
Pericardial Effusion Due to Trichosporon japonicum: A Case Report and Review of the Literature

 and
and
Abstract
:1. Introduction
2. Case Presentation
2.1. Patient History
2.2. Diagnostic Assessment and Therapeutic Intervention
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Colombo, A.L.; Padovan, A.C.B.; Chaves, G.M. Current Knowledge of Trichosporon spp. and Trichosporonosis. Clin. Microbiol. Rev. 2011, 24, 682–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bretagne, S.; Renaudat, C.; Desnos-Ollivier, M.; Sitbon, K.; Lortholary, O.; Dromer, F. French Mycosis Study Group Predisposing Factors and Outcome of Uncommon Yeast Species-Related Fungaemia Based on an Exhaustive Surveillance Programme (2002-14). J. Antimicrob. Chemother. 2017, 72, 1784–1793. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.-A.; Perfect, J.; Colombo, A.L.; Cornely, O.A.; Groll, A.H.; Seidel, D.; Albus, K.; de Almedia, J.N.; Garcia-Effron, G.; Gilroy, N.; et al. Global Guideline for the Diagnosis and Management of Rare Yeast Infections: An Initiative of the ECMM in Cooperation with ISHAM and ASM. Lancet Infect. Dis. 2021, 21, e375–e386. [Google Scholar] [CrossRef]
- Kabtani, J.; Diongue, K.; Dione, J.-N.; Delmas, A.; L’Ollivier, C.; Amoureux, M.-C.; Ndiaye, D.; Ranque, S. Real-Time PCR Assay for the Detection of Dermatophytes: Comparison between an In-House Method and a Commercial Kit for the Diagnosis of Dermatophytoses in Patients from Dakar, Senegal. J. Fungi 2021, 7, 949. [Google Scholar] [CrossRef]
- Sugita, T.; Nakase, T. Trichosporon Japonicum sp. Nov. Isolated from the Air. Int. J. Syst. Bacteriol. 1998, 48 Pt 4, 1425–1429. [Google Scholar] [CrossRef] [Green Version]
- Bongomin, F.; Otu, A.; Calisti, G.; Richardson, M.D.; Barnard, J.; Venkateswaran, R.; Vergidis, P. Trichosporon Japonicum Fungemia and Ventricular Assist Device Infection in an Immunocompetent Patient. Open Forum Infect. Dis. 2019, 6, ofz343. [Google Scholar] [CrossRef] [Green Version]
- Albitar-Nehme, S.; Agosta, M.; Kowalska, A.H.; Mancinelli, L.; Onori, M.; Lucignano, B.; Mattana, G.; Quagliarella, F.; Cefalo, M.G.; Merli, P.; et al. Case Report: Trichosporon Japonicum Fungemia in a Pediatric Patient with Refractory Acute B Cell Lymphoblastic Leukemia. Front. Pediatr. 2022, 10, 861476. [Google Scholar] [CrossRef]
- Li, T.; Huang, Y.; Chen, X.; Wang, Z.; Xu, Y. Urinary Tract Infections Caused by Fluconazole-Resistant Trichosporon Japonicum in 2 Kidney Transplant Patients and Analysis of Their Homology. Open Forum Infect. Dis. 2020, 7, ofaa365. [Google Scholar] [CrossRef]
