) | (4) |
|---|---|---|---|---|
| Variables | U5MR | U5MR | U5MR | U5MR |
| MBD (1-year lagged) | −26.545 *** | −326.535 *** | −93.719 *** | −90.191 *** |
| (2.826) | (21.131) | (15.850) | (15.625) | |
| MBD (squared) | 109.098 *** | 33.350 *** | 31.872 *** | |
| (7.621) | (5.651) | (5.566) | ||
| Log GDP per Capita | −15.261 *** | −12.189 *** | ||
| (0.933) | (0.995) | |||
| Remittances | −0.227 *** | −0.262 *** | ||
| (0.061) | (0.060) | |||
| Health Expenditures | −1.273 *** | −1.136 *** | ||
| (0.199) | (0.197) | |||
| Log PGER | −26.894 *** | −25.546 *** | ||
| (1.671) | (1.649) | |||
| TFR | 23.252 *** | 22.741 *** | ||
| (0.776) | (0.772) | |||
| Log Medical Schools | −1.235 | −0.487 | ||
| (0.647) | (0.641) | |||
| Low-income | 10.372 *** | |||
| (1.587) | ||||
| Lower-middle Income | 2.702 * | |||
| (1.293) | ||||
| Upper-middle Income | −0.498 | |||
| (1.008) | ||||
| Constant | 41.702 *** | −65.221 *** | 209.333 *** | 173.615 *** |
| (0.259) | (7.473) | (14.172) | (14.632) | |
| Observations | 2818 | 2818 | 2818 | 2818 |
| R-squared | 0.032 | 0.102 | 0.554 | 0.570 |
| Number of Countries | 188 | 188 | 188 | 188 |
Standard Errors in Parentheses; *** p < 0.001, * p < 0.05.
Table 6.
Interaction effects of MBD (1-year lagged) and levels of economy on IMR in 188 countries over 2000–2015.
Table 6.
Interaction effects of MBD (1-year lagged) and levels of economy on IMR in 188 countries over 2000–2015.
| Models | (1) | (2) | (3) | (4) |
|---|---|---|---|---|
| Variables | IMR | IMR | IMR | IMR |
| MBD (1-year lagged) | −102.842 *** | 4.261 *** | 0.600 | −7.787 *** |
| (10.267) | (1.049) | (1.054) | (1.571) | |
| Log GDP per capita | −8.407 *** | −8.020 *** | −8.338 *** | −8.197 *** |
| (0.501) | (0.496) | (0.512) | (0.507) | |
| Remittances | −0.222 *** | −0.226 *** | −0.225 *** | −0.227 *** |
| (0.030) | (0.030) | (0.031) | (0.031) | |
| Health Expenditures | −0.778 *** | −0.737 *** | −0.806 *** | −0.757 *** |
| (0.099) | (0.098) | (0.101) | (0.100) | |
| Log PGER | −11.008 *** | −10.445 *** | −12.080 *** | −11.752 *** |
| (0.838) | (0.833) | (0.851) | (0.842) | |
| TFR | 12.108 *** | 11.950 *** | 12.813 *** | 12.499 *** |
| (0.395) | (0.390) | (0.396) | (0.395) | |
| Log Medical Schools | −1.199 *** | −1.385 *** | −1.036 ** | −1.116 *** |
| (0.323) | (0.320) | (0.330) | (0.326) | |
| Low-income | 8.836 *** | 9.577 *** | 8.047 *** | 7.541 *** |
| (0.805) | (0.802) | (0.817) | (0.811) | |
| Lower-middle income | 3.742 *** | 3.439 *** | 3.099 *** | 2.501 *** |
| (0.657) | (0.646) | (0.681) | (0.661) | |
| Upper-middle Income | 0.764 | 0.318 | 0.054 | −0.993 |
| (0.514) | (0.504) | (0.519) | (0.535) | |
| MBD-GDP Interaction | 11.210 *** | |||
| (1.110) | ||||
| MBD-low-income Interaction | −38.674 *** | |||
| (3.047) | ||||
| MBD-lower-middle-income Interaction | −4.156 | |||
| (3.191) | ||||
| MBD-upper-middle-income Interaction | 12.468 *** | |||
| (1.832) | ||||
| Constant | 122.941 *** | 117.583 *** | 125.563 *** | 124.302 *** |
| (6.624) | (6.579) | (6.746) | (6.690) | |
| Observations | 2818 | 2818 | 2818 | 2818 |
| R-squared | 0.648 | 0.656 | 0.635 | 0.641 |
| Number of Countries | 188 | 188 | 188 | 188 |
Standard Errors in Parentheses; *** p < 0.001, ** p < 0.01.
Table 7.
Interaction effects of MBD (1-year lagged) and levels of economy on U5MR in 188 countries over 2000–2015.
Table 7.
