
Embedding Behavioral and Social Sciences across the Medical Curriculum: (Auto) Ethnographic Insights from Medical Schools in the United Kingdom


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
People do not go to their doctor and say: “Doctor, doctor, I’ve got health inequality”.
2. Methods
2.1. Ethnographic Study among Medical Students
2.1.1. Participant Observation among Medical Students
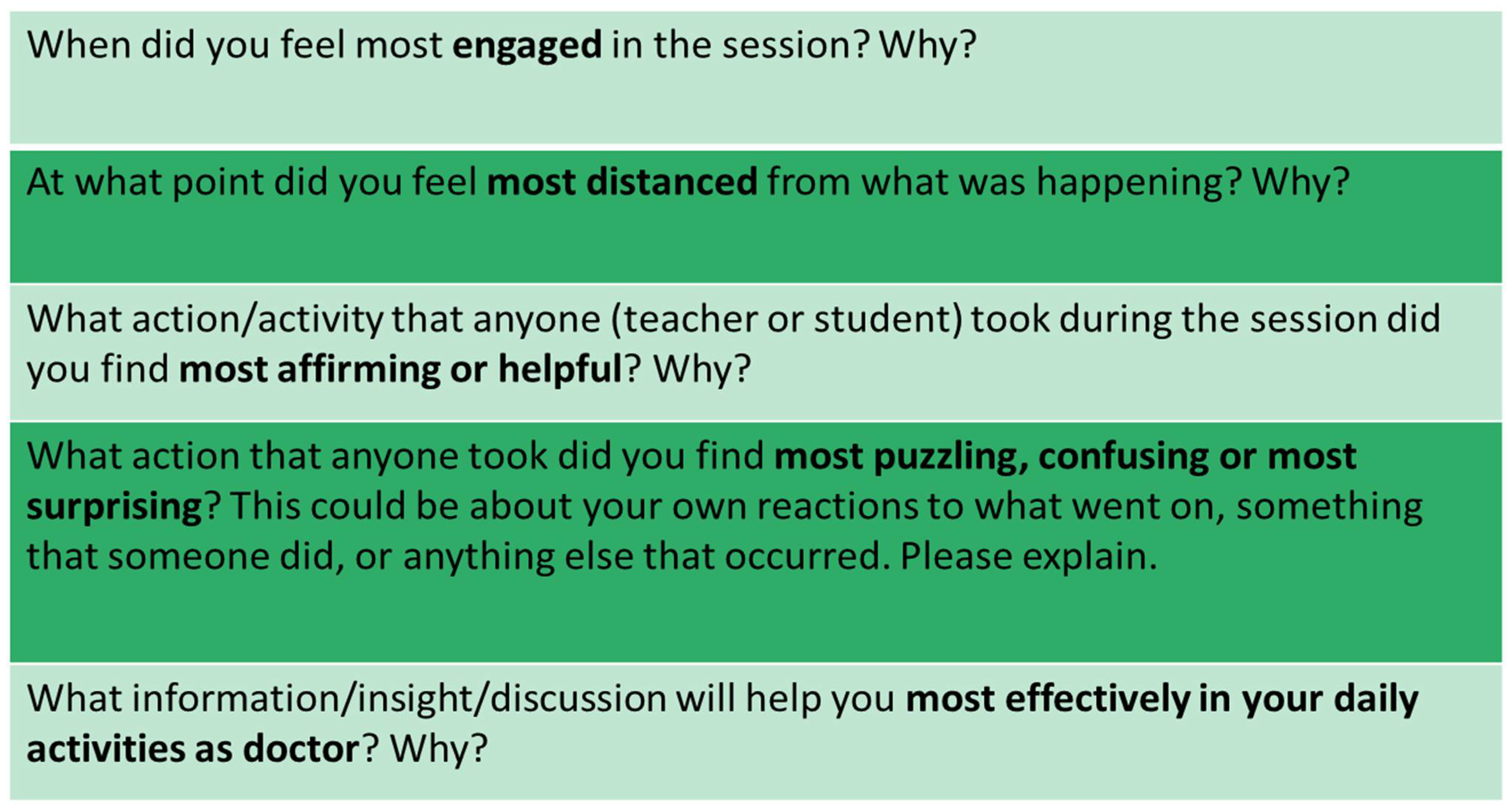
2.1.2. Critical Incident Questionnaires
2.1.3. Essays and Reflective Statements
2.1.4. Focus Group
2.1.5. Interview Study
2.2. Turning the Ethnographic Gaze on Our Educational Practice
2.3. Data Analysis
2.4. Ethical Considerations
2.5. Limitations
3. Results
- Perceptions of the behavioural and social sciences in the medical curriculum;
- Experiences of teaching, learning, and assessing BSS;
- Culture surrounding the formal and hidden curriculum in relation to BSS;
- Relevance of BSS to clinical practice.
