
Diversity Competence in Healthcare: Experts’ Views on the Most Important Skills in Caring for Migrant and Minority Patients

Abstract
:1. Introduction
2. Methods
2.1. Sample Size and Selection of Experts
2.2. Expert Panel and Study Schedule
2.3. Design and Analysis of Round 1: Collection of Most Important Diversity Competences
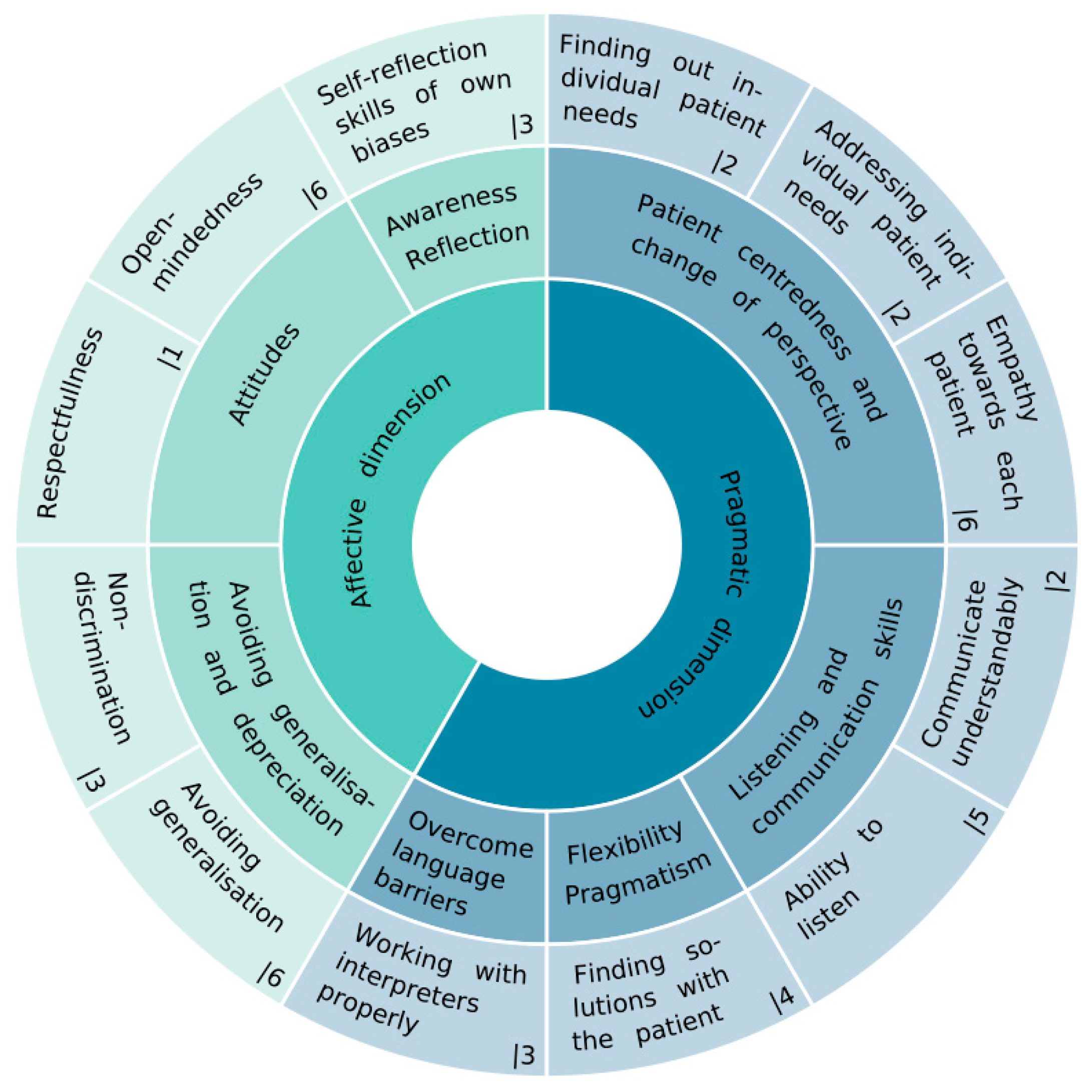
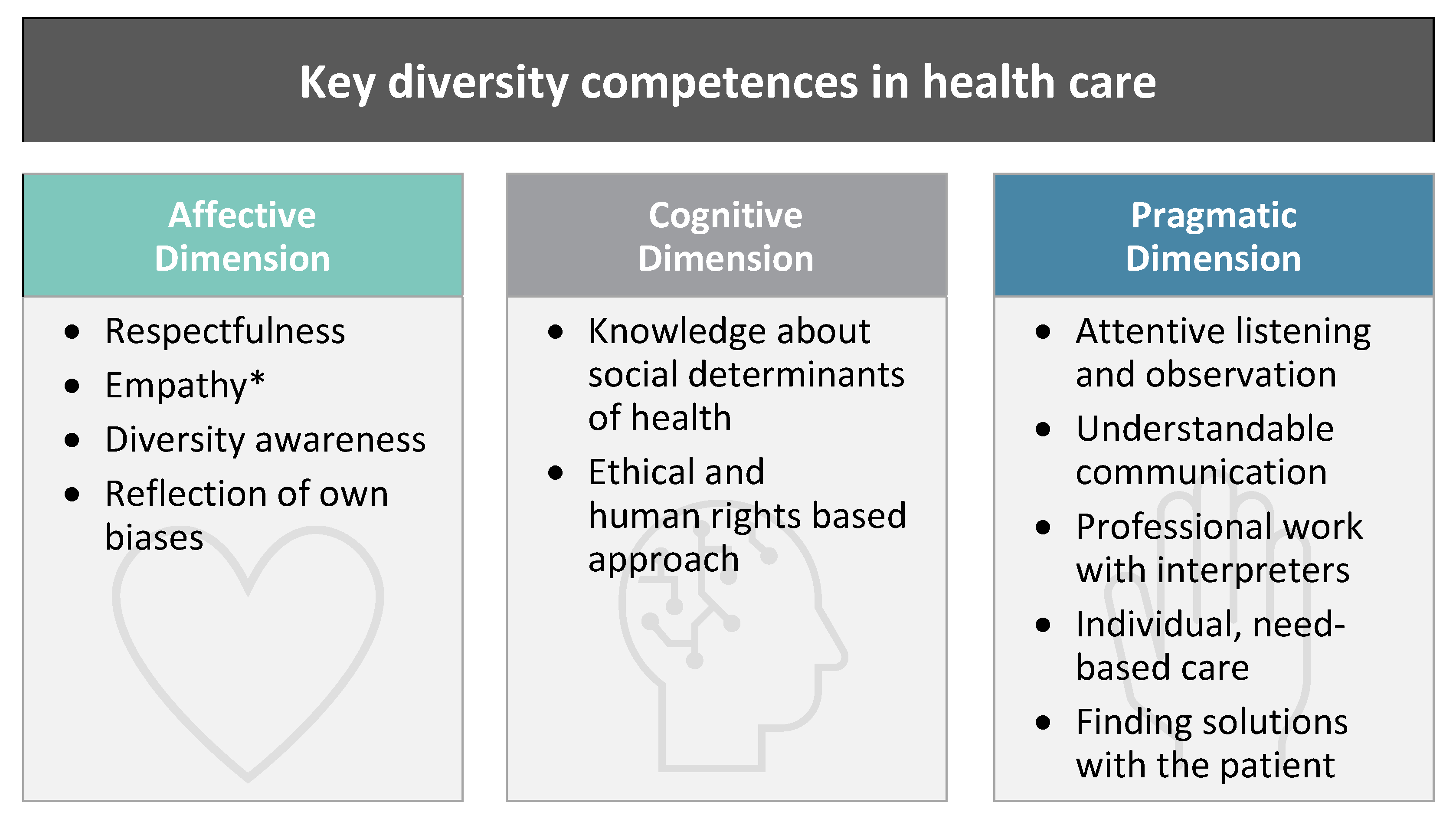
‘Diversity competence is most commonly described as consisting of three key dimensions: affective, cognitive, and pragmatic. The affective dimension includes what we want, what we think about things and people, how we feel and how we deal with these feelings. The cognitive dimension includes what we know, consider and reflect upon. The pragmatic dimension includes what we are able to do. With this in mind, what are—in your opinion—the three most important qualities/abilities/skills that a health professional should possess in order to provide good and diversity-sensitive healthcare, especially to migrant and ethnic minority patients?’
2.4. Design and Analysis of Round 2: Prioritisation of Diversity Competences

{kind=link}
{kind=link}
| Affective Dimension | Number of Items |
|---|---|
| ATTITUDES | |
| 7 |
| 3 |
| AWARENESS | |
| 2 |
| 5 |
| 7 |
| 4 |
| Cognitive Dimension | |
| KNOWLEDGE | |
| 6 |
| 6 |
| 4 |
| 3 |
| Pragmatic Dimension | |
| SKILLS | |
| 3 |
| 1 |
| 4 |
| 3 |
| 2 |
| 4 |
| 3 |
| 2 |
3. Results
3.1. Affective Dimension
In the affective dimension, the professional should be open-minded and be curious so [as] to allow them to learn from the patient, especially around health issues affecting patient’s life and how to solve them even when the strategies might be different from those of biomedicine. The first step is to be reflective and critical about [the] professional’s power position in relation to patients, and the second, the willingness to change(AER11)
Develop more understanding of the effects of the diversity dimension on conflicts, tension, misunderstandings, or opportunities(AETR1)
To gain information about the meaning of the diversity dimensions in the healthcare system (including: knowledge about Diversity Self-Awareness) […](AETR1)
3.2. Cognitive Dimension
Self-reflection (affective, cognitive and pragmatic) about social-cultural background, context and position (‘positionally‘) and not exclusively focusing on the ‘culture’ of the ‘other’!(AER1)
