
High Incidence of Congenital Syphilis after Implementation of the Brazilian Ministry of Health Ordinances Related to Maternal Diagnostics

 and
and
Abstract
:1. Introduction
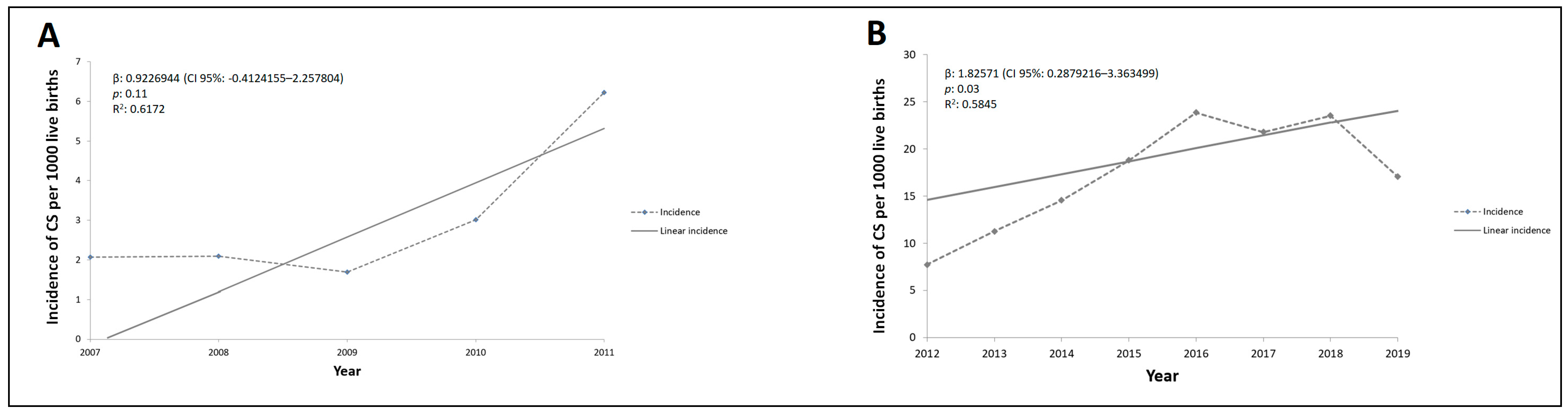
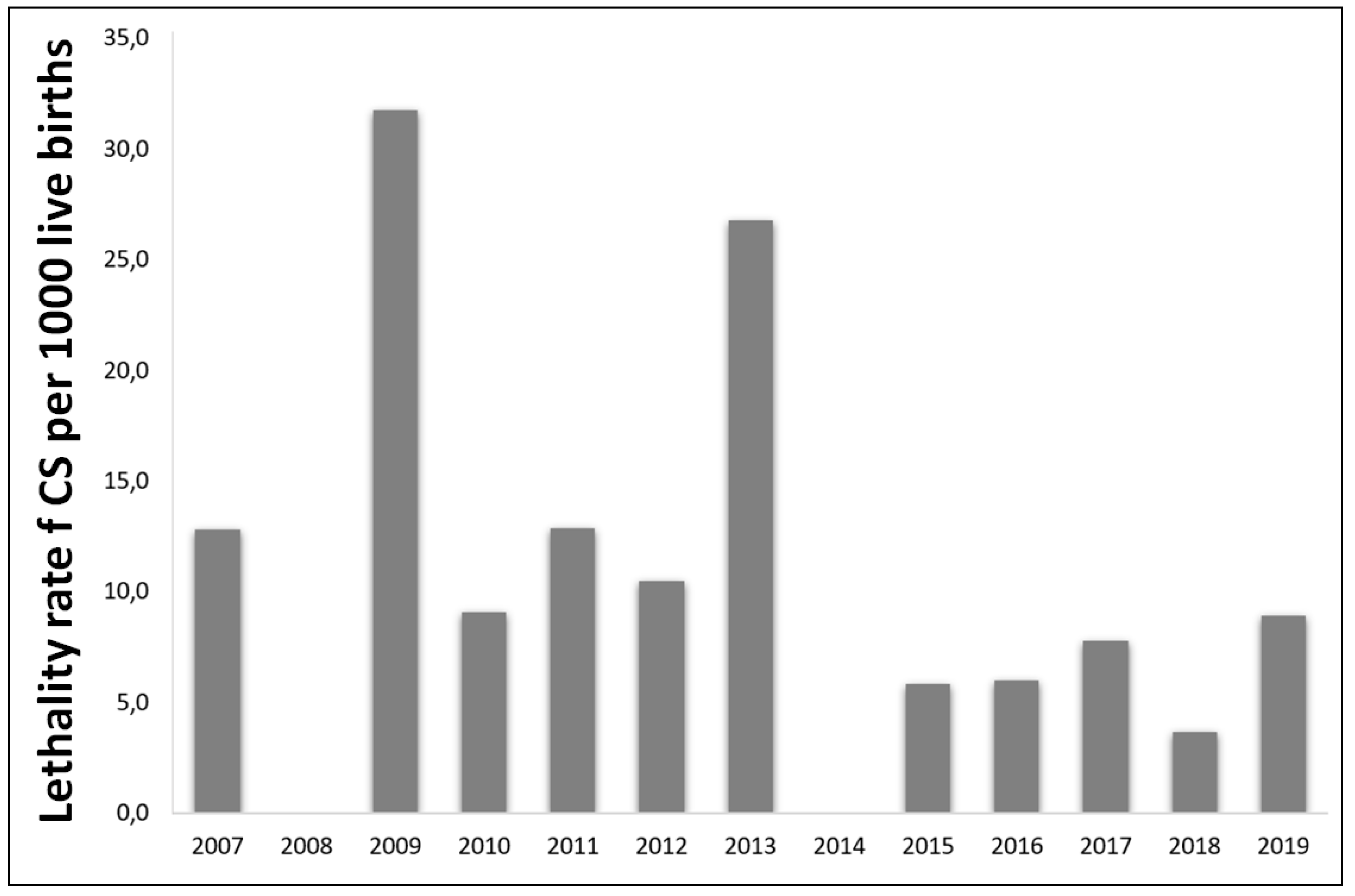
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Design and Population
4.2. Data Analysis
4.3. Ethical Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Korenromp, E.L.; Rowley, J.; Alonso, M.; Mello, M.B.; Wijesooriya, N.S.; Mahiané, S.G.; Ishikawa, N.; Le, L.V.; Newman-Owiredu, M.; Nagelkerke, N.; et al. Global burden of maternal and congenital syphilis and associated adverse birth outcomes—Estimates for 2016 and progress since 2012. PLoS ONE 2019, 14, e0211720. [Google Scholar]
- Cooper, J.M.; Michelow, I.C.; Wozniak, P.S.; Sánchez, P.J. In time: The persistence of congenital syphilis in Brazil—More progress needed! Rev Paul Pediatr. 2016, 34, 251–253. (In Portuguese) [Google Scholar] [CrossRef]
- Hopkins, A.O.; Trinh, T.; Fakile, Y.F.; Pillay, A.; Taylor, M.M.; Kersh, E.; Kamb, M. Evaluation of the WHO/CDC Syphilis Serology Proficiency Programme to support the global elimination of mother-to-child transmission of syphilis: An observational cross-sectional study, 2008–2015. BMJ Open 2020, 10, e029434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez, G.B.; Kamb, M.L.; Newman, L.M.; Mark, J.; Broutet, N.; Hawkes, S.J. Untreated maternal syphilis and adverse outcomes of pregnancy: A systematic review and meta-analysis. Bull. World Health Organ. 2013, 91, 217–226. [Google Scholar] [CrossRef]
