
Exposure to Leptospira spp. and Associated Risk Factors in the Human, Cattle and Dog Populations in Bhutan

 ,
,  , ,
, ,
Abstract
:
1. Introduction
2. Methods
2.1. Study Populations, Samples and Data Collection
2.2. Serological Testing
ELISA and Microscopic Agglutination Test
2.3. Data Analysis
2.3.1. Case Definitions
2.3.2. Humans
2.3.3. Bovines and Dogs
3. Results
3.1. Humans
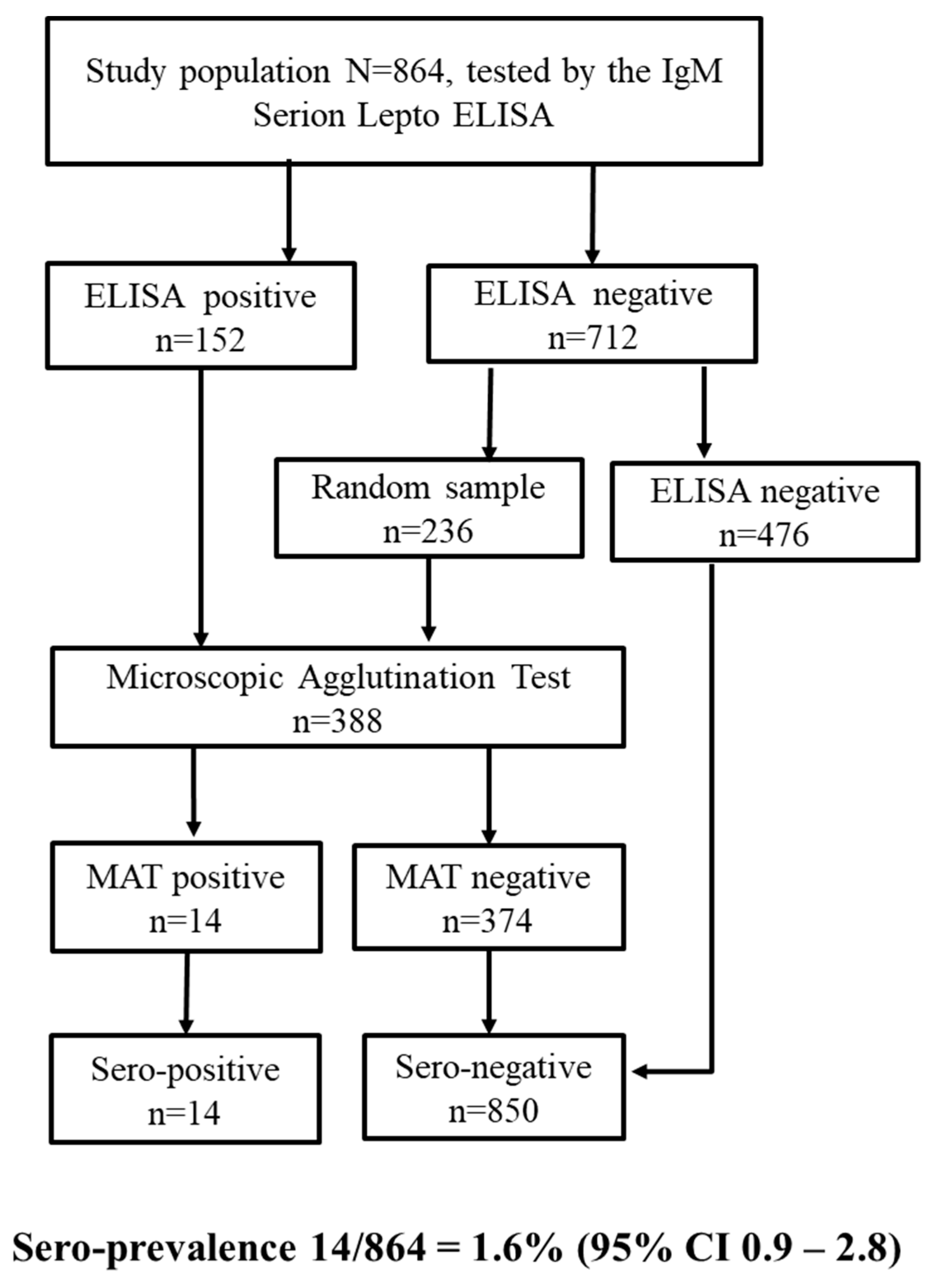
3.1.1. Serological Tests
3.1.2. ELISA Performance Based on the MAT
3.1.3. Seroprevalence
3.1.4. Risk Factors for Seropositivity
3.2. Animals
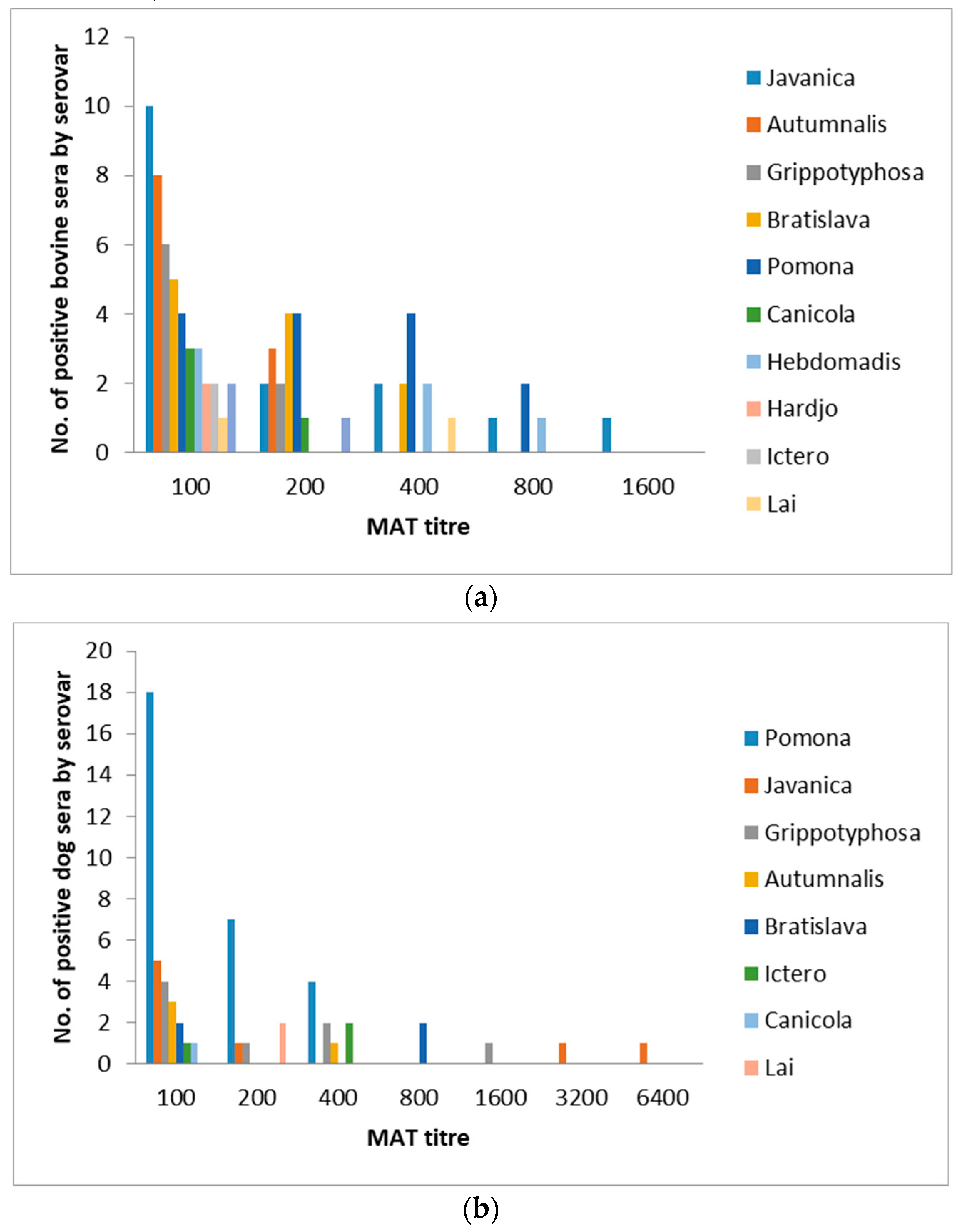
3.2.1. Leptospira spp. Seroprevalence in Bovines
3.2.2. Leptospira spp. Seroprevalence in Dogs
4. Discussion
4.1. Leptospira spp. Seroprevalence and Risk Factors in Humans and Animals
4.2. Study Design Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Costa, F.; Hagan, J.E.; Calcagno, J.; Kane, M.; Torgerson, P.; Martinez-Silveira, M.S.; Stein, C.; Abela-Ridder, B.; Ko, A.I. Global Morbidity and Mortality of Leptospirosis: A Systematic Review. PLoS Negl. Trop. Dis. 2015, 9, e0003898. [Google Scholar] [CrossRef] [Green Version]
- Bharti, A.R.; Nally, J.E.; Ricaldi, J.N.; Matthias, M.A.; Diaz, M.M.; Lovett, M.A.; Levett, P.N.; Gilman, R.H.; Willig, M.R.; Gotuzzo, E.; et al. Leptospirosis: A zoonotic disease of global importance. Lancet Infect. Dis. 2003, 3, 757–771. [Google Scholar] [CrossRef]
- Yasuda, P.H.; Steigerwalt, A.G.; Sulzer, K.R.; Kaufmann, A.F.; Rogers, F.; Brenner, D.J. Deoxyribonucleic-Acid Relatedness between Serogroups and Serovars in the Family Leptospiraceae with Proposals for 7 New Leptospira Species. Int. J. Syst. Bacteriol. 1987, 37, 407–415. [Google Scholar] [CrossRef] [Green Version]
