
Lyme Carditis: From Pathophysiology to Clinical Management

 , , and
, , and
Abstract
:1. Introduction
2. Lyme Disease: Pathogen, Transmission, and Clinical Manifestations
3. Epidemiology of Lyme Disease and Lyme Carditis
4. Pathogenesis and Histology
4.1. Pathogenesis of Cardiac Damage and Histological Findings
4.2. Histological Findings
5. Clinical Manifestations
5.1. Conduction Abnormalities
5.2. Endocarditis, Myocarditis, and Pericarditis
5.3. Dilated Cardiomyopathy
6. Diagnosis
6.1. Serologic Testing
6.2. Other Laboratory Tests
6.3. Cardiac Evaluation: Electrocardiogram, Echocardiogram, and Other Imaging Techniques
7. Therapy
7.1. Antibiotic Prophylaxis
7.2. Antibiotic Therapy
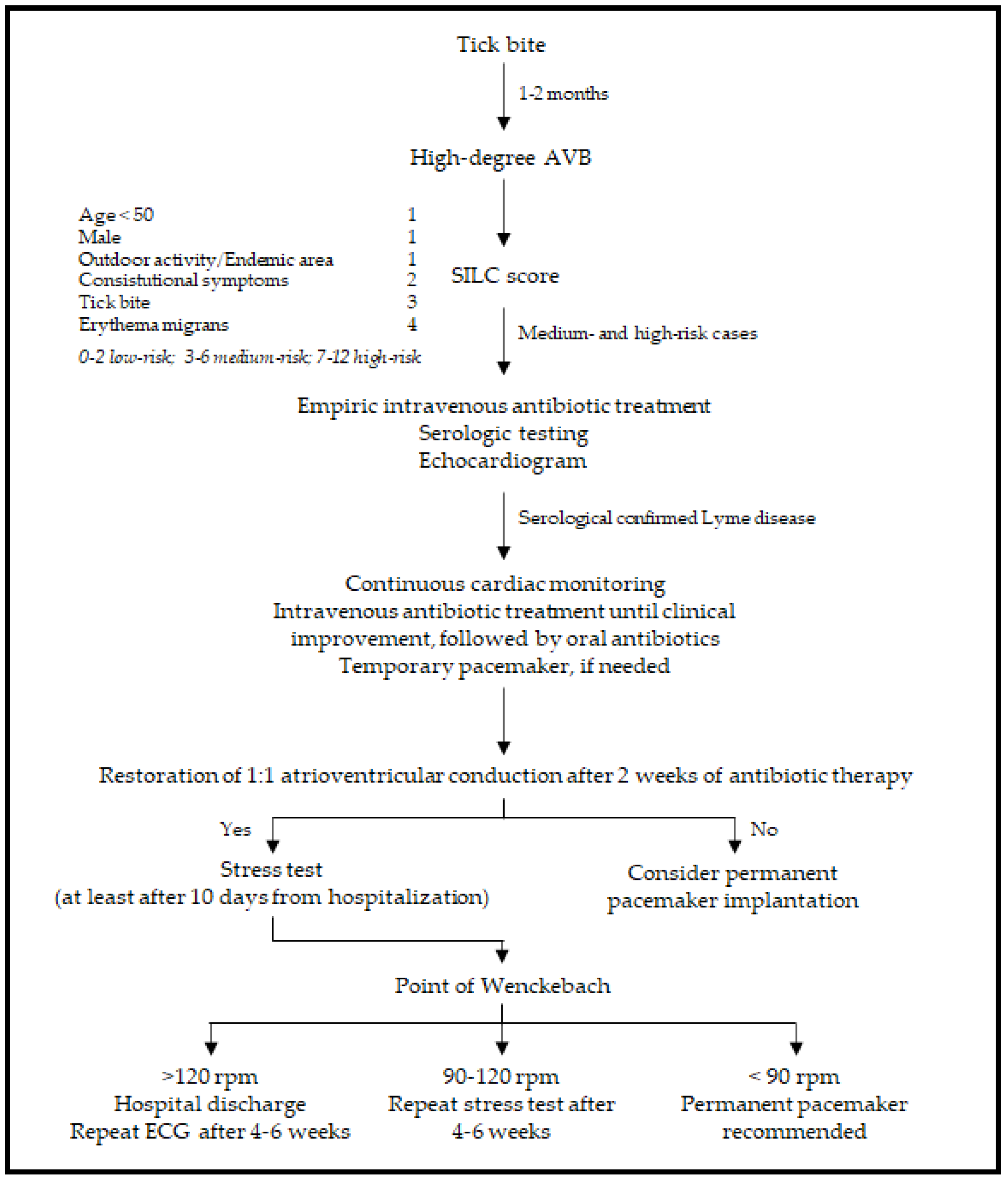
7.3. Pacing
8. Prognosis and Probability of Reinfection
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Radolf, J.D.; Strle, K.; Lemieux, J.E.; Strle, F. Lyme Disease in Humans. Curr. Issues Mol. Biol. 2021, 42, 333–384. [Google Scholar] [CrossRef]
- Trevisan, G.; Cinco, M.; Trevisini, S.; di Meo, N.; Chersi, K.; Ruscio, M.; Forgione, P.; Bonin, S. Borreliae Part 1: Borrelia Lyme Group and Echidna-Reptile Group. Biology 2021, 10, 1036. [Google Scholar] [CrossRef]
- Pritt, B.S.; Mead, P.S.; Johnson, D.K.H.; Neitzel, D.F.; Respicio-Kingry, L.B.; Davis, J.P.; Schiffman, E.; Sloan, L.M.; Schriefer, M.E.; Replogle, A.J.; et al. Identification of a novel pathogenic Borrelia species causing Lyme borreliosis with unusually high spirochaetaemia: A descriptive study. Lancet Infect. Dis. 2016, 16, 556–564. [Google Scholar] [CrossRef] [Green Version]
- Steere, A.C.; Strle, F.; Wormser, G.P.; Hu, L.T.; Branda, J.A.; Hovius, J.W.; Li, X.; Mead, P.S. Lyme borreliosis. Nat. Rev. Dis. Primers 2016, 2, 16090. [Google Scholar] [CrossRef]