I have serious doubts if there is any useful knowledge on ‘cultures’, using the plural of this word and thus an essentialist concept of ‘cultures’ that can be described and distinguished one from the other. I think it’s important to talk about ‘culture’ yet problematic to talk about ‘cultures’ (the only useful way of doing this in teaching is probably by satire and irony for triggering reflection on stereotype etc.)(AER2)
3.3. Pragmatic Dimension
Communication skills are also important—both in listening as well as imparting information to others, including verbal and nonverbal communication. Poor communication can easily shut down or swing the focus of a healthcare encounter wildly off course—there are countless examples of this—and can delay diagnosis, lead to unnecessary investigations and/or inaccurate diagnoses, and thus harm the patient. Poor communication also makes healthcare encounters uncomfortable for health workers, and may influence the way they interact with patients from other ethnic or cultural backgrounds in the future.(HPR1)
In the pragmatic dimension, professionals should listen instead of asking and talking all the time(AER1)
Communication: listening, creating a bearing/empathic/attentive relationship to patient and relatives(AER1)
The art of listening has been lost, in the development of cultural competence listening is basic(AER1)
All […] attributes […] should ideally be informed by empathy: an ability to put yourself in the other’s shoes, no matter who they are(AER1)
Rather than relying exclusively on a preconceived knowledge about patients’ assumptions and expectations, professionals should develop a critical thinking in order to be able to recognise and reflect upon the unique experience of the patient based on the dynamic intersection of factors which are generally not lived in isolation, and to respond to them in an integrated and comprehensive way(AER1)
To see the patient as an ‘individual’, while keep in mind that group dynamics and belonging to a particular (cultural/ethnic) group can affect ‘individuality’(AETR1)
To leave his rationality and try to understand the needs, the problems, the world of the person(AETR1)
Ability to understand patients’ context and sociocultural representations. Knowing the immigrant patient involves their daily life, the difficulties faced, the supportive environment they have and what is significant in their health from their individual and cultural perspective(HPR1)
- (1)
- it ‘is very important but also a very delicate issue’ (AER2) and
- (2)
- it ‘is important as long as the patient demands help or agrees to be helped by the professional. Caution should be exercised because not all people who have suffered trauma, whether or not linked to the migration process, want to relieve and share it’ (HPR2).