3.1. Perceptions of Behavioural and Social Sciences in the Medical Curriculum
Because I was very good at sciences, I was top of my year and so because if you’re top of your year in sciences everyone said you had to do medicine.(Liz)
Obviously I know there would be a bit of it but the fact that there was like a whole exam on it and lectures on it and learning outcomes and everything, I didn’t realise it would be such a big part.
3.2. Experiences of Teaching, Learning and Assessing BSS
3.2.1. BSS Teaching
- From the SSC “Health Inequalities”:
Throughout the session I felt engaged in the discussions. I enjoyed exploring the underlying causes of ill health and their relation to inequality. I felt that the lecturer and all the students made interesting and thought-provoking points.
- From the SSC “Introduction to Medical Anthropology”:
Talking about structural violence in the lecture was really engaging and allowed us to draw in our personal experiences.
Medical students are often reticent during placements when supervising clinicians encourage them to engage with BSS learning, or students do it as a “tick box” exercise. When students are on a hospital ward taking a clinical history and they forget to ask about “ideas, concerns, and expectations” (they remember it as “ICE”), this is when they might roll their eyes or make a noise and say “oh and I forgot to ask about ICE”. As if it does not really matter as much, because they can still formulate the diagnosis without asking about the issues they consider “peripheral”.(From reflective note by Ghobrial)
3.2.2. Learning BSS Content
What the lungs do and what goes wrong with the lungs would be my top priority, but the impact of lung disease on the patient? That goes a bit lower down, I don’t really have to know much about this now, it seems too far in the future [that she would treat a patient with a lung problem]. I’ll do it when I’ve made sure I’ve done everything else I need to do, so it can end up being quite a quick job.
I think we’re all becoming doctors because we are actually people who want to get up and do something and when you present us with just questions and questions and problems without even, without skills to know how to solve these or even just discuss a solution, then I think we all become cynical.
3.2.3. Assessment of BSS Content
3.3. Culture of the Formal and Hidden Curriculum in Relation to BSS
If your tutor is a heart surgeon, they’re not really going to be that fussed about like talking to you about like what that patient’s going to do when they get home, like they’re more interested, in, like the anatomy of the heart.
3.4. Relevance of BSS to Clinical Practice
- From the SSC “Introduction to Medical Anthropology”:
This [anthropology content] is helpful because it makes me more aware of people’s opinions and cultures.
Anthropological research—understanding why certain cultures behave the way they do—will help me understand certain health behaviors and be better prepared to address them.
All the discussions—how to deal with other cultural beliefs (e.g., religious beliefs and beliefs in witchcraft) and the importance of using anthropology to inform policy.
Discussion regarding beliefs surrounding health, and similarities between what we see as normal (e.g., Christian religion) and abnormal (e.g., witchcraft).
- From the SSC “Health Inequalities”:
Realizing that a biomedical attitude to everything often needs a social perspective to make a difference.
