
Seroprevalence of Antibodies to SARS-CoV-2 in Guangdong Province, China between March to June 2020

 , and
, and
Abstract
:1. Introduction
2. Results
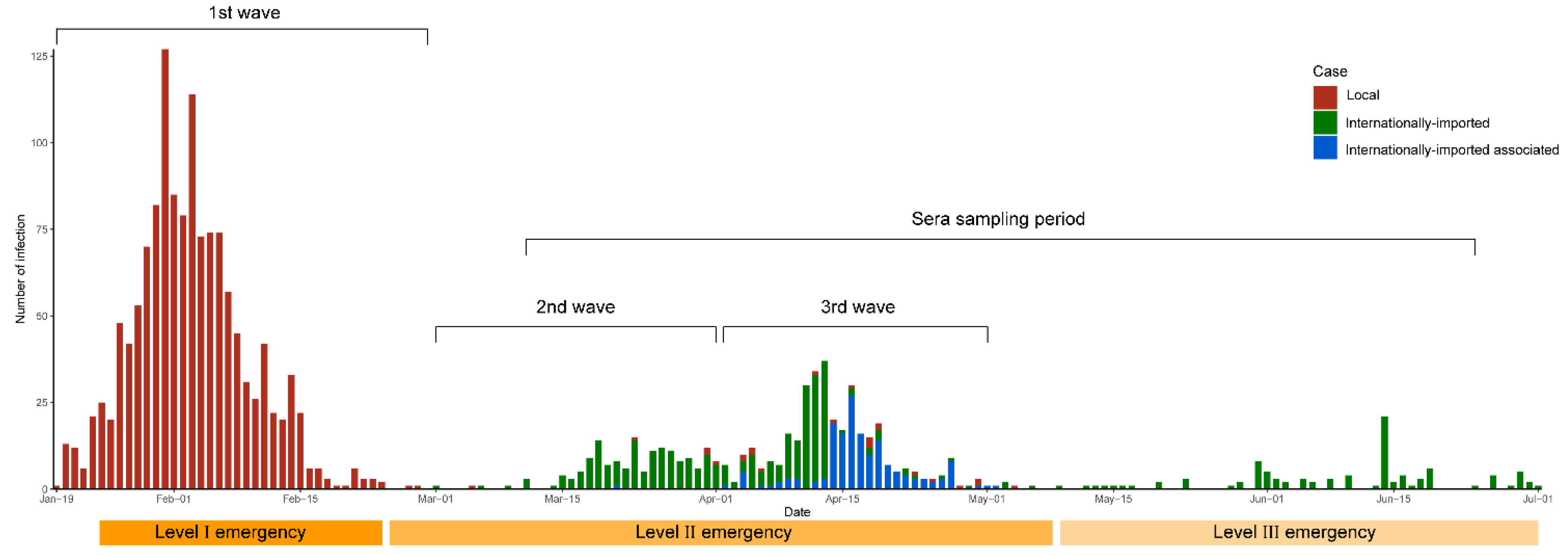
2.1. Reported COVID-19 Cases in Guangdong Province between 19 January and 1 July 2020
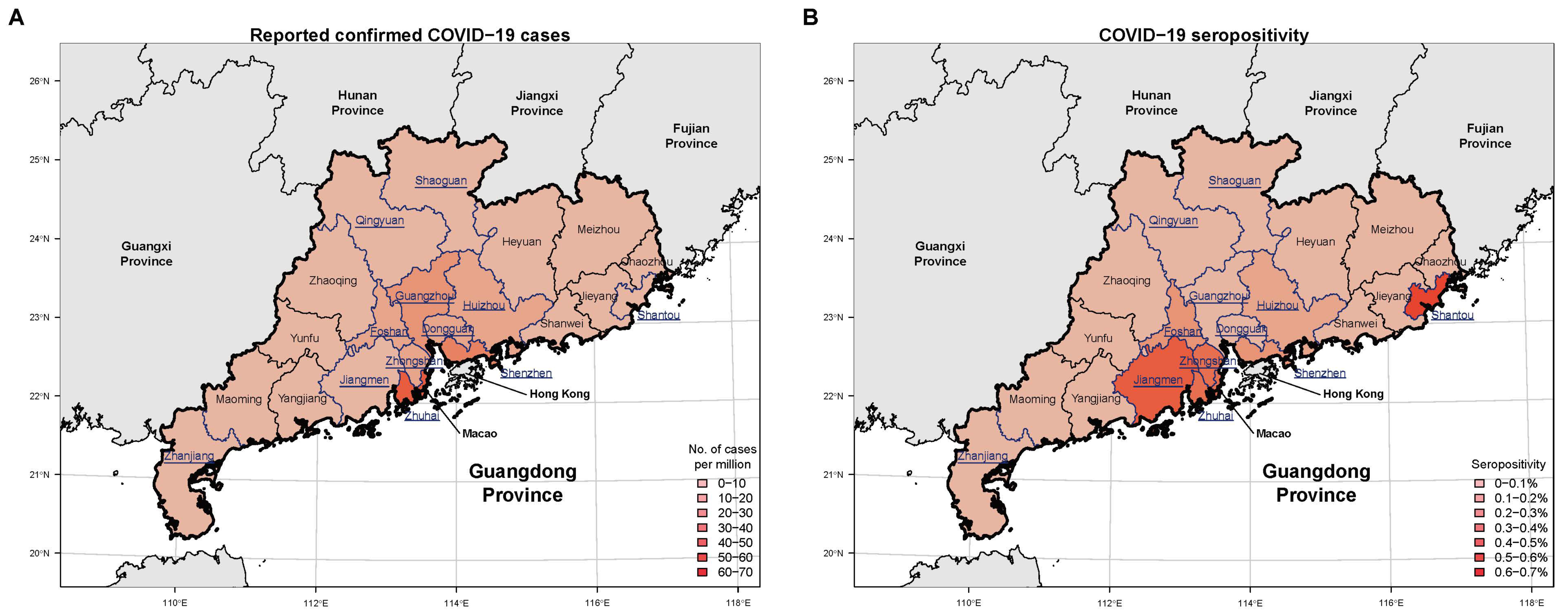
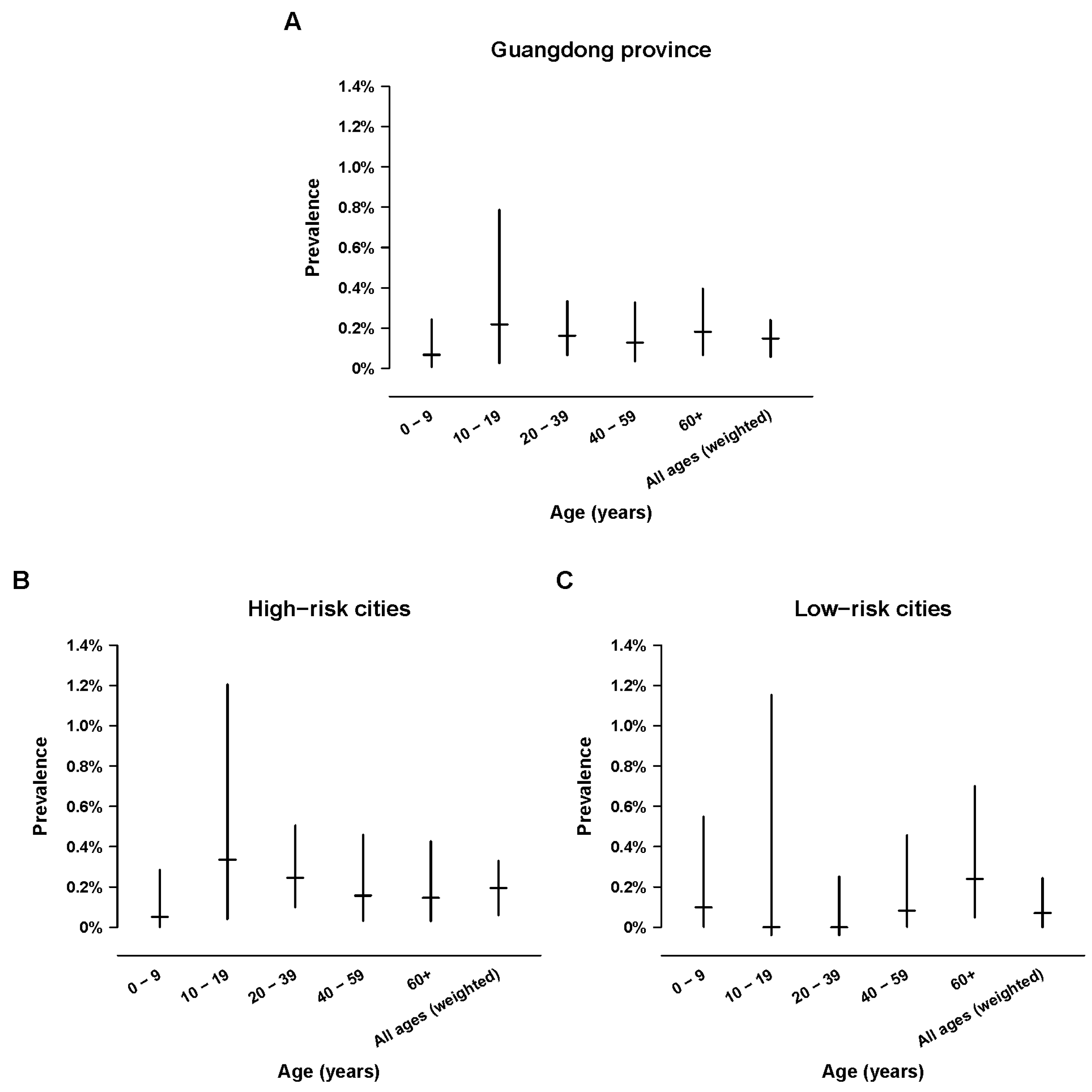
2.2. Seroprevalence in Guangdong
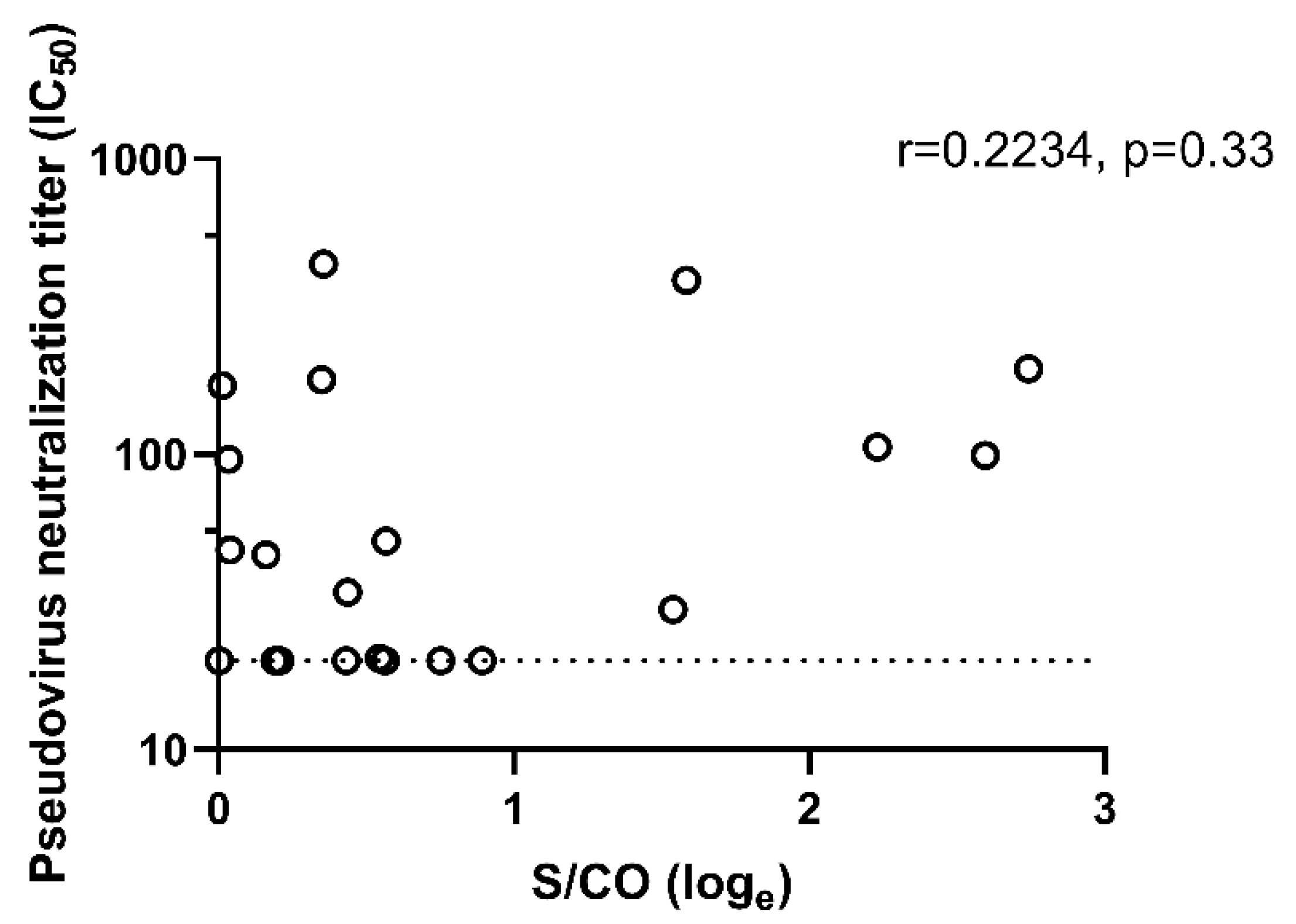
2.3. Proportion of Seropositive Samples with Neutralizing Titers
