
Fragmentation of Healthcare Services as a Possible Determinant of the Low Completion for the Tuberculosis Cascade of Prevention among Asylum Seekers: Results from a Prospective Study with Historical Comparison

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Setting and Study Population
2.2. Screening Procedures
2.2.1. Centralized Screening for TBI (June 2018)
2.2.2. Decentralized Screening for TBI (January 2017 to May 2018)—Historical Control
2.3. Preventive Therapy
2.4. Data Analysis
2.5. Ethical Aspects
3. Results
3.1. Subjects Enrolled
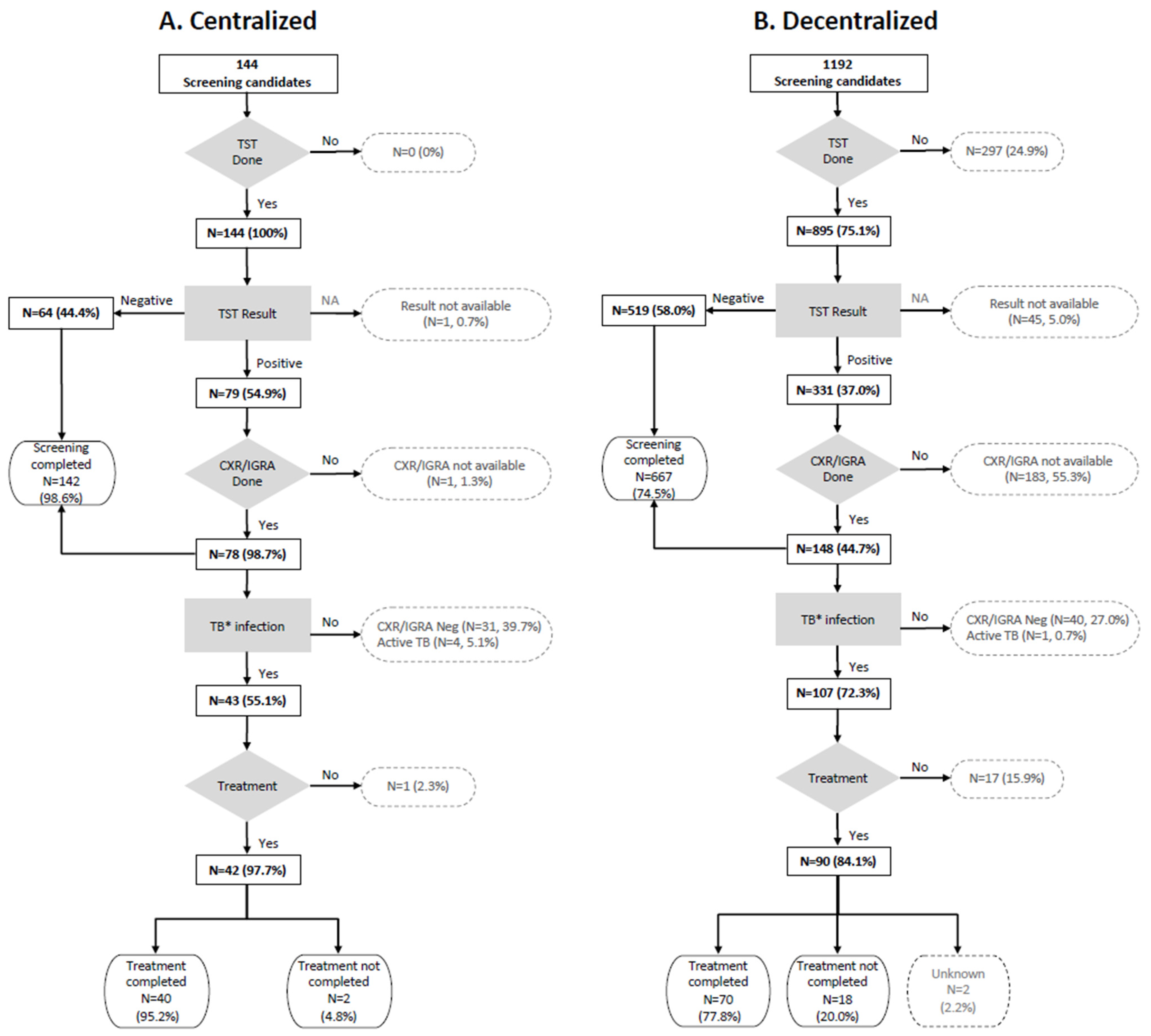
3.2. Screening Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
UNESCO Disclaimer
References
- International Organization for Migration. World Migration Report. 2022. Available online: http://www.iom.int/wmr (accessed on 1 April 2022).