3.4. Structural Competence: An Issue Cutting across All Diversity Dimensions
Structural Factors and Public Health Approach: To know how the administrative situation of the immigrant in the host country (legal or illegal) influences his/her health status, due to the numerous socio-economic conditions, and to know what these are(HPR2)
[…] The first step is to be reflective and critical about [the] professional’s power position in relation to patients(AER1)
[Reflection on] various forms of abuse of power (conscious and/or unconscious), paternalism and any other form of imbalance of power in the relationship between health professionals and patients(HPR2)
Self-reflection […] including individual and structural racism(AETR1)
[Knowledge on] the influence of social exclusion and discrimination(HPR1)
4. Discussion
Diversity-competent health professionals respect their patients and are aware of the wide variety of possible attributes and collective memberships that all participants bring to a healthcare encounter. They can reflect on their own biases and strive towards equitable treatment, applying an ethical, human rights-based approach. Their competence also includes knowledge on social determinants that can affect the health of their patients. Diversity competent health professionals can communicate understandably and are empathetic listeners, who identify and address the individual needs of each patient and find solutions together. If necessary, they are able to work with interpreters in a professional manner.
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
| 1 | Pseudonyms only refer to professions and rounds, without individual assignment: HP = Health Professional, AE = Academic Expert (AET, in case the AE is additionally a diversity trainer or teacher); statements from Round 1 = R1, from Round 2 = R2. |
| 2 | Multiple answers possible regarding the current job position. |
| 3 | ‘It is a spectrum of complex abilities that are more or less closely bound to the person, which in part can only be influenced to a limited extent by educational offers or can only be initiated as a learning process by the subject himself’ (Leenen et al., 2013, p 114; own translation). |
| 4 | He mentions experiences of discrimination and after-effects of colonial history as examples (Auernheimer 2013, p 118). |
| 5 | The real goal of diversity competence training is to reach a level of normalisation in dealing with perceived and constructed differences, thereby making acts of naming, and reflection on diversity obsolete. |
References
- Hansen, K.P. Kultur und Kulturwissenschaft; UTB: Paderborn, Germany, 2000. [Google Scholar]
- Hansen, K.P. Kultur, Kollektivität, Nation; Stutz: Passau, Germany, 2009. [Google Scholar]
- Rathje, S. The definition of culture: An application-oriented overhaul. Intercult. J. 2009, 8, 35–58. [Google Scholar]
- International Organization for Migration. Who Is a Migrant? Available online: https://www.iom.int/node/102743 (accessed on 10 November 2021).
- Keupp, H. Identitätskonstruktionen: Das Patchwork der Identitäten in der Spätmoderne; Rowohlt-Taschenbuch-Verl.: Reinbek, Germany, 2008; ISBN 978-3-499-55634-0. [Google Scholar]
- Vertovec, S. Towards post-multiculturalism? Changing communities, conditions and contexts of diversity. Int. Soc. Sci. J. 2018, 68, 167–178. [Google Scholar] [CrossRef] [Green Version]
- Vertovec, S. Super-diversity and its implications. Ethn. Racial Stud. 2007, 30, 1024–1054. [Google Scholar] [CrossRef]
- Kunz, T. Von Interkultureller Kompetenz zu Vielfaltskompetenz? Zur Bedeutung von Interkultureller Kompetenz und möglicher Entwicklungsperspektiven. In Handbuch Diversity Kompetenz: Band 2: Gegenstandsbereiche; Genkova, P., Ringeisen, T., Eds.; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2016; pp. 13–31. ISBN 978-3-658-08853-8. [Google Scholar]
- Deardorff, D.K. Intercultural competence: Mapping the future research agenda. Int. J. Intercult. Relat. 2015, 48, 3–5. [Google Scholar] [CrossRef]
- Peng, R.-Z.; Zhu, C.; Wu, W.-P. Visualizing the knowledge domain of intercultural competence research: A bibliometric analysis. Int. J. Intercult. Relat. 2020, 74, 58–68. [Google Scholar] [CrossRef]
- Leung, K.; Ang, S.; Tan, M.L. Intercultural Competence. Annu. Rev. Organ. Psychol. Organ. Behav. 2014, 1, 489–519. [Google Scholar] [CrossRef] [Green Version]
- Betancourt, J.R.; Green, A.R.; Carrillo, J.E.; Ananeh-Firempong, O. Defining cultural competence: A practical framework for addressing racial/ethnic disparities in health and health care. Public Health Rep. 2003, 118, 293–302. [Google Scholar] [CrossRef]
- Campinha-Bacote, J. The Process of Cultural Competence in the Delivery of Healthcare Services: A model of care. J. Transcult. Nurs. 2002, 13, 181–184; discussion 200–201. [Google Scholar] [CrossRef]
- Henderson, S.; Kendall, E.; See, L. The effectiveness of culturally appropriate interventions to manage or prevent chronic disease in culturally and linguistically diverse communities: A systematic literature review. Health Soc. Care Community 2011, 19, 225–249. [Google Scholar] [CrossRef]
- Deardorff, D.K. Intercultural competence: An emerging focus in international higher education. In The SAGE Handbook of International Higher Education; Deardorff, D.K., Ed.; Sage: Los Angeles, CA, USA, 2012; pp. 283–304. ISBN 978-1-4129-9921-2. [Google Scholar]
- Fantini, A. Assessing intercultural competence: Issues and Tools. In The Sage Handbook of Intercultural Competence; Deardorff, D.K., Ed.; Sage: Thousand Oaks, CA, USA, 2009; pp. 456–476. ISBN 1412960452. [Google Scholar]
- Auernheimer, G. (Ed.) Interkulturelle Kompetenz und Pädagogische Professionalität, 4th ed.; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2013; ISBN 9783531199306. [Google Scholar]
- Danso, R. Cultural competence and cultural humility: A critical reflection on key cultural diversity concepts. J. Soc. Work 2018, 18, 410–430. [Google Scholar] [CrossRef]
- Dreachslin, J.L.; Gilbert, M.J.; Malone, B. Diversity and Cultural Competence in Health Care: A Systems Approach; Emerald Group Publishing Limited: Bradford, UK, 2013. [Google Scholar]
- Fleckman, J.M.; Dal Corso, M.; Ramirez, S.; Begalieva, M.; Johnson, C.C. Intercultural Competency in Public Health: A Call for Action to Incorporate Training into Public Health Education. Front. Public Health 2015, 3, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjarnason, D.; Mick, J.; Thompson, J.A.; Cloyd, E. Perspectives on transcultural care. Nurs. Clin. N. Am. 2009, 44, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Leininger, M.M. (Ed.) Culture Care Diversity and Universality: A Theory of Nursing; National League for Nursing Press: New York, NY, USA, 1991; ISBN 0887375197. [Google Scholar]
