
Enabling Immersive Exercise Activities for Older Adults: A Comparison of Virtual Reality Exergames and Traditional Video Exercises

 ,
, 
Abstract
:1. Introduction
2. Related Work
2.1. Fitness in Old Age
2.2. Serious Games for Older Adults
3. Materials and Methods
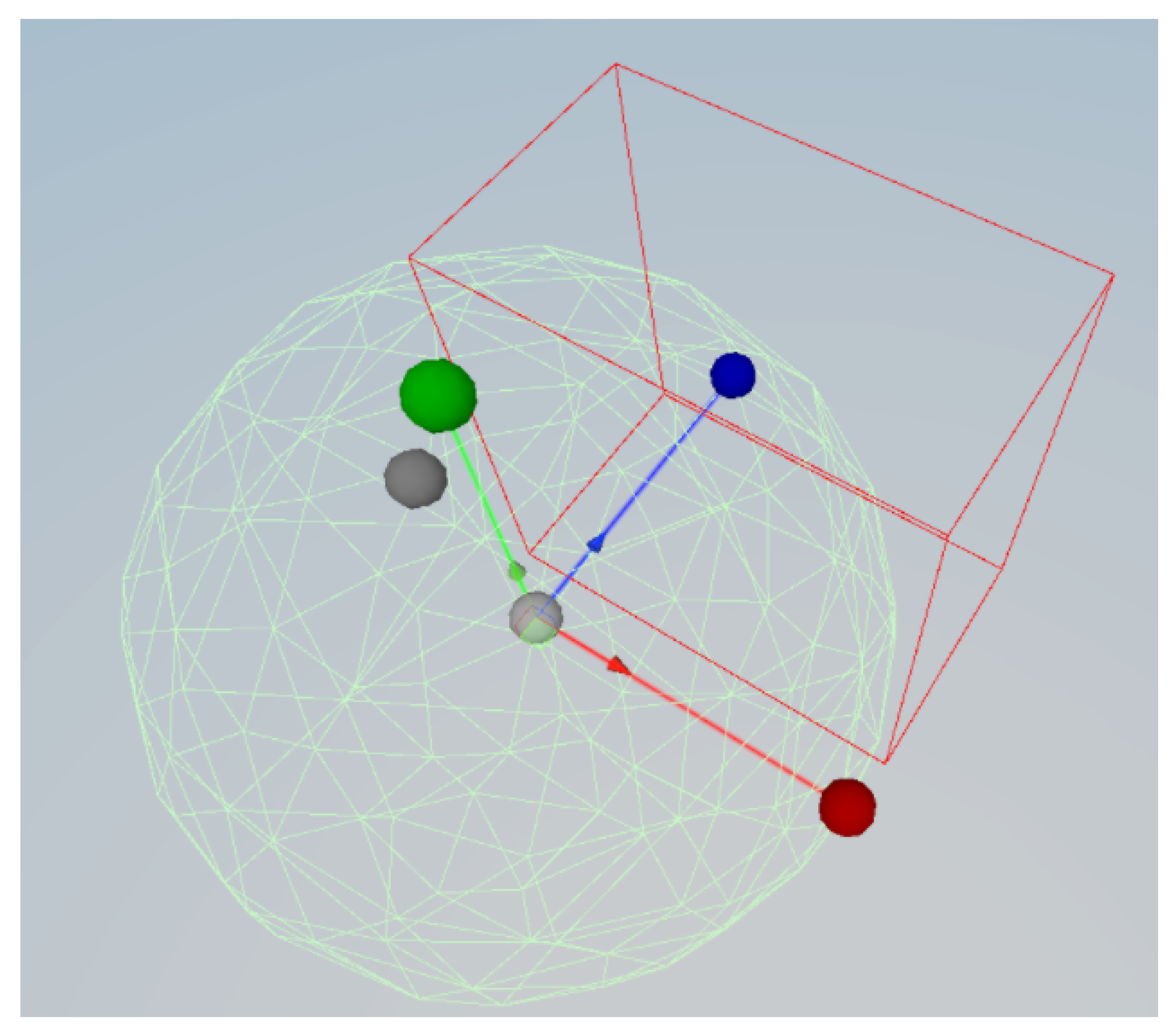
3.1. VR Exergame: Maestro Game VR
- A disco ball which the player is supposed to follow with the tip of the baton.
- A tunnel with staff lines extending before and after the disco ball to help the player anticipate the target’s path.
- Music notes that regularly spawn along the tunnel to calculate the player’s accuracy when the disco ball hits them.