- World Health Organization. Report on the Health of Refugees and Migrants in the WHO European Region. 2018. Available online: https://www.euro.who.int/en/publications/abstracts/report-on-the-health-of-refugees-and-migrants-in-the-who-european-region-no-public-health-without-refugee-and-migrant-health-2018 (accessed on 1 April 2022).
- United Nations High Commissioner for Refugees. Mediterranean Situation. Available online: https://data2.unhcr.org/en/situations/mediterranean (accessed on 1 April 2022).
- European Centre for Disease Prevention and Control. Programmatic Management of Latent Tuberculosis Infection in the European Union. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/October-2018-Programmatic-management-LTBI-EU.pdf (accessed on 1 April 2022).
- World Health Organization. Towards Tuberculosis Elimination: An Action Framework for Low-Incidence Countries 2014. Available online: http://apps.who.int/iris/bitstream/handle/10665/132231/9789241507707_eng.pdf?sequence=1 (accessed on 1 April 2022).
- Lönnroth, K.; Mor, Z.; Erkens, C.; Bruchfeld, J.; Nathavitharana, R.R.; Van Der Werf, M.J.; Lange, C. Tuberculosis in migrants in low-incidence countries: Epidemiology and intervention entry points. Int. J. Tuberc. Lung Dis. 2017, 21, 624–637. [Google Scholar] [CrossRef]
- Kunst, H.; Burman, M.; Arnesen, T.M.; Fiebig, L.; Hergens, M.P.; Kalkouni, O.; Klinkenberg, E.; Orcau, À.; Soini, H.; Sotgiu, G.; et al. Tuberculosis and latent tuberculous infection screening of migrants in Europe: Comparative analysis of policies, surveillance systems and results. Int. J. Tuberc. Lung Dis. 2017, 21, 840–851. [Google Scholar] [CrossRef] [PubMed]
- Dhavan, P.; Dias, H.M.; Creswell, J.; Weil, D. An overview of tuberculosis and migration. Int. J. Tuberc. Lung Dis. 2017, 21, 610–623. [Google Scholar] [CrossRef] [PubMed]
- Greenaway, C.; Pareek, M.; Abou Chakra, C.N.; Walji, M.; Makarenko, I.; Alabdulkarim, B.; Hogan, C.; McConnell, T.; Scarfo, B.; Christensen, R.; et al. The effectiveness and cost-effectiveness of screening for latent tuberculosis among migrants in the EU/EEA: A systematic review. Eurosurveillance 2018, 23, 17–00543. [Google Scholar] [CrossRef] [PubMed]
- Greenaway, C.; Pareek, M.; Abou Chakra, C.N.; Walji, M.; Makarenko, I.; Alabdulkarim, B.; Hogan, C.; McConnell, T.; Scarfo, B.; Christensen, R.; et al. The effectiveness and cost-effectiveness of screening for active tuberculosis among migrants in the EU/EEA: A systematic review. Eurosurveillance 2018, 23, 17–00542. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Public Health Guidance on Screening and Vaccination for Infectious Diseases in Newly Arrived Migrants within the EU/EEA; ECDC: Stockholm, Sweden, 2018.
- E-DETECT-TB Consortium. Official Website. Available online: https://e-detecttb.eu/ (accessed on 1 April 2022).
