
Presence of SARS-CoV-2 in a Cornea Transplant

 , and
, and 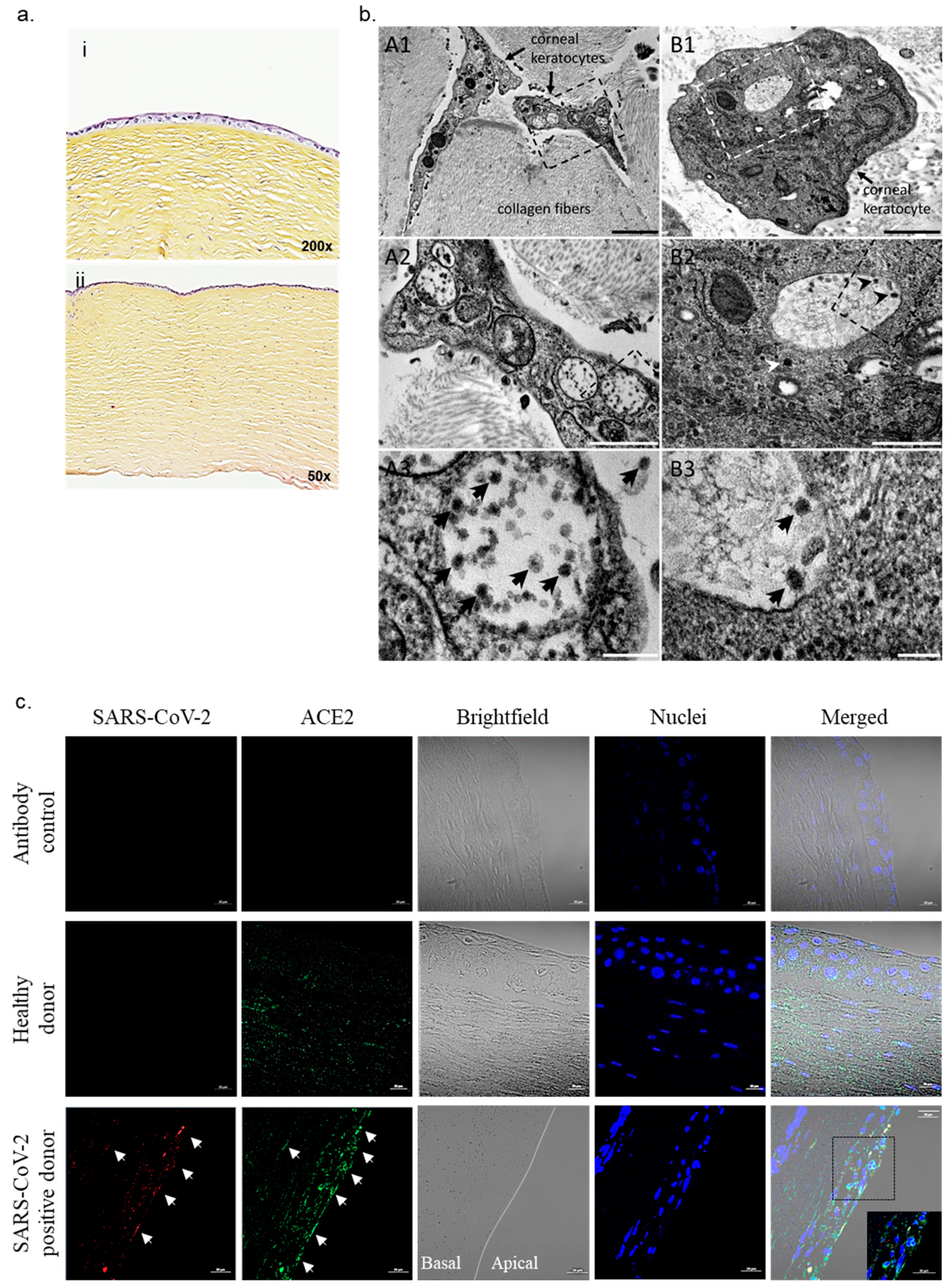{kind=link}
Abstract
:1. Introduction, Results and Discussion
2. Materials and Methods
2.1. Cornea Tissue
2.2. RT-PCR Analysis
2.3. Histological Analysis
2.4. Transmission Electron Microscopy
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bayyoud, T.; Iftner, A.; Iftner, T.; Bartz-Schmidt, K.U.; Ueffing, M.; Schindler, M.; Thaler, S. Absence of Severe Acute Respiratory Syndrome-Coronavirus-2 RNA in ocular tissues. Am. J. Ophthalmol. Case Rep. 2020, 19, 100805. [Google Scholar] [CrossRef] [PubMed]
- Deng, W.; Bao, L.; Gao, H.; Xiang, Z.; Qu, Y.; Song, Z.; Gong, S.; Liu, J.; Liu, J.; Yu, P.; et al. Ocular conjunctival inoculation of SARS-CoV-2 can cause mild COVID-19 in rhesus macaques. Nat. Commun. 2020, 11, 1–7. [Google Scholar] [CrossRef]
- Lange, C.; Wolf, J.; Auw-Haedrich, C.; Schlecht, A.; Boneva, S.; Lapp, T.; Horres, R.; Agostini, H.; Martin, G.; Reinhard, T.; et al. Expression of the COVID-19 receptor ACE2 in the human conjunctiva. J. Med. Virol. 2020, 92, 2081–2086. [Google Scholar] [CrossRef]
- Yan, Y.; Diao, B.; Liu, Y.; Zhang, W.; Wang, G.; Chen, X. Severe Acute Respiratory Syndrome Coronavirus 2 Nucleocapsid Protein in the Ocular Tissues of a Patient Previously Infected with Coronavirus Disease. JAMA Ophthalmol. 2020, 138, 1201–1204. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, V.; Motwani, R.; Kumar, A.; Kumari, C.; Raza, K. Histopathological observations in COVID-19: A systematic review. J. Clin. Pathol. 2021, 74, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J. Adenovirus: Ocular manifestations. Community Eye Health 2020, 33, 73–75. [Google Scholar] [PubMed]
- Sawant, O.B.; Singh, S.; Wright, R.E.; Jones, K.M.; Titus, M.S.; Dennis, E.; Hicks, E.; Majmudar, P.A.; Kumar, A.; Mian, S.I. Prevalence of SARS-CoV-2 in human post-mortem ocular tissues. Ocul. Surf. 2021, 19, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.K.; Mudgil, N.; Wadgave, Y.; Mishra, S.S. Corneal transplantation during COVID-19 pandemic: Need for special considerations—A live review. AIMS Public Health 2021, 8, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Desautels, J.D.; Moshirfar, M.; Martheswaran, T.; Shmunes, K.M.; Ronquillo, Y. Risks Posed to Corneal Transplant Recipients by COVID-19-Affected Donors. Ophthalmol. Ther. 2020, 9, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Gambardella, C.; Pagliuca, R.; Pomilla, G.; Gambardella, A. COVID-19 risk contagion: Organization and procedures in a South Italy geriatric oncology ward. J. Geriatr. Oncol. 2020, 11, 1187–1188. [Google Scholar] [CrossRef] [PubMed]