- Trinh, T.; Kamb, M.L.; Luu, M.; Ham, D.C.; Perez, F. Syphilis Testing Practices in the Americas. Trop. Med. Int. Health 2017, 12, 3218–3221. [Google Scholar] [CrossRef]
- Avelleira, J.C.R.; Bottino, G. Syphilis: Diagnosis, treatment and control. An. Bras. Dermatol. 2006, 81, 111–126. [Google Scholar] [CrossRef]
- Cooper, J.M.; Sánchez, P.J. Congenital syphilis. Semin Perinatol. 2018, 42, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, L.R.P.; Monteiro, D.L.M.; Taquette, S.R.; Rodrigues, N.C.P.; Trajano, A.J.B.; Souza, F.M.; Araújo, B.M. The magnitude of syphilis: From prevalence to vertical transmission. Rev. Inst. Med. Trop. Sao Paulo 2017, 59, e78. [Google Scholar] [CrossRef] [Green Version]
- Brasil Secretaria de Vigilância em Saúde. Ministério da Saúde. Boletim Epidemiológico: Sífilis 2017. In Ministério da Saúde; 2017; Volume 48, p. 41. Available online: http://www.aids.gov.br/pt-br/pub/2017/boletim-epidemiologico-de-sifilis-2017 (accessed on 3 August 2020).
- Brasil Secretaria de Vigilância em Saúde. Ministério da Saúde. Boletim Epidemiológico: Sífilis 2018. In Ministério da Saúde; 2018; Volume 49, pp. 1–43. Available online: http://www.aids.gov.br/pt-br/pub/2018/boletim-epidemiologico-de-sifilis-2018 (accessed on 3 August 2020).
- Brazil Ministry of Health. Ordinance no. 3.242, 30 December 2011. Fluxograma Laboratorial da Sífilis, Utilização de Testes Rápidos Para Triagem da Sífilis em Situações Especiais e Outras Recomendações. Available online: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2011/prt3242_30_12_2011.html (accessed on 3 August 2020). (In Portuguese)