- Ramadass, P.; Jarvis, B.D.W.; Corner, R.J.; Penny, D.; Marshall, R.B. Genetic-Characterization of Pathogenic Leptospira Species by DNA Hybridization. Int. J. Syst. Bacteriol. 1992, 42, 215–219. [Google Scholar] [CrossRef] [Green Version]
- Hartskeerl, R.A.; Collares-Pereira, M.; Ellis, W.A. Emergence, control and re-emerging leptospirosis: Dynamics of infection in the changing world. Clin. Microbiol. Infect. 2011, 17, 494–501. [Google Scholar] [CrossRef] [Green Version]
- Cerqueira, G.M.; Picardeau, M. A century of Leptospira strain typing. Infect. Genet. Evol. 2009, 9, 760–768. [Google Scholar] [CrossRef]
- Thibeaux, R.; Iraola, G.; Ferrés, I.; Bierque, E.; Girault, D.; Soupé-Gilbert, M.-E.; Picardeau, M.; Goarant, C. Deciphering the unexplored Leptospira diversity from soils uncovers genomic evolution to virulence. Microb Genom. 2018, 4, e000144. [Google Scholar] [CrossRef] [PubMed]
- Caimi, K.; Ruybal, P. Leptospira spp., a genus in the stage of diversity and genomic data expansion. Infect. Genet. Evol. J. Mol. Epidemiol. Evol. Genet. Infect. Dis. 2020, 81, 104241. [Google Scholar] [CrossRef] [PubMed]
- Faine, S.; Adler, B.; Bolin, C.; Perolat, P. Leptospira and Leptospirosis, 2nd ed.; MediSci: Melbourne, Australia, 1999; p. 272. [Google Scholar]
- Adler, B.; de la Pena Moctezuma, A. Leptospira and leptospirosis. Vet. Microbiol. 2010, 140, 287–296. [Google Scholar] [CrossRef]
