
Do All Roads Lead to Rome? The Potential of Different Approaches to Diagnose Aelurostrongylus abstrusus Infection in Cats

 ,
,  , and
, and
Abstract
:
1. Introduction
2. Results
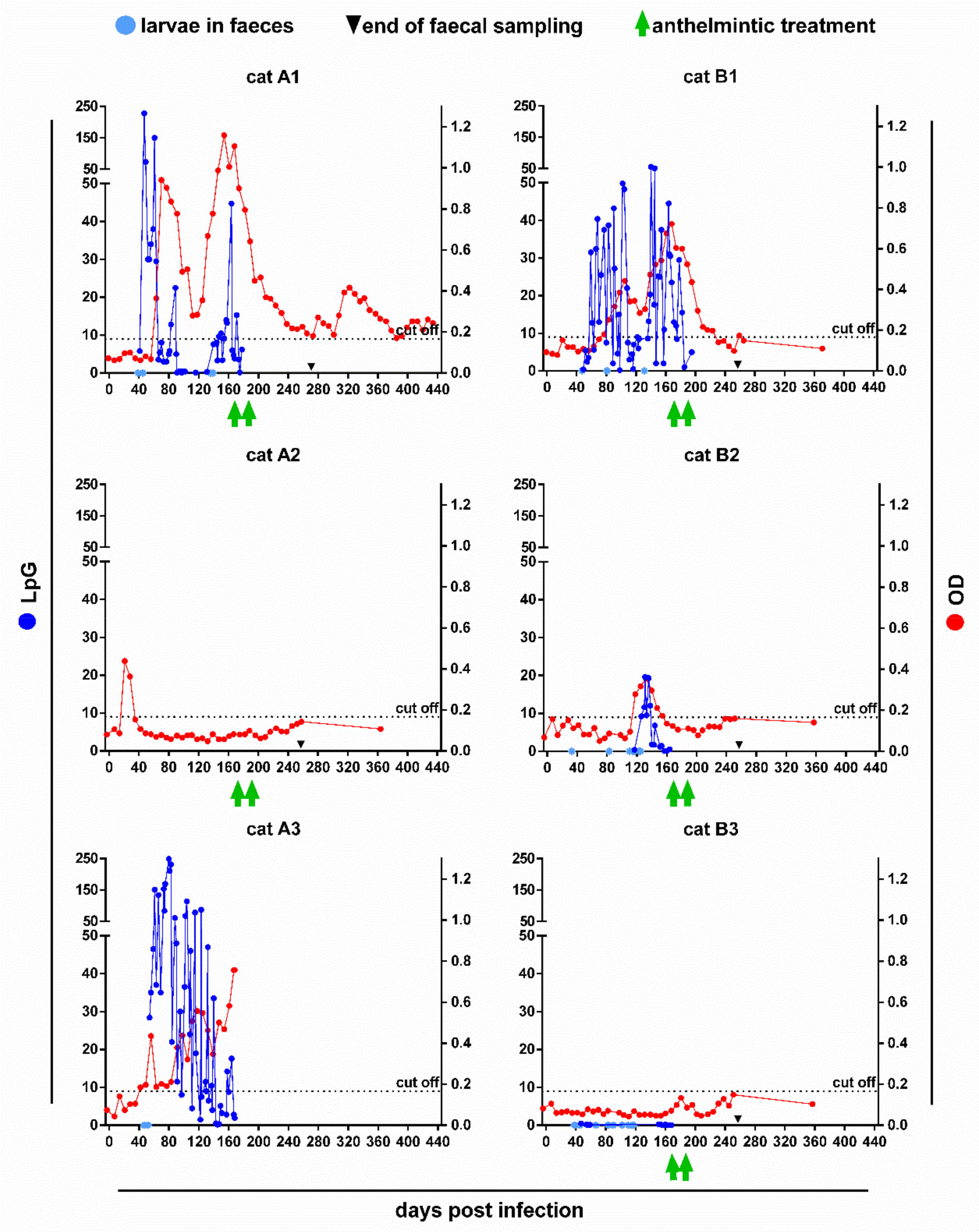
2.1. Faecal Larvae Counts
2.2. Serology
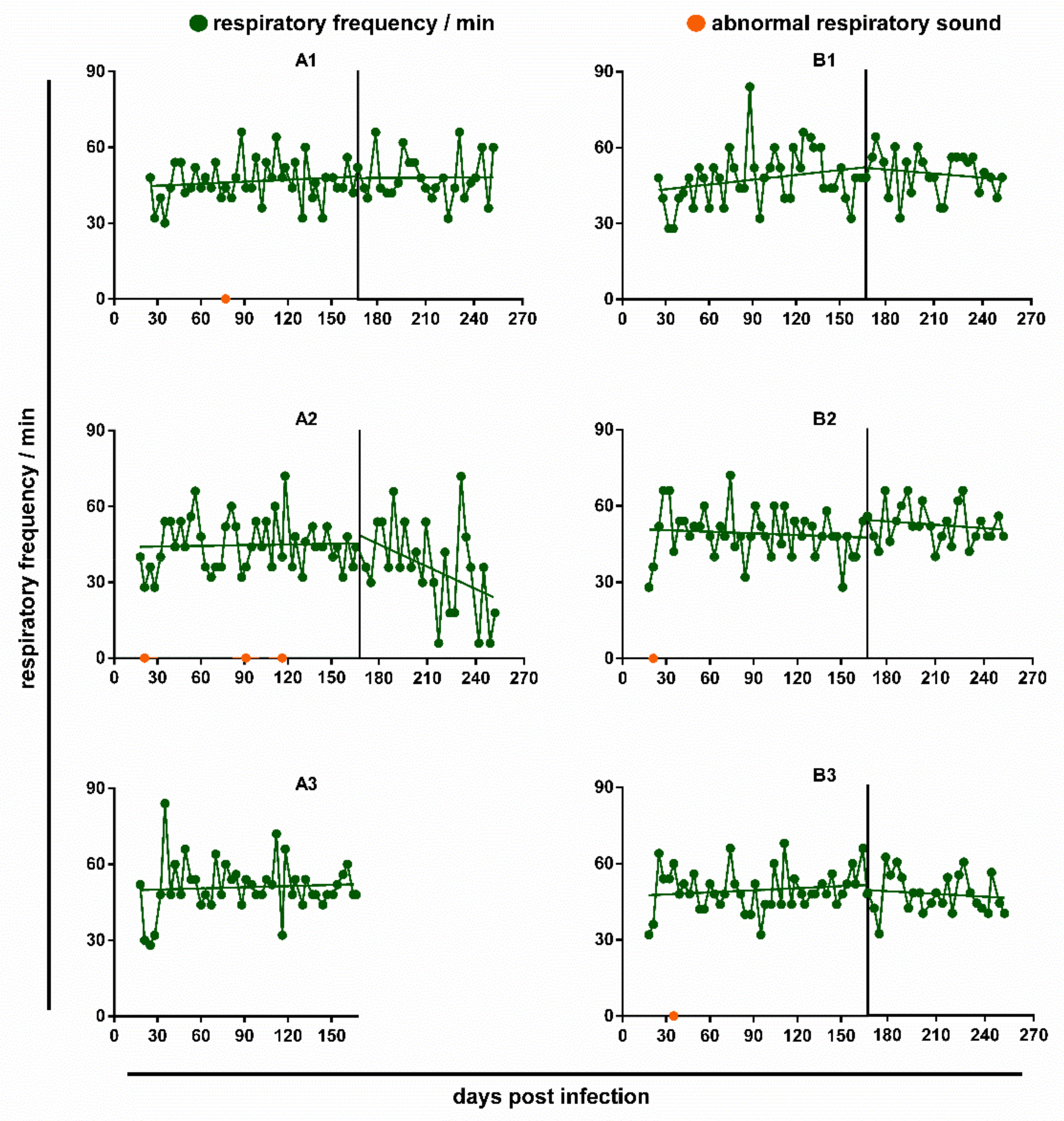
2.3. Respiratory Parameters
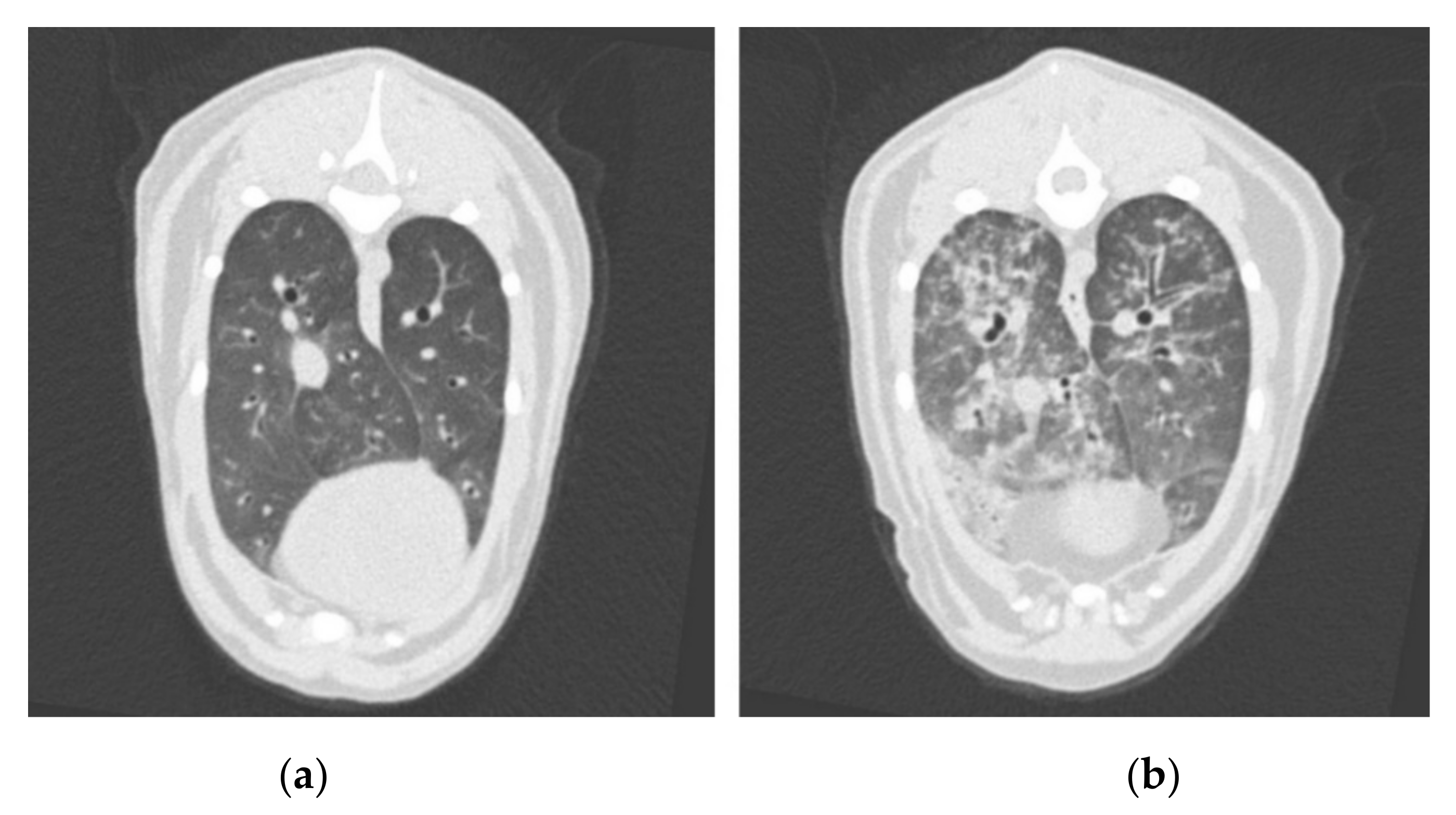
2.4. Computed Tomography
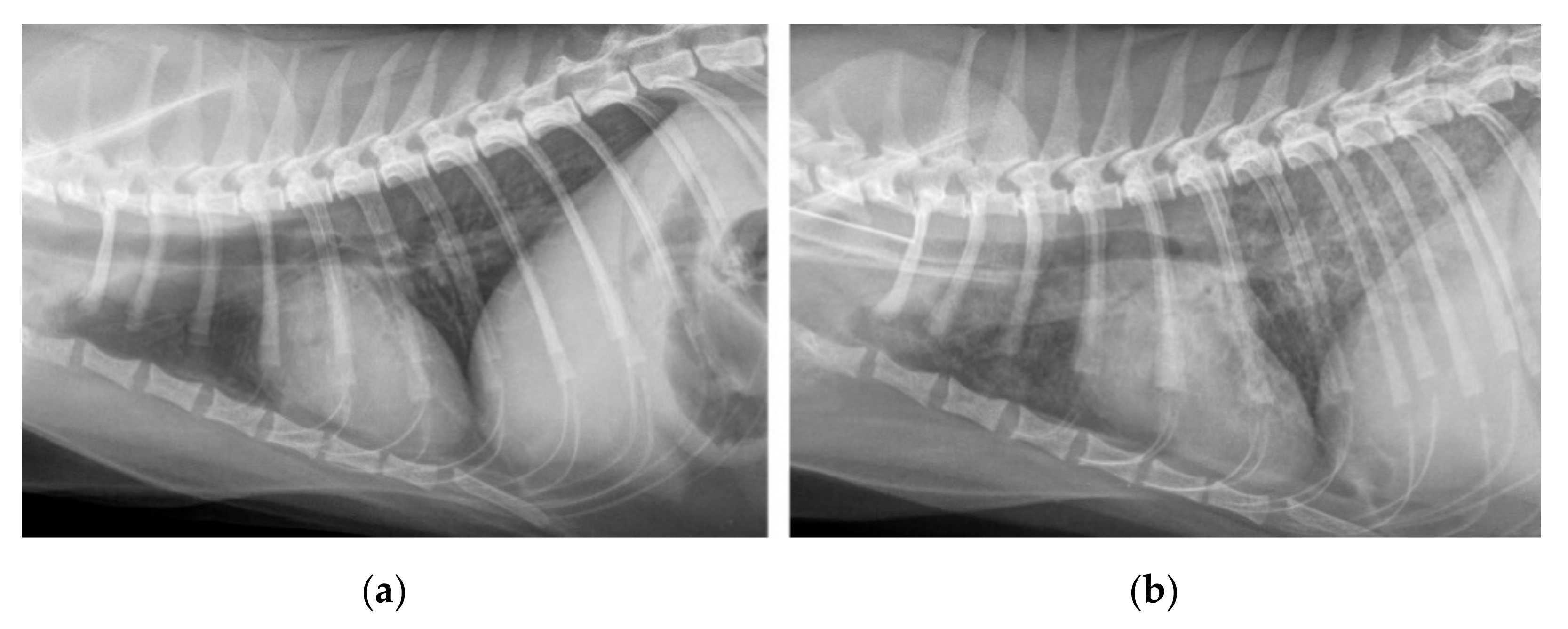
2.5. Radiography
2.6. Post Mortem Nematode Counts
3. Discussion
4. Materials and Methods
4.1. Study Animals
4.2. Infection Material and Experimental Inoculation
4.3. Faecal Larvae Counts
4.4. Respiratory Assessment and General Health Monitoring
4.5. Anti-MSP Antibody ELISA
4.6. Diagnostic Imaging
4.6.1. Anaesthesia
4.6.2. CT Image Acquisition
4.6.3. Radiography
4.6.4. Image Assessment
4.7. Parasitological Necropsy
4.8. Anthelmintic Treatment
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Giannelli, A.; Capelli, G.; Joachim, A.; Hinney, B.; Losson, B.; Kirkova, Z.; Rene-Martellet, M.; Papadopoulos, E.; Farkas, R.; Napoli, E.; et al. Lungworms and gastrointestinal parasites of domestic cats: A European perspective. Int. J. Parasitol. 2017, 47, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Abu-Madi, M.A.; Al-Ahbabi, D.A.; Al-Mashhadani, M.M.; Al-Ibrahim, R.; Pal, P.; Lewis, J.W. Patterns of parasitic infections in faecal samples from stray cat populations in Qatar. J. Helminthol. 2007, 81, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Penagos-Tabares, F.; Lange, M.K.; Chaparro-Gutierrez, J.J.; Taubert, A.; Hermosilla, C. Angiostrongylus vasorum and Aelurostrongylus abstrusus: Neglected and underestimated parasites in South America. Parasites Vectors 2018, 11, 208. [Google Scholar] [CrossRef] [Green Version]
- Carruth, A.J.; Buch, J.S.; Braff, J.C.; Chandrashekar, R.; Bowman, D.D. Distribution of the feline lungworm Aelurostrongylus abstrusus in the USA based on fecal testing. JFMS Open Rep. 2019, 5, 2055116919869053. [Google Scholar] [CrossRef] [PubMed]