- Tolone, S.; Gambardella, C.; Brusciano, L.; del Genio, G.; Lucido, F.S.; Docimo, L. Telephonic triage before surgical ward admission and telemedicine during COVID-19 outbreak in Italy. Effective and easy procedures to reduce in-hospital positivity. Int. J. Surg. 2020, 78, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Vogels, C.B.F.; Brito, A.F.; Wyllie, A.L.; Fauver, J.R.; Ott, I.M.; Kalinich, C.C.; Petrone, M.E.; Casanovas-Massana, A.; Muenker, M.C.; Moore, A.J.; et al. Analytical sensitivity and efficiency comparisons of SARS-CoV-2 RT–qPCR primer–probe sets. Nat. Microbiol. 2020, 5, 1299–1305. [Google Scholar] [CrossRef] [PubMed]
- Heim, A.; Ebnet, C.; Harste, G.; Pring-Åkerblom, P. Rapid and quantitative detection of human adenovirus DNA by real-time PCR. J. Med. Virol. 2003, 70, 228–239. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.Y.Q.; Ninove, L.; Gaudart, J.; Nougairède, A.; Zandotti, C.; Thirion-Perrier, L.; Charrel, R.N.; De Lamballerie, X. A Retrospective Overview of Enterovirus Infection Diagnosis and Molecular Epidemiology in the Public Hospitals of Marseille, France (1985–2005). PLoS ONE 2011, 6, e18022. [Google Scholar] [CrossRef] [PubMed]
- Griscelli, F.; Barrois, M.; Chauvin, S.; Lastere, S.; Bellet, D.; Bourhis, J.-H. Quantification of Human Cytomegalovirus DNA in Bone Marrow Transplant Recipients by Real-Time PCR. J. Clin. Microbiol. 2001, 39, 4362–4369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, H.H.; Mühlbauer, G.; Rinner, B.; Stelzl, E.; Berger, A.; Dörr, H.-W.; Santner, B.; Marth, E.; Rabenau, H. Detection of Herpes Simplex Virus DNA by Real-Time PCR. J. Clin. Microbiol. 2000, 38, 2638–2642. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otmani Idrissi, M.; Baudoin, J.-P.; Chateau, A.-L.; Aherfi, S.; Bedotto-Buffet, M.; Latil, A.; Lepidi, H.; Chiaroni, J.; Picard, C.; Mege, J.-L.; et al. Presence of SARS-CoV-2 in a Cornea Transplant. Pathogens 2021, 10, 934. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10080934
Otmani Idrissi M, Baudoin J-P, Chateau A-L, Aherfi S, Bedotto-Buffet M, Latil A, Lepidi H, Chiaroni J, Picard C, Mege J-L, et al. Presence of SARS-CoV-2 in a Cornea Transplant. Pathogens. 2021; 10(8):934. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10080934
Chicago/Turabian StyleOtmani Idrissi, Myriem, Jean-Pierre Baudoin, Anne-Line Chateau, Sarah Aherfi, Marielle Bedotto-Buffet, Alain Latil, Hubert Lepidi, Jacques Chiaroni, Christophe Picard, Jean-Louis Mege, and et al. 2021. "Presence of SARS-CoV-2 in a Cornea Transplant" Pathogens 10, no. 8: 934. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10080934