4. Discussion
4.1. Embedding BSS in the Undergraduate Medical Curriculum
4.2. Implications for Medical Education
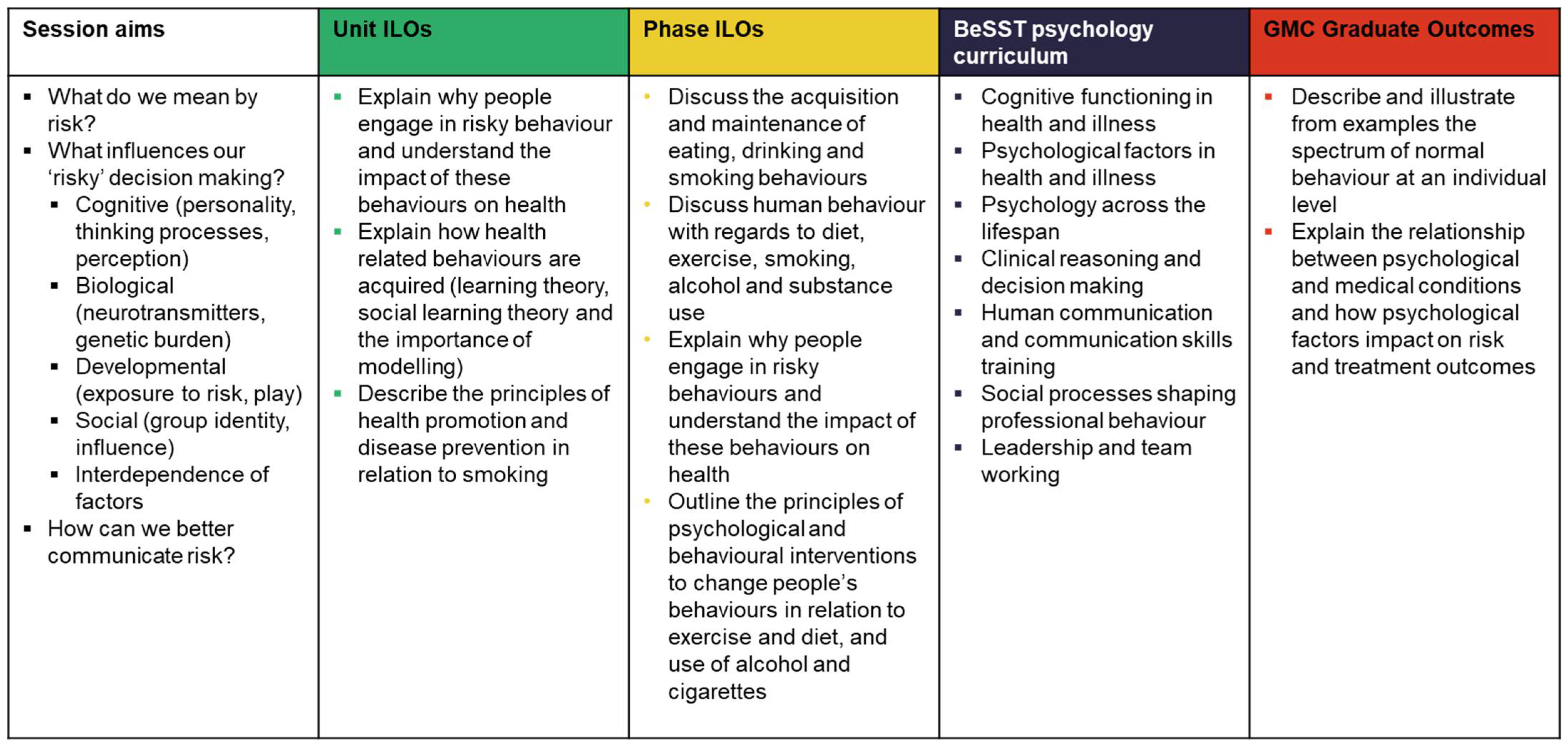
4.2.1. Curriculum Mapping: From Session Aims to Graduate Outcomes
4.2.2. Multidisciplinary Co-Teaching
4.3. Innovative Assessment of BSS Content
- (1)
- theoretically underpinned by anthropological concepts introduced in the SSC;
- (2)
- methodologically sound and used appropriate methods. They were encouraged to use examples discussed in the course;
- (3)
- impactful and able to improve the health outcomes of the population or community they proposed to study.