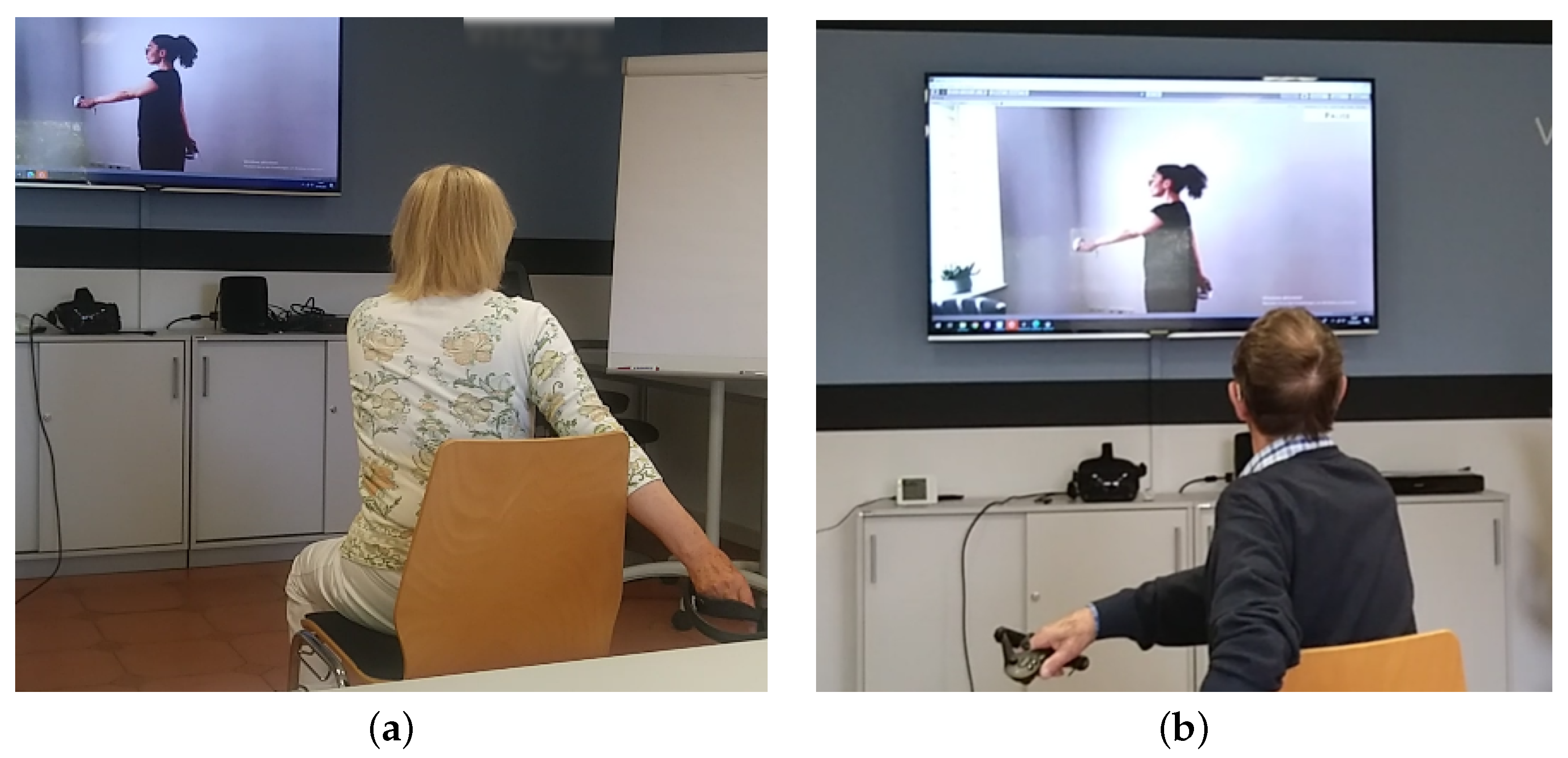
3.2. Exercise Video
- Side arm raises ();
- Neck lateral flexion stretch ();
- Neck rotation to the sides ();
- Neck flexion/extension forward and backward ();
- Shoulder circles to the front ();
- Shoulder circles to the front, including elbows ();
- Shoulder circles to the back ();
- Shoulder circles to the back including elbows ();
- Arm circles to the front ();
- Arm circles to the back ();
- Torso rotations ();
- Punches to the upper sides ();
- Overhead punches ();
- Side arm raises ().
3.3. User Study
3.3.1. Pre-Study
3.3.2. Participants
3.3.3. Measurements
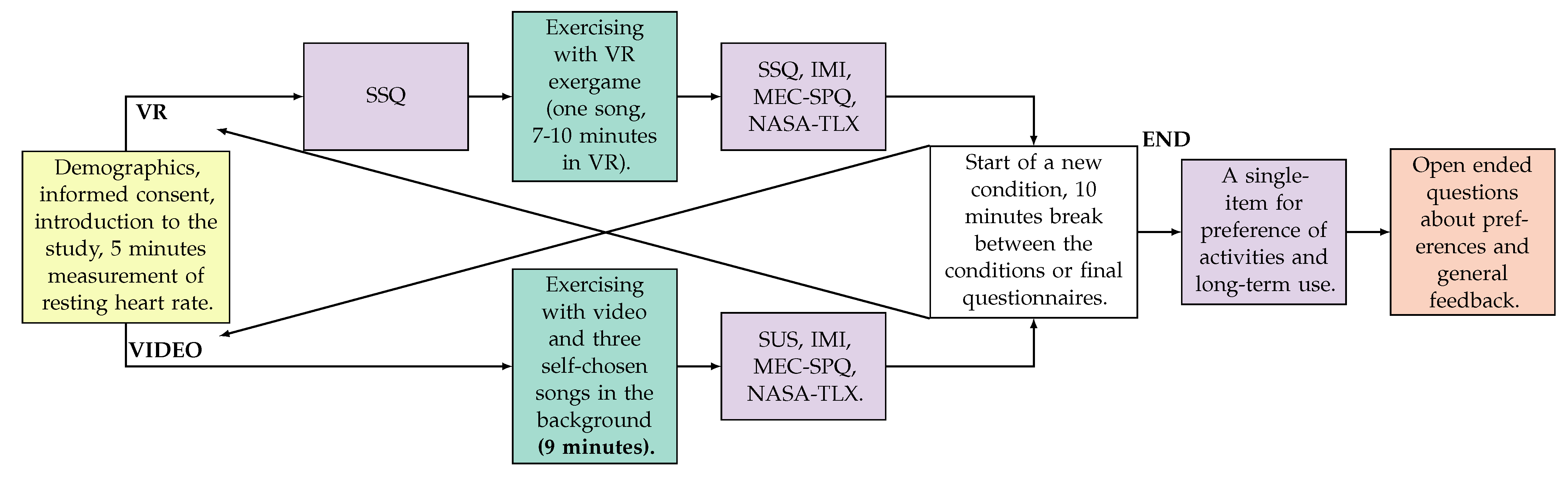
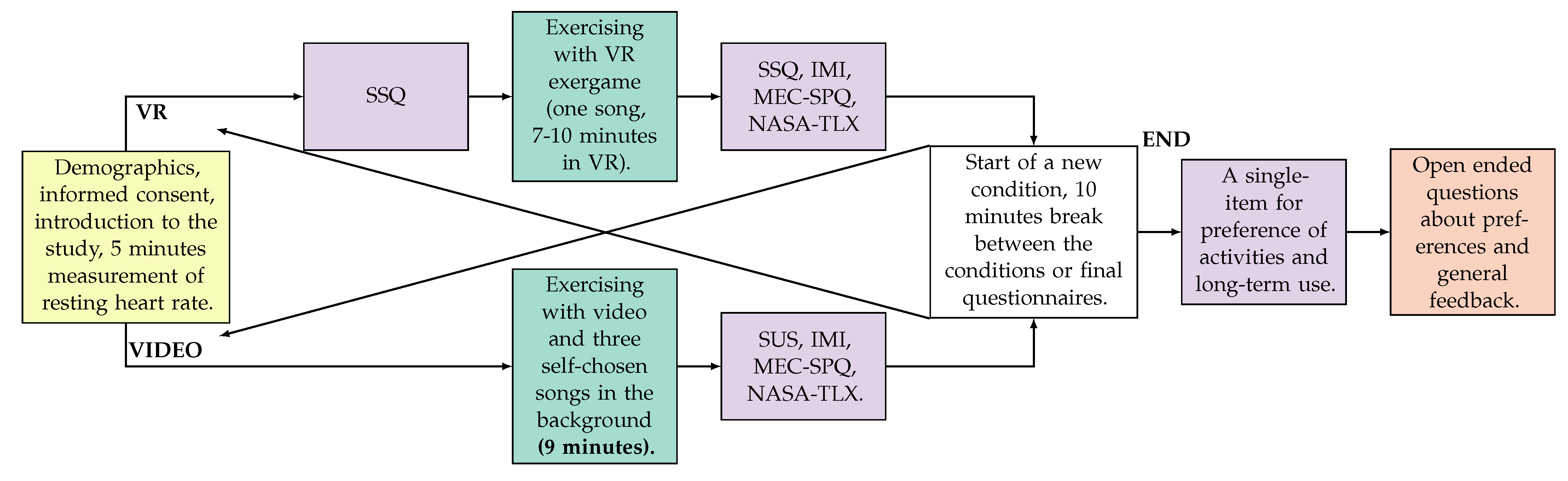
3.3.4. Procedure
4. Evaluation
4.1. Questionnaires
4.2. Heart Rate Data
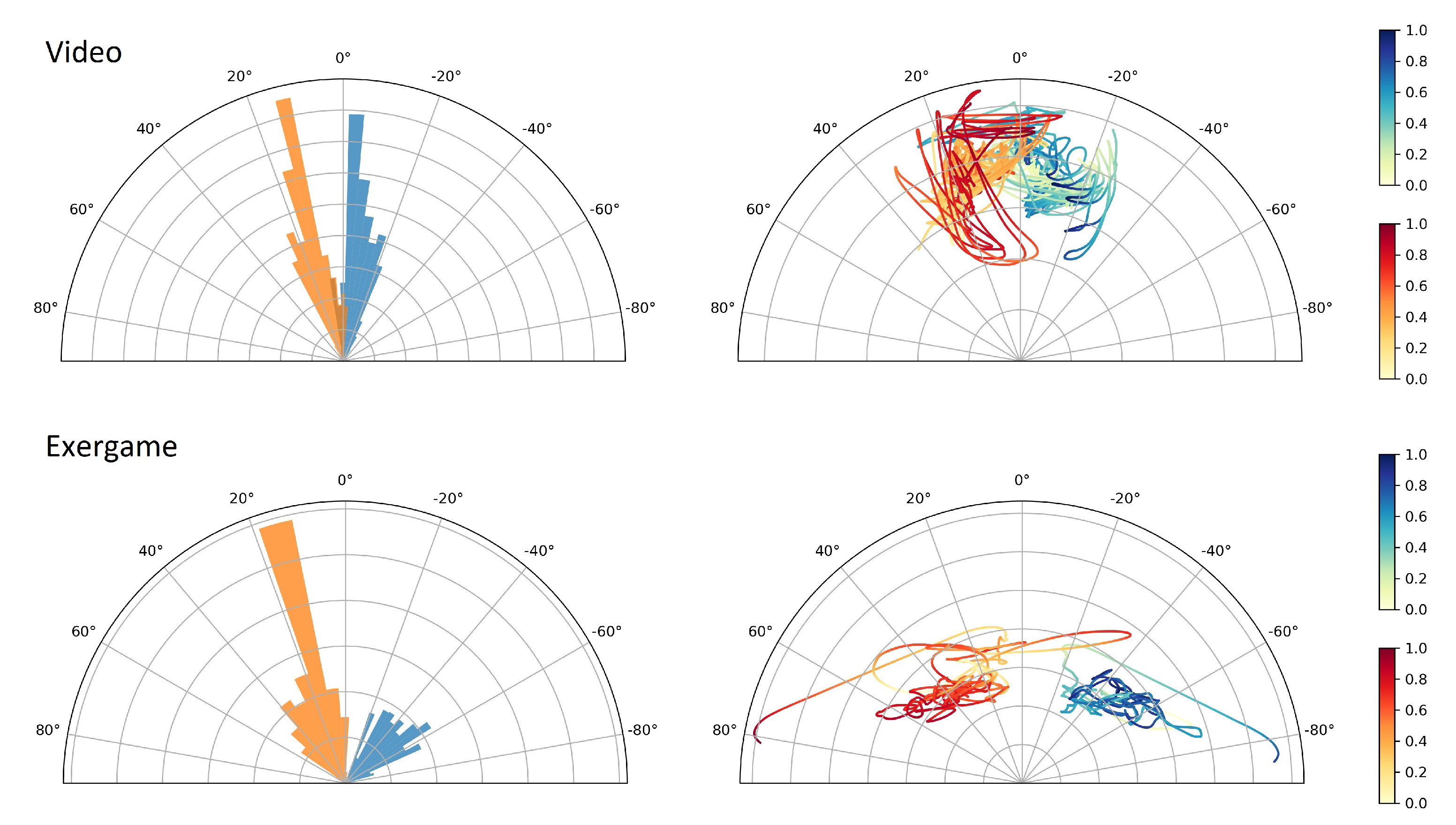
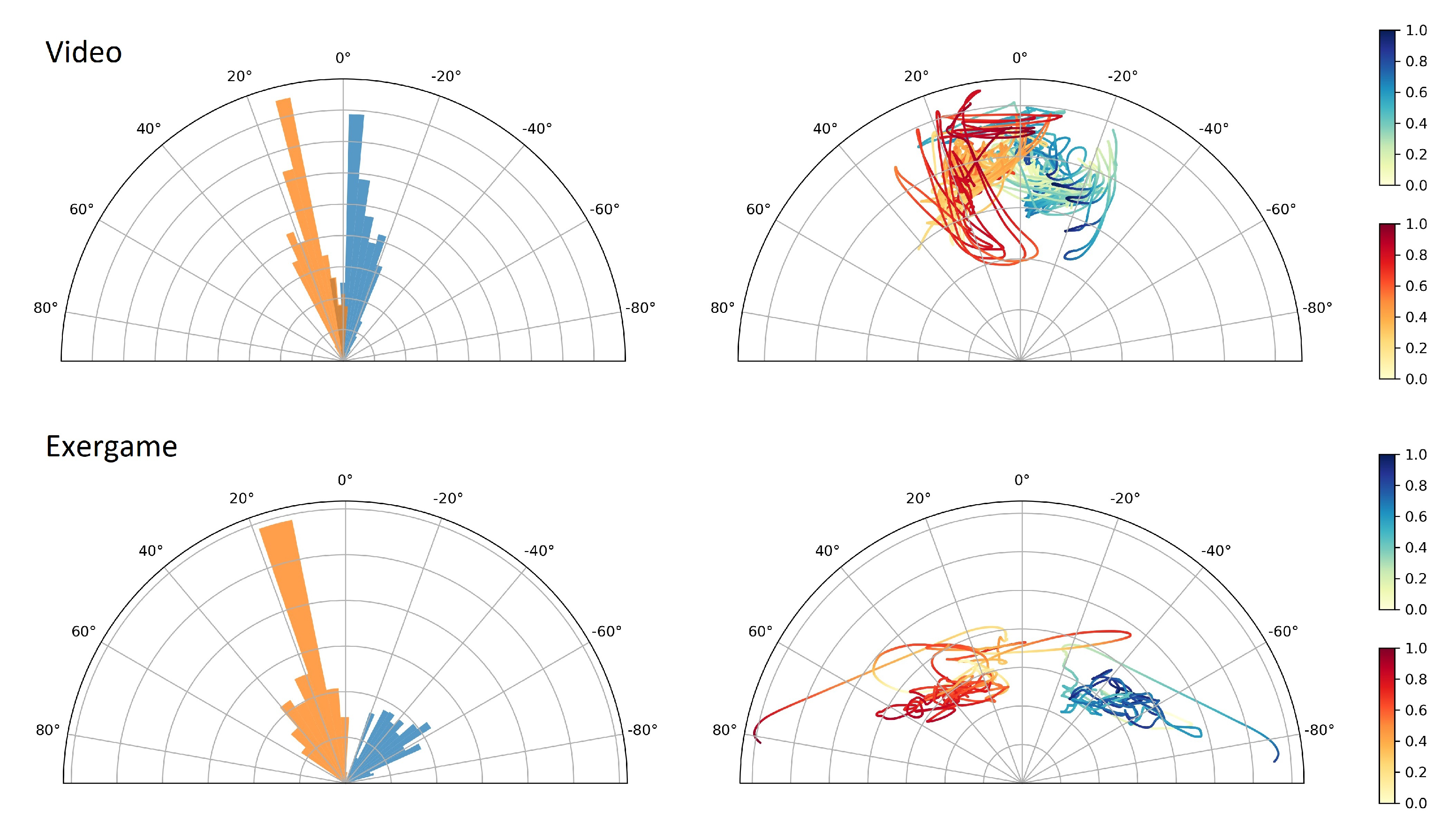
4.3. Movement Data
4.4. Qualitative Feedback
5. Discussion
Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| VR | Virtual Reality |
| VE | Virtual Environment |
| IVE | Immersive Virtual Environment |
| HMD | Head-Mounted Display |
| 1 | https://unity.com/accessed on 6 November 2021 |
| 2 | https://beatsaber.com/ accessed on 6 November 2021 |
| 3 | https://ohshapevr.com/ accessed on 6 November 2021 |
| 4 | https://www.polar.com/products/accessories/oh1-optical-heart-rate-sensor accessed on 28 September 2021 |
| 5 | https://jasp-stats.org/ accessed on 6 November 2021 |
References
- Liu-Ambrose, T.; Donaldson, M.G.; Ahamed, Y.; Graf, P.; Cook, W.L.; Close, J.; Lord, S.R.; Khan, K.M. Otago home-based strength and balance retraining improves executive functioning in older fallers: A randomized controlled trial. J. Am. Geriatr. Soc. 2008, 56, 1821–1830. [Google Scholar] [CrossRef]
- Langlois, F.; Vu, T.T.M.; Chassé, K.; Dupuis, G.; Kergoat, M.J.; Bherer, L. Benefits of physical exercise training on cognition and quality of life in frail older adults. J. Gerontol. Ser. B 2013, 68, 400–404. [Google Scholar] [CrossRef]
- Hogan, M. Physical and cognitive activity and exercise for older adults: A review. Int. J. Aging Hum. Dev. 2005, 60, 95–126. [Google Scholar] [CrossRef] [PubMed]
- Hauer, K.; Schwenk, M.; Zieschang, T.; Essig, M.; Becker, C.; Oster, P. Physical training improves motor performance in people with dementia: A randomized controlled trial. J. Am. Geriatr. Soc. 2012, 60, 8–15. [Google Scholar] [CrossRef]