- Pontarelli, A.; Marchese, V.; Scolari, C.; Capone, S.; El-Hamad, I.; Donato, F.; Moioli, R.; Girardi, E.; Cirillo, D.M.; Castelli, F.; et al. Screening for active and latent tuberculosis among asylum seekers in Italy: A retrospective cohort analysis. Travel Med. Infect. Dis. 2019, 27, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Italian National Health Statistics (ISTAT). Annuario Statistico Italiano. 2021. Available online: https://www.istat.it/it/archivio/264305 (accessed on 7 May 2022).
- Lombardy Region. Aggiornamenti su Prevenzione Dell’infezione, Sorveglianza e Controllo della Malattia Tubercolare in Regione Lombardia—2017. [Updates on Prevention, Surveillance and Control of Tuberculosis Infection and Disease in Lombardy Region]. Regional Official Bulletin. 2017. Available online: https://www.regione.lombardia.it/wps/wcm/connect/e8405eb0-2f52-473c-9c9e-2a565a019bae/SEO29_18-07-2017.pdf?MOD=AJPERES&CACHEID=e8405eb0-2f52-473c-9c9e-2a565a019bae (accessed on 1 April 2022).
- Bradby, H.; Humphris, R.; Newall, D.; Phillimore, J. Public Health Aspects of Migrant Health: A Review of the Evidence on Health Status for Refugees and Asylum Seekers in the European Region; Health Evidence Network Synthesis Report 44; WHO Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- Italian Ministry of Interior. Official Website. In Vigore il Decreto Legge Sicurezza e Immigrazione. 2018. Available online: https://www.interno.gov.it/it/notizie/vigore-decreto-legge-sicurezza-e-immigrazione (accessed on 1 April 2022).
- Villa, S.; Codecasa, L.R.; Faccini, M.; Pontello, M.M.; Ferrarese, M.; Castellotti, P.F.; Senatore, S.; Lamberti, A.; Mazzola, E.; Perno, C.F.; et al. Tuberculosis among asylum seekers in Milan, Italy: Epidemiological analysis and evaluation of interventions. Eur. Respir. J. 2019, 54, 1900896. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.G.; Cremers, A.L.; Heuvelings, C.C.; Greve, P.F.; Visser, B.J.; Bélard, S.; Janssen, S.; Spijker, R.; Shaw, B.; Hill, R.A.; et al. Barriers and facilitators to the uptake of tuberculosis diagnostic and treatment services by hard-to-reach populations in countries of low and medium tuberculosis incidence: A systematic review of qualitative literature. Lancet Infect. Dis. 2017, 17, e128–e143. [Google Scholar] [CrossRef]
- Isphording, I.E. What Drives the Language Proficiency of Immigrants; IZA Institute of Labour Economics: Bonn, Germany, 2015; Volume 177, Available online: https://wol.iza.org/uploads/articles/177/pdfs/what-drives-language-proficiency-of-immigrants.pdf (accessed on 1 April 2022).
- Spruijt, I.; Erkens, C.; Suurmond, J.; Huisman, E.; Koenders, M.; Kouw, P.; Toumanian, S.; Cobelens, F.; van den Hof, S. Implementation of latent tuberculosis infection screening and treatment among newly arriving immigrants in the Netherlands: A mixed methods pilot evaluation. PLoS ONE 2019, 14, e0219252. [Google Scholar] [CrossRef] [PubMed]
- Migrants Refugees. Country Profiles. Italy. Available online: https://migrants-refugees.va/country-profile/italy/ (accessed on 1 April 2022).
- Barbiano di Belgiojoso, E. Intentions on desired length of stay among immigrants in Italy. Genus 2016, 72, 1. [Google Scholar] [CrossRef]
- European Council. Migration Flows in the Central Mediterranean Route. Available online: https://www.consilium.europa.eu/en/policies/eu-migration-policy/central-mediterranean-route/ (accessed on 7 May 2022).
- UNHCR. Operational Data Portal, Mediterranean Refugee Situations. Updated 1 May 2022. Available online: https://data2.unhcr.org/en/situations/mediterranean (accessed on 7 May 2022).