3. Discussion
Limitations of the Study
4. Materials and Methods
4.1. Epidemiologic Data Source
4.2. Study Design
4.3. Serologic Assays
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guangdong Provincial Bureau of Statistics. Analysis of Guangdong’s Population Development in 2019. Available online: http://stats.gd.gov.cn/tjfx/content/post_2985688.html (accessed on 28 April 2020).
- Yang, Q.S.; Zhang, H.X.; Mwenda, K.M. County-Scale Destination Migration Attractivity Measurement and Determinants Analysis: A Case Study of Guangdong Province, China. Sustainability 2019, 11, 362. [Google Scholar] [CrossRef] [Green Version]
- Health Commission of Guangdong Province. The National Health Commission Confirmed the First Confirmed Case of Pneumonia Infected by Novel Coronavirus in Guangdong Province. Available online: http://wsjkw.gd.gov.cn/xxgzbdfk/content/post_2880738.html (accessed on 20 January 2020).
- Guangzhou Municipal Health Commission. Guangzhou Confirmed 2 Cases of Pneumonia with Novel Coronavirus Infection. Available online: http://wjw.gz.gov.cn/ztzl/xxfyyqfk/yqtb/content/post_5643152.html (accessed on 22 January 2020).
- Health Commission of Guangdong Province. Guangdong Province Decided to Launch a First-Level Response to a Major Public Health Emergency. Available online: http://wsjkw.gd.gov.cn/xxgzbdfk/fkdt/content/post_2879152.html (accessed on 23 January 2020).