- Brazil Ministry of Health. Ordinance no. 77, 12 January 2012. Dispõe Sobre a Realização de Testes Rápidos, na Atenção Básica, Para a Detecção de HIV e Sífilis, Assim Como Testes Rápidos Para Outros Agravos, no Âmbito da Atenção Pré-Natal Para Gestantes e Suas Parcerias Sexuais. Available online: http://bvsms.saude.gov.br/bvs/saudelegis/sas/2012/prt1126_08_10_2012.html (accessed on 3 August 2020). (In Portuguese)
- Bezerra, M.L.M.B.; Fernandes, F.E.C.V.; Nunes, J.P.O.; de Araújo Baltar, S.L.S.M.; Randau, K.P. Congenital Syphilis as a Measure of Maternal and Child Healthcare, Brazil. Emerg. Infect. Dis. 2019, 25, 1469–1476. [Google Scholar] [CrossRef]
- Moreira, K.F.A.; Oliveira, D.M.; Alencar, L.N.; Cavalcante, D.F.B.; Pinheiro, A.S.; Orfão, N.H. Profile of Notified Cases of Congenital Syphilis. Cogitare Enferm. 2017, 22, e48949. [Google Scholar]
- Teixeira, M.A.; Santos, P.P.; Santos, P.N.; Santos, M.R.; Menezes, A.M.F.; Alves, K.A.N. Epidemiological and Soci-odemographic Profile of Children Infected Congenital Syphilis in Jequié/Bahia. Rev. Saude Com. 2015, 11, 303–313. [Google Scholar]
- Magalhães, D.M.S.; Kawaguchi, I.A.L.; Dias, A.; Calderon, I.M.P. Sífilis materna e congênita: Ainda um desafio. Cad Saude Publica 2013, 29, 1109–1120. [Google Scholar] [CrossRef] [Green Version]
- Brasil Ministério da Saúde. Rede Cegonha. Portaria GM/MS nº 2.351/2011. Available online: https://aps.saude.gov.br/ape/cegonha (accessed on 3 August 2020).