5. Conclusions
- It is important to ensure the visibility of the behavioural and social scientists teaching medical students, regardless of whether these BSS experts are based in medical schools or in other departments. Our experience shows that when BSS colleagues are offered the same opportunities, with regard to educational leadership roles and responsibilities, they feel valued, and they become respected members of medical educational teams;
- Educators in medical schools should be encouraged to explore opportunities for multidisciplinary team teaching. This enables the wider educational team to have a better appreciation of each discipline’s distinct contributions to medical education, and it facilitates concrete subject integration for students to model in their own learning;
- Team meetings to discuss how both positive and negative perceptions of BSS content are reinforced by each student cohort, and how BSS is incorporated into the formal curriculum that is producing a hidden curriculum with, for instance, negative institutional slang concerning BSS;
- Exploration into different examination strategies for BSS topics to ensure that the application of knowledge can be assessed more reliably.
- BSS educators should be familiar with the medical education curriculum, and they should appreciate the demands that are required of medical students, which are very different from those required of social and behavioural science students. One could, for instance, carry out a small autoethnographic project by becoming a student in one’s own medical school, attending a wide range of clinical and biomedical teaching activities in order to observe different teaching and assessment strategies. This is particularly valuable for BSS experts who are sometimes “parachuted” in from other departments in order to deliver teaching;
- We strongly encourage reflexive educational practice, bringing an ethnographic lens to one’s own medical classroom and developing communities of practice in places where these do not exist in order to facilitate discussion, reflections, and peer reviews.
- Ensure clear signposting to relevant, appropriate, and readily available academic resources that support the BSS teaching content. These should be highlighted to both staff and students, and the importance of using resources produced by BSS experts, rather than relying on quick internet searches, should be emphasized frequently;
- Course materials should be reviewed regularly to ensure BSS concepts and theories are current, in addition to being represented in a valid and coherent way, rather than being tokenistic and “shoe-horned” into “empty” curriculum slots. Any significant curriculum development should be evaluated using CIQs to assess what works well and what does not;
- Experience is often an underused resource, and many staff and students have personal and professional experiences concerning gender, race, age, behavior, or inequalities. PBL tutors should be encouraged to prompt students to share relevant experiences, offering them support when doing so, and they should discuss how their BSS knowledge can be applied in order to consolidate learning. After all, we want medical students to become reflective practitioners.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Association of American Medical Colleges (AAMC). Cultural Competence Education for Medical Students; American Association of Medical Colleges: Washington, DC, USA, 2005; Available online: https://www.aamc.org/media/20856/download (accessed on 30 December 2021).
- Tervalon, M.; Murray-Garcia, J. Cultural humility versus cultural competence: A critical distinction in defining physician training outcomes in multicultural education. J. Health Care Poor Underserved 1998, 9, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Donald, C.A.; DasGupta, S.; Metzl, J.M.; Eckstrand, K.L. Queer frontiers in medicine: A structural competency approach. Acad. Med. 2017, 92, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Castillo, E.G.; Isom, J.; DeBonis, K.L.; Jordan, A.; Braslow, J.T.; Rohrbaugh, R. Reconsidering systems-based practice: Advancing structural competency, health equity, and social responsibility in graduate medical education. Acad. Med. 2020, 95, 1817–1822. [Google Scholar] [CrossRef] [PubMed]