- Rollend, L.; Fish, D.; Childs, J.E. Transovarial transmission of Borrelia spirochetes by Ixodes scapularis: A summary of the literature and recent observations. Ticks Tick Borne Dis. 2013, 4, 46–51. [Google Scholar] [CrossRef]
- Radolf, J.D.; Caimano, M.J.; Stevenson, B.; Hu, L.T. Of ticks, mice and men: Understanding the dual-host lifestyle of Lyme disease spirochaetes. Nat. Rev. Microbiol. 2012, 10, 87–99. [Google Scholar] [CrossRef] [Green Version]
- Scheffold, N.; Herkommer, B.; Kandolf, R.; May, A.E. Lyme carditis—Diagnosis, treatment and prognosis. Deutsches Ärzteblatt International 2015, 112, 202–208. [Google Scholar] [CrossRef] [Green Version]
- Kugeler, K.J.; Schwartz, A.M.; Delorey, M.J.; Mead, P.S.; Hinckley, A.F. Estimating the Frequency of Lyme Disease Diagnoses, United States, 2010–2018. Emerg. Infect. Dis. 2021, 27, 616–619. [Google Scholar] [CrossRef]
- Fish, A.E.; Pride, Y.B.; Pinto, D.S. Lyme carditis. Infect. Dis. Clin. N. Am. 2008, 22, 275–288. [Google Scholar] [CrossRef]
- Forrester, J.D.; Meiman, J.; Mullins, J.; Nelson, R.; Ertel, S.H.; Cartter, M.; Brown, C.M.; Lijewski, V.; Schiffman, E.; Neitzel, D.; et al. Notes from the field: Update on Lyme carditis, groups at high risk, and frequency of associated sudden cardiac death—United States. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 982–983. [Google Scholar]
- Kostic, T.; Momcilovic, S.; Perisic, Z.D.; Apostolovic, S.R.; Cvetkovic, J.; Jovanovic, A.; Barac, A.; Salinger-Martinovic, S.; Tasic-Otasevic, S. Manifestations of Lyme carditis. Int. J. Cardiol. 2017, 232, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Linden, H. Lyme Carditis. Available online: https://www.uptodate.com/contents/lyme-carditis (accessed on 19 March 2022).