- Schim, S.M.; Doorenbos, A.Z. A three-dimensional model of cultural congruence: Framework for intervention. J. Soc. Work End Life Palliat. Care 2010, 6, 256–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharifi, N.; Adib-Hajbaghery, M.; Najafi, M. Cultural competence in nursing: A concept analysis. Int. J. Nurs. Stud. 2019, 99, 103386. [Google Scholar] [CrossRef]
- Curtis, E.; Jones, R.; Tipene-Leach, D.; Walker, C.; Loring, B.; Paine, S.-J.; Reid, P. Why cultural safety rather than cultural competency is required to achieve health equity: A literature review and recommended definition. Int. J. Equity Health 2019, 18, 174. [Google Scholar] [CrossRef]
- Tervalon, M.; Murray-García, J. Cultural humility versus cultural competence: A critical distinction in defining physician training outcomes in multicultural education. J. Health Care Poor Underserved 1998, 9, 117–125. [Google Scholar] [CrossRef]
- Handschuck, S.; Schröer, H. Interkulturelle Orientierung und Öffnung: Theoretische Grundlagen und 50 Aktivitäten zur Umsetzung, 1. Aufl.; ZIEL: Augsburg, Germany, 2012; ISBN 9783940562708. [Google Scholar]
- Rathje, S. Intercultural Competence: The Status and Future of a Controversial Concept. Lang. Intercult. Commun. 2007, 7, 254–266. [Google Scholar] [CrossRef] [Green Version]
- Vertovec, S. ‘Diversity’ and the Social Imaginary. Eur. J. Sociol. 2012, 53, 287–312. [Google Scholar] [CrossRef] [Green Version]
- Bolten, J. “Diversität” aus der Perspektive eines offenen Interkulturalitätsbegriffs. In Interkulturalität und Kulturelle Diversität; Moosmüller, A., Möller-Kiero, J., Eds.; Waxmann: Münster, NY, USA, 2014; pp. 47–60. ISBN 978-3-8309-2998-7. [Google Scholar]
- Zhang, X.; Zhou, M. Interventions to promote learners’ intercultural competence: A meta-analysis. Int. J. Intercult. Relat. 2019, 71, 31–47. [Google Scholar] [CrossRef]
- O’Brien Pott, M.; Blanshan, A.S.; Huneke, K.M.; Baasch Thomas, B.L.; Cook, D.A. Barriers to identifying and obtaining CME: A national survey of physicians, nurse practitioners and physician assistants. BMC Med. Educ. 2021, 21, 168. [Google Scholar] [CrossRef]
- Keeney, S.; McKenna, H.; Hasson, F. The Delphi Technique in Nursing and Health Research; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2011; ISBN 9781405187541. [Google Scholar]
- Gertsen, M.C. Intercultural competence and expatriates. Int. J. Hum. Resour. Manag. 1990, 1, 341–362. [Google Scholar] [CrossRef]
- Bolten, J. Was heißt “Interkulturelle Kompetenz?”: Perspektiven für die internationale Personalentwicklung. In Wirtschaft Als Interkulturelle Herausforderung: Business across Cultures; Künzer, V., Berninghausen, J., Eds.; IKO-Verl. für Interkulturelle Kommunikation: Frankfurt am Main, Germany, 2007; pp. 21–42. ISBN 3-88939-849-9. [Google Scholar]
- Müller, S.; Gelbrich, K. Interkulturelles Marketing, 2nd ed.; Franz Vahlen: Berlin, Germany, 2015; ISBN 9783800644612. [Google Scholar]
- Alizadeh, S.; Chavan, M. Cultural competence dimensions and outcomes: A systematic review of the literature. Health Soc. Care Community 2016, 24, e117–e130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, A.; Benson, P. Anthropology in the clinic: The problem of cultural competency and how to fix it. PLoS Med. 2006, 3, e294. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Cultural Formulation Interview (CFI). Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwi10c2tkaf2AhWRS_EDHaWwBbQQFnoECDoQAQ&url=https%3A%2F%2Fwww.psychiatry.org%2FFile%2520Library%2FPsychiatrists%2FPractice%2FDSM%2FAPA_DSM5_Cultural-Formulation-Interview.pdf&usg=AOvVaw0yl4EMDbxmpSbT2uVcJfOL (accessed on 2 March 2022).
- Schröer, H. Interkulturelle Öffnung und Diversity Management: Konturen einer neuen Diversitätspolitik der Sozialen Arbeit. In Soziale Arbeit in der Migrationsgesellschaft: Grundlagen-Konzepte-Handlungsfelder; Blank, B., Gögercin, S., Sauer, K.E., Schramkowski, B., Eds.; Springer VS: Wiesbaden, Germany, 2018; pp. 773–785. ISBN 3658195398. [Google Scholar]
- Auernheimer, G. Diversity und interkulturelle Kompetenz. In Arbeitsfeld Interkulturalität: Grundlagen, Methoden und Praxisansätze der Sozialen Arbeit in der Zuwanderungsgesellschaft; Kunz, T., Puhl, R., Eds.; Juventa-Verl.: Weinheim, Basel, 2011; pp. 167–181. ISBN 9783779922087. [Google Scholar]
- Leenen, W.R.; Groß, A.; Grosch, H. Interkulturelle Kompetenz in der Sozialen Arbeit. In Interkulturelle Kompetenz und Pädagogische Professionalität, 4th ed.; Auernheimer, G., Ed.; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2013; pp. 105–126. ISBN 9783531199306. [Google Scholar]
- Henderson, S.; Horne, M.; Hills, R.; Kendall, E. Cultural competence in healthcare in the community: A concept analysis. Health Soc. Care Community 2018, 26, 590–603. [Google Scholar] [CrossRef]
- Brottman, M.R.; Char, D.M.; Hattori, R.A.; Heeb, R.; Taff, S.D. Toward Cultural Competency in Health Care: A Scoping Review of the Diversity and Inclusion Education Literature. Acad. Med. 2020, 95, 803–813. [Google Scholar] [CrossRef]
- Hordijk, R.; Hendrickx, K.; Lanting, K.; MacFarlane, A.; Muntinga, M.; Suurmond, J. Defining a framework for medical teachers’ competencies to teach ethnic and cultural diversity: Results of a European Delphi study. Med. Teach. 2019, 41, 68–74. [Google Scholar] [CrossRef]
- Stone, J.R. Healthcare inequality, cross-cultural training, and bioethics: Principles and applications. Camb. Q. Healthc. Ethics 2008, 17, 216–226. [Google Scholar] [CrossRef]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics, 7th ed.; Oxford Univ. Press: New York, NY, USA, 2013; ISBN 978-0-19-992458-5. [Google Scholar]
- World Medical Association. Declaration of Geneva: Adopted by the 2nd General Assembly of the World Medical Association, Geneva, Switzerland, September 1948; and amended by the 22nd World Medical Assembly, Sydney, Australia, August 1968; and the 35th World Medical Assembly, Venice, Italy, October 1983 and the 46th WMA General Assembly, Stockholm, Sweden, September 1994: And editorially revised by the 170th WMA Council Session, Divonne-les-Bains, France, May 2005; and the 173rd WMA Council Session, Divonne-les-Bains, France, May 2006; and amended by the 68th WMA General Assembly, Chicago, United States, October 2017. Available online: https://www.wma.net/policies-post/wma-declaration-of-geneva/ (accessed on 10 December 2021).