- Lubell, Y.; Althaus, T.; Blacksell, S.D.; Paris, D.H.; Mayxay, M.; Pan-Ngum, W.; White, L.J.; Day, N.P.; Newton, P.N. Modelling the Impact and Cost-Effectiveness of Biomarker Tests as Compared with Pathogen-Specific Diagnostics in the Management of Undifferentiated Fever in Remote Tropical Settings. PLoS ONE 2016, 11, e0152420. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.; Paris, D.H.; Blacksell, S.D.; Laongnualpanich, A.; Kantipong, P.; Chierakul, W.; Wuthiekanun, V.; Day, N.P.; Cooper, B.S.; Limmathurotsakul, D. How to Determine the Accuracy of an Alternative Diagnostic Test when It Is Actually Better than the Reference Tests: A Re-Evaluation of Diagnostic Tests for Scrub Typhus Using Bayesian LCMs. PLoS ONE 2015, 10, e0114930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regmi, L.; Pandey, K.; Malla, M.; Khanal, S.; Pandey, B.D. Sero-epidemiology study of leptospirosis in febrile patients from Terai region of Nepal. BioMed Cent. Infect. Dis. 2017, 17, 628. [Google Scholar] [CrossRef] [Green Version]
- Victoriano, A.F.B.; Smythe, L.D.; Gloriani-Barzaga, N.; Cavinta, L.L.; Kasai, T.; Limpakarnjanarat, K.; Ong, B.L.; Gongal, G.; Hall, J.; Coulombe, C.A.; et al. Leptospirosis in the Asia Pacific region. BioMed Cent. Ltd Infect. Dis. 2009, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattachan, B.; Jb, S.; Bg, D.; Sherchand, J. Leptospirosis: An Emerging Infectious Disease in Nepal. J. Inst. Med. 2016, 38, 2–3. [Google Scholar]
- Public Health Laboratory Ministry of Health, Notifiable Disease Surveillance Manual. Department of Public Health. Thimpu, Bhutan, 2008; p. 101. Available online: http://www.rcdc.gov.bt/web/wp-content/uploads/2015/07/Notifiable-Disease-Surveillance-Manual.pdf (accessed on 22 February 2021).