- O’Connell, S.; Granström, M.; Gray, J.S.; Stanek, G. Epidemiology of European Lyme borreliosis. Zentralblatt für Bakteriologie 1998, 287, 229–240. [Google Scholar] [CrossRef]
- Lantos, P.M.; Rumbaugh, J.; Bockenstedt, L.K.; Falck-Ytter, Y.T.; Aguero-Rosenfeld, M.E.; Auwaerter, P.G.; Baldwin, K.; Bannuru, R.R.; Belani, K.K.; Bowie, W.R.; et al. Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the Prevention, Diagnosis and Treatment of Lyme Disease. Clin. Infect. Dis. 2021, 72, e1–e48. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, E.D.; Wormser, G.P. Lyme Disease in 2018: What Is New (and What Is Not). JAMA 2018, 320, 635–636. [Google Scholar] [CrossRef]
- Schwartz, A.M.; Hinckley, A.F.; Mead, P.S.; Hook, S.A.; Kugeler, K.J. Surveillance for Lyme Disease—United States, 2008–2015. MMWR Surveill. Summ. 2017, 66, 1–12. [Google Scholar] [CrossRef]
- van der Linde, M.R. Lyme carditis: Clinical characteristics of 105 cases. Scand. J. Infect. Dis. Suppl. 1991, 77, 81–84. [Google Scholar]
- Caine, J.A.; Coburn, J. A short-term Borrelia burgdorferi infection model identifies tissue tropisms and bloodstream survival conferred by adhesion proteins. Infect. Immun. 2015, 83, 3184–3194. [Google Scholar] [CrossRef] [Green Version]
- Brown, E.L.; Wooten, R.M.; Johnson, B.J.; Iozzo, R.V.; Smith, A.; Dolan, M.C.; Guo, B.P.; Weis, J.J.; Höök, M. Resistance to Lyme disease in decorin-deficient mice. J. Clin. Investig. 2001, 107, 845–852. [Google Scholar] [CrossRef]
- Lin, Y.P.; Benoit, V.; Yang, X.; Martinez-Herranz, R.; Pal, U.; Leong, J.M. Strain-specific variation of the decorin-binding adhesin DbpA influences the tissue tropism of the lyme disease spirochete. PLoS Pathog. 2014, 10, e1004238. [Google Scholar] [CrossRef]
- Liang, F.T.; Brown, E.L.; Wang, T.; Iozzo, R.V.; Fikrig, E. Protective niche for Borrelia burgdorferi to evade humoral immunity. Am. J. Pathol. 2004, 165, 977–985. [Google Scholar] [CrossRef] [Green Version]
- Weening, E.H.; Parveen, N.; Trzeciakowski, J.P.; Leong, J.M.; Höök, M.; Skare, J.T. Borrelia burgdorferi lacking DbpBA exhibits an early survival defect during experimental infection. Infect. Immun. 2008, 76, 5694–5705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Koning, J.; Hoogkamp-Korstanje, J.A.; van der Linde, M.R.; Crijns, H.J. Demonstration of spirochetes in cardiac biopsies of patients with Lyme disease. J. Infect. Dis. 1989, 160, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Yeung, C.; Baranchuk, A. Diagnosis and Treatment of Lyme Carditis: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 73, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Cadavid, D.; Bai, Y.; Hodzic, E.; Narayan, K.; Barthold, S.W.; Pachner, A.R. Cardiac involvement in non-human primates infected with the Lyme disease spirochete Borrelia burgdorferi. Lab. Investig. 2004, 84, 1439–1450. [Google Scholar] [CrossRef] [PubMed]
- Saba, S.; VanderBrink, B.A.; Perides, G.; Glickstein, L.J.; Link, M.S.; Homoud, M.K.; Bronson, R.T.; Estes, M., III; Wang, P.J. Cardiac conduction abnormalities in a mouse model of Lyme borreliosis. J. Interv. Card. Electrophysiol. 2001, 5, 137–143. [Google Scholar] [CrossRef]
- Raveche, E.S.; Schutzer, S.E.; Fernandes, H.; Bateman, H.; McCarthy, B.A.; Nickell, S.P.; Cunningham, M.W. Evidence of Borrelia autoimmunity-induced component of Lyme carditis and arthritis. J. Clin. Microbiol. 2005, 43, 850–856. [Google Scholar] [CrossRef] [Green Version]