- Newham, R.; Hewison, A.; Graves, J.; Boyal, A. Human rights education in patient care: A literature review and critical discussion. Nurs. Ethics 2021, 28, 190–209. [Google Scholar] [CrossRef]
- Erdman, J.N. Human rights education in patient care. Public Health Rev. 2017, 38, 14. [Google Scholar] [CrossRef]
- McKenzie, K.C.; Mishori, R.; Ferdowsian, H. Twelve tips for incorporating the study of human rights into medical education. Med. Teach. 2020, 42, 871–879. [Google Scholar] [CrossRef] [PubMed]
- Physicians for Human Rights. Through Evidence, Change is Possible. Physicians for Human Rights. Available online: https://phr.org/ (accessed on 19 November 2021).
- IFHHRO. Medical Human Rights Network. Available online: https://www.ifhhro.org/ (accessed on 27 August 2021).
- Pacquiao, D.F. Nursing care of vulnerable populations using a framework of cultural competence, social justice and human rights. Contemp. Nurse 2008, 28, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Czollek, L.C.; Perko, G.; Weinbach, H. Social justice und diversity training. Arch. FÜR Wiss. Und Prax. Der Soz. Arb. 2012, 43, 31–40. [Google Scholar] [CrossRef]
- Czollek, L.C.; Perko, G.; Czollek, M.; Kaszner, C. Praxishandbuch Social Justice und Diversity: Theorien, Training, Methoden, Übungen, 2nd ed.; Juventa Verlag ein Imprint der Julius Beltz: Weinheim, Basel, 2019; ISBN 3779938456. [Google Scholar]
- Jirwe, M.; Gerrish, K.; Keeney, S.; Emami, A. Identifying the core components of cultural competence: Findings from a Delphi study. J. Clin. Nurs. 2009, 18, 2622–2634. [Google Scholar] [CrossRef] [Green Version]
- Shepherd, S.M.; Willis-Esqueda, C.; Newton, D.; Sivasubramaniam, D.; Paradies, Y. The challenge of cultural competence in the workplace: Perspectives of healthcare providers. BMC Health Serv. Res. 2019, 19, 135. [Google Scholar] [CrossRef] [Green Version]
- Kitson, A.; Marshall, A.; Bassett, K.; Zeitz, K. What are the core elements of patient-centred care? A narrative review and synthesis of the literature from health policy, medicine and nursing. J. Adv. Nurs. 2013, 69, 4–15. [Google Scholar] [CrossRef]
- Mead, N.; Bower, P. Patient-centredness: A conceptual framework and review of the empirical literature. Soc. Sci. Med. An. Int. J. 2000, 51, 1087–1110. [Google Scholar] [CrossRef]
- Kalpaka, A.; Mecheril, P. “Interkulturell”: Von spezifisch kulturalistischen Ansätzen zu allgemein reflexiven Perspektiven. In Migrationspädagogik; Mecheril, P., Castro Varela, M.d.M., Dirim, İ., Kalpaka, A., Melter, C., Eds.; Beltz Verlag: Weinheim, Basel, 2010; pp. 77–98. ISBN 9783407342058. [Google Scholar]
- Zanting, A.; Meershoek, A.; Frambach, J.M.; Krumeich, A. The ‘exotic other’ in medical curricula: Rethinking cultural diversity in course manuals. Med. Teach. 2020, 42, 791–798. [Google Scholar] [CrossRef] [Green Version]
- Phillips, A. What’s wrong with Essentialism? Distinktion J. Soc. Theory 2010, 11, 47–60. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, J.I.; Medkik, N. The Effects of Diversity Awareness Training on Differential Treatment. Group Organ. Manag. 2004, 29, 517–536. [Google Scholar] [CrossRef]
- Leiba-O’sullivan, S. The Distinction between Stable and Dynamic Cross-cultural Competencies: Implications for Expatriate Trainability. J. Int. Bus. Stud. 1999, 30, 709–725. [Google Scholar] [CrossRef]
- Shirts, R.G. BAFA BAFA: A Cross-Cultural Simulation; Intercultural Press: Del Mar, CA, USA, 1977. [Google Scholar]
- Thiagarajan, S. Barnga: A Simulation Game on Cultural Clashes, 25th ed.; revised and enhanced, [repr.]; Intercultural Press: Boston, MA, USA, 2009; ISBN 9781931930307. [Google Scholar]
- Gudykunst, W.B.; Guzley, R.M.; Hammer, M.R. Designing Intercultural Training. In Handbook of Intercultural Training: Issues in Theory and Design; Landis, D., Brislin, R.W., Eds.; Elsevier Science: Burlington, NJ, USA, 1996; pp. 61–80. ISBN 9780080275338. [Google Scholar]
- Lim, M.Y.; Kriegel, M.; Aylett, R.; Enz, S.; Vannini, N.; Hall, L.; Rizzo, P.; Leichtenstern, K. Technology-Enhanced Role-Play for Intercultural Learning Contexts. In Entertainment Computing–ICEC 2009; Natkin, S., Dupire, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; pp. 73–84. ISBN 978-3-642-04052-8. [Google Scholar]
- Bhawuk, D.; Brislin, R. Cross-cultural Training: A Review. Appl. Psychol. 2000, 49, 162–191. [Google Scholar] [CrossRef]
- Zembylas, M. Engaging With Issues of Cultural Diversity and Discrimination Through Critical Emotional Reflexivity in Online Learning. Adult Educ. Q. 2008, 59, 61–82. [Google Scholar] [CrossRef]
- Novy, I. Interkulturelle Kompetenz–zu viel Theorie? Erwägen Wissen Ethik 2003, 14, 206–207. [Google Scholar]
- Linck, G. Auf Katzenpfoten Gehen und das qi Miteinander Tauschen-Überlegungen Einer China-Wissenschaftlerin Zur Transkulturellen Kommunikation und Kompetenz. Erwägen Wissen Ethik 2003, 14, 189–192. [Google Scholar] [CrossRef] [Green Version]
- Brach, C.; Fraser, I. Can cultural competency reduce racial and ethnic health disparities? A review and conceptual model. Med. Care Res. Rev. 2000, 57 (Suppl. S1), 181–217. [Google Scholar] [CrossRef] [PubMed]