- Tanne, J.H. Covid-19: US cases are greatly underestimated, seroprevalence studies suggest. BMJ 2020, 370. [Google Scholar] [CrossRef] [PubMed]
- Pollan, M.; Perez-Gomez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernan, M.A.; Perez-Olmeda, M.; Sanmartin, J.L.; Fernandez-Garcia, A.; Cruz, I.; de Larrea, F.N.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Stringhini, S.; Wisniak, A.; Piumatti, G.; Azman, A.S.; Lauer, S.A.; Baysson, H.; De Ridder, D.; Petrovic, D.; Schrempft, S.; Marcus, K.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Geneva, Switzerland (SEROCoV-POP): A population-based study. Lancet 2020, 396, 313–319. [Google Scholar] [CrossRef]
- Lu, J.; du Plessis, L.; Liu, Z.; Hill, V.; Kang, M.; Lin, H.; Sun, J.; Francois, S.; Kraemer, M.U.G.; Faria, N.R.; et al. Genomic Epidemiology of SARS-CoV-2 in Guangdong Province, China. Cell 2020, 181, 997–1003 e1009. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zuiani, A.; Fischinger, S.; Mullur, J.; Atyeo, C.; Travers, M.; Lelis, F.J.N.; Pullen, K.M.; Martin, H.; Tong, P.; et al. Quick COVID-19 Healers Sustain Anti-SARS-CoV-2 Antibody Production. Cell 2020, 183, 1496–1507 e1416. [Google Scholar] [CrossRef] [PubMed]
- Lei, Q.; Li, Y.; Hou, H.Y.; Wang, F.; Ouyang, Z.Q.; Zhang, Y.; Lai, D.Y.; Jo-Lewis, B.N.; Xu, Z.W.; Zhang, B.; et al. Antibody dynamics to SARS-CoV-2 in asymptomatic COVID-19 infections. Allergy 2020. [Google Scholar] [CrossRef] [PubMed]
- Marien, J.; Ceulemans, A.; Michiels, J.; Heyndrickx, L.; Kerkhof, K.; Foque, N.; Widdowson, M.A.; Mortgat, L.; Duysburgh, E.; Desombere, I.; et al. Evaluating SARS-CoV-2 spike and nucleocapsid proteins as targets for antibody detection in severe and mild COVID-19 cases using a Luminex bead-based assay. J. Virol. Methods 2021, 288. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Liu, M.; Wang, A. Evaluating the association of clinical characteristics with neutralizing antibody levels in patients who have recovered from mild COVID-19 in Shanghai, China. JAMA Intern. Med. 2020, 180, 1405. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Sun, J.; Nie, S.; Li, H.Y.; Kong, Y.Z.; Liang, M.; Hou, J.L.; Huang, X.Z.; Li, D.F.; Ma, T.; et al. Seroprevalence of immunoglobulin M and G antibodies against SARS-CoV-2 in China. Nat. Med. 2020, 76. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Lin, Y.; Bi, J.; Li, J.; Liang, Y.; Wong, S.S.; Zanin, M.; Yang, Z.; Li, C.; Zhong, R.; et al. Serosurvey of SARS-CoV-2 among hospital visitors in China. Cell Res. 2020, 30, 817–818. [Google Scholar] [CrossRef]
- Pan, Y.; Li, X.; Yang, G.; Fan, J.; Tang, Y.; Hong, X.; Guo, S.; Li, J.; Yao, D.; Cheng, Z.; et al. Seroprevalence of SARS-CoV-2 immunoglobulin antibodies in Wuhan, China: Part of the city-wide massive testing campaign. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Wu, S.; Tao, H.; Zeng, G.; Zhou, F.; Guo, F.; Wang, X. Prevalence of IgG Antibodies to SARS-CoV-2 in Wuhan—Implications for the Ability to Produce Long-Lasting Protective Antibodies against SARS-CoV-2. MedRxiv 2020. [Google Scholar] [CrossRef]
- Chang, L.; Hou, W.; Zhao, L.; Zhang, Y.; Wang, Y.; Wu, L.; Xu, T.; Wang, L.; Wang, J.; Ma, J.; et al. The Prevalence of Antibodies to SARS-CoV-2 among Blood Donors in China. Nat. Commun. 2021, 12, 1–10. [Google Scholar] [CrossRef]
- Kang, M. Three Waves of COVID-19 Epidemic and Adaptive Response Measures in Guangdong Province, China; Guangdong Provincial Center for Disease Control and Prevention: Guangzhou, China, 2020; Manuscript in preparation. [Google Scholar]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11. [Google Scholar] [CrossRef]
- National Health Commission of the People’s Republic of China. Protocol on Prevention and Control of Novel Coronavirus Pneumonia (Edition 5). Available online: http://www.nhc.gov.cn/jkj/s3577/202002/a5d6f7b8c48c451c87dba14889b30147.shtml (accessed on 4 January 2021).