- Lima, V.C.; Mororó, R.M.; Martins, M.A.; Ribeiro, S.M.; Linhares, M.S.C. Perfil epidemiológico dos casos de sífilis congênita em um município de médio porte no nordeste brasileiro. J. Health Biol. Sci. 2017, 5, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Domingues, R.M.S.M.; Leal, M.C. Incidência de sífilis congênita e fatores associados à transmissão vertical da sífilis: Dados do estudo Nascer no Brasil. Cad. Saude Publica 2016, 32, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saraceni, V.; Pereira, G.F.M.; Araújo, M.A.L.; Miranda, A.E. Vigilância epidemiológica da transmissão vertical da sífilis: Dados de seis unidades federativas no Brasil. Rev. Panam. Salud Publica 2017, 41, e44. [Google Scholar]
- Silva, H.C.G.; Sousa, T.O.; Sakae, T.M. Incidência de Sífilis Congênita no Estado de Santa Catarina no Ano de 2012. Arq. Catarin. Med. 2017, 46, 15–25. [Google Scholar]
- Oliveira, J.S.; Santos, J.V. Perfil Epidemiológico da Sífilis Congênita no Estado da Bahia, no período de 2010 a 2013. Rev. Eletrôn. Atualiza Saúde 2015, 2, 20–30. [Google Scholar]
- Cavalcante, P.A.M.; Pereira, R.B.L.; Castro, J.G.D. Syphilis in pregnancy and congenital syphilis in Palmas, Tocantins State, Brazil, 2007–2014*. Epidemiol. Serv. Saude 2017, 26, 255–264. [Google Scholar] [CrossRef]
- Swartzendruber, A.; Steiner, R.J.; Adler, M.R.; Kamb, M.L.; Newman, L.M. Introduction of rapid syphilis testing in antenatal care: A systematic review of the impact on HIV and syphilis testing uptake and coverage. Int. J. Gynecol. Obstet. 2015, 130, S15–S21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montoya, P.J.; Lukehart, S.A.; Brentlinger, P.E.; Blanco, A.J.; Floriano, F.; Sairosse, J.; Gloyd, S. Comparison of the diagnostic accuracy of a rapid immunochromatographic test and the rapid plasma reagin test for antenatal syphilis screening in Mozambique. Bull. World Health Organ. 2006, 84, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Peeling, R.W.; Ye, H. Diagnostic tools for preventing and managing maternal and congenital syphilis: An overview. Bull. World Health Organ. 2004, 82, 439–446. [Google Scholar] [PubMed]
- Brasil Ministério da Saúde. Orientações Sobre o Tratamento de Sífilis Congênita e Neurossífilis Em Recém-Nascidos Somente na Indisponibilidade De Penicilina G Cristalina ou Potássica. Nota Informativa n. 68, de 19 de Agosto de 2016. Available online: http://www.aids.gov.br/sites/default/files/legislacao/2016/-notas_informativas/nota_da_compra_penicilina_benzatina_pdf_11355.pdf (accessed on 3 August 2020). (In Portuguese)
- Brazil Ministry of Health. Censos (1980, 1991, 2000 e 2010), Contagem (1996) e Projeções Intercensitárias (1981 a 2012), Segundo Faixa Etária, Sexo e Situação de Domicílio; Health Surveillance: Brasília, Brazil, 2012. Available online: www2.datasus.gov.br/DATASUS/index.php?area=0206&id=6942&VObj=http://tabnet.datasus.gov.br/cgi/deftohtm.exe?ibge/cnv/pop (accessed on 3 August 2020). (In Portuguese)




{kind=link}
{kind=link}
{kind=link}