- Phuentshok, Y.; Dorji, K.; Zangpo, T.; Davidson, S.A.; Takhampunya, R.; Tenzinla, T.; Dorjee, C.; Morris, R.S.; Jolly, P.D.; Dorjee, S.; et al. Survey and Phylogenetic Analysis of Rodents and Important Roden Borne Zoonotic Pathogens in Gedu, Bhutan. Korean J. Parasitol. 2018, 56, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Tenzin, T. Risk Based Surveillance of Leptospirosis in Cross-Species Domestic Animals in Bhutan; Disease Prevention & Control Unit National Centre for Animal Health: Thimphu, 2015. Available online: https://www.ncah.gov.bt/up_Files/pic_177.pdf (accessed on 22 February 2021).
- National. Statistics. Bureau Bhutan at a Glance 2019. Available online: http://www.nsb.gov.bt/publication/files/pub1ai6514dg.pdf (accessed on 12 December 2020).
- Tshokey, T.; Stenos, J.; Durrheim, D.N.; Eastwood, K.; Nguyen, C.; Graves, S.R. Seroprevalence of rickettsial infections and Q fever in Bhutan. PLoS Negl. Trop. Dis. 2017, 11, e0006107. [Google Scholar] [CrossRef] [Green Version]
- Tshokey, T.; Stenos, J.; Tenzin, T.; Drukpa, K.; Gurung, R.B.; Graves, S.R. Serological Evidence of Rickettsia, Orientia, and Coxiella in Domestic Animals from Bhutan: Preliminary Findings. Vector Borne Zoonotic Dis. 2019, 19, 95–101. [Google Scholar] [CrossRef]
- Wangdi, J.; Mindu; Bhujel, P.; Karma; Wangchuk, S. Productive and reproductive performance of dairy cattle and their crossbreds in Bhutan. Livest. Res. Rural. Dev. 2014, 26, 181. [Google Scholar]
- Office International des Epizooties (OIE), Leptospirosis. In OIE Terrestrial Manual; Office International des Epizooties (OIE), 2018; pp. 503–513. Available online: https://www.oie.int/en/standard-setting/terrestrial-manual/access-online/ (accessed on 12 December 2020).