- National Health Commission of the People’s Republic of China. Pneumonia Prevention and Control Plan for Novel Coronavirus Infection (Second Edition). Available online: http://www.nhc.gov.cn/xcs/zhengcwj/202001/c67cfe29ecf1470e8c7fc47d3b751e88.shtml (accessed on 4 January 2021).
- National Health Commission of the People’s Republic of China. Protocol on Prevention and Control of Novel Coronavirus Pneumonia (Edition 6). Available online: http://www.nhc.gov.cn/jkj/s3577/202003/4856d5b0458141fa9f376853224d41d7.shtml (accessed on 4 January 2021).
- National Health Commission of the People’s Republic of China. Protocol on Prevention and Control of Novel Coronavirus Pneumonia (Edition 3). Available online: http://www.nhc.gov.cn/jkj/s7923/202001/470b128513fe46f086d79667db9f76a5.shtml (accessed on 4 January 2021).
- National Health Commission of the People’s Republic of China. Protocol on Prevention and Control of Novel Coronavirus Pneumonia (Edition 4). Available online: http://www.nhc.gov.cn/jkj/s3577/202002/573340613ab243b3a7f61df260551dd4.shtml (accessed on 4 January 2021).
- Tsang, T.K.; Wu, P.; Lin, Y.; Lau, E.H.Y.; Leung, G.M.; Cowling, B.J. Effect of changing case definitions for COVID-19 on the epidemic curve and transmission parameters in mainland China: A modelling study. Lancet Public Health 2020, 5, e289–e296. [Google Scholar] [CrossRef]
- Health Commission of Guangdong Province. Available online: http://wsjkw.gd.gov.cn/ (accessed on 4 January 2021).
- Guangdong Provincial Bureau of Statistics. The Data Bulletin of the 1% Population Sample Survey of Guangdong Province in 2015. Available online: http://stats.gd.gov.cn/tjgb/content/post_1430125.html (accessed on 10 May 2016).
- Long, Q.X.; Liu, B.Z.; Deng, H.J.; Wu, G.C.; Deng, K.; Chen, Y.K.; Liao, P.; Qiu, J.F.; Lin, Y.; Cai, X.F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Ou, X.; Liu, Y.; Lei, X.; Li, P.; Mi, D.; Ren, L.; Guo, L.; Guo, R.; Chen, T.; Hu, J.; et al. Characterization of spike glycoprotein of SARS-CoV-2 on virus entry and its immune cross-reactivity with SARS-CoV. Nat. Commun. 2020, 11, 1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prefecture | Total Cases by March 3 a n(%) | Total Cases by July 1 a n(%) | Population (Million) b | Female (%) a | Incidence (Per Million) | Designated Risk Level | Migration Index with Wuhan c |
|---|---|---|---|---|---|---|---|
| Yunfu | 0 (0) | 0 (0) | 2.5269 | 49 | 0 | Low | 0 |
| Heyuan | 4 (0.3) | 5 (0.3) | 3.0939 | 49 | 1.29 | Low | 0 |
| Jieyang | 8 (0.6) | 11 (0.7) | 6.0894 | 49 | 1.32 | Low | 0 |
| Shanwei | 5 (0.4) | 5 (0.3) | 2.9936 | 47 | 1.67 | Low | 0 |
| Chaozhou | 5 (0.4) | 6 (0.4) | 2.6566 | 50 | 1.81 | Low | 0 |
| Maoming | 14 (1.0) | 14 (0.9) | 6.3132 | 47 | 2.22 | Low | 0 |
| Meizhou | 16 (1.2) | 17 (1.0) | 4.3788 | 51 | 2.91 | Low | 0 |
| Zhanjiang | 22 (1.6) | 24 (1.5) | 7.3320 | 47 | 3.00 | Low | 1,2 |
| Qingyuan | 12 (0.9) | 12 (0.7) | 3.8740 | 49 | 3.10 | Low | 2 |
| Shaoguan | 10 (0.7) | 10 (0.6) | 2.9976 | 50 | 3.34 | Low | 2 |