- Ağirbasli, H.; Bilgen, H.; Ozcan, S.K.; Otlu, B.; Sinik, G.; Cerikçioğlu, N.; Durmaz, R.; Can, E.; Yalman, N.; Gedikoğlu, G.; et al. Two Possible Cases of Trichosporon Infections in Bone-Marrow-Transplanted Children: The First Case of T. Japonicum Isolated from Clinical Specimens. Jpn. J. Infect. Dis. 2008, 61, 130–132. [Google Scholar]
- Unoura, K.; Miyazaki, Y.; Sumi, Y.; Tamaoka, M.; Sugita, T.; Inase, N. Identification of Fungal DNA in BALF from Patients with Home-Related Hypersensitivity Pneumonitis. Respir. Med. 2011, 105, 1696–1703. [Google Scholar] [CrossRef] [Green Version]
- Lara, B.R.; de Camargo, B.B.; Paula, C.R.; Junior, D.P.L.; Garces, H.G.; Arnoni, M.V.; Silveira, M.; Gimenes, V.M.F.; Siqueira, L.P.M.; Takahashi, J.P.F.; et al. Comparing the Phenotypic, Genotypic, and Proteomic Identification of Trichosporon Species: A Globally Emerging Yeast of Medical Importance. Med. Mycol. 2021, 59, 1181–1190. [Google Scholar] [CrossRef] [PubMed]
- Aydin, M.; Kustimur, S.; Kalkanci, A.; Duran, T. Identification of Medically Important Yeasts by Sequence Analysis of the Internal Transcribed Spacer and D1/D2 Region of the Large Ribosomal Subunit. Rev. Iberoam. Micol. 2019, 36, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Sugita, T.; Nakajima, M.; Ikeda, R.; Matsushima, T.; Shinoda, T. Sequence Analysis of the Ribosomal DNA Intergenic Spacer 1 Regions of Trichosporon Species. J. Clin. Microbiol. 2002, 40, 1826–1830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz, M.R.; Fell, J.W. High-Throughput Detection of Pathogenic Yeasts of the Genus Trichosporon. J. Clin. Microbiol. 2004, 42, 3696–3706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desnos-Ollivier, M.; Maufrais, C.; Pihet, M.; Aznar, C.; Dromer, F. French Mycoses Study Group Epidemiological Investigation for Grouped Cases of Trichosporon Asahii Using Whole Genome and IGS1 Sequencing. Mycoses 2020, 63, 942–951. [Google Scholar] [CrossRef]
- McManus, E.J.; Jones, J.M. Detection of a Trichosporon beigelii Antigen Cross-Reactive with Cryptococcus neoformans Capsular Polysaccharide in Serum from a Patient with Disseminated Trichosporon Infection. J. Clin. Microbiol. 1985, 21, 681–685. [Google Scholar] [CrossRef] [Green Version]
- Melcher, G.P.; Reed, K.D.; Rinaldi, M.G.; Lee, J.W.; Pizzo, P.A.; Walsh, T.J. Demonstration of a Cell Wall Antigen Cross-Reacting with Cryptococcal Polysaccharide in Experimental Disseminated Trichosporonosis. J. Clin. Microbiol. 1991, 29, 192–196. [Google Scholar] [CrossRef] [Green Version]
- Shimazu, K.; Ando, M.; Sakata, T.; Yoshida, K.; Araki, S. Hypersensitivity Pneumonitis Induced by Trichosporon cutaneum. Am. Rev. Respir. Dis. 1984, 130, 407–411. [Google Scholar] [CrossRef]
- Gökahmetoğlu, S.; Nedret Koç, A.; Nas, H. Case Reports. Isolation of Two Trichosporon cutaneum Strains from Urine. Mycoses 2002, 45, 132–134. [Google Scholar] [CrossRef]