- Levett, P.N. Leptospirosis. Clin. Microbiol. Rev. 2001, 14, 296–326. [Google Scholar] [CrossRef] [Green Version]
- Fleiss, J.L. Statistical methods for RATES and Proportions; John Wiley & Sons Inc.: New York, NY, USA, 1981. [Google Scholar]
- Jansen, A.; Luge, E.; Guerra, B.; Wittschen, P.; Gruber, A.D.; Loddenkemper, C.; Schneider, T.; Lierz, M.; Ehlert, D.; Appel, B.; et al. Leptospirosis in urban wild boars, Berlin, Germany. Emerg. Infect. Dis 2007, 13, 739–742. [Google Scholar] [CrossRef]
- Levett, P.N. Usefulness of Serologic Analysis as a Predictor of the Infecting Serovar in Patients with Severe Leptospirosis. Clin. Infect. Dis. 2003, 36, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Chirathaworn, C.; Inwattana, R.; Poovorawan, Y.; Suwancharoen, D. Interpretation of microscopic agglutination test for leptospirosis diagnosis and seroprevalence. Asian Pac. J. Trop. Biomed. 2014, 4, S162–S164. [Google Scholar] [CrossRef] [Green Version]
- Blanco, R.M.; dos Santos, L.F.; Galloway, R.L.; Romero, E.C. Is the microagglutination test (MAT) good for predicting the infecting serogroup for leptospirosis in Brazil? Comp. Immunol. Microbiol. Infect. Dis. 2016, 44, 34–36. [Google Scholar] [CrossRef] [PubMed]
- Dreyfus, A.; Wilson, P.; Benschop, J.; Collins-Emerson, J.; Verdugo, C.; Heuer, C. Seroprevalence and herd-level risk factors for seroprevalence of Leptospira spp. in sheep, beef cattle and deer in New Zealand. N. Z. Vet. J. 2018, 66, 302–311. [Google Scholar] [CrossRef]
- Shrestha, R.; McKenzie, J.S.; Gautam, M.; Adhikary, R.; Pandey, K.; Koirala, P.; Bc, G.B.; Miller, L.C.; Collins-Emerson, J.; Craig, S.B.; et al. Determinants of clinical leptospirosis in Nepal. Zoonoses Public Health 2018, 65, 972–983. [Google Scholar] [CrossRef] [PubMed]
- Gompo, T.R.; Jyoti, S.; Pandit, S.; Sapkota, R.C.; Pandey, A. Sero-prevalence and risk factors of leptospirosis in commercial cattle herds of Rupandehi district, Nepal. bioRxiv 2020. [Google Scholar] [CrossRef]
- Ojha, K.C.; Singh, D.K.; Kaphle, K.; Shah, Y.; Pant, D.K. Sero-prevalence of leptospirosis and differentiation in blood parameters between positive and negative cases in dogs of Kathmandu Valley. Trans. R. Soc. Trop. Med. Hyg. 2018, 112, 378–382. [Google Scholar] [CrossRef]
- Alinaitwe, L.; Kankya, C.; Allan, K.J.; Rodriguez-Campos, S.; Torgerson, P.; Dreyfus, A. Bovine leptospirosis in abattoirs in Uganda: Molecular detection and risk of exposure among workers. Zoonoses Public Health 2019, 66, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Goarant, C. Leptospirosis: Risk factors and management challenges in developing countries. Res. Rep. Trop. Med. 2016, ume 7, 49–62. [Google Scholar] [CrossRef] [Green Version]