- Adams, P.J.; Elliot, A.D.; Algar, D.; Brazell, R.I. Gastrointestinal parasites of feral cats from Christmas Island. Aust. Vet. J. 2008, 86, 60–63. [Google Scholar] [CrossRef]
- Gerichter, C.B. Studies on the nematodes parasitic in the lungs of Felidae in Palestine. Parasitology 1949, 39, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Hobmaier, M.; Hobmaier, A. Zur entwicklung des lungenwurmes der katze Aelurostrongylus abstrusus. Z. Parasitenkd. 1935, 7, 717–718. [Google Scholar] [CrossRef]
- Jezewski, W.; Bunkowska-Gawlik, K.; Hildebrand, J.; Perec-Matysiak, A.; Laskowski, Z. Intermediate and paratenic hosts in the life cycle of Aelurostrongylus abstrusus in natural environment. Vet. Parasitol. 2013, 198, 401–405. [Google Scholar] [CrossRef]
- Mackerras, M. Observations on the life history of the cat Lungworm. Aelurostrongylus abstrusus (Railliet, 1898) (Nematoda: Metastrongylidae). Aust. J. Zool. 1957, 5, 188–195. [Google Scholar] [CrossRef]
- Hobmaier, M.H.; Hobmaier, A. Mammalian phase of the lung-worm Aelurostrongylus abstrusus in the cat. J. Am. Vet. Med. Assoc. 1935, 87, 191–198. [Google Scholar]
- Vezzosi, T.; Perrucci, S.; Parisi, F.; Morelli, S.; Maestrini, M.; Mennuni, G.; Traversa, D.; Poli, A. Fatal pulmonary hypertension and right-sided congestive heart failure in a kitten infected with Aelurostrongylus abstrusus. Animals 2020, 10, 2263. [Google Scholar] [CrossRef]
- Philbey, A.W.; Krause, S.; Jefferies, R. Verminous pneumonia and enteritis due to hyperinfection with Aelurostrongylus abstrusus in a kitten. J. Comp. Pathol. 2014, 150, 357–360. [Google Scholar] [CrossRef]
- Schnyder, M.; di Cesare, A.; Basso, W.; Guscetti, F.; Riond, B.; Glaus, T.; Crisi, P.; Deplazes, P. Clinical, laboratory and pathological findings in cats experimentally infected with Aelurostrongylus abstrusus. Parasitol. Res. 2014, 113, 1425–1433. [Google Scholar] [CrossRef] [PubMed]