- Campbell, C.K.; Payne, A.L.; Teall, A.J.; Brownell, A.; Mackenzie, D.W. Cryptococcal Latex Antigen Test Positive in Patient with Trichosporon Beigelii Infection. Lancet 1985, 2, 43–44. [Google Scholar] [CrossRef]
- Kobayashi, M.; Kotani, S.; Fujishita, M.; Taguchi, H.; Moriki, T.; Enzan, H.; Miyoshi, I. Immunohistochemical Identification of Trichosporon Beigelii in Histologic Section by Immunoperoxidase Method. Am. J. Clin. Pathol. 1988, 89, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Surmont, I.; Vergauwen, B.; Marcelis, L.; Verbist, L.; Verhoef, G.; Boogaerts, M. First Report of Chronic Meningitis Caused by Trichosporon Beigelii. Eur. J. Clin. Microbiol. Infect. Dis. 1990, 9, 226–229. [Google Scholar] [CrossRef]
- Walsh, T.J.; Melcher, G.P.; Rinaldi, M.G.; Lecciones, J.; McGough, D.A.; Kelly, P.; Lee, J.; Callender, D.; Rubin, M.; Pizzo, P.A. Trichosporon Beigelii, an Emerging Pathogen Resistant to Amphotericin B. J. Clin. Microbiol. 1990, 28, 1616–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, M.P.; Nguyen, T.T.; Parkes, L.O.; Dufresne, P.J.; Sheppard, D.C. Cross-Reacting Ustilago Maydis Causing False-Positive Cryptococcal Antigen Test Results. J. Clin. Microbiol. 2017, 55, 3135–3137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karigane, D.; Sakurai, M.; Matsuyama, E.; Ide, K.; Yamamoto-Takeuchi, S.; Inazumi, T.; Kohashi, S. Successful Treatment of Breakthrough Disseminated Trichosporon Asahii Fungemia in a Patient with Acute Myeloid Leukemia Receiving Itraconazole Prophylaxis. Med. Mycol. Case Rep. 2018, 20, 1–3. [Google Scholar] [CrossRef]
- Fekkar, A.; Brun, S.; D’Ussel, M.; Uzunov, M.; Cracco, C.; Dhédin, N.; Buffet, P.; Mazier, D.; Datry, A. Serum Cross-Reactivity with Aspergillus Galactomannan and Cryptococcal Antigen during Fatal Disseminated Trichosporon Dermatis Infection. Clin. Infect. Dis. 2009, 49, 1457–1458. [Google Scholar] [CrossRef] [Green Version]
- Lyman, C.A.; Devi, S.J.; Nathanson, J.; Frasch, C.E.; Pizzo, P.A.; Walsh, T.J. Detection and Quantitation of the Glucuronoxylomannan-like Polysaccharide Antigen from Clinical and Nonclinical Isolates of Trichosporon Beigelii and Implications for Pathogenicity. J. Clin. Microbiol. 1995, 33, 126–130. [Google Scholar] [CrossRef] [Green Version]
- Arendrup, M.C.; Boekhout, T.; Akova, M.; Meis, J.F.; Cornely, O.A.; Lortholary, O. European Society of Clinical Microbiology and Infectious Diseases Fungal Infection Study Group; European Confederation of Medical Mycology ESCMID and ECMM Joint Clinical Guidelines for the Diagnosis and Management of Rare Invasive Yeast Infections. Clin. Microbiol. Infect. 2014, 20 (Suppl. S3), 76–98. [Google Scholar] [CrossRef] [Green Version]