- Hall, C.D.; Smith, A.L.; Keele, S.W. The impact of aerobic activity on cognitive function in older adults: A new synthesis based on the concept of executive control. Eur. J. Cogn. Psychol. 2001, 13, 279–300. [Google Scholar] [CrossRef]
- Gajewski, P.D.; Falkenstein, M. Physical activity and neurocognitive functioning in aging—A condensed updated review. Eur. Rev. Aging Phys. Act. 2016, 13, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Schlichtiger, J.; Steffen, J.; Huber, B.C.; Brunner, S. Physical activity during COVID-19 lockdown in older adults. J. Sport. Med. Phys. Fit. 2021, 61, 1. [Google Scholar]
- Simek, E.M.; McPhate, L.; Haines, T.P. Adherence to and efficacy of home exercise programs to prevent falls: A systematic review and meta-analysis of the impact of exercise program characteristics. Prev. Med. 2012, 55, 262–275. [Google Scholar] [CrossRef]
- Department, S.R. Distribution of Opinions of Adults on the Preferred Use of Virtual Reality (VR) for Personal Fitness Training in Great Britain (GB) in 2019. 2019. Available online: https://0-www-statista-com.brum.beds.ac.uk/statistics/1137335/distribution-of-opinions-on-the-preferred-use-of-vr-for-personal-fitness-training/ (accessed on 13 July 2021).
- Oh, Y.; Yang, S. Defining exergames & exergaming. Proc. Mean. Play 2010, 2010, 21–23. [Google Scholar]
- Johnson, J. Effect of COVID-19 on Online Fitness Video Usage in the U.S. 2020. 2021. Available online: https://0-www-statista-com.brum.beds.ac.uk/statistics/1108538/online-fitness-video-usage-during-coronavirus-usa/ (accessed on 12 July 2021).
- Chodzko-Zajko, W.J.; Proctor, D.N.; Singh, M.A.F.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sport. Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Schaie, K.W.; Willis, S.L. Handbook of the Psychology of Aging; Academic Press: Cambridge, MA, USA, 2010. [Google Scholar]
- de Bruijn, R.F.; Schrijvers, E.M.; de Groot, K.A.; Witteman, J.C.; Hofman, A.; Franco, O.H.; Koudstaal, P.J.; Ikram, M.A. The association between physical activity and dementia in an elderly population: The Rotterdam Study. Eur. J. Epidemiol. 2013, 28, 277–283. [Google Scholar] [CrossRef]
- Rolland, Y.; Pillard, F.; Klapouszczak, A.; Reynish, E.; Thomas, D.; Andrieu, S.; Rivière, D.; Vellas, B. Exercise program for nursing home residents with Alzheimer’s disease: A 1-year randomized, controlled trial. J. Am. Geriatr. Soc. 2007, 55, 158–165. [Google Scholar] [CrossRef]
