
Acute Inflammatory Mediators in Young Adult Patients with COVID-19 in Mexico

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Results
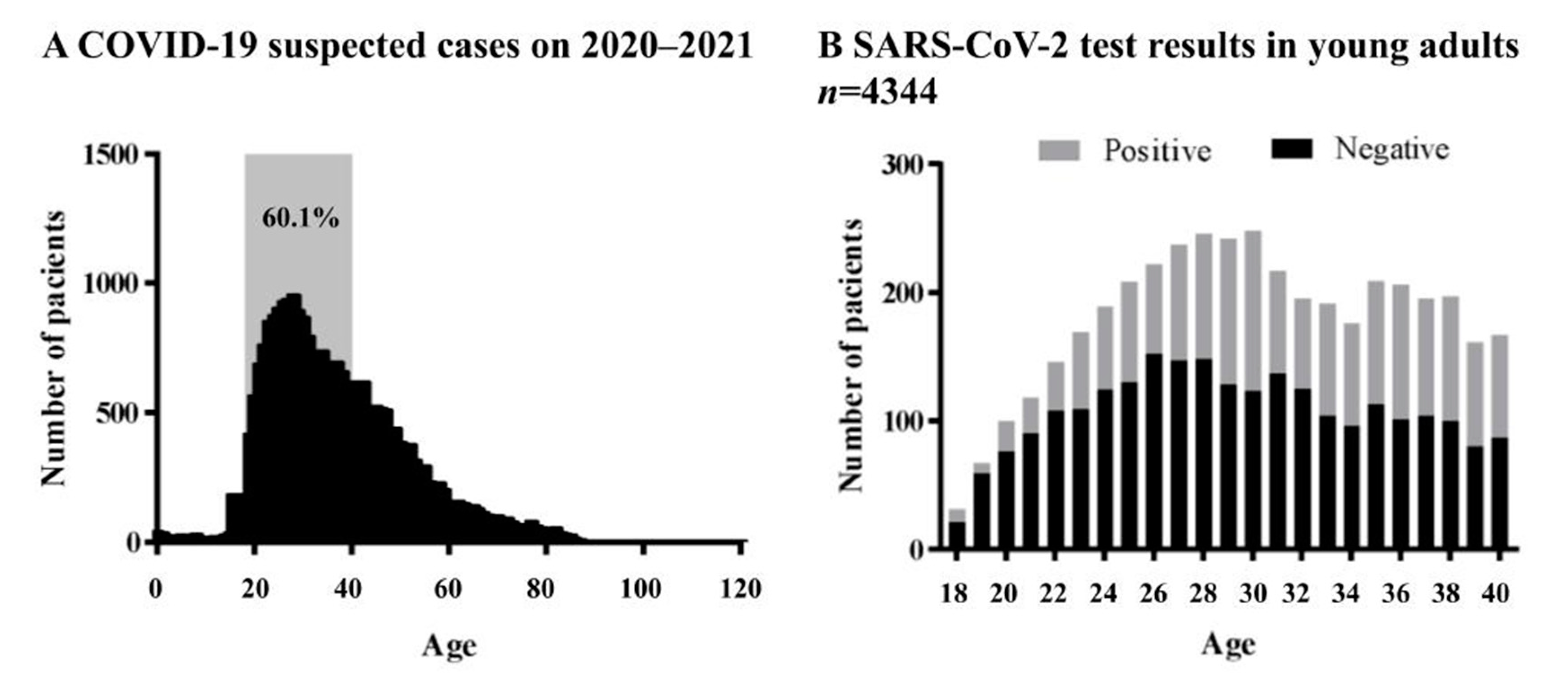
2.1. Epidemiological Results
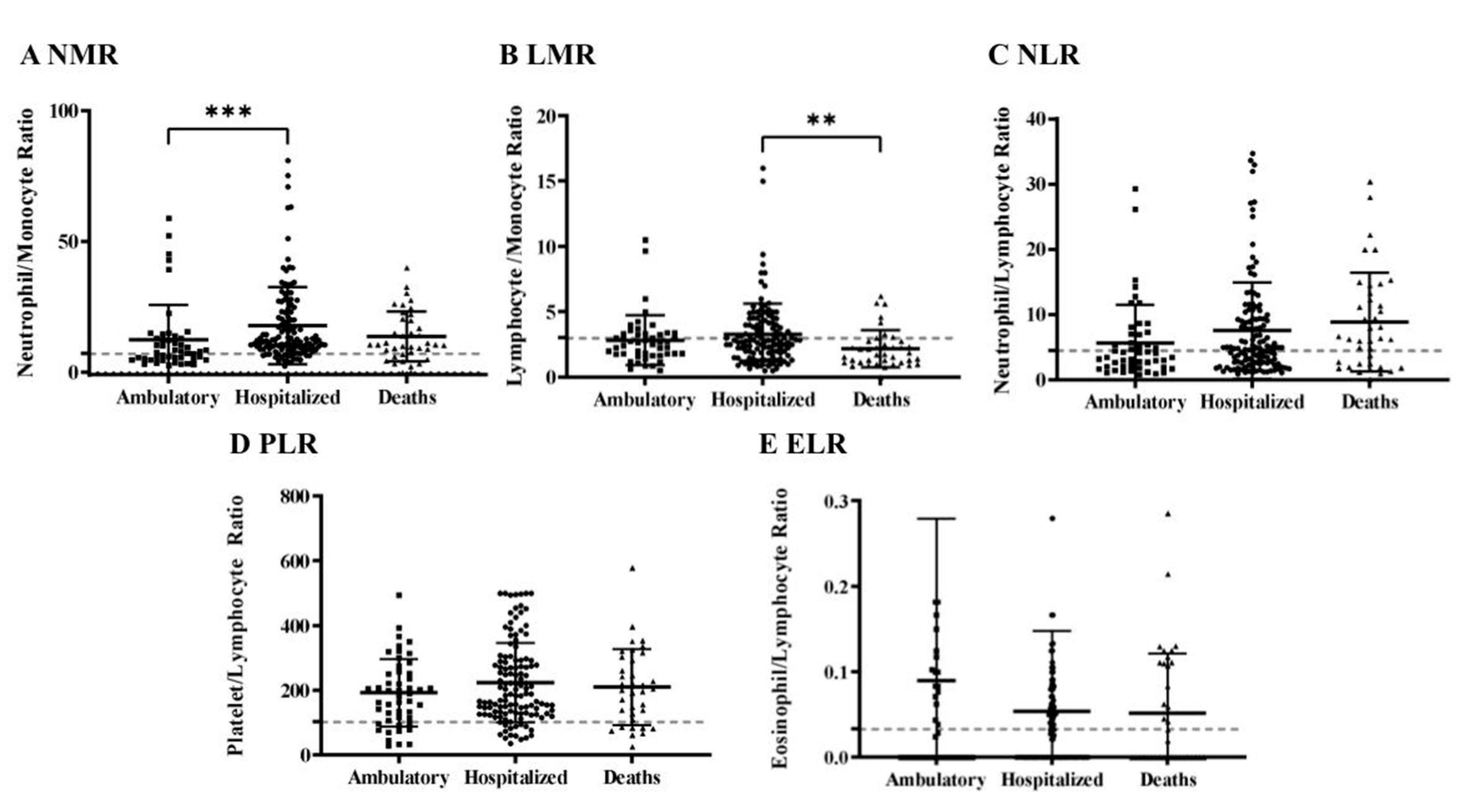
2.2. Acute Inflammatory Mediators
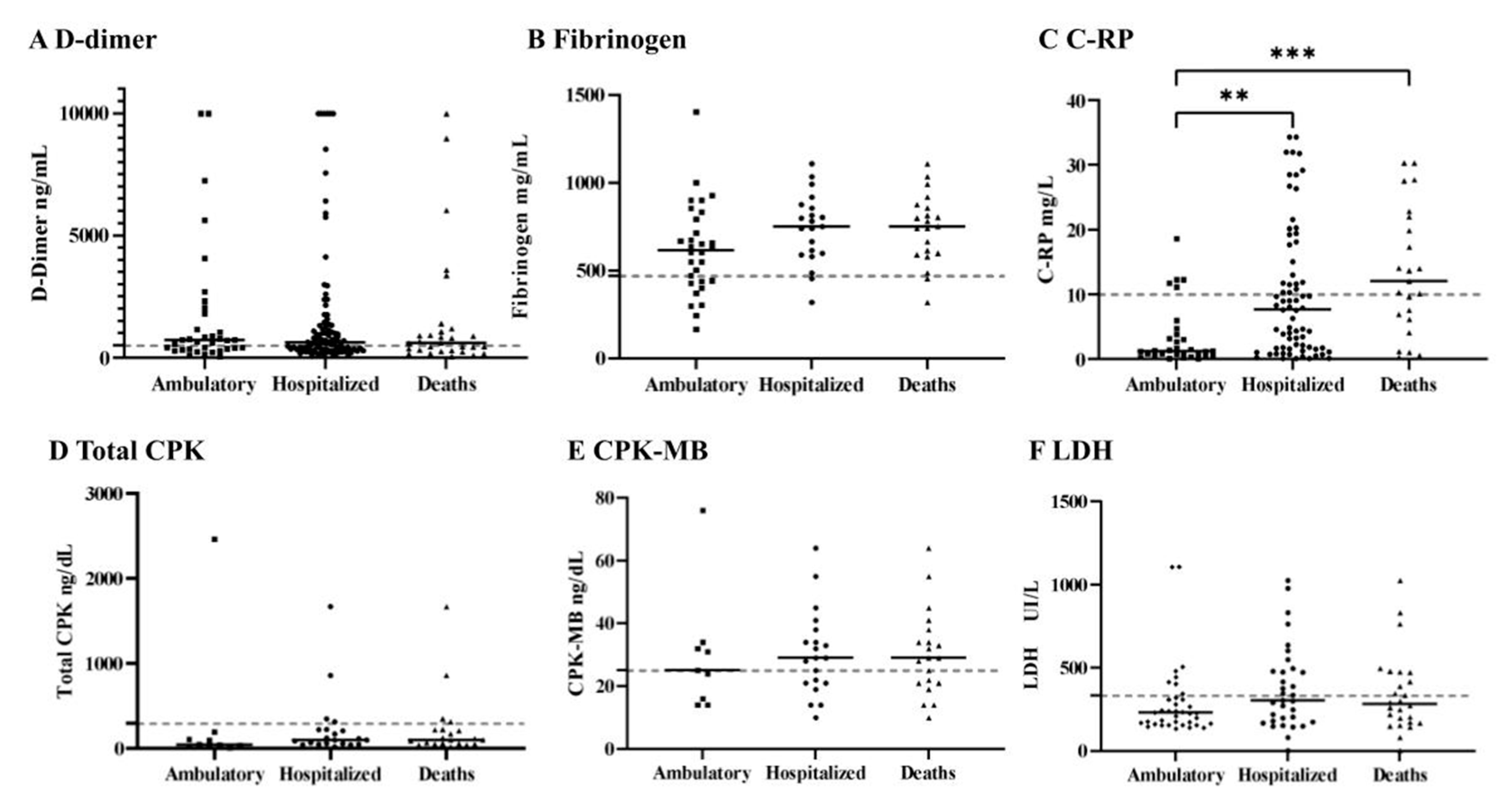
2.3. Coagulopathy Alterations
3. Discussion
4. Materials and Methods
4.1. Data Sources
4.2. Exposure Variable
4.3. Outcome Measures
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Sun, S.; Cai, X.; Wang, H.; He, G.; Lin, Y.; Lu, B.; Chen, C.; Pan, Y.; Hu, X. Abnormalities of peripheral blood system in patients with COVID-19 in Wenzhou, China. Clin. Chim. Acta 2020, 507, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Warkentin, T.E.; Thachil, J.; Levi, M.; Levy, J.H. Proposal of the Definition for COVID-19-Associated Coagulopathy. J. Clin. Med. 2021, 10, 191. [Google Scholar] [CrossRef]
- Levi, M.; Iba, T. COVID-19 coagulopathy: Is it disseminated intravascular coagulation? Intern. Emerg. Med. 2021, 16, 309–312. [Google Scholar] [CrossRef]
- Asakura, H.; Ogawa, H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int. J. Hematol. 2021, 113, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, T.; Chaudhuri, R.; Joshi, M.C.; Almatroudi, A.; Rahmani, A.H.; Ali, S.M. COVID-19: The Emerging Immunopathological Determinants for Recovery or Death. Front. Microbiol. 2020, 11, 58840. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Reyes Morales, H.; Hernández Serrato, M.I.; Gutiérrez Reyes, J.P. Condiciones de salud. In Utilización de Servicios de Salud Encuesta Nacional de Salud y Nutrición 2018–2019; Resultados Nacionales: Cuernavaca, Mexico, 2020; pp. 126–158. [Google Scholar]