- Pfaller, M.A.; Messer, S.A.; Woosley, L.N.; Jones, R.N.; Castanheira, M. Echinocandin and Triazole Antifungal Susceptibility Profiles for Clinical Opportunistic Yeast and Mold Isolates Collected from 2010 to 2011: Application of New CLSI Clinical Breakpoints and Epidemiological Cutoff Values for Characterization of Geographic and Temporal Trends of Antifungal Resistance. J. Clin. Microbiol. 2013, 51, 2571–2581. [Google Scholar] [CrossRef] [Green Version]
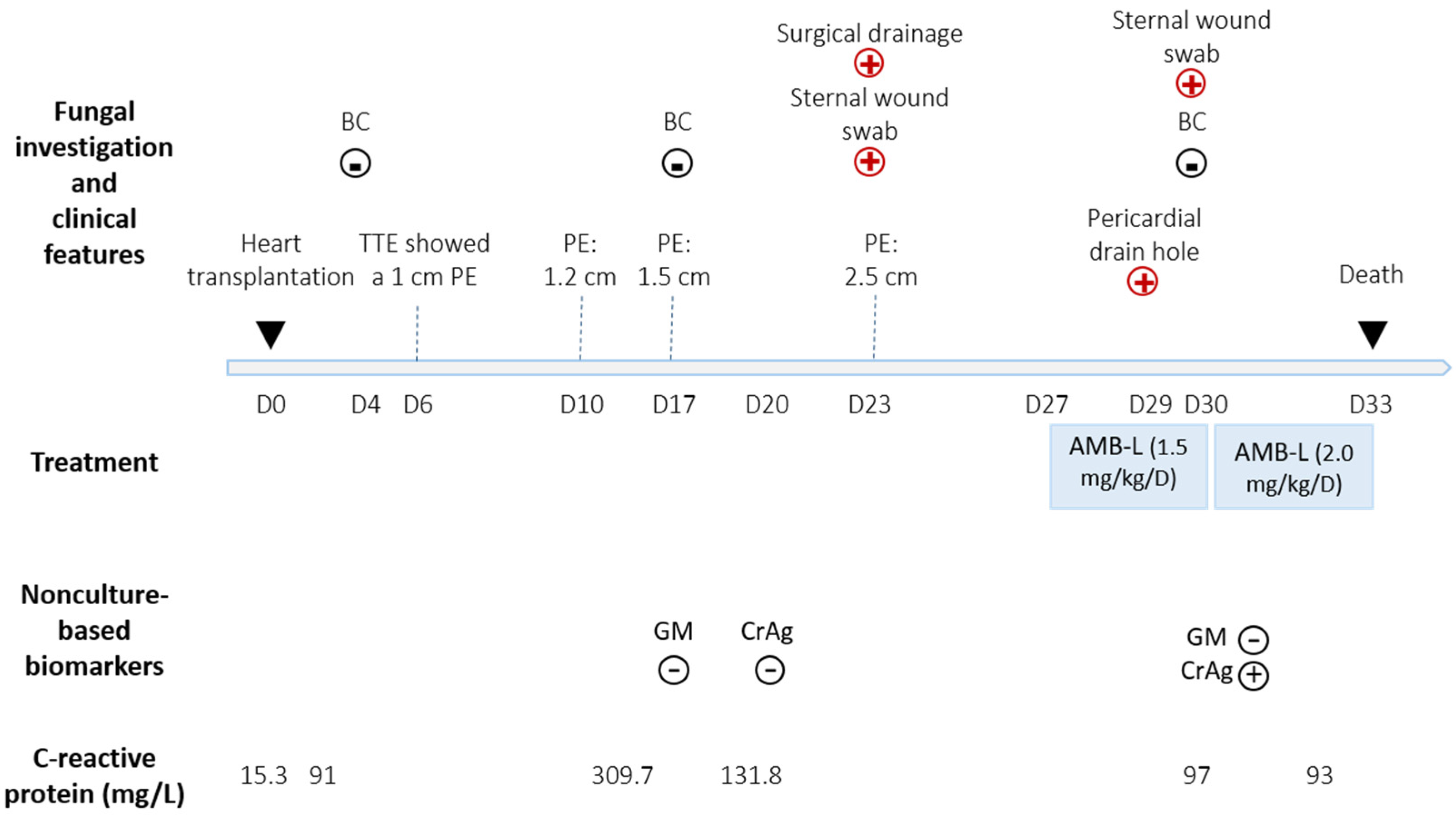
 : positive Trichosporon japonicum culture; ▪: negative Trichosporon japonicum culture.
: positive Trichosporon japonicum culture; ▪: negative Trichosporon japonicum culture.
: positive Trichosporon japonicum culture; ▪: negative Trichosporon japonicum culture.
: positive Trichosporon japonicum culture; ▪: negative Trichosporon japonicum culture.


{kind=link}
{kind=link}
| Age | Gender | Comorbidity Conditions | Clinical Presentation | Site of Positive Culture | Treatment | Outcome | Reference | |
|---|---|---|---|---|---|---|---|---|
| Molecule | Duration | |||||||
| 8 | F | AML | Respiratory distress | Sputum | AMB-L (5 mg/kg/D) + ITRA (100 mg/D) | NS | Death | [9] |
| - | - | - | Hypersensitivity pneumonitis | BALF | - | - | - | [10] |
| 18 | F | Transcutaneous biventricular assist device | Fungemia | Blood, aortic cannula, removed left ventricular apex cuff | AMB-L + 5FC switch VORI | 11 days / 6 weeks | Survival at 2 months | [6] |
| 36 | M | Kidney transplant recipient | Urinary tract infection | Urine | VORI + CASPO | NS | Survival | [8] |
| 50 | M | Kidney transplant recipient | Urinary tract infection | Urine | VORI + CASPO | 15 days | Death | [8] |
| 8 | M | ALL | Fungemia | Blood | AMB (3 mg/kg/D) + VORI (8 mg/kg twice a day) | 11 days | Death | [7] |
| 42 | F | Heart transplant recipient | Pericardial effusion | Pericardial fluid | AMB-L (1.5 mg/kg/D) | 6 days | Death | Present case |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menu, E.; Kabtani, J.; Roubin, J.; Ranque, S.; L’Ollivier, C. Pericardial Effusion Due to Trichosporon japonicum: A Case Report and Review of the Literature. Pathogens 2022, 11, 598. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11050598
Menu E, Kabtani J, Roubin J, Ranque S, L’Ollivier C. Pericardial Effusion Due to Trichosporon japonicum: A Case Report and Review of the Literature. Pathogens. 2022; 11(5):598. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11050598
Chicago/Turabian StyleMenu, Estelle, Jihane Kabtani, Johanna Roubin, Stéphane Ranque, and Coralie L’Ollivier. 2022. "Pericardial Effusion Due to Trichosporon japonicum: A Case Report and Review of the Literature" Pathogens 11, no. 5: 598. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11050598