- Pinder, R.J.; Ferguson, J.; Møller, H. Minority ethnicity patient satisfaction and experience: Results of the National Cancer Patient Experience Survey in England. BMJ Open 2016, 6, e011938. [Google Scholar] [CrossRef] [Green Version]
- Kambale Mastaki, J. Migrant patients’ satisfaction with health care services: A comprehensive review. Ital. J. Public Health 2012, 7. [Google Scholar] [CrossRef]
- Suphanchaimat, R.; Kantamaturapoj, K.; Putthasri, W.; Prakongsai, P. Challenges in the provision of healthcare services for migrants: A systematic review through providers’ lens. BMC Health Serv. Res. 2015, 15, 390. [Google Scholar] [CrossRef] [Green Version]
- Robertshaw, L.; Dhesi, S.; Jones, L.L. Challenges and facilitators for health professionals providing primary healthcare for refugees and asylum seekers in high-income countries: A systematic review and thematic synthesis of qualitative research. BMJ Open 2017, 7, e015981. [Google Scholar] [CrossRef] [Green Version]
- Brandenberger, J.; Tylleskär, T.; Sontag, K.; Peterhans, B.; Ritz, N. A systematic literature review of reported challenges in health care delivery to migrants and refugees in high-income countries-the 3C model. BMC Public Health 2019, 19, 755. [Google Scholar] [CrossRef] [PubMed]
- Fortin, S.; Maynard, S. Diversity, Conflict, and Recognition in Hospital Medical Practice. Cult. Med. Psychiatry 2018, 42, 32–48. [Google Scholar] [CrossRef] [PubMed]
- Mecheril, P. Natio-kulturelle Mitgliedschaft-ein Begriff und die Methode seiner Generierung. Tertium Comp. 2002, 8, 104–115. [Google Scholar]
- Bolten, J. Fuzzy Cultures: Konsequenzen eines offenen und mehrwertigen Kulturbegriffs für Konzeptualisierungen interkultureller Personalentwicklungsmaßnahmen. Mondial. Sietar J. FÜR Interkult. Perspekt. 2013, 19, 4–10. [Google Scholar]
- Welsch, W. Transkulturalität: Realität und Aufgabe. In Migration, Diversität und Kulturelle Identitäten: Sozial-und Kulturwissenschaftliche Perspektiven; Giessen, H.W., Rink, C., Eds.; J.B. Metzler: Stuttgart, Germany, 2020; pp. 3–18. ISBN 978-3-476-04372-6. [Google Scholar]
- Hoffman, E.; Verdooren, A. Diversity Competence: Cultures Don’t Meet, People Do; CABI: Oxfordshire, UK; Boston, MA, USA, 2019; ISBN 9781789242409. [Google Scholar]
- Herrmann, E.; Kätker, S. Diversity Management: Organisationale Vielfalt im Pflege-und Gesundheitsbereich Erkennen und Nutzen, 1. Aufl.; Huber: Bern, Switzerland, 2007; ISBN 3-456-84419-0. [Google Scholar]
- Van Keuk, E.; Giesler, W. Diversity Training im Gesundheits-und Sozialwesen am Beispiel des EQUAL Projektes. In Interkulturelle Kompetenz im Wandel: Ausbildung, Training und Beratung; Otten, M., Scheitza, A., Cnyrim, A., Eds.; IKO: Frankfurt, Germany, 2007; pp. 147–173. ISBN 9783889399007. [Google Scholar]
- WHO Commission on Social Determinants of Health. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2008; ISBN 9789241563703. [Google Scholar]
- Auernheimer, G. Einführung in die Interkulturelle Pädagogik, 7th ed.; WBG (Wiss. Buchges.): Darmstadt, Germany, 2012; ISBN 978-3-534-25721-8. [Google Scholar]
- Adams, M.; Bell, L.A.; Griffin, P. Teaching for Diversity and Social Justice, 3rd ed.; Routledge: New York, NY, USA, 2016; ISBN 9781138023345. [Google Scholar]
- Kumagai, A.K.; Lypson, M.L. Beyond cultural competence: Critical consciousness, social justice, and multicultural education. Acad. Med. 2009, 84, 782–787. [Google Scholar] [CrossRef]
- Neff, J. The Structural Competency Working Group: Lessons from Iterative, Interdisciplinary Development of a Structural Competency Training Module. In Structural Competency in Mental Health and Medicine: A Case-Based Approach to Treating the Social Determinants of Health; Hansen, H., Metzl, J.M., Eds.; Springer Nature: Cham, Switzerland, 2019; pp. 53–74. ISBN 9783030105242. [Google Scholar]
- Metzl, J.M.; Hansen, H. Structural competency: Theorizing a new medical engagement with stigma and inequality. Soc. Sci. Med. 2014, 103, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Hansen, H.; Metzl, J.M. (Eds.) Structural Competency in Mental Health and Medicine: A Case-Based Approach to Treating the Social Determinants of Health; Springer Nature: Cham, Switzerland, 2019; ISBN 9783030105242. [Google Scholar]
- Riegel, C. Diversity-Kompetenz? Intersektionale Perspektiven der Reflexion, Kritik und Veränderung. In Kompetenz, Performanz, soziale Teilhabe: Sozialpädagogische Perspektiven auf ein Bildungstheoretisches Konstrukt; Faas, S., Bauer, P., Treptow, R., Eds.; Springer: Wiesbaden, Germany, 2014; pp. 183–195. ISBN 978-3-531-19854-5. [Google Scholar]
- Farmer, P.E.; Nizeye, B.; Stulac, S.; Keshavjee, S. Structural violence and clinical medicine. PLoS Med. 2006, 3, e449. [Google Scholar] [CrossRef] [Green Version]
- United Nations Economic and Social Council. The Right to the Highest Attainable Standard of Health, November 8, 2000. E/C.12/2000/4 General Comment of the UN Economic and Social Council. Available online: https://www.refworld.org/pdfid/4538838d0.pdf (accessed on 30 July 2004).