- Nardelli, D.T.; Callister, S.M.; Schell, R.F. Lyme arthritis: Current concepts and a change in paradigm. Clin. Vaccine Immunol. 2008, 15, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Barthold, S.W.; Persing, D.H.; Armstrong, A.L.; Peeples, R.A. Kinetics of Borrelia burgdorferi dissemination and evolution of disease after intradermal inoculation of mice. Am. J. Pathol. 1991, 139, 263–273. [Google Scholar]
- Armstrong, A.L.; Barthold, S.W.; Persing, D.H.; Beck, D.S. Carditis in Lyme disease susceptible and resistant strains of laboratory mice infected with Borrelia burgdorferi. Am. J. Trop. Med. Hyg. 1992, 47, 249–258. [Google Scholar] [CrossRef]
- Sharma, A.K.; Almaddah, N.; Chaudhry, K.; Ganatra, S.; Chaudhry, G.M.; Silver, J. Without Further Delay: Lyme Carditis. Am. J. Med. 2018, 131, 384–386. [Google Scholar] [CrossRef]
- Muehlenbachs, A.; Bollweg, B.C.; Schulz, T.J.; Forrester, J.D.; DeLeon Carnes, M.; Molins, C.; Ray, G.S.; Cummings, P.M.; Ritter, J.M.; Blau, D.M.; et al. Cardiac Tropism of Borrelia burgdorferi: An Autopsy Study of Sudden Cardiac Death Associated with Lyme Carditis. Am. J. Pathol. 2016, 186, 1195–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavora, F.; Burke, A.; Li, L.; Franks, T.J.; Virmani, R. Postmortem confirmation of Lyme carditis with polymerase chain reaction. Cardiovasc. Pathol. 2008, 17, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Haddad, F.A.; Nadelman, R.B. Lyme disease and the heart. Front. Biosci. 2003, 8, s769–s782. [Google Scholar] [CrossRef]
- McAlister, H.F.; Klementowicz, P.T.; Andrews, C.; Fisher, J.D.; Feld, M.; Furman, S. Lyme carditis: An important cause of reversible heart block. Ann. Intern. Med. 1989, 110, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Steere, A.C.; Batsford, W.P.; Weinberg, M.; Alexander, J.; Berger, H.J.; Wolfson, S.; Malawista, S.E. Lyme carditis: Cardiac abnormalities of Lyme disease. Ann. Intern. Med. 1980, 93, 8–16. [Google Scholar] [CrossRef]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef]
- Bush, L.M.; Vazquez-Pertejo, M.T. Tick borne illness-Lyme disease. Dis. Mon. 2018, 64, 195–212. [Google Scholar] [CrossRef]
- Nikolic, A.; Boljevic, D.; Bojic, M.; Veljkovic, S.; Vukovic, D.; Paglietti, B.; Micic, J.; Rubino, S. Lyme Endocarditis as an Emerging Infectious Disease: A Review of the Literature. Front. Microbiol. 2020, 11, 278. [Google Scholar] [CrossRef]
- Maher, B.; Murday, D.; Harden, S.P. Cardiac MRI of Lyme disease myocarditis. Heart 2012, 98, 264. [Google Scholar] [CrossRef]
- Gasser, R.; Dusleag, J.; Reisinger, E.; Stauber, R.; Feigl, B.; Pongratz, S.; Klein, W.; Furian, C.; Pierer, K. Reversal by ceftriaxone of dilated cardiomyopathy Borrelia burgdorferi infection. Lancet 1992, 339, 1174–1175. [Google Scholar] [CrossRef]
- Sonnesyn, S.W.; Diehl, S.C.; Johnson, R.C.; Kubo, S.H.; Goodman, J.L. A prospective study of the seroprevalence of Borrelia burgdorferi infection in patients with severe heart failure. Am. J. Cardiol. 1995, 76, 97–100. [Google Scholar] [CrossRef]
- Rees, D.H.; Keeling, P.J.; McKenna, W.J.; Axford, J.S. No evidence to implicate Borrelia burgdorferi in the pathogenesis of dilated cardiomyopathy in the United Kingdom. Br. Heart J. 1994, 71, 459–461. [Google Scholar] [CrossRef] [PubMed]