- Crisi, P.E.; Aste, G.; Traversa, D.; di Cesare, A.; Febo, E.; Vignoli, M.; Santori, D.; Luciani, A.; Boari, A. Single and mixed feline lungworm infections: Clinical, radiographic and therapeutic features of 26 cases (2013–2015). J. Feline Med. Surg. 2017, 19, 1017–1029. [Google Scholar] [CrossRef]
- Briggs, K.R.; Yaros, J.P.; Liotta, J.L.; Lucio-Forster, A.; Lee, A.C.; Bowman, D.D. Detecting Aelurostrongylus abstrusus-specific IgG antibody using an immunofluorescence assay. J. Feline Med. Surg. 2013, 15, 1114–1118. [Google Scholar] [CrossRef] [PubMed]
- Raue, K.; Rohdich, N.; Hauck, D.; Zschiesche, E.; Morelli, S.; Traversa, D.; di Cesare, A.; Roepke, R.K.A.; Strube, C. Efficacy of Bravecto® Plus spot-on solution for cats (280 mg/mL fluralaner and 14 mg/mL moxidectin) for the prevention of aelurostrongylosis in experimentally infected cats. Parasites Vectors 2021, 14, 110. [Google Scholar] [CrossRef] [PubMed]
- Genchi, M.; Ferrari, N.; Fonti, P.; de Francesco, I.; Piazza, C.; Viglietti, A. Relation between Aelurostrongylus abstrusus larvae excretion, respiratory and radiographic signs in naturally infected cats. Vet. Parasitol. 2014, 206, 182–187. [Google Scholar] [CrossRef]
- Foster, S.F.; Martin, P. Lower respiratory tract infections in cats: Reaching beyond empirical therapy. J. Feline Med. Surg. 2011, 13, 313–332. [Google Scholar] [CrossRef]
- Dennler, M.; Bass, D.A.; Gutierrez-Crespo, B.; Schnyder, M.; Guscetti, F.; di Cesare, A.; Deplazes, P.; Kircher, P.R.; Glaus, T.M. Thoracic computed tomography, angiographic computed tomography, and pathology findings in six cats experimentally infected with Aelurostrongylus abstrusus. Vet. Radiol. Ultrasound 2013, 54, 459–469. [Google Scholar] [CrossRef]