| N | % | Missing Data | |
|---|---|---|---|
| Age | 3 | ||
| 25–34 years | 1 | 4 | |
| 35–44 years | 7 | 25 | |
| 45–54 years | 13 | 46 | |
| 55–64 years | 4 | 14 | |
| 65–74 years | 3 | 11 | |
| Sex | 3 | ||
| Male | 12 | 39 | |
| Female | 19 | 61 | |
| Country of residency | 5 | ||
| Austria | 1 | 3 | |
| Bulgaria | 1 | 3 | |
| Denmark | 4 | 13 | |
| France | 2 | 6 | |
| Germany | 5 | 16 | |
| Greece | 1 | 3 | |
| Italy | 1 | 3 | |
| The Netherlands | 3 | 10 | |
| Norway | 1 | 3 | |
| Spain | 3 | 10 | |
| Sweden | 5 | 16 | |
| Switzerland | 3 | 10 | |
| United Kingdom | 1 | 3 | |
| Academic Degree | |||
| MSc, MA, MD | 15 | 48 | |
| Ph.D. and Dr. | 14 | 45 | |
| Other | 1 | 3 | |
| Discipline (multiple possible) | |||
| Medicine and public health | 17 | 55 | |
| Nursing and nursing sciences | 3 | 10 | |
| Psychology | 2 | 6 | |
| Social and cultural sciences | 10 | 32 | |
| Current job position (multiple possible) | |||
| Administrator | 2 | 6 | |
| Teacher | 8 | 26 | |
| Nurse | 2 | 6 | |
| Medical doctor | 8 | 26 | |
| Research/academic expert | 23 | 74 | |
| Diversity trainer | 4 | 13 | |
| Other (specified in attachment) | 6 | 19 | |
| Years of experience in this position | 2 | ||
| min. = 2; max. = 36 average = 14.6 years | |||
| (Past or present) involvement in the medical care of migrant and ethnic minority patients? | |||
| Yes | 18 | 58 | |
| No | 13 | 42 | |
| Number of publications published on diversity and/or transcultural competence topics | |||
| None | 4 | 13 | |
| 1–5 | 9 | 29 | |
| 6–10 | 4 | 13 | |
| More than 10 | 14 | 45 | |
| Involvement in training or teaching activities regarding diversity sensitivity for (health) professionals | |||
| Yes | 25 | 81 | |
| No | 6 | 19 | |
| Responsibilities (multiple possible) | 6 | ||
| Course development | 23 | 92 | |
| Course implementation/teaching | 25 | 100 | |
| Advisory role | 13 | 52 | |
| Mean | SD | ||
|---|---|---|---|
| 1 | Respectfulness | 2.96 | 0.522 |
| 2 | Ability to communicate understandably (for this patient) | 2.93 | 0.258 |
| 2 | Ability to find out what this individual patient needs | 2.93 | 0.621 |
| 2 | Ability to address the individual needs of the patient | 2.93 | 0.258 |
| 3 | Self-reflection skills of own biases | 2.90 | 0.305 |
| 3 | Non-discrimination | 2.90 | 0.402 |
| 4 | Working with interpreters properly | 2.89 | 0.309 |
| 4 | Finding solutions together with the patient | 2.89 | 0.309 |
| 5 | Ability to listen | 2.81 | 0.393 |
| 6 | Being empathetic towards each patient | 2.79 | 0.410 |
| 6 | Avoiding generalisation | 2.79 | 0.483 |
| 6 | Open-mindedness | 2.79 | 0.550 |
| Competence | M | SD | Mode | Consensus |
|---|---|---|---|---|
| Respectfulness | 2.96 | 0.522 | 3 | 100.0 |
| Self-reflection skills of own biases | 2.90 | 0.305 | 3 | 100.0 |
| Diversity awareness | 2.76 | 0.532 | 3 | 100.0 |
| Non-discrimination | 2.90 | 0.402 | 3 | 96.6 |
| Avoiding generalisation | 2.79 | 0.483 | 3 | 96.6 |
| Ability to change the perspective (get to know and emphasise with the position of the ‘other’) | 2.76 | 0.502 | 3 | 96.6 |
| Being non-judgemental | 2.76 | 0.502 | 3 | 96.6 |
| Cross-/cultural awareness | 2.69 | 0.532 | 3 | 96.6 |
| Open-mindedness | 2.79 | 0.550 | 3 | 93.1 |
| Self-reflection skills of own (power) position in the medical encounter | 2.72 | 0.581 | 3 | 93.1 |
| Avoiding prejudice | 2.66 | 0.603 | 3 | 93.1 |
| Self-reflection skills of own sociocultural background | 2.59 | 0.628 | 3 | 93.1 |
| Self-reflection skills of own cultural habits of thought, evaluation and practice | 2.59 | 0.617 | 3 | 93.1 |
| Humility | 2.48 | 0.623 | 3 | 93.1 |
| Curiosity | 2.45 | 0.621 | 3 | 93.1 |
| Self-reflection skills of own behaviour | 2.45 | 0.621 | 3 | 93.1 |
| Readiness to work with uncertainty | 2.54 | 0.626 | 3 | 92.9 |
| Self-reflection skills of own context | 2.45 | 0.674 | 3 | 89.7 |
| Self-reflection skills of own feelings | 2.21 | 0.663 | 2 | 86.2 |
| Self-reflection skills of own cultural health beliefs | 2.41 | 0.720 | 3 | 86.2 |
| Patience | 2.32 | 0.710 | 3 | 85.7 |
| Politeness | 2.07 | 0.640 | 2 | 82.8 |
| Compassion | 2.14 | 0.742 | 2 | 78.6 |
| Readiness to be courageous | 2.03 | 0.809 | nm * | 69.0 |
| Competence | M | SD | Mode | Consensus |
|---|---|---|---|---|
| Knowledge about social determinants of health | 2.72 | 0.447 | 3 | 100.0 |
| Ethical and human rights competence | 2.46 | 0.566 | 3 | 96.4 |