- Khanal, D.; Paudyal, N.; Khanal, S.; Prajapati, M.; Shrestha, M.; Bowen, R.; Acharya, M.; Shrestha, S.; Singh, U.; Thakur, R.; et al. Detection of Antibodies Against Leptospira hardjo in Large Ruminants of Nepal. Acta Sci. Agric. 2018, 2, 131–133. [Google Scholar]
- Goris, M. Diagnostic tests for human leptospirosis. In Second Meeting of the European Leptospirosis Society on Leptospirosis and Other Rodent Borne Hemorrhagic Fevers; European Leptospirosis Society Royal Tropical Institute: Amsterdam, The Netherlands, 16–18 April 2015. [Google Scholar]
- Schlichting, D.; Nöckler, K.; Bahn, P.; Luge, E.; Greiner, M.; Müller-Graf, C.; Mayer-Scholl, A. Estimation of the sensitivity and specificity of a Leptospira spp. in-house ELISA through Bayesian modelling. Int. J. Med. Microbiol. 2015, 305, 756–761. [Google Scholar] [CrossRef] [PubMed]
- Hem, S.; Ly, S.; Votsi, I.; Vogt, F.; Asgari, N.; Buchy, P.; Heng, S.; Picardeau, M.; Sok, T.; Ly, S.; et al. Estimating the Burden of Leptospirosis among Febrile Subjects Aged below 20 Years in Kampong Cham Communities, Cambodia, 2007-2009. PLoS ONE 2016, 11, e0151555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niloofa, R.; Fernando, N.; De Silva, N.L.; Karunanayake, L.; Wickramasinghe, H.; Dikmadugoda, N.; Premawansa, G.; Wickramasinghe, R.; De Silva, H.J.; Premawansa, S.; et al. Diagnosis of Leptospirosis: Comparison between Microscopic Agglutination Test, IgM-ELISA and IgM Rapid Immunochromatography Test. PLoS ONE 2015, 10, e0129236. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Humans (N = 864) | Bovines (N = 130) | Dogs (N = 84) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| District | n (%) | N Pos (%) | 95% CI | n (%) | N Pos (%) | 95% CI | n (%) | N Pos (%) | 95% CI |
| Chukha | 108 (12.5) | 2 (1.8) | 0.32–7.19 | 20 (15.4) | 4 (20.0) | 6.61–44.27 | - 1 | - | |
| Mongar | 108 (12.5) | 1 (0.9) | 0.05–5.80 | 20 (15.4) | 9 (45.0) | 23.83–67.95 | 8 (9.5) | 6 (75.0) | 35.58–95.54 |
| Punakha | 108 (12.5) | 4 (2.8) | 1.19–9.77 | 7 (5.4) | 5 (71.4) | 30.26–94.89 | 9 (10.7) | 3 (33.3) | 9.04–69.08 |
| Samtse | 108 (12.5) | 3 (2.8) | 0.72–8.50 | 21 (16.1) | 9 (42.9) | 22.59–65.56 | 15 (17.9) | 7 (46.7) | 22.28–72.58 |
| Thimphu | 108 (12.5) | 0 (0.0) | 0.08–4.28 | 20 (15.4) | 2 (10.0) | 1.75–33.13 | 20 (23.8) | 8 (40.0) | 19.98–63.59 |
| Trashigang | 108 (12.5) | 3 (2.8) | 0.72–8.50 | 12 (9.23) | 4 (33.3) | 11.27–64.56 | 12 (14.3) | 5 (41.7) | 16.50–71.40 |
| Trongsa | 108 (12.5) | 0 (0.0) | 0.08–4.28 | 10 (7.7) | 2 (20.0) | 3.54–55.78 | 10 (11.9) | 5 (50.0) | 20.14–79.86 |
| Zhemgang | 108 (12.5) | 1 (0.3) | 0.05–5.80 | 20 (15.4) | 13 (65.0) | 40.95–83.69 | 10 (11.9) | 6 (60.0) | 27.37–86.31 |
| Explanatory Variable | Category | n (%) 1 | N Pos (%) 2 | p-Value 3 |
|---|---|---|---|---|
| Gender | Female | 519 (60.1) | 7 (1.35) | 0.584 |
| Male | 365 (39.9) | 7 (2.03) | ||
| Age groups (years) | 13–20 | 74 (8.6) | 0 (0.0) | 0.87 |
| 21–35 | 305 (35.3) | 5 (1.6) | ||