- Cunningham, J.W.; Vaduganathan, M.; Claggett, B.L.; Jering, K.S.; Bhatt, A.S.; Rosenthal, N.; Solomon, S.D. Clinical Outcomes in Young US Adults Hospitalized With COVID-19. JAMA Intern. Med. 2021, 181, 379. [Google Scholar] [CrossRef]
- Xie, J.; Tong, Z.; Guan, X.; Du, B.; Qiu, H. Clinical Characteristics of Patients Who Died of Coronavirus Disease 2019 in China. JAMA Netw. Open 2020, 3, e205619. [Google Scholar] [CrossRef] [Green Version]
- Rojas-Martínez, R.; Basto-Abreu, A.; Aguilar-Salinas, C.A.; Zárate-Rojas, E.; Villalpando, S.; Barrientos-Gutiérrez, T. Prevalencia de diabetes por diagnóstico médico previo en México. Salud Pública de México 2018, 60, 224. [Google Scholar] [CrossRef]
- Centers for Disease Prevention and Control. National Diabetes Statistics Report; Centers for Disease Prevention and Control: Atlanta, GA, USA, 2020; pp. 1–32.
- de Oliveira Toledo, S.L.; Nogueira, L.S.; das Gracas Carvalho, M.; Alves Rios, D.R.; de Barros Pinheiro, M. COVID-19: Review and hematologic impact. Clin. Chim. Acta 2020, 510, 170–176. [Google Scholar] [CrossRef] [PubMed]
- López, P.G.T.; Ramires, S.M.L.P.; Torres, A.M.S. Participantes de la respuesta inmunológica ante la infección por SARS-CoV-2. Alergia. Asma e Inmunología Pediátricas 2020, 29, 5–15. [Google Scholar] [CrossRef]
- Fischbach, F.T.; Dunning, M.B. A Manual of Laboratory and Diagnostic Tests, 8th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2009; pp. 56–183. [Google Scholar]
- Rizo-Téllez, S.A.; Méndez-García, L.A.; Flores-Rebollo, C.; Alba-Flores, F.; Alcántara-Suárez, R.; Manjarrez-Reyna, A.N.; Baltazar-Lopez, N.; Hernandez-Guzman, V.A.; Leon-Perdoza, J.I.; Zapata-Arenas, R.; et al. The Neutrophil-to-Monocyte Ratio and Lymphocyte-to-Neutrophil Ratio at Admission Predict In-Hospital Mortality in Mexican Patients with Severe SARS-CoV-2 Infection (COVID-19). Microorganisms 2020, 8, 1560. [Google Scholar] [CrossRef]