- Hayman, K.; Wen, M.; Khan, F.; Mann, T.; Pinto, A.D.; Ng, S.L. What knowledge is needed? Teaching undergraduate medical students to “go upstream” and advocate on social determinants of health. Can. Med. Educ. J. 2020, 11, e57–e61. [Google Scholar] [CrossRef]
- Woolsey, C.; Narruhn, R. Structural competency: A pilot study. Public Health Nurs. 2020, 37, 602–613. [Google Scholar] [CrossRef]
- Neff, J.; Holmes, S.M.; Knight, K.R.; Strong, S.; Thompson-Lastad, A.; McGuinness, C.; Duncan, L.; Saxena, N.; Harvey, M.J.; Langford, A.; et al. Structural competency: Curriculum for medical students, residents, and interprofessional teams on the structural factors that produce health disparities. MedEdPORTAL 2020, 16, 10888. [Google Scholar] [CrossRef]
- Metzl, J.M. Structural competency. Am. Q. 2012, 64, 213–218. [Google Scholar] [CrossRef]
- Metzl, J.M.; Hansen, H. Structural competency: Theorizing a new medical engagement with stigma and inequality. Soc. Sci. Med. 2014, 103, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Cai, D.Y. A concept analysis of cultural competence. Int. J. Nurs. Sci. 2016, 3, 268–273. [Google Scholar] [CrossRef] [Green Version]
- Mews, C.; Schuster, S.; Vajda, C.; Lindtner-Rudolph, H.; Schmidt, L.; Bösner, S.; Güzelsoy, L.; Kressing, F.; Hallal, H.; Peters, T.; et al. Cultural competence and global health: Perspectives for medical education—position paper of the GMA Committee on Cultural Competence and Global Health. GMS J. Med. Educ. 2018, 35, Doc28. [Google Scholar]
- Kleinman, A.; Benson, P. Anthropology in the clinic: The problem of cultural competency and how to fix it. PLoS Med. 2006, 3, 1673–1676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, A.J.; van Teijlingen, E.; Lambert, H.; Stacy, R. Social and Behavioural Sciences in Medical Education. Report on a Workshop Held on 27–28 June 2002; Department of Anthropology, University of Durham: Durham, UK, 2002. [Google Scholar]
- General Medical Council (GMC). 1993, 2003, 2009. Tomorrow’s Doctors. Recommendations on Undergraduate Medical Education. Available online: https://www.educacionmedica.net/pdf/documentos/modelos/tomorrowdoc.pdf (accessed on 30 December 2021).
- General Medical Council (GMC). Outcomes for Graduates. 2018. Available online: https://www.gmc-uk.org/education/standards-guidance-and-curricula/standards-and-outcomes/outcomes-for-graduates (accessed on 28 December 2021).
- Dikomitis, L.; Kelly, E. Enquiry into Learning and Teaching in the Social Sciences: Engaging with Ethnographic Research. In Teaching and Learning in Higher Education: Disciplinary Approaches to Educational Enquiry; Cleaver, E., Lintern, M., McLinden, M., Eds.; Sage: London, UK, 2018; pp. 253–265. [Google Scholar]
- De Visser, R. Psychology in medical curricula: “Need to know’ or “nice to know’. Eur. Health Psychol. 2009, 11, 20–23. [Google Scholar]
- Forrest, S. Teaching social science research methods to undergraduate medical students: The state of the art and opportunities for practice and curriculum development. Teach. Public Adm. 2017, 35, 280–300. [Google Scholar] [CrossRef] [Green Version]
- Russell, A.; Van Teijlingen, E.; Lambert, H.; Stacy, R. Social and behavioural science education in UK medical schools: Current practice and future directions. Med. Educ. 2004, 38, 409–417. [Google Scholar] [CrossRef]
- Benbassat, J.; Baumal, R.; Borkan, J.M.; Ber, R. Overcoming barriers to teaching the behavioral and social sciences to medical students. Acad. Med. 2003, 78, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, S.; Wallace, S.; Nathan, Y.; McGrath, D. “Soft and fluffy”: Medical students’ attitudes towards psychology in medical education. J. Health Psychol. 2015, 20, 91–101. [Google Scholar] [CrossRef] [Green Version]
- Satterfield, J.M.; Adler, S.R.; Chen, H.C.; Hauer, K.E.; Saba, G.W.; Salazar, R. Creating an ideal social and behavioural sciences curriculum for medical students. Med. Educ. 2010, 44, 194–202. [Google Scholar] [CrossRef]
- BeSST. Behavioural and Social Sciences Teaching in Medicine. 2021. Available online: https://www.besst.info (accessed on 28 December 2021).
- BeSST. A Core Curriculum for Psychology in Undergraduate Medical Education. 2010. Available online: https://www.advance-he.ac.uk/knowledge-hub/core-curriculum-psychology-undergraduate-medical-education (accessed on 28 December 2021).