Interaction effects of MBD (1-year lagged) and levels of economy on U5MR in 188 countries over 2000–2015.
| Models | (1) | (2) | (3) | (4) |
|---|---|---|---|---|
| Variables | U5MR | U5MR | U5MR | U5MR |
| MBD (1-year lagged) | –194.335 *** | 5.556 ** | −1.051 | −14.654 *** |
| (20.094) | (2.061) | (2.060) | (3.079) | |
| Log GDP per capita | −12.724 *** | −12.035 *** | −12.620 *** | −12.381 *** |
| (0.980) | (0.975) | (1.001) | (0.993) | |
| Remittances | −0.264 *** | −0.272 *** | −0.270 *** | −0.272 *** |
| (0.060) | (0.059) | (0.061) | (0.060) | |
| Health Expenditures | −1.212 *** | −1.143 *** | −1.268 *** | −1.187 *** |
| (0.194) | (0.193) | (0.197) | (0.196) | |
| Log PGER | −24.113 *** | −23.197 *** | −26.083 *** | −25.562 *** |
| (1.641) | (1.635) | (1.663) | (1.650) | |
| TFR | 21.788 *** | 21.570 *** | 23.112 *** | 22.599 *** |
| (0.773) | (0.767) | (0.774) | (0.775) | |
| Log Medical Schools | −1.015 | −1.336* | −0.724 | −0.850 |
| (0.633) | (0.629) | (0.645) | (0.639) | |
| Low-income | 12.519 *** | 13.764 *** | 11.020 *** | 10.206 *** |
| (1.575) | (1.574) | (1.596) | (1.589) | |
| Lower-middle Income | 4.793 *** | 4.179 ** | 3.513 ** | 2.570 * |
| (1.286) | (1.269) | (1.331) | (1.295) | |
| Upper-middle Income | 1.144 | 0.284 | −0.199 | −1.896 |
| (1.006) | (0.990) | (1.015) | (1.048) | |
| MBD-GDP Interaction | 20.957 *** | |||
| (2.173) | ||||
| MBD-low-income Interaction | −68.906 *** | |||
| (5.985) | ||||
| MBD-lower-middle-income Interaction | −6.142 | |||
| (6.236) | ||||
| MBD-upper-middle-income Interaction | 20.282 *** | |||
| (3.590) | ||||
| Constant | 205.624 *** | 196.328 *** | 210.615 *** | 208.529 *** |
| (12.964) | (12.922) | (13.183) | (13.108) | |
| Observations | 2818 | 2818 | 2818 | 2818 |
| R-squared | 0.580 | 0.586 | 0.565 | 0.570 |
| Number of Countries | 188 | 188 | 188 | 188 |
Standard Errors in Parentheses; *** p < 0.001, ** p < 0.01, * p < 0.05.
Table 8.
Fixed-effects regression of MBD (1-year lagged) on IMR and U5MR in 158 countries (excluding major destination countries) over 2000–2015.
Table 8.
Fixed-effects regression of MBD (1-year lagged) on IMR and U5MR in 158 countries (excluding major destination countries) over 2000–2015.
| Variables | IMR | U5MR |
|---|---|---|
| MBD (1-year lagged) | −53.054 *** | −88.222 *** |
| (8.983) | (17.622) | |
| MBD (squared) | 19.274 *** | 31.374 *** |
| (3.183) | (6.243) | |
| Log GDP per capita | −7.855 *** | −11.762 *** |
| (0.564) | (1.106) | |
| Remittances | −0.217 *** | −0.256 *** |
| (0.033) | (0.065) | |
| Health Expenditures | −0.763 *** | −1.192 *** |
| (0.115) | (0.226) | |
| Log PGER | −11.786 *** | −25.717 *** |
| (0.919) | (1.802) | |
| TFR | 13.194 *** | 23.936 *** |
| (0.445) | (0.874) | |
| Log Medical Schools | −0.951 ** | −0.626 |
| (0.368) | (0.722) | |
| Low-income | 7.605 *** | 10.508 *** |
| (0.960) | (1.883) | |
| Lower-middle Income | 2.692 ** | 3.154 * |
| (0.819) | (1.606) | |
| Upper-middle Income | 0.008 | −0.029 |
| (0.686) | (1.347) | |
| Constant | 98.307 *** | 164.452 *** |
| (8.214) | (16.114) | |
| Observations | 2368 | 2368 |
| R-squared | 0.648 | 0.579 |
| Number of Country | 158 | 158 |
Standard Errors in Parentheses; *** p < 0.001, ** p < 0.01, * p < 0.05.
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Quamruzzaman, A. Exploring the Impact of Medical Brain Drain on Child Health in 188 Countries over 2000–2015. Societies 2020, 10, 73. https://0-doi-org.brum.beds.ac.uk/10.3390/soc10040073
AMA Style
Quamruzzaman A. Exploring the Impact of Medical Brain Drain on Child Health in 188 Countries over 2000–2015. Societies. 2020; 10(4):73. https://0-doi-org.brum.beds.ac.uk/10.3390/soc10040073
Chicago/Turabian StyleQuamruzzaman, Amm. 2020. "Exploring the Impact of Medical Brain Drain on Child Health in 188 Countries over 2000–2015" Societies 10, no. 4: 73. https://0-doi-org.brum.beds.ac.uk/10.3390/soc10040073
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.