- Mutz, M.; Gerke, M. Sport and exercise in times of self-quarantine: How Germans changed their behaviour at the beginning of the Covid-19 pandemic. Int. Rev. Sociol. Sport 2021, 56, 305–316. [Google Scholar] [CrossRef]
- Jette, A.M.; Harris, B.A.; Sleeper, L.; Lachman, M.E.; Heislein, D.; Giorgetti, M.; Levenson, C. A home-based exercise program for nondisabled older adults. J. Am. Geriatr. Soc. 1996, 44, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Gschwind, Y.J.; Schoene, D.; Lord, S.R.; Ejupi, A.; Valenzuela, T.; Aal, K.; Woodbury, A.; Delbaere, K. The effect of sensor-based exercise at home on functional performance associated with fall risk in older people—A comparison of two exergame interventions. Eur. Rev. Aging Phys. Act. 2015, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Davis, J.C.; Best, J.R.; Dian, L.; Madden, K.; Cook, W.; Hsu, C.L.; Khan, K.M. Effect of a home-based exercise program on subsequent falls among community-dwelling high-risk older adults after a fall: A randomized clinical trial. JAMA 2019, 321, 2092–2100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vestergaard, S.; Kronborg, C.; Puggaard, L. Home-based video exercise intervention for community-dwelling frail older women: A randomized controlled trial. Aging Clin. Exp. Res. 2008, 20, 479–486. [Google Scholar] [CrossRef]
- Campbell, A.; Robertson, M.C. Otago Exercise Programme to Prevent Falls in Older Adults; ACC Thinksafe: Wellington, New Zealand, 2003; Volume 3. [Google Scholar]
- Mehra, S.; Visser, B.; Cila, N.; van den Helder, J.; Engelbert, R.H.; Weijs, P.J.; Kröse, B.J. Supporting older adults in exercising with a tablet: A usability study. JMIR Hum. Factors 2019, 6, e11598. [Google Scholar] [CrossRef]
- Simek, E.M.; McPhate, L.; Hill, K.D.; Finch, C.F.; Day, L.; Haines, T.P. What are the characteristics of home exercise programs that older adults prefer?: A cross-sectional study. Am. J. Phys. Med. Rehabil. 2015, 94, 508–521. [Google Scholar] [CrossRef]
- Eisapour, M.; Cao, S.; Domenicucci, L.; Boger, J. Virtual reality exergames for people living with dementia based on exercise therapy best practices. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting; SAGE Publication: Los Angeles, CA, USA, 2018; Volume 62, pp. 528–532. [Google Scholar]
- Rings, S.; Karaosmanoglu, S.; Kruse, L.; Apken, D.; Picker, T.; Steinicke, F. Using Exergames to Train Patients with Dementia to Accomplish Daily Routines. In Proceedings of the Extended Abstracts of the 2020 Annual Symposium on Computer-Human Interaction in Play, Virtual Event, Canada, 2–4 November 2020; pp. 345–349. [Google Scholar]