| Shantou | 25 (1.9) | 26 (1.6) | 5.6385 | 50 | 4.44 | Low | 2 |
| Zhaoqing * | 19 (1.4) | 20 (1.2) | 4.1517 | 49 | 4.58 | Low | 0 |
| Jiangmen * | 23 (1.7) | 24 (1.5) | 4.5982 | 49 | 5.01 | Low | 2 |
| Yangjiang | 14 (1.0) | 14 (0.9) | 2.5556 | 47 | 5.51 | Low | 0 |
| Foshan * | 84 (6.2) | 100 (6.1) | 7.9057 | 46 | 10.63 | High | 2 |
| Dongguan * | 99 (7.3) | 100 (6.1) | 8.3922 | 44 | 11.80 | High | 1,2 |
| Huizhou * | 62 (4.6) | 62 (3.8) | 4.8300 | 47 | 12.84 | High | 1,2 |
| Zhongshan * | 66 (4.9) | 69 (4.2) | 3.3100 | 46 | 19.94 | High | 2 |
| Guangzhou * | 346 (25.6) | 558 (33.9) | 14.9044 | 49 | 23.22 | High | 1,2 |
| Shenzhen * | 418 (31.0) | 462 (28.2) | 13.0266 | 46 | 32.10 | High | 1,2 |
| Zhuhai * | 98 (7.3) | 103 (6.3) | 1.8911 | 48 | 51.85 | High | 1,2 |
| Total (%) | 1350 (100) | 1642 (100) | 113.46 | ||||
| Average | 48 | 9.65 |
| Author | Location | Sampling Period | Seropositivity for IgG or IgG and IgM (%) | 95% Confidence Interval | Total Population Surveyed | Sampling Population | Approach |
|---|---|---|---|---|---|---|---|
| Xu et al. [14] | Wuhan | March–April 2020 | 3.8 | 2.6 to 5.4 | 714 | Healthcare Workers | Screening |
| Guangzhou, Foshan | 2.80 | 1.8 to 4.6 | 563 | Hemodialysis Patients | |||
| 1.20 | 0.4 to 3.3 | 260 | Healthcare Workers | ||||
| 1.40 | 0.6 to 2.9 | 442 | Factory Workers | ||||
| Sichuan | 0.58 | 0.45 to 0.76 | 9442 | General Community | |||
| Liang et al. [15] | Wuhan | January–April 2020 | 2.10 | Not reported | 8272 | Hospital Visitors | Residual Sera |
| Guangzhou | 0.60 | Not reported | 8782 | Hospital Visitors | Residual Sera | ||
| Pan et al. [16] | Wuhan | May 2020 | 2.39 | 2.27 to 2.52 | 61,437 | General Community | Cluster Sampling |
| Liu et al. [17] | Wuhan | February–April 2020 | 4.60 | 4.3 to 4.9 | 19,555 | General Workers | Screening |
| Chang et al. [18] | Shijiazhuang | April 2020 | 0.0074 | 0.0013 to 0.042 | 13,540 | Blood Donors | Residual Sera |
| Shenzhen | 0.029 | 0.0081 to 0.11 | 6810 | ||||
| Wuhan | 2.29 | 2.08 to 2.52 | 17,794 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiao, C.; Leung, N.H.L.; Cheng, Y.; Lei, H.; Ling, S.; Lin, X.; Tao, R.; Huang, X.; Guan, W.; Yang, Z.; et al. Seroprevalence of Antibodies to SARS-CoV-2 in Guangdong Province, China between March to June 2020. Pathogens 2021, 10, 1505. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10111505
Xiao C, Leung NHL, Cheng Y, Lei H, Ling S, Lin X, Tao R, Huang X, Guan W, Yang Z, et al. Seroprevalence of Antibodies to SARS-CoV-2 in Guangdong Province, China between March to June 2020. Pathogens. 2021; 10(11):1505. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10111505
Chicago/Turabian StyleXiao, Cheng, Nancy Hiu Lan Leung, Yating Cheng, Hui Lei, Shiman Ling, Xia Lin, Ran Tao, Xianzhong Huang, Wenda Guan, Zifeng Yang, and et al. 2021. "Seroprevalence of Antibodies to SARS-CoV-2 in Guangdong Province, China between March to June 2020" Pathogens 10, no. 11: 1505. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10111505