- Rustage, K.; Lobe, J.; Hayward, S.E.; Kristensen, K.L.; Margineanu, I.; Stienstra, Y.; Goletti, D.; Zenner, D.; Noori, T.; Pareek, M.; et al. Initiation and completion of treatment for latent tuberculosis infection in migrants globally: A systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 1701–1712. [Google Scholar] [CrossRef]
- Rosano, A.; Dauvrin, M.; Buttigieg, S.C.; Ronda, E.; Tafforeau, J.; Dias, S. Migrant’s access to preventive health services in five EU countries. BMC Health Serv. Res. 2017, 17, 588. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K.; Sharma, A.; Kadhiravan, T.; Tharyan, P. Rifamycins (rifampicin, rifabutin and rifapentine) compared to isoniazid for preventing tuberculosis in HIV-negative people at risk of active TB. Cochrane Rev. J. 2013, 2013, CD007545. [Google Scholar] [CrossRef]
- Shete, P.B.; Boccia, D.; Dhavan, P.; Gebreselassie, N.; Lönnroth, K.; Marks, S.; Matteelli, A.; Posey, D.L.; van der Werf, M.J.; Winston, C.A.; et al. Defining a migrant-inclusive tuberculosis research agenda to end TB. Int. J. Tuberc. Lung Dis. 2018, 22, 835–843. [Google Scholar] [CrossRef]
- Sarivalasis, A.; Zellweger, J.P.; Faouzi, M.; Daher, O.; Deslarzes, C.; Bodenmann, P. Factors associated with latent tuberculosis among asylum seekers in Switzerland: A cross-sectional study in Vaud County. BMC Infect. Dis. 2012, 12, 285. [Google Scholar] [CrossRef] [PubMed]
- Médecins Sans Frontières. Libya International Activity Report. 2019. Available online: https://www.msf.org/libya (accessed on 1 April 2022).
- Barcellini, L.; Borroni, E.; Cimaglia, C.; Girardi, E.; Matteelli, A.; Marchese, V.; Stancanelli, G.; Abubakar, I.; on behalf of the members of the E-Detect TB Consortium; Cirillo, D.M. App-based symptoms screening with Xpert MTB/RIF Ultra assay used for active tuberculosis detection in migrants at point of arrivals in Italy: The E-DETECT TB intervention analysis. PLoS ONE 2019, 14, e0218039. [Google Scholar] [CrossRef] [PubMed]
- Dara, M.; de Colombani, P.; Petrova-Benedict, R.; Centis, R.; Zellweger, J.P.; Sandgren, A.; Heldal, E.; Sotgiu, G.; Jansen, N.; Bahtijarevic, R.; et al. Transborder Migration Task Force. Minimum package for cross-border TB control and care in the WHO European region: A Wolfheze consensus statement. Eur. Respir. J. 2012, 40, 1081–1090. [Google Scholar] [CrossRef] [PubMed]
- Berrocal-Almanza, L.C.; Harris, R.J.; Collin, S.M.; Muzyamba, M.C.; Conroy, O.D.; Mirza, A.; O’Connell, A.M.; Altass, L.; Anderson, S.R.; Thomas, H.L.; et al. Effectiveness of nationwide programmatic testing and treatment for latent tuberculosis infection in migrants in England: A retrospective, population-based cohort study. Lancet Public Health 2022, 7, e305–e315. [Google Scholar] [CrossRef]


{kind=link}
| Centralized Screening | Decentralized Screening | Total | p-Value | |
|---|---|---|---|---|
| N (%) | N (%) | |||
| Total | 144 (10.8) | 1192 (89.2) | 1336 (100) | |
| Gender | ||||
| Male | 125 (86.8) | 1035 (86.8) | 1160 (86.8) | 0.994 |
| Female | 19 (13.2) | 157 (13.2) | 176 (13.2) | |
| Age at arrival (years) | ||||
| ≤20 | 66 (45.8) | 544 (45.6) | 610 (45.7) | 0.964 |
| >20 | 78 (54.2) | 648 (54.4) | 726 (54.3) | |