- Weisman, S. Computer games for the frail elderly. Gerontologist 1983, 23, 361–363. [Google Scholar] [CrossRef]
- Tait, J.L.; Duckham, R.L.; Milte, C.M.; Main, L.C.; Daly, R.M. Influence of sequential vs. simultaneous dual-task exercise training on cognitive function in older adults. Front. Aging Neurosci. 2017, 9, 368. [Google Scholar] [CrossRef]
- Gschwind, Y.J.; Eichberg, S.; Ejupi, A.; de Rosario, H.; Kroll, M.; Marston, H.R.; Drobics, M.; Annegarn, J.; Wieching, R.; Lord, S.R.; et al. ICT-based system to predict and prevent falls (iStoppFalls): Results from an international multicenter randomized controlled trial. Eur. Rev. Aging Phys. Act. 2015, 12, 10. [Google Scholar] [CrossRef] [Green Version]
- Kruse, L.; Karaosmanoglu, S.; Rings, S.; Ellinger, B.; Apken, D.; Mangana, T.F.; Steinicke, F. A Long-Term User Study of an Immersive Exergame for Older Adults with Mild Dementia during the COVID-19 Pandemic. In ICAT-EGVE 2021—International Conference on Artificial Reality and Telexistence and Eurographics Symposium on Virtual Environments; Orlosky, J., Reiners, D., Weyers, B., Eds.; The Eurographics Association: Goslar, Germany, 2021. [Google Scholar] [CrossRef]
- Mulvenna, M.D.; Nugent, C.D.; Moelaert, F.; Craig, D.; Dröes, R.M.; Bengtsson, J.E. Supporting people with dementia using pervasive healthcare technologies. In Supporting People with Dementia Using Pervasive Health Technologies; Springer: London, UK, 2010; pp. 3–14. [Google Scholar]
- Unbehaun, D.; Taugerbeck, S.; Aal, K.; Vaziri, D.D.; Lehmann, J.; Tolmie, P.; Wieching, R.; Wulf, V. Notes of memories: Fostering social interaction, activity and reminiscence through an interactive music exergame developed for people with dementia and their caregivers. Hum. Comput. Interact. 2020, 36, 439–472. [Google Scholar] [CrossRef]
- Lilla, D.; Herrlich, M.; Malaka, R.; Krannich, D. The influence of music on player performance in exergames for parkinson’s patients. In International Conference on Entertainment Computing; Springer: Berlin/Heidelberg, Germany, 2012; pp. 433–436. [Google Scholar]
- Gerling, K.M.; Schild, J.; Masuch, M. Exergame design for elderly users: The case study of SilverBalance. In Proceedings of the 7th International Conference on Advances in Computer Entertainment Technology, Taipei, Taiwan, 17–19 November 2010; pp. 66–69. [Google Scholar]