- BeSST. A Core Curriculum for Sociology in Undergraduate Medical Education. 2016. Available online: https://pearl.plymouth.ac.uk/bitstream/handle/10026.1/8596/FINAL%20PREPUBLICATION%20Core%20Curriculum%20booklet%20%20-%20spreads.pdf?sequence=2 (accessed on 28 December 2021).
- Atkinson, P. For Ethnography; Sage: London, UK, 2015. [Google Scholar]
- Cholerton, S.; Jordan, R. Core Curriculum and Student-Selected Components. A Practical Guide for Medical Teachers, 3rd ed.; Churchill Livingstone Elsevier: Edinburgh, UK, 2009; pp. 193–201. [Google Scholar]
- Metcalfe, N.H.; Brown, A.K. History of medicine student selected components at UK medical schools: A questionnaire-based study. JRSM Short Rep. 2011, 2, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Murdoch-Eaton, D.; Ellershaw, J.; Garden, A.; Newble, D.; Perry, M.; Robinson, L.; Smith, J.; Stark, P.; Whittle, S. Student-selected components in the undergraduate medical curriculum: A multi-institutional consensus on purpose. Med. Teach. 2004, 26, 33–38. [Google Scholar] [CrossRef]
- Dikomitis, L. How Medical Students in the United Kingdom Think: About Anthropology, for Example. In Anthropology in Medical Education: Sustaining Engagement and Impact; Martinez, I., Wiedman, D.W., Eds.; Springer Nature: Cham, Switzerland, 2021; pp. 91–113. [Google Scholar]
- Walford, G. The practice of writing ethnographic fieldnotes. Ethnogr. Educ. 2009, 4, 117–130. [Google Scholar] [CrossRef]
- Stephen, B. Becoming a Critically Reflective Teacher; John Wiley & Sons: New York, NY, USA, 1995. [Google Scholar]
- Tripp, D. Critical Incidents in Teaching: Developing Professional Judgement; Routledge: London, UK, 1993. [Google Scholar]
- Keefer, J.M. The critical incident questionnaire (CIQ): From research to practice and back again. In Proceedings of the 50th Annual Adult Education Research Conference, Chicago, IL, USA, 28–30 May 2009; pp. 177–180. [Google Scholar]
- Farrell, L.; Bourgeois-Law, G.; Regehr, G.; Ajjawi, R. Autoethnography: Introducing “I’ into medical education research. Med. Educ. 2015, 49, 974–982. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clark, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2014, 11, 589–597. [Google Scholar] [CrossRef]
- Fram, S. The constant comparative analysis method outside of grounded theory. Qual. Rep. 2013, 18, 1–25. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Nathan, R. My Freshman Year: What a Professor Learned by Becoming a Student; Cornell University Press: Ithaca, NY, USA, 2005. [Google Scholar]
- Tuchman, G. Wannabe U: Inside the Corporate University; University of Chicago Press: Chicago, IL, USA, 2009. [Google Scholar]
- Kendall, K.; Collett, T.; de Iongh, A.; Forrest, S.; Kelly, M. Teaching sociology to undergraduate medical students. Med. Teach. 2018, 40, 1201–1207. [Google Scholar] [CrossRef]
- Thompson, B.M.; Haidet, P.; Casanova, R.; Vivo, R.P.; Gomez, A.G.; Brown, A.F.; Richter, R.A.; Crandall, S.J. Medical students’ perceptions of their teachers’ and their own cultural competency: Implications for education. J. Gen. Intern. Med. 2010, 25, S91–S94. [Google Scholar] [CrossRef] [Green Version]
- Beagan, B. Teaching social and cultural awareness to medical students: “it’s all very nice to talk about it in theory, but ultimately it makes no difference”. Acad. Med. 2003, 78, 605–614. [Google Scholar] [CrossRef]
- Dogra, N. The views of medical education stakeholders on guidelines for cultural diversity teaching. Med Teach. 2007, 29, e41–e46. [Google Scholar] [CrossRef]