- Seyit, M.; Avci, E.; Nar, R.; Senol, H.; Yilmaz, A.; Ozen, M.; Oskay, A.; Aybek, H. Neutrophil to lymphocyte ratio, lymphocyte to monocyte ratio and platelet to lymphocyte ratio to predict the severity of COVID-19. Am. J. Emerg. Med. 2021, 40, 110–114. [Google Scholar] [CrossRef]
- Lagunas-Rangel, F.A. Neutrophil-to-lymphocyte ratio and lymphocyte-to-C-reactive protein ratio in patients with severe coronavirus disease 2019 (COVID-19): A meta-analysis. J. Med. Virol. 2020, 92, 1733–1734. [Google Scholar] [CrossRef] [Green Version]
- Georgakopoulou, V.E.; Garmpis, N.; Damaskos, C.; Valsami, S.; Dimitroulis, D.; Diamantis, E.; Farmaki, P.; Papageorgiou, C.V.; Makrodimitri, S.; Gravvanis, N.; et al. The Impact of Peripheral Eosinophil Counts and Eosinophil to Lymphocyte Ratio (ELR) in the Clinical Course of COVID-19 Patients: A Retrospective Study. In Vivo 2021, 35, 641–648. [Google Scholar] [CrossRef]
- Ye, W.; Chen, G.; Li, X.; Lan, X.; Ji, C.; Hou, M.; Zhang, D.; Zeng, G.; Wang, Y.; Xu, C.; et al. Dynamic changes of D-dimer and neutrophil-lymphocyte count ratio as prognostic biomarkers in COVID-19. Respir. Res. 2020, 21, 1–7. [Google Scholar] [CrossRef]
- Ocampo-Salgado, C.; Palacio-Uribe, J.; Duque-Ramírez, M.; Orrego-Garay, M.J. Valor pronóstico de biomarcadores cardíacos en la enfermedad por COVID-19. Revista Colombiana de Cardiología 2021, 27, 137–141. [Google Scholar] [CrossRef]
- Akbar, M.R.; Pranata, R.; Wibowo, A.; Lim, M.A.; Sihite, T.A.; Martha, J.W. The prognostic value of elevated creatine kinase to predict poor outcome in patients with COVID-19—A systematic review and meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Zhang, H.; Mu, S.; Wei, W.; Jin, C.; Tong, C.; Song, Z.; Zha, Y.; Xue, Y.; Gu, G. Lactate dehydrogenase, an independent risk factor of severe COVID-19 patients: A retrospective and observational study. Aging 2020, 12, 11245–11258. [Google Scholar] [CrossRef] [PubMed]