- Gerling, K.M.; Schild, J.; Masuch, M. Exergaming for elderly persons: Analyzing player experience and performance. In Mensch Comput. überMEDIEN| ÜBERmorgen; Oldenbourg Wissenschaftsverlag: Munich, Germany, 2011. [Google Scholar]
- van Diest, M.; Stegenga, J.; Wörtche, H.J.; Verkerke, G.J.; Postema, K.; Lamoth, C.J. Exergames for unsupervised balance training at home: A pilot study in healthy older adults. Gait Posture 2016, 44, 161–167. [Google Scholar] [CrossRef]
- Unbehaun, D.; Vaziri, D.D.; Aal, K.; Wieching, R.; Tolmie, P.; Wulf, V. Exploring the Potential of Exergames to affect the Social and Daily Life of People with Dementia and their Caregivers. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems, Montreal, QC, Canada, 21–26 April 2018; pp. 1–15. [Google Scholar]
- Unbehaun, D.; Aal, K.; Vaziri, D.D.; Wieching, R.; Tolmie, P.; Wulf, V. Facilitating Collaboration and Social Experiences with Videogames in Dementia: Results and Implications from a Participatory Design Study. Proc. ACM Hum. Comput. Interact. 2018, 2, 1–23. [Google Scholar] [CrossRef]
- Unbehaun, D.; Vaziri, D.; Aal, K.; Li, Q.; Wieching, R.; Wulf, V. MobiAssist-ICT-based Training System for People with Dementia and Their Caregivers: Results from a Field Study. In Proceedings of the 2018 ACM Conference on Supporting Groupwork, Sanibel Island, FL, USA, 7–10 January 2018; pp. 122–126. [Google Scholar]
- Xu, W.; Liang, H.N.; Zhang, Z.; Baghaei, N. Studying the effect of display type and viewing perspective on user experience in virtual reality exergames. Games Health J. 2020, 9, 405–414. [Google Scholar] [CrossRef]
- Xu, W.; Liang, H.N.; Yu, K.; Baghaei, N. Effect of Gameplay Uncertainty, Display Type, and Age on Virtual Reality Exergames. In Proceedings of the 2021 CHI Conference on Human Factors in Computing Systems, Yokohama, Japan, 8–13 May 2021; pp. 1–14. [Google Scholar]
- Huang, K.T. Exergaming executive functions: An immersive virtual reality-based cognitive training for adults aged 50 and older. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Eisapour, M.; Cao, S.; Domenicucci, L.; Boger, J. Participatory design of a virtual reality exercise for people with mild cognitive impairment. In Proceedings of the Extended Abstracts of the 2018 CHI Conference on Human Factors in Computing Systems, Montreal, QC, Canada, 21–26 April 2018; pp. 1–9. [Google Scholar]