- Lacava, G.; Zini, E.; Marchesotti, F.; Domenech, O.; Romano, F.; Manzocchi, S.; Venco, L.; Auriemma, E. Computed tomography, radiology and echocardiography in cats naturally infected with Aelurostrongylus abstrusus. J. Feline Med. Surg. 2017, 19, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Traversa, D.; di Cesare, A. Diagnosis and management of lungworm infections in cats: Cornerstones, dilemmas and new avenues. J. Feline Med. Surg. 2016, 18, 7–20. [Google Scholar] [CrossRef] [Green Version]
- Traversa, D.; Guglielmini, C. Feline aelurostrongylosis and canine angiostrongylosis: A challenging diagnosis for two emerging verminous pneumonia infections. Vet. Parasitol. 2008, 157, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Abbate, J.M.; Arfuso, F.; Gaglio, G.; Napoli, E.; Cavalera, M.A.; Giannetto, S.; Otranto, D.; Brianti, E. Larval survival of Aelurostrongylus abstrusus lungworm in cat litters. J. Feline Med. Surg. 2019, 21, 992–997. [Google Scholar] [CrossRef]
- Di Cesare, A.; Veronesi, F.; Frangipane di Regalbono, A.F.; Iorio, R.; Traversa, D. Novel molecular assay for simultaneous identification of neglected lungworms and heartworms affecting cats. J. Clin. Microbiol. 2015, 53, 3009–3013. [Google Scholar] [CrossRef] [Green Version]
- Traversa, D.; di Cesare, A.; Milillo, P.; Iorio, R.; Otranto, D. Aelurostrongylus abstrusus in a feline colony from central Italy: Clinical features, diagnostic procedures and molecular characterization. Parasitol. Res. 2008, 103, 1191–1196. [Google Scholar] [CrossRef]
- Morelli, S.; Diakou, A.; Colombo, M.; di Cesare, A.; Barlaam, A.; Dimzas, D.; Traversa, D. Cat respiratory nematodes: Current knowledge, novel data and warranted studies on clinical features, treatment and control. Pathogens 2021, 10, 454. [Google Scholar] [CrossRef]
- Traversa, D.; Iorio, R.; Otranto, D. Diagnostic and clinical implications of a nested PCR specific for ribosomal DNA of the feline lungworm Aelurostrongylus abstrusus (Nematoda, Strongylida). J. Clin. Microbiol. 2008, 46, 1811–1817. [Google Scholar] [CrossRef] [Green Version]