- Uaprasert, N.; Moonla, C.; Sosothikul, D.; Rojnuckarin, P.; Chiasakul, T. Systemic Coagulopathy in Hospitalized Patients with Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Clin. Appl. Thromb. 2021, 27. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, E.; Wright, E.; Kushner, B. In Young Adults with COVID-19, Obesity Is Associated with Adverse Outcomes. West. J. Emerg. Med. 2020, 21, 752–755. [Google Scholar] [CrossRef] [PubMed]
- Bonifazi, M.; Mei, F.; Skrami, E.; Latini, L.; Amico, D.; Balestro, E.; Bini, F.; Bonifazi, F.; Caminati, A.; Candoli, P.; et al. Predictors of Worse Prognosis in Young and Middle-Aged Adults Hospitalized with COVID-19 Pneumonia: A Multi-Center Italian Study (COVID-UNDER50). J. Clin. Med. 2021, 10, 1218. [Google Scholar] [CrossRef]
- Liu, J.; Liu, Y.; Xiang, P.; Pu, L.; Xiong, H.; Li, C.; Zhang, M.; Tan, J.; Xu, Y.; Song, R.; et al. Neutrophil-to-lymphocyte ratio predicts critical illness patients with 2019 coronavirus disease in the early stage. J. Transl. Med. 2020, 18, 206. [Google Scholar] [CrossRef]
- Ding, X.; Yu, Y.; Lu, B.; Huo, J.; Chen, M.; Kang, Y.; Lou, J.; Liu, Z. Dynamic profile and clinical implications of hematological parameters in hospitalized patients with coronavirus disease 2019. Clin. Chem. Lab. Med. 2020, 58, 1365–1371. [Google Scholar] [CrossRef]
- Fu, J.; Kong, J.; Wang, W.; Wu, M.; Yao, L.; Wang, Z.; Jin, J.; Wu, D.; Yu, X. The clinical implication of dynamic neutrophil to lymphocyte ratio and D-dimer in COVID-19: A retrospective study in Suzhou China. Thromb. Res. 2020, 192, 3–8. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, K.; Wei, H.; Chen, W.; Wang, W.; Jia, L.; Liu, Q.; Zhang, J.; Shan, T.; Peng, Z.; et al. Dynamic relationship between D-dimer and COVID-19 severity. Br. J. Haematol. 2020, 190, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Wu, C.; Zhang, Q.; Wu, F.; Yu, B.; Lv, J.; Li, Y.; Li, T.; Zhang, S.; Wu, C.; et al. C-Reactive Protein Level May Predict the Risk of COVID-19 Aggravation. Open Forum Infect. Dis. 2020, 7, ofaa153. [Google Scholar] [CrossRef] [PubMed]
- Orsucci, D. Is creatine kinase associated with outcome in COVID-19? Neuroimmunol. Neuroinflamm. 2020, 7. [Google Scholar] [CrossRef]
- Zhang, A.; Leng, Y.; Zhang, Y.; Wu, K.; Ji, Y.; Lei, S.; Xia, Z. Meta-analysis of coagulation parameters associated with disease severity and poor prognosis of COVID-19. Int. J. Infect. Dis. 2020, 100, 441–448. [Google Scholar] [CrossRef]
- Guo, J.; Zhou, B.; Zhu, M.; Yuan, Y.; Wang, Q.; Zhou, H.; Wang, X.; Lv, T.; Li, S.; Liu, P.; et al. CURB-65 may serve as a useful prognostic marker in COVID-19 patients within Wuhan, China: A retrospective cohort study. Epidemiol. Infect. 2020, 148, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Toh, C.H.; Hoots, W.K. The scoring system of the Scientific and Standardization Committee on Disseminated Intravascular Coagulation of the International Society on Thrombosis and Haemostasis: A 5-year overview. J. Thromb. Haemost. 2007, 5, 604–606. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Patients n (%) | Ambulatory n (%) | Hospitalized n (%) | Deaths n (%) | p-Value | |
|---|---|---|---|---|---|
| Obesity | 214 (12.7%) | 136 (63.6%) | 56 (26.2%) | 22 (10.3%) | <0.000 *** |
| AH | 144 (8.6%) | 96 (66.7%) | 35 (24.3%) | 13 (9.0%) | <0.000 *** |
| T2DM | 83 (4.9%) | 41 (49.4%) | 25 (30.1%) | 17 (20.5%) | <0.000 *** |
