Correlation of Feline Coronavirus Shedding in Feces with Coronavirus Antibody Titer



 ,
,
Abstract
:1. Introduction
2. Results
2.1. Correlation between Mean Fecal FCoV Load and Antibody Titer
2.2. Correlation between Frequency of Fecal FCoV Shedding and Antibody Titer and Mean Fecal FCoV Load
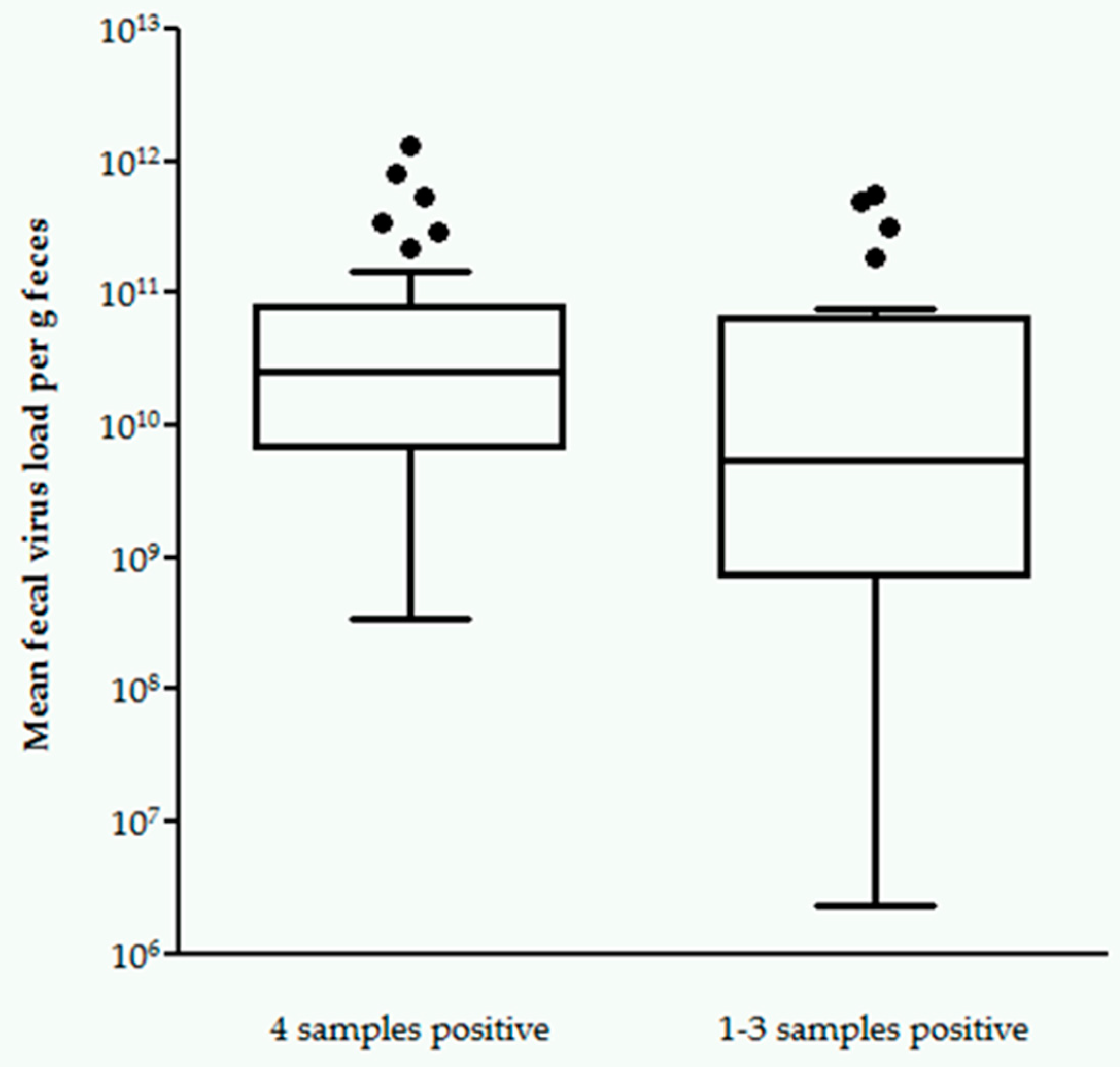
2.3. Correlation between FCoV Shedding in All Four vs. One to Three Samples and Antibody Titer
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Addie, D.D.; Dennis, J.M.; Toth, S.; Callanan, J.J.; Reid, S.; Jarrett, O. Long-term impact on a closed household of pet cats of natural infection with feline coronavirus, feline leukaemia virus and feline