- Besant, G.; Wan, D.; Yeung, C.; Blakely, C.; Branscombe, P.; Suarez-Fuster, L.; Redfearn, D.; Simpson, C.; Abdollah, H.; Glover, B.; et al. Suspicious index in Lyme carditis: Systematic review and proposed new risk score. Clin. Cardiol. 2018, 41, 1611–1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steere, A.C.; McHugh, G.; Damle, N.; Sikand, V.K. Prospective study of serologic tests for lyme disease. Clin. Infect. Dis. 2008, 47, 188–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dressler, F.; Whalen, J.A.; Reinhardt, B.N.; Steere, A.C. Western blotting in the serodiagnosis of Lyme disease. J. Infect. Dis. 1993, 167, 392–400. [Google Scholar] [CrossRef]
- Talagrand-Reboul, E.; Raffetin, A.; Zachary, P.; Jaulhac, B.; Eldin, C. Immunoserological Diagnosis of Human Borrelioses: Current Knowledge and Perspectives. Front. Cell. Infect. Microbiol. 2020, 10, 241. [Google Scholar] [CrossRef]
- Bobe, J.R.; Jutras, B.L.; Horn, E.J.; Embers, M.E.; Bailey, A.; Moritz, R.L.; Zhang, Y.; Soloski, M.J.; Ostfeld, R.S.; Marconi, R.T.; et al. Recent Progress in Lyme Disease and Remaining Challenges. Front. Med. 2021, 8, 666554. [Google Scholar] [CrossRef]
- Theel, E.S. The Past, Present, and (Possible) Future of Serologic Testing for Lyme Disease. J. Clin. Microbiol. 2016, 54, 1191–1196. [Google Scholar] [CrossRef] [Green Version]
- Branda, J.A.; Steere, A.C. Laboratory Diagnosis of Lyme Borreliosis. Clin. Microbiol. Rev. 2021, 34. [Google Scholar] [CrossRef]
- Branda, J.A.; Body, B.A.; Boyle, J.; Branson, B.M.; Dattwyler, R.J.; Fikrig, E.; Gerald, N.J.; Gomes-Solecki, M.; Kintrup, M.; Ledizet, M.; et al. Advances in Serodiagnostic Testing for Lyme Disease Are at Hand. Clin. Infect. Dis. 2018, 66, 1133–1139. [Google Scholar] [CrossRef] [Green Version]
- Moore, A.; Nelson, C.; Molins, C.; Mead, P.; Schriefer, M. Current Guidelines, Common Clinical Pitfalls, and Future Directions for Laboratory Diagnosis of Lyme Disease, United States. Emerg. Infect. Dis. 2016, 22, 1169–1177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnarelli, L.A.; Miller, J.N.; Anderson, J.F.; Riviere, G.R. Cross-reactivity of nonspecific treponemal antibody in serologic tests for Lyme disease. J. Clin. Microbiol. 1990, 28, 1276–1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnarelli, L.A.; Anderson, J.F. Enzyme-linked immunosorbent assays for the detection of class-specific immunoglobulins to Borrelia burgdorferi. Am. J. Epidemiol. 1988, 127, 818–825. [Google Scholar] [CrossRef] [PubMed]
- Porwancher, R.B.; Hagerty, C.G.; Fan, J.; Landsberg, L.; Johnson, B.J.; Kopnitsky, M.; Steere, A.C.; Kulas, K.; Wong, S.J. Multiplex immunoassay for Lyme disease using VlsE1-IgG and pepC10-IgM antibodies: Improving test performance through bioinformatics. Clin. Vaccine Immunol. 2011, 18, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Seriburi, V.; Ndukwe, N.; Chang, Z.; Cox, M.E.; Wormser, G.P. High frequency of false positive IgM immunoblots for Borrelia burgdorferi in clinical practice. Clin. Microbiol. Infect. 2012, 18, 1236–1240. [Google Scholar] [CrossRef] [Green Version]
- Karatolios, K.; Maisch, B.; Pankuweit, S. Suspected inflammatory cardiomyopathy. Prevalence of Borrelia burgdorferi in endomyocardial biopsies with positive serological evidence. Herz 2015, 40 (Suppl. 1), 91–95. [Google Scholar] [CrossRef]