| Smoking | 82 (4.9%) | 64 (78.0%) | 15 (18.3%) | 3 (3.7%) | 0.304 |
| Asthma | 81 (4.8%) | 70 (86.4%) | 7 (8.6%) | 4 (4.9%) | 0.424 |
| Pregnancy | 44 (2.6%) | 35 (79.5%) | 9 (20.5%) | 0 (0%) | 0.153 |
| Total | 1681 (100%) | 1407 (83.7%) | 215 (12.7%) | 59 (3.5%) |
| Total n (%) | Ambulatory n (%) | Hospitalized n (%) | Deaths n (%) | p-Value | |
|---|---|---|---|---|---|
| Disseminated intravascular coagulation (DIC) | 4 (1.1%) | 0 (0%) | 3 (75%) | 1 (25.0%) | 0.0297 * |
| COVID-19-associated coagulopathy (CAC) | 33 (9.1%) | 4 (12.1%) | 20 (60.6%) | 9 (27.3%) | <0.0001 *** |
| Risk of CAC | 109 (30.3%) | 21 (19.3%) | 69 (63.3%) | 19 (17.4%) | <0.0001 *** |
| No alterations | 213 (59.3%) | 136 (63.8%) | 62 (29.1%) | 15 (7.0%) | |
| Total | 359 (100%) | 161 (44.8%) | 154 (42.9%) | 44 (12%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maldonado-Cabrera, A.; Angulo-Molina, A.; Haque, U.; Velazquez, C.; Álvarez-Villaseñor, A.S.; Santacruz-Gómez, K.J.; Gallego-Hernández, A.L. Acute Inflammatory Mediators in Young Adult Patients with COVID-19 in Mexico. Pathogens 2021, 10, 1056. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10081056
Maldonado-Cabrera A, Angulo-Molina A, Haque U, Velazquez C, Álvarez-Villaseñor AS, Santacruz-Gómez KJ, Gallego-Hernández AL. Acute Inflammatory Mediators in Young Adult Patients with COVID-19 in Mexico. Pathogens. 2021; 10(8):1056. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10081056
Chicago/Turabian StyleMaldonado-Cabrera, Anahí, Aracely Angulo-Molina, Ubydul Haque, Carlos Velazquez, Andrea S. Álvarez-Villaseñor, Karla J. Santacruz-Gómez, and Ana L. Gallego-Hernández. 2021. "Acute Inflammatory Mediators in Young Adult Patients with COVID-19 in Mexico" Pathogens 10, no. 8: 1056. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10081056