- Zottler, E.M.; Strube, C.; Schnyder, M. Detection of specific antibodies in cats infected with the lung nematode Aelurostrongylus abstrusus. Vet. Parasitol. 2017, 235, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Holtum, C.; Strube, C.; Schnieder, T.; von Samson-Himmelstjerna, G. Development and evaluation of a recombinant antigen-based ELISA for serodiagnosis of cattle lungworm. Vet. Parasitol. 2008, 151, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Cavalera, M.A.; Schnyder, M.; Gueldner, E.K.; Furlanello, T.; Iatta, R.; Brianti, E.; Strube, C.; Colella, V.; Otranto, D. Serological survey and risk factors of Aelurostrongylus abstrusus infection among owned cats in Italy. Parasitol. Res. 2019, 118, 2377–2382. [Google Scholar] [CrossRef] [PubMed]
- Di Cesare, A.; Gueldner, E.K.; Traversa, D.; Veronesi, F.; Morelli, S.; Crisi, P.E.; Pampurini, F.; Strube, C.; Schnyder, M. Seroprevalence of antibodies against the cat lungworm Aelurostrongylus abstrusus in cats from endemic areas of Italy. Vet. Parasitol. 2019, 272, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Gueldner, E.K.; Gilli, U.; Strube, C.; Schnyder, M. Seroprevalence, biogeographic distribution and risk factors for Aelurostrongylus abstrusus infections in Swiss cats. Vet. Parasitol. 2019, 266, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Morelli, S.; Diakou, A.; di Cesare, A.; Schnyder, M.; Colombo, M.; Strube, C.; Dimzas, D.; Latino, R.; Traversa, D. Feline lungworms in Greece: Copromicroscopic, molecular and serological study. Parasitol. Res. 2020, 119, 2877–2883. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, J.M. The influence of infestation by Aelurostrongylus abstrusus on the pulmonary vasculature of the cat. Br. Vet. J. 1970, 126, 202–209. [Google Scholar] [CrossRef]
- Gerdin, J.A.; Slater, M.R.; Makolinski, K.V.; Looney, A.L.; Appel, L.D.; Martin, N.M.; McDonough, S.P. Post-mortem findings in 54 cases of anesthetic associated death in cats from two spay-neuter programs in New York State. J. Feline Med. Surg. 2011, 13, 959–966. [Google Scholar] [CrossRef]