- Robinson, M.L.; Kobayashi, T.; Higgins, Y.; Calkins, H.; Melia, M.T. Lyme carditis. Infect. Dis. Clin. N. Am. 2015, 29, 255–268. [Google Scholar] [CrossRef]
- Koene, R.; Boulware, D.R.; Kemperman, M.; Konety, S.H.; Groth, M.; Jessurun, J.; Eckman, P.M. Acute heart failure from lyme carditis. Circ. Heart Fail. 2012, 5, e24–e26. [Google Scholar] [CrossRef] [Green Version]
- Avitabile, C.M.; Harris, M.A.; Chowdhury, D. Cardiac Magnetic Resonance Characterizes Myocarditis in a 16-Year-Old Female With Lyme Disease. World J. Pediatr. Congenit. Heart Surg. 2016, 7, 394–396. [Google Scholar] [CrossRef]
- Munk, P.S.; Orn, S.; Larsen, A.I. Lyme carditis: Persistent local delayed enhancement by cardiac magnetic resonance imaging. Int. J. Cardiol. 2007, 115, e108–e110. [Google Scholar] [CrossRef]
- Karadag, B.; Spieker, L.E.; Schwitter, J.; Ruschitzka, F.; Luscher, T.F.; Noll, G.; Corti, R. Lyme carditis: Restitutio ad integrum documented by cardiac magnetic resonance imaging. Cardiol. Rev. 2004, 12, 185–187. [Google Scholar] [CrossRef] [PubMed]
- Alpert, L.I.; Welch, P.; Fisher, N. Gallium-positive Lyme disease myocarditis. Clin. Nucl. Med. 1985, 10, 617. [Google Scholar] [CrossRef] [PubMed]
- Bergler-Klein, J.; Sochor, H.; Stanek, G.; Globits, S.; Ullrich, R.; Glogar, D. Indium 111-monoclonal antimyosin antibody and magnetic resonance imaging in the diagnosis of acute Lyme myopericarditis. Arch. Intern. Med. 1993, 153, 2696–2700. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef] [PubMed]
- Reznick, J.W.; Braunstein, D.B.; Walsh, R.L.; Smith, C.R.; Wolfson, P.M.; Gierke, L.W.; Gorelkin, L.; Chandler, F.W. Lyme carditis. Electrophysiologic and histopathologic study. Am. J. Med. 1986, 81, 923–927. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Lyme Carditis. Available online: https://www.cdc.gov/lyme/treatment/lymecarditis.html (accessed on 19 March 2022).
- Hu, L.; Eugene, D.S. Treatment of Lyme Disease. Available online: https://www.uptodate.com/contents/treatment-of-lyme-disease (accessed on 19 March 2022).
- National Institute for Health and Care Excellence Guidelines. Lyme Disease. Available online: https://www.nice.org.uk/guidance/ng95/chapter/Recommendations#management (accessed on 19 March 2022).
- Todd, S.R.; Dahlgren, F.S.; Traeger, M.S.; Beltrán-Aguilar, E.D.; Marianos, D.W.; Hamilton, C.; McQuiston, J.H.; Regan, J.J. No visible dental staining in children treated with doxycycline for suspected Rocky Mountain Spotted Fever. J. Pediatr. 2015, 166, 1246–1251. [Google Scholar] [CrossRef] [Green Version]
- Volovitz, B.; Shkap, R.; Amir, J.; Calderon, S.; Varsano, I.; Nussinovitch, M. Absence of tooth staining with doxycycline treatment in young children. Clin. Pediatr. 2007, 46, 121–126. [Google Scholar] [CrossRef]
- Wormser, G.P.; Strle, F.; Shapiro, E.D. Is Doxycycline Appropriate for Routine Treatment of Young Children With Erythema Migrans? Pediatr. Infect. Dis. J. 2019, 38, 1113–1114. [Google Scholar] [CrossRef]
- Smith, G.N.; Gemmill, I.; Moore, K.M. Management of Tick Bites and Lyme Disease During Pregnancy. J. Obstet. Gynaecol. Can. 2012, 34, 1087–1091. [Google Scholar] [CrossRef]
- Doxycycline. In Drugs and Lactation Database (LactMed); National Library of Medicine: Bethesda, MD, USA, 2006.