| Demographics | Total Cases * | Pre-Resolution Era (2007–2011) n (%) ** | Post-Resolution Era (2012–2019) n (%) ** | p Value † |
|---|---|---|---|---|
| Newborns’ gender | 5470 | 444 | 4481 | |
| Female | 2540 | 211 (47.5) | 2329 (52.0) | 0.07 |
| Male | 2385 | 233 (52.5) | 2152 (48.0) | |
| Newborns’ age | 5469 | 556 | 4830 | |
| ≤ 6 days of life | 5228 | 534 (96.0) | 4694 (97.2) | 0.09 |
| ≥ 7 days of life | 153 | 22 (4.0) | 131 (2.7) | |
| Newborns’ skin color | 3631 | 254 | 3377 | |
| Non-black and/or non-mixed | 159 | 14 (5.5) | 145 (4.3) | 0.07 |
| Black | 495 | 49 (19.3) | 446 (13.2) | |
| Mixed | 2977 | 191 (75.2) | 2786 (82.5) | |
| Mother’s education level | 3045 | 287 | 2758 | |
| Never studied | 39 | 12 (4.2) | 27 (1.0) | 0.004 |
| ≤ 5 years | 1757 | 203 (70.7) | 1554 (56.3) | |
| ≥ 6 years | 1249 | 72 (25.1) | 1177 (42.7) |
| Factors | Total Cases * n (%) | Pre-Resolution Era (2007–2011) n (%) ** | Post-Resolution Era (2012–2019) n (%) ** | p Value |
|---|---|---|---|---|
| Attended prenatal care | 4434 | 396 | 4038 | |
| Yes | 3537 | 247 (62.4) | 3290 (81.5) | <0.0001 † |
| No | 897 | 149 (37.6) | 748 (18.5) | |
| Mothers’ diagnosis | 4811 | 441 | 4370 | |
| Prenatal | 2623 | 154 (34.9) | 2469 (56.5) | <0.0001 † |
| During delivery | 1723 | 193 (43.7) | 1530 (35.0) | |
| After delivery | 431 | 85 (19.3) | 346 (7.9) | |
| Non-realized | 34 | 9 (2.0) | 25 (0.6) | |
| Final diagnosis | 5024 | 488 | 4536 | |
| Early CS | 3945 | 404 (82.8) | 3541 (78.0) | <0.0001 ‡ |
| Late CS | 8 | 2 (0.4) | 6 (0.1) | |
| Abortion | 9 | 2 (0.4) | 7 (0.1) | |
| Stillbirth | 68 | 35 (7.2) | 33 (0.7) | |
| Inconclusive | 994 | 45 (9.2) | 949 (20.9) | |
| Newborns’ CS outcome | 4596 | 434 | 4162 | |
| Alive | 4528 | 424 (97.7) | 4104 (98.6) | 0.13 † |
| Died due to syphilis | 44 | 7 (1.6) | 37 (0.9) | |
| Died from other causes | 24 | 3 (0.7) | 21 (0.5) | |
| Partners’ treatment | 4236 | 331 | 3807 | |
| Yes | 2646 | 114 (34.4) | 2512 (66.0) | <0.0001 † |
| No | 1590 | 217 (65.6) | 1295 (34.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veras, Í.S.; Feitosa, C.A.; de Souza, A.J.; Campos, L.C.; Barbosa Costa, G.; Ferreira, V.M. High Incidence of Congenital Syphilis after Implementation of the Brazilian Ministry of Health Ordinances Related to Maternal Diagnostics. Pathogens 2021, 10, 606. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10050606
Veras ÍS, Feitosa CA, de Souza AJ, Campos LC, Barbosa Costa G, Ferreira VM. High Incidence of Congenital Syphilis after Implementation of the Brazilian Ministry of Health Ordinances Related to Maternal Diagnostics. Pathogens. 2021; 10(5):606. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10050606
Chicago/Turabian StyleVeras, Ítala Santos, Caroline Alves Feitosa, Amâncio José de Souza, Leila Carvalho Campos, Galileu Barbosa Costa, and Viviane Matos Ferreira. 2021. "High Incidence of Congenital Syphilis after Implementation of the Brazilian Ministry of Health Ordinances Related to Maternal Diagnostics" Pathogens 10, no. 5: 606. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10050606