- Heuer, L.; Petry, G.; Pollmeier, M.; Schaper, R.; Deuster, K.; Schmidt, H.; Blazejak, K.; Strube, C.; di Cesare, A.; Traversa, D.; et al. Efficacy of imidacloprid 10%/moxidectin 1% spot-on formulation (Advocate®) in the prevention and treatment of feline aelurostrongylosis. Parasites Vectors 2020, 13, 65. [Google Scholar] [CrossRef]
- Böhm, C.; Wolken, S.; Schnyder, M.; Basso, W.; Deplazes, P.; di Cesare, A.; Deuster, K.; Schaper, R. Efficacy of emodepside/praziquantel spot-on (Profender®) against adult Aelurostrongylus abstrusus nematodes in experimentally infected cats. Parasitol. Res. 2015, 114, 155–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stockdale, P.H. The pathogenesis of the lesions elicited by Aelurostrongylus abstrusus during its prepatent period. Pathol. Vet. 1970, 7, 102–115. [Google Scholar] [CrossRef] [PubMed]
- Losonsky, J.M.; Thrall, D.E.; Prestwood, A.K. Radiographic evaluation of pulmonary abnormalities after Aelurostrongylus abstrusus inoculation in cats. Am. J. Vet. Res. 1983, 44, 478–482. [Google Scholar]
- Foster, S.F.; Allan, G.S.; Martin, P.; Robertson, I.D.; Malik, R. Twenty-five cases of feline bronchial disease (1995–2000). J. Feline Med. Surg. 2004, 6, 181–188. [Google Scholar] [CrossRef]
- Febo, E.; Crisi, P.E.; Traversa, D.; Luciani, A.; di Tommaso, M.; Pantaleo, S.; Santori, D.; di Cesare, A.; Boari, A.; Terragni, R.; et al. Comparison of clinical and imaging findings in cats with single and mixed lungworm infection. J. Feline Med. Surg. 2019, 21, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Prather, A.B.; Berry, C.R.; Thrall, D.E. Use of radiography in combination with computed tomography for the assessment of noncardiac thoracic disease in the dog and cat. Vet. Radiol. Ultrasound 2005, 46, 114–121. [Google Scholar] [CrossRef]