| Age (years), median (IQR) | 22 (19–27) | 22 (19–26) | 22 (19–26) | 0.342 |
| Area of origin * | ||||
| Sub-Saharan Africa | 134 (93.1) | 857 (71.9) | 991 (74.2) | <0.001 |
| Other | 10 (6.9) | 335 (28.1) | 345 (25.8) | |
| TB incidence in country of origin ^ | ||||
| <150/100,0000 | 56 (38.9) | 460 (38.6) | 516 (38.6) | 0.945 |
| ≥150/100,0000 | 88 (61.1) | 732 (61.4) | 820 (61.4) | |
| Influx period # | ||||
| Low | 28 (19.4) | 82 (6.9) | 110 (8.2) | <0.001 |
| High | 116 (80.6) | 1110 (93.1) | 1226 (91.8) | |
| Semester of arrival | ||||
| 1st 2017 | 56 (38.9) | 92 (77.9) | 985 (73.7) | <0.001 |
| 2nd 2017 | 74 (51.4) | 213 (17.9) | 287 (21.5) | |
| 1st 2018 | 14 (9.7) | 50 (4.2) | 64 (4.8) |
| N. Screening Completed/Tot (809/1336) | aIRR (95% CI) | p-Value | |
|---|---|---|---|
| Screening procedure | |||
| Decentralized | 667/1192 | Ref. | |
| Centralized | 142/144 | 1.78 (1.68–1.88) | <0.001 |
| Gender | |||
| Female | 95/176 | Ref. | |
| Male | 714/1160 | 1.13 (0.98–1.29) | 0.090 |
| Age at arrival, by 5 years increase | 1.00 (0.97–1.02) | 0.741 | |
| TB incidence in country of origin | |||
| <150/100,0000 | 287/516 | Ref. | |
| ≥150/100,0000 | 522/820 | 1.14 (1.04–1.25) | 0.004 |
| Influx period | |||
| Low | 67/110 | Ref. | |
| High | 742/1226 | 1.06 (0.92–1.22) | 0.445 |
| N. TBI/Tot (150/809) | aOR (95% CI) | p-Value | |
|---|---|---|---|
| Gender | |||
| Female | 13/95 | Ref. | |
| Male | 137/714 | 1.56 (0.84–2.91) | 0.163 |
| Age at arrival, by 5 years increase | 1.14 (1.01–1.29) | 0.032 | |
| TB incidence in country of origin | |||
| <150/100,0000 | 53/287 | Ref. | |
| ≥150/100,0000 | 97/522 | 1.02 (0.70–1.49) | 0.907 |
| Screening start | |||
| ≤6 months | 111/675 | Ref. | |
| >6 months | 39/134 | 2.09 (1.36–3.20) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchese, V.; Zanotti, P.; Cimaglia, C.; Rossi, B.; Formenti, B.; Magro, P.; Gulletta, M.; Stancanelli, G.; El-Hamad, I.; Girardi, E.; et al. Fragmentation of Healthcare Services as a Possible Determinant of the Low Completion for the Tuberculosis Cascade of Prevention among Asylum Seekers: Results from a Prospective Study with Historical Comparison. Pathogens 2022, 11, 613. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11060613
Marchese V, Zanotti P, Cimaglia C, Rossi B, Formenti B, Magro P, Gulletta M, Stancanelli G, El-Hamad I, Girardi E, et al. Fragmentation of Healthcare Services as a Possible Determinant of the Low Completion for the Tuberculosis Cascade of Prevention among Asylum Seekers: Results from a Prospective Study with Historical Comparison. Pathogens. 2022; 11(6):613. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11060613
Chicago/Turabian StyleMarchese, Valentina, Paola Zanotti, Claudia Cimaglia, Benedetta Rossi, Beatrice Formenti, Paola Magro, Maurizio Gulletta, Giovanna Stancanelli, Issa El-Hamad, Enrico Girardi, and et al. 2022. "Fragmentation of Healthcare Services as a Possible Determinant of the Low Completion for the Tuberculosis Cascade of Prevention among Asylum Seekers: Results from a Prospective Study with Historical Comparison" Pathogens 11, no. 6: 613. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11060613