- Rings, S.; Steinicke, F.; Picker, T.; Prasuhn, C. Memory Journalist: Creating Virtual Reality Exergames for the Treatment of Older Adults with Dementia. In Proceedings of the IEEE Virtual Reality (VR) (Poster Presentation), Atlanta, GA, USA, 22–26 March 2020. [Google Scholar]
- Karaosmanoglu, S.; Rings, S.; Kruse, L.; Stein, C.; Steinicke, F. Lessons Learned from a Human-Centered Design of an Immersive Exergame for People with Dementia. PACM Hum. Comput. Interact. 2021, 5, 1–27. [Google Scholar]
- Cobb, S.V.; Nichols, S.; Ramsey, A.; Wilson, J.R. Virtual reality-induced symptoms and effects (VRISE). Presence Teleoperators Virtual Environ. 1999, 8, 169–186. [Google Scholar] [CrossRef]
- Stamm, O.; Vorwerg, S. Virtual Reality Sickness Evaluation in Exergames for Older Hypertensive Patients: A Comparative Study of Training Methods in a Virtual Environment. In International Conference on Human-Computer Interaction; Springer: Berlin/Heidelberg, Germany, 2021; pp. 134–146. [Google Scholar]
- Schraepen, B.; Huygelier, H.; Van Ee, R.; Vanden Abeele, V.; Gillebert, C. Attitudes towards and Usability of Head-mounted Virtual Reality in Older Adults. In Proceedings of the CHI PLAY, Amsterdam, The Netherlands, 15–18 October 2017. [Google Scholar]
- Hennequin, R.; Khlif, A.; Voituret, F.; Moussallam, M. Spleeter: A fast and efficient music source separation tool with pre-trained models. J. Open Source Softw. 2020, 5, 2154. [Google Scholar] [CrossRef]
- Kaur, H.; Singh, T.; Arya, Y.K.; Mittal, S. Physical fitness and exercise during the COVID-19 pandemic: A qualitative enquiry. Front. Psychol. 2020, 11, 2943. [Google Scholar] [CrossRef]
- NHS. Sitting Exercises. 2021. Available online: https://www.nhs.uk/live-well/exercise/sitting-exercises/ (accessed on 6 November 2021).
- Yoga, G. Wellness. Standing Yoga for Seniors—Yoga for Seniors—Standing Yoga—Senior Yoga. 2021. Available online: https://youtu.be/y5DbD0Zl-Kg (accessed on 6 November 2021).
- yes2next. Warm up for Seniors. 2020. Available online: https://youtu.be/9khVr_NtBxI (accessed on 6 November 2021).
- yes2next. 16 min. Senioren-Gymnastik am Morgen|ohne Geräte, im Stehen. 2020. Available online: https://youtu.be/BQnxFLkXAAI (accessed on 6 November 2021).
- yes2next. 13 min. Sanfte Senioren-Gymnastik im Stehen, ohne Hilfsmittel. 2019. Available online: https://youtu.be/IRZXXcjfgOs (accessed on 6 November 2021).