- American Academy of Pediatrics Committee on Drugs. Transfer of drugs and other chemicals into human milk. Pediatrics 2001, 108, 776–789. [Google Scholar] [CrossRef] [Green Version]
- Krause, P.J.; Bockenstedt, L.K. Cardiology patient pages. Lyme disease and the heart. Circulation 2013, 127, e451–e454. [Google Scholar] [CrossRef]
- Mayer, W.; Kleber, F.X.; Wilske, B.; Preac-Mursic, V.; Maciejewski, W.; Sigl, H.; Holzer, E.; Doering, W. Persistent atrioventricular block in Lyme borreliosis. Klinische Wochenschrift 1990, 68, 431–435. [Google Scholar] [CrossRef] [PubMed]
- van der Linde, M.R.; Crijns, H.J.; de Koning, J.; Hoogkamp-Korstanje, J.A.; de Graaf, J.J.; Piers, D.A.; van der Galien, A.; Lie, K.I. Range of atrioventricular conduction disturbances in Lyme borreliosis: A report of four cases and review of other published reports. Br. Heart J. 1990, 63, 162–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artigao, R.; Torres, G.; Guerrero, A.; Jimenez-Mena, M.; Bayas Paredes, M. Irreversible complete heart block in Lyme disease. Am. J. Med. 1991, 90, 531–533. [Google Scholar] [CrossRef]
- Wang, C.N.; Yeung, C.; Enriquez, A.; Chacko, S.; Hanson, S.; Redfearn, D.; Simpson, C.; Abdollah, H.; Baranchuk, A. Long-term Outcomes in Treated Lyme Carditis. Curr. Probl. Cardiol. 2021, 100939. [Google Scholar] [CrossRef] [PubMed]
- Nadelman, R.B.; Wormser, G.P. Reinfection in Patients with Lyme Disease. Clin. Infect. Dis. 2007, 45, 1032–1038. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| INTRINSIC | EXTRINSIC |
|---|---|
| Infectious Diseases | Metabolic Disorders |
| Endocarditis (perivalvular abscess) Myocarditis Lyme disease Diphtheria Toxoplasmosis Chagas disease | Hypothyroidism Anorexia Hypoxia Acidosis Hypothermia |
| Infiltrative Diseases | Electrolyte Imbalance |
| Sarcoidosis Amyloidosis Hemochromatosis | Hypokalemia Hyperkaliemia Hypercalcemia Hypermagnesemia |
| Collagen Vascular Diseases | Neurological Disorders |
| Rheumatoid arthritis Scleroderma Systemic lupus erythematosus Storage diseases Neuromuscular diseases | Increased intracranial pressure Central nervous system tumors Temporal epilepsy Obstructive sleep apnea |
| Cardiac Surgery | Miscellaneous |
| Coronary artery bypass grafting Valve surgery (including TAVI) Heart transplant Radiation therapy Intended or iatrogenic AVB | Physical training (sports) Vagal refle XDrug effects Idiopathic paroxysmal AVB |
| Others | |
| Idiopathic (aging, degenerative) Infarction/ischemia Cardiomyopathies Genetic disorders Congenital heart diseases |
| MILD (1st-Degree AVB with PR Interval <300 msec) | ADULTS | Antibiotic Drug | Dosage and Way of Administration | Duration (Days) |
| Doxycycline | 100 mg, twice per day orally | 14–21 days | ||
| Amoxicillin | 500 mg, three times per day orally | 14–21 days | ||
| Cefuroxime | 500 mg, twice per day orally | 14–21 days | ||
| CHILDREN | Doxycycline ** | 4.4 mg/kg per day orally, divided into 2 doses Maximum 100 mg per dose | 14–21 days | |
| Amoxicillin | 50 mg/kg per day orally, divided into 3 doses Maximum 500 mg per dose | 14–21 days | ||
| Cefuroxime | 30 mg/kg per day orally, divided into 2 doses Maximum 500 mg per dose | 14–21 days | ||
| SEVERE (Symptomatic, 1st-degree AVB with PR interval ≥300 msec, 2nd or 3rd degree AV block) | ADULTS | Ceftriaxone | 2 g intravenously * once a day | 14–21 days |
| CHILDREN | Ceftriaxone | 2 g intravenously * once a day | 14–21 days |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radesich, C.; Del Mestre, E.; Medo, K.; Vitrella, G.; Manca, P.; Chiatto, M.; Castrichini, M.; Sinagra, G. Lyme Carditis: From Pathophysiology to Clinical Management. Pathogens 2022, 11, 582. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11050582
Radesich C, Del Mestre E, Medo K, Vitrella G, Manca P, Chiatto M, Castrichini M, Sinagra G. Lyme Carditis: From Pathophysiology to Clinical Management. Pathogens. 2022; 11(5):582. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11050582
Chicago/Turabian StyleRadesich, Cinzia, Eva Del Mestre, Kristen Medo, Giancarlo Vitrella, Paolo Manca, Mario Chiatto, Matteo Castrichini, and Gianfranco Sinagra. 2022. "Lyme Carditis: From Pathophysiology to Clinical Management" Pathogens 11, no. 5: 582. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11050582