- Litva, A.; Peters, S. Exploring barriers to teaching behavioural and social sciences in medical education. Med. Educ. 2008, 42, 309–314. [Google Scholar] [CrossRef]
- Hafferty, F.W. Beyond curriculum reform: Confronting medicine’s hidden curriculum. Acad. Med. 1998, 73, 403–407. [Google Scholar] [CrossRef]
- Willen, S.S.; Bullon, A.; Good, M.J. Opening up a huge can of worms: Reflections on a “cultural sensitivity” course for psychiatry residents. Harv. Rev. Psychiatry 2010, 18, 247–253. [Google Scholar] [CrossRef]
- Iida, J.; Nishigori, H. Managing Uncertainty: Collaborative Clinical Case Conferences for Physicians and Anthropologists in Japan. In Anthropology in Medical Education: Sustaining Engagement and Impact; Martinez, I., Wiedman, D.W., Eds.; Springer Nature: Cham, Switzerland, 2021; pp. 69–90. [Google Scholar]
- Lukšaitė, E.; Fricker, R.A.; McKinley, R.K.; Dikomitis, L. Conceptualising and teaching biomedical uncertainty to medical students: An exploratory qualitative study. Med. Sci. Educ. 2022, 32, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Blonder, L.X. Inclusivity in Medical Education: Teaching Integrative and Alternative Medicine in Kentucky. In Anthropology in Medical Education: Sustaining Engagement and Impact; Martinez, I., Wiedman, D.W., Eds.; Springer Nature: Cham, Switzerland, 2021; pp. 269–293. [Google Scholar]
- Constantinou, C.S. Applied Sociology of Health and Illness: A Problem Based Learning Approach; CRC Press: London, UK, 2014. [Google Scholar]
- Barr, J.; Ogden, K.; Rooney, K. Committing to patient-centred medical education. Clin. Teach. 2014, 11, 503–506. [Google Scholar] [CrossRef]
- Engel, G.L. The biopsychosocial model and the education of health professionals. Ann. N. Y. Acad. Sci. 1978, 310, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Engel, G.L. The biopsychosocial model and medical education: Who are to be the teachers? N. Engl. J. Med. 1982, 306, 802–805. [Google Scholar] [CrossRef] [PubMed]
- Astin, J.A.; Sierpina, V.S.; Forys, K.; Clarridge, B. Integration of the biopsychosocial model: Perspectives of medical students and residents. Acad. Med. 2008, 83, 20–27. [Google Scholar] [CrossRef]
- Wade, D.T.; Halligan, P.W. The biopsychosocial model of illness: A model whose time has come. Clin. Rehabil. 2017, 31, 995–1004. [Google Scholar] [CrossRef] [Green Version]
- ECLIPSE. Available online: www.eclipse-community.com (accessed on 30 December 2021).
- Scheffer, C.; Tausche, D.; Edelhäuser, F. “I wish I had a physician like that…”—The use of triangulation on the way towards a patient-centred medical education. Patient Educ. Couns. 2011, 82, 465–467. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dikomitis, L.; Wenning, B.; Ghobrial, A.; Adams, K.M. Embedding Behavioral and Social Sciences across the Medical Curriculum: (Auto) Ethnographic Insights from Medical Schools in the United Kingdom. Societies 2022, 12, 101. https://0-doi-org.brum.beds.ac.uk/10.3390/soc12040101
Dikomitis L, Wenning B, Ghobrial A, Adams KM. Embedding Behavioral and Social Sciences across the Medical Curriculum: (Auto) Ethnographic Insights from Medical Schools in the United Kingdom. Societies. 2022; 12(4):101. https://0-doi-org.brum.beds.ac.uk/10.3390/soc12040101
Chicago/Turabian StyleDikomitis, Lisa, Brianne Wenning, Andrew Ghobrial, and Karen M. Adams. 2022. "Embedding Behavioral and Social Sciences across the Medical Curriculum: (Auto) Ethnographic Insights from Medical Schools in the United Kingdom" Societies 12, no. 4: 101. https://0-doi-org.brum.beds.ac.uk/10.3390/soc12040101