| 36–65 | 406 (47.0) | 8 (2.0) | ||
| 66–98 | 79 (9.1) | 1 (1.3) | ||
| Occupation | Herder/Farmer | 455 (52.7) | 4 (0.9) | 0.009 |
| Employee | 135 (15.6) | 5 (3.7) | ||
| Military | 9 (1.0) | 1 (11.1) | ||
| Student | 45 (5.2) | 1 (2.2) | ||
| Homemaker | 182 (21.0) | 1 (0.5) | ||
| Unemployed | 38 (4.4) | 2 (5.3) | ||
| Altitude (m) | High >2000 | 140 (16.2) | 0 (0.0) | 0.229 |
| Middle 1000–2000 | 584 (67.6) | 11 (1.9) | ||
| Low < 1000 | 140 (16.2) | 3 (2.1) | ||
| Geographical distribution | Rural | 608 (70.4) | 12 (2.0) | 0.252 |
| Urban | 256 (29.6) | 2 (0.8) | ||
| Contact to sheep 4 | No | - 5 | - | - |
| Yes | 16 | - | - | |
| Contact to yaks | No | - | - | - |
| Yes | 57 | - | - | |
| Contact to cattle | No | - | - | - |
| Yes | 268 | - | - | |
| Contact to dogs | No | - | - | - |
| Yes | 292 | - | - | |
| Contact to cats | No | - | - | - |
| Yes | 284 | - | - | |
| Contact to horses | No | - | - | - |
| Yes | 74 | - | - | |
| Had fever recently | No | 637 (75.6) | 6 (0.9) | 0.008 |
| Yes | 206 (24.4) | 8 (3.9) | ||
| Seropositive to SFG | No | 673 (77.9) | 12 (1.8) | 0.746 |
| Yes | 191 (22.1) | 2 (1.0) | ||
| Seropositive to TG | No | 834 (96.5) | 12 (1.4) | 0.082 |
| Yes | 30 (3.5) | 2 (6.7) | ||
| Seropositive to STG | No | 668 (77.3) | 8 (1.2) | 0.1 |
| Yes | 196 (22.7) | 6 (3.1) | ||
| Seropositive to Q-fever | No | 801 (93.0) | 13 (1.6) | 1.0 |
| Yes | 60 (7.0) | 1 (1.7) |
| Genomspecies | Serogroup | Serovar | Strain |
|---|---|---|---|
| L. interrogans | Australis | Australis | Ballico h |
| L. interrogans | Australis | Bratislava | Jez Bratislava bhc |
| L. interrogans | Autumnalis | Autumnalis | Akiyami A bhc |
| L. interrogans | Bataviae | Bataviae | Swart h |
| L. interrogans | Canicola | Canicola | Hond Utrecht IV bhc |
| L. interrogans | Hebdomadis | Hebdomadis | Hebdomadis bhc |
| L. interrogans | Icterohaemorrhagiae | Copenhageni | M20 h |
| L. interrogans | Icterohaemorrhagiae | Icterohaemorrhagiae | Ictero I bc |
| L. interrogans | Icterohaemorrhagiae | Icterohaemorrhagiae | RGA h |
| L. interrogans | Icterohaemorrhagiae | Lai | Lai bc |
| L. interrogans | Pomona | Pomona | Pomona bhc |
| L. interrogans | Pyrogenes | Pyrogenes | Salinem h |
| L. interrogans | Sejroe | Hardjo | Hardjoprajitno bhc |
| L. borgpetersenii | Ballum | Ballum | Mus 127 h |
| L. borgpetersenii | Javanica | Javanica | Veldrat Batavia 46 bhc |
| L. borgpetersenii | Sejroe | Saxkoebing | Mus 24 h |
| L. borgpetersenii | Sejroe | Sejroe | M 84 bhc |
| L. borgpetersenii | Tarassovi | Tarassovi | Perepelitsin h |
| L. kirschneri | Grippotyphosa | Grippotyphosa | Moskva V bhc |
| Humans | Bovines | Dogs | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Serovar | n Pos 1 | Prev 2 % | 95% CI 3 | n Pos 1 | Prev 2 % | 95% CI 4 | n Pos 1 | Prev 2 % | 95% CI 3 |