- Xu, W.; Liang, H.N.; He, Q.; Li, X.; Yu, K.; Chen, Y. Results and Guidelines From a Repeated-Measures Design Experiment Comparing Standing and Seated Full-Body Gesture-Based Immersive Virtual Reality Exergames: Within-Subjects Evaluation. JMIR Serious Games 2020, 8, e17972. [Google Scholar] [CrossRef]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator sickness questionnaire: An enhanced method for quantifying simulator sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Intrinsic Motivation Inventory. 1982. Available online: http://selfdeterminationtheory.org/intrinsic-motivation-inventory/ (accessed on 6 November 2021).
- Wilde, M.; Bätz, K.; Kovaleva, A.; Urhahne, D. Überprüfung einer Kurzskala intrinsischer Motivation (KIM). Z. Didakt. Naturwissenschaften 2009, 15, 31–45. [Google Scholar]
- Vorderer, P.; Wirth, W.; Gouveia, F.R.; Biocca, F.; Saari, T.; Jäncke, L.; Böcking, S.; Schramm, H.; Gysbers, A.; Hartmann, T.; et al. Mec spatial presence questionnaire. Retrieved Sept 2004, 18, 2015. [Google Scholar]
- Slater, M.; Usoh, M.; Steed, A. Depth of presence in virtual environments. Presence Teleoperators Virtual Environ. 1994, 3, 130–144. [Google Scholar] [CrossRef]
- Hart, S.G.; Staveland, L.E. Development of NASA-TLX (Task Load Index): Results of empirical and theoretical research. In Advances in Psychology; Elsevier: Amsterdam, The Netherlands, 1988; Volume 52, pp. 139–183. [Google Scholar]
- Jarosz, A.F.; Wiley, J. What are the odds? A practical guide to computing and reporting Bayes factors. J. Probl. Solving 2014, 7, 2. [Google Scholar] [CrossRef] [Green Version]
- Kass, R.E.; Raftery, A.E. Bayes factors. J. Am. Stat. Assoc. 1995, 90, 773–795. [Google Scholar] [CrossRef]
- Raftery, A.E. Bayesian model selection in social research. Sociol. Methodol. 1995, 25, 111–163. [Google Scholar] [CrossRef]
- Slater, M.; Lotto, B.; Arnold, M.M.; Sánchez-Vives, M.V. How we experience immersive virtual environments: The concept of presence and its measurement. Anu. Psicol. 2009, 40, 193–210. [Google Scholar]
- Epstein, R.A.; Patai, E.Z.; Julian, J.B.; Spiers, H.J. The cognitive map in humans: Spatial navigation and beyond. Nat. Neurosci. 2017, 20, 1504–1513. [Google Scholar] [CrossRef] [PubMed]
- Armbrüster, C.; Wolter, M.; Kuhlen, T.; Spijkers, W.; Fimm, B. Depth perception in virtual reality: Distance estimations in peri-and extrapersonal space. Cyberpsychol. Behav. 2008, 11, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Karaosmanoglu, S.; Rogers, K.; Wolf, D.; Rukzio, E.; Steinicke, F.; Nacke, L.E. Feels like Team Spirit: Biometric and Strategic Interdependence in Asymmetric Multiplayer VR Games. In CHI ’21: Proceedings of the 2021 CHI Conference on Human Factors in Computing Systems; Association for Computing Machinery: New York, NY, USA, 2021. [Google Scholar] [CrossRef]
- DiDomenico, A.; Nussbaum, M.A. Interactive effects of physical and mental workload on subjective workload assessment. Int. J. Ind. Ergon. 2008, 38, 977–983. [Google Scholar] [CrossRef]
- Miller, K.J.; Adair, B.S.; Pearce, A.J.; Said, C.M.; Ozanne, E.; Morris, M.M. Effectiveness and feasibility of virtual reality and gaming system use at home by older adults for enabling physical activity to improve health-related domains: A systematic review. Age Ageing 2014, 43, 188–195. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Conditions | Pre-SSQ | Post-SSQ | IMI | MEC-SPQ | NASA-TLX | Heart Rate | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| VR Exergame | 8.98 | 11.48 | 8.08 | 11.46 | 4.57 | 0.63 | 4.44 | 0.72 | 19.77 | 11.91 | 76.77 | 9.8 |
| Exercise Video | — | — | — | — | 4.6 | 0.68 | 4.63 | 0.56 | 17.23 | 10.94 | 81.97 | 11.56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kruse, L.; Karaosmanoglu, S.; Rings, S.; Ellinger, B.; Steinicke, F. Enabling Immersive Exercise Activities for Older Adults: A Comparison of Virtual Reality Exergames and Traditional Video Exercises. Societies 2021, 11, 134. https://0-doi-org.brum.beds.ac.uk/10.3390/soc11040134
Kruse L, Karaosmanoglu S, Rings S, Ellinger B, Steinicke F. Enabling Immersive Exercise Activities for Older Adults: A Comparison of Virtual Reality Exergames and Traditional Video Exercises. Societies. 2021; 11(4):134. https://0-doi-org.brum.beds.ac.uk/10.3390/soc11040134
Chicago/Turabian StyleKruse, Lucie, Sukran Karaosmanoglu, Sebastian Rings, Benedikt Ellinger, and Frank Steinicke. 2021. "Enabling Immersive Exercise Activities for Older Adults: A Comparison of Virtual Reality Exergames and Traditional Video Exercises" Societies 11, no. 4: 134. https://0-doi-org.brum.beds.ac.uk/10.3390/soc11040134