| Knowledge of migrant-health differences such as psychosocial stressors in exile | 2.62 | 0.611 | 3 | 93.1 |
| Knowledge of migrant-health differences such as the influence of social exclusion and discrimination | 2.66 | 0.603 | 3 | 93.1 |
| Knowledge of migrant-health differences such as influence of (forced) migration | 2.55 | 0.621 | 3 | 93.1 |
| Knowledge about the influence of policies on own field of activity | 2.34 | 0.603 | 2 | 93.1 |
| Knowledge about the legal context in the country in which you are working as a health professional | 2.38 | 0.715 | 3 | 86.2 |
| Knowledge about the asylum process in the country in which you are working as a health professional | 2.31 | 0.700 | 3 | 86.2 |
| Knowledge of migrant-health differences such as special diseases | 2.21 | 0.663 | 2 | 86.2 |
| Knowledge of migrant-health differences such as differences in effective treatment | 2.34 | 0.708 | 3 | 86.2 |
| Knowledge about the network of local actors | 2.34 | 0.708 | 3 | 86.2 |
| Knowledge about clinically applied ethnography * | 2.31 | 0.748 | 3 | 82.8 |
| Knowledge about different belief-systems/world views/cosmovisions | 2.24 | 0.727 | nm | 82.8 |
| Knowledge of migrant-health differences such as differences in morbidity | 2.14 | 0.681 | 2 | 82.8 |
| Knowledge about different religions | 1.79 | 0.609 | 2 | 69.0 |
| Being able to circumscribe own field of professional activity from the influence of the political sphere (quote: ‘evidence-based more than policy-based medicine’ AETR1) | 2.04 | 0.838 | 3 | 66.7 |
| Knowledge on critical theoretical approaches to ‘culture’ | 2.00 | 0.871 | nm | 62.1 |
| Knowledge about different cultures | 1.66 | 0.603 | 2 | 58.6 |
| Knowledge about anthropology (how social and cultural habits are studied scientifically) | 1.71 | 0.795 | 1 | 50.0 |
| Competence | M | SD | Mode | Consensus |
|---|---|---|---|---|
| Communicate understandably (explain and provide information in a way that this patient can understand) | 2.93 | 0.258 | 3 | 100.0 |
| Finding out what this individual patient needs | 2.93 | 0.621 | 3 | 100.0 |
| Addressing the individual needs of the patient | 2.93 | 0.258 | 3 | 100.0 |
| Working with interpreters properly | 2.89 | 0.309 | 3 | 100.0 |
| Finding solutions together with the patient | 2.89 | 0.309 | 3 | 100.0 |
| Ability to listen | 2.81 | 0.393 | 3 | 100.0 |
| Ability to be empathetic towards each patient | 2.79 | 0.410 | 3 | 100.0 |
| Knowledge of the pitfalls of ad hoc/lay interpreters | 2.75 | 0.433 | 3 | 100.0 |
| Communicate with awareness of non-verbal aspects of communication | 2.64 | 0.549 | 3 | 96.4 |
| Communicate in an open-ended enquiry | 2.59 | 0.562 | 3 | 96.3 |
| Getting to know the patient in a holistic way (understand collective and cultural ties, know about their experiences and daily lives) | 2.32 | 0.601 | 2 | 92.9 |
| Being flexible and adaptive | 2.75 | 0.575 | 3 | 92.9 |
| Identifying if patients had traumatic experiences | 2.46 | 0.680 | 3 | 89.3 |
| Actively ask about patient’s personal point of view concerning the disease (e.g., beliefs of how it came to be and how it should be treated, the meaning of the diagnosis for the patient’s life) | 2.44 | 0.697 | 3 | 88.0 |
| Providing stress- and trauma-sensitive care | 2.36 | 0.718 | 3 | 85.7 |
| Being able to address conceptual differences related to health/disease and treatment | 2.19 | 0.680 | 2 | 84.6 |
| Ability to use non-verbal signals to communicate | 2.15 | 0.755 | 2 | 77.8 |
| Ability to improvise | 2.29 | 0.839 | 3 | 75.0 |
| Language skills | 1.79 | 0.860 | 1 | 50.0 |
| Delivering spiritual care or refer to professionals in the field of spiritual care | 1.54 | 0.778 | 1 | 35.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ziegler, S.; Michaëlis, C.; Sørensen, J. Diversity Competence in Healthcare: Experts’ Views on the Most Important Skills in Caring for Migrant and Minority Patients. Societies 2022, 12, 43. https://0-doi-org.brum.beds.ac.uk/10.3390/soc12020043
Ziegler S, Michaëlis C, Sørensen J. Diversity Competence in Healthcare: Experts’ Views on the Most Important Skills in Caring for Migrant and Minority Patients. Societies. 2022; 12(2):43. https://0-doi-org.brum.beds.ac.uk/10.3390/soc12020043
Chicago/Turabian StyleZiegler, Sandra, Camilla Michaëlis, and Janne Sørensen. 2022. "Diversity Competence in Healthcare: Experts’ Views on the Most Important Skills in Caring for Migrant and Minority Patients" Societies 12, no. 2: 43. https://0-doi-org.brum.beds.ac.uk/10.3390/soc12020043