| Autumnalis | 0 | 0.00 | 0.01–0.55 | 11 | 8.46 | 3.34–19.80 | 4 | 4.76 | 1.54–12.40 |
| Bratislava | 8 | 0.93 | 0.43–1.89 | 11 | 8.46 | 3.49–19.07 | 4 | 4.76 | 1.54–12.40 |
| Canicola | 2 | 0.23 | 0.04–0.93 | 4 | 3.08 | 0.71–12.32 | 1 | 1.19 | 0.06–7.37 |
| Grippotyphosa | 0 | 0.00 | 0.01–0.55 | 8 | 6.15 | 2.63–13.75 | 8 | 9.52 | 4.48–18.40 |
| Hardjo | 0 | 0.00 | 0.01–0.55 | 2 | 1.54 | 0.35–6.41 | 0 | 0.00 | 0.10–5.45 |
| Hebdomadis | 1 | 0.12 | 0.01–0.75 | 6 | 4.62 | 1.04–18.20 | 0 | 0.00 | 0.10–5.45 |
| Icterohaemorrhagiae 5 | 0 | 0.00 | 0.01–0.55 | 2 | 1.54 | 0.18–12.00 | 3 | 3.57 | 0.92–10.80 |
| Javanica | 0 | 0.00 | 0.01–0.55 | 16 | 12.31 | 6.64–21.70 | 8 | 9.52 | 4.48–18.40 |
| Pomona | 0 | 0.00 | 0.01–0.55 | 14 | 10.77 | 5.42–20.25 | 33 | 39.29 | 28.99–50.57 |
| Sejroe | 0 | 0.00 | 0.01–0.55 | 3 | 2.31 | 0.26–17.61 | 0 | 0.000 | 0.10–5.45 |
| Lai | - 6 | - | - | 2 | 1.54 | 0.17–12.80 | 1 | 1.19 | 0.06–7.37 |
| Australis | 3 | 0.35 | 0.09–1.10 | - | - | - | - | - | - |
| Ballum | 0 | 0.00 | 0.01–0.55 | - | - | - | - | - | - |
| Bataviae | 2 | 0.23 | 0.04–0.93 | - | - | - | - | - | - |
| Copenhageni | 0 | 0.00 | 0.01–0.55 | - | - | - | - | - | - |
| Pyrogenes | 1 | 0.12 | 0.01–0.75 | - | - | - | - | - | - |
| Saxkoebing | 0 | 0.00 | 0.01–0.55 | - | - | - | - | - | - |
| Tarassovi | 0 | 0.00 | 0.01–0.55 | - | - | - | - | - | - |
| Explanatory Variable | Odds Ratio (OR) | p-Value | 95% Confidence Interval |
|---|---|---|---|
| Fever | 5.24 | 0.004 | 1.70–16.16 |
| Occupation | |||
| Homemaker | reference | ||
| Herder/farmer | 1.18 | 0.886 | 0.13–10.78 |
| Employee | 5.70 | 0.116 | 0.65–50.09 |
| Military | 26.65 | 0.028 | 1.44–494.28 |
| Student | 3.41 | 0.393 | 0.20–56.83 |
| Unemployed | 12.94 | 0.041 | 1.11–150.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dreyfus, A.; Ruf, M.-T.; Mayer-Scholl, A.; Zitzl, T.; Loosli, N.; Bier, N.S.; Hiereth, S.; Ulrich, S.; Poppert, S.; Straubinger, R.K.; et al. Exposure to Leptospira spp. and Associated Risk Factors in the Human, Cattle and Dog Populations in Bhutan. Pathogens 2021, 10, 308. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10030308
Dreyfus A, Ruf M-T, Mayer-Scholl A, Zitzl T, Loosli N, Bier NS, Hiereth S, Ulrich S, Poppert S, Straubinger RK, et al. Exposure to Leptospira spp. and Associated Risk Factors in the Human, Cattle and Dog Populations in Bhutan. Pathogens. 2021; 10(3):308. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10030308
Chicago/Turabian StyleDreyfus, Anou, Marie-Thérèse Ruf, Anne Mayer-Scholl, Theresa Zitzl, Nadine Loosli, Nadja Seyhan Bier, Stephanie Hiereth, Sebastian Ulrich, Sven Poppert, Reinhard K. Straubinger, and et al. 2021. "Exposure to Leptospira spp. and Associated Risk Factors in the Human, Cattle and Dog Populations in Bhutan" Pathogens 10, no. 3: 308. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10030308