- Nemanic, S.; London, C.A.; Wisner, E.R. Comparison of thoracic radiographs and single breath-hold helical CT for detection of pulmonary nodules in dogs with metastatic neoplasia. J. Vet. Intern. Med. 2006, 20, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Armbrust, L.J.; Biller, D.S.; Bamford, A.; Chun, R.; Garrett, L.D.; Sanderson, M.W. Comparison of three-view thoracic radiography and computed tomography for detection of pulmonary nodules in dogs with neoplasia. J. Am. Vet. Med. Assoc. 2012, 240, 1088–1094. [Google Scholar] [CrossRef] [PubMed]
- Coia, M.E.; Hammond, G.; Chan, D.; Drees, R.; Walker, D.; Murtagh, K.; Stone, J.; Bexfield, N.; Reeve, L.; Helm, J. Retrospective evaluation of thoracic computed tomography findings in dogs naturally infected by Angiostrongylus vasorum. Vet. Radiol. Ultrasound 2017, 58, 524–534. [Google Scholar] [CrossRef] [Green Version]
- Ray Dillon, A.; Tillson, D.M.; Wooldridge, A.; Cattley, R.; Hathcock, J.; Brawner, W.R.; Cole, R.; Welles, B.; Christopherson, P.W.; Lee-Fowler, T.; et al. Effect of pre-cardiac and adult stages of Dirofilaria immitis in pulmonary disease of cats: CBC, bronchial lavage cytology, serology, radiographs, CT images, bronchial reactivity, and histopathology. Vet. Parasitol. 2014, 206, 24–37. [Google Scholar] [CrossRef] [Green Version]
- Dillon, A.R.; Tillson, D.M.; Hathcock, J.; Brawner, B.; Wooldridge, A.; Cattley, R.; Welles, B.; Barney, S.; Lee-Fowler, T.; Botzman, L.; et al. Lung histopathology, radiography, high-resolution computed tomography, and bronchio-alveolar lavage cytology are altered by Toxocara cati infection in cats and is independent of development of adult intestinal parasites. Vet. Parasitol. 2013, 193, 413–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicines Agency. VICH Guideline 7: Efficacy of Anthelmintics: General Requirements. Veterinary International Cooperation on Harmonization; CVMP/VICH/832/99-corr.; European Agency for the Evaluation of Medicinal Products: London, UK, 2000.
- European Medicines Agency. VICH Guideline 20: Efficacy of Anthelmintics: Specific Recommendations for Felines. Veterinary International Cooperation on Harmonization; CVMP/VICH/545/00-Final; European Agency for the Evaluation of Medicinal Products: London, UK, 2001.
- Jacobs, D.E.; Arakawa, A.; Courtney, C.H.; Gemmell, M.A.; McCall, J.W.; Myers, G.H.; Vanparijs, O. World Association for the Advancement of Veterinary Parasitology (W.A.A.V.P.) guidelines for evaluating the efficacy of anthelmintics for dogs and cats. Vet. Parasitol. 1994, 52, 179–202. [Google Scholar] [CrossRef]
- Traversa, D.; Joachim, A. The 3Rs concept: Time to change how we evaluate the efficacy of anthelmintics in companion animals. Trends Parasitol. 2018, 34, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Di Cesare, A.; Crisi, P.E.; di Giulio, E.; Veronesi, F.; Frangipane di Regalbono, A.F.; Talone, T.; Traversa, D. Larval development of the feline lungworm Aelurostrongylus abstrusus in Helix aspersa. Parasitol. Res. 2013, 112, 3101–3108. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cat | Imaging Modality | Week Post Infection | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | 12 | 18/19th | 25th * | 30th/31th | 36th/37th | 42 | 48th | ||
| A1 | CT | 0 | 3 | 2 | 2 | 0 | |||
| XRAY | 0 | 7 | 6 | 5 | 1 | ||||
| A2 | CT | 0 | 2 | 3 | 3 | 1 | 0 | ||
| XRAY | 1 | 4 | 4 | 4 | 1 | 0 | |||
| A3 | CT | 0 | 3 | 3 | |||||
| XRAY | 0 | 5 | 4 | ||||||
| B1 | CT | 0 | 3 | 2 | 3 | 1 | 0 | ||
| XRAY | 0 | 5 | 3 | 5 | 2 | 0 | |||
| B2 | CT | 0 | 2 | 3 | 2 | 1 | 0 | ||
| XRAY | 0 | 5 | 5 | 2 | 0 | 0 | |||
| B3 | CT | 0 | 3 | 2 | 2 | 1 | 1 | 1 | 0 |
| XRAY | 0 | 5 | 3 | 3 | 2 | 1 | 0 | 0 | |
| CT Lung Severity Score | Imaging Features |
|---|---|
| 0 = normal | No changes |
| 1 = mild | Some or all zones affected, some areas of ground-glass opacity, only occasional nodules or consolidated areas, mild reticular and/or mosaic pattern, no or mild bronchial wall thickening, no lymph node enlargement |
| 2 = moderate | All zones affected, some or multiple areas of ground-glass opacity, multiple or all lobes affected, occasional consolidated areas, no or some nodules, moderate reticular and/or mosaic pattern, bronchial wall thickening, partial loss of visual separation between bronchial walls and peribronchial vessels, enlarged lymph nodes |
| 3 = severe | All zones affected, multiple nodules or general nodular pattern, multiple consolidated areas, severe reticular and/or mosaic pattern bronchial wall thickening, marked ground-glass opacity, loss of visual separation between bronchial walls and peribronchial vessels, enlarged lymph nodes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raue, K.; Raue, J.; Hauck, D.; Söbbeler, F.; Morelli, S.; Traversa, D.; Schnyder, M.; Volk, H.; Strube, C. Do All Roads Lead to Rome? The Potential of Different Approaches to Diagnose Aelurostrongylus abstrusus Infection in Cats. Pathogens 2021, 10, 602. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10050602
Raue K, Raue J, Hauck D, Söbbeler F, Morelli S, Traversa D, Schnyder M, Volk H, Strube C. Do All Roads Lead to Rome? The Potential of Different Approaches to Diagnose Aelurostrongylus abstrusus Infection in Cats. Pathogens. 2021; 10(5):602. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10050602
Chicago/Turabian StyleRaue, Katharina, Jonathan Raue, Daniela Hauck, Franz Söbbeler, Simone Morelli, Donato Traversa, Manuela Schnyder, Holger Volk, and Christina Strube. 2021. "Do All Roads Lead to Rome? The Potential of Different Approaches to Diagnose Aelurostrongylus abstrusus Infection in Cats" Pathogens 10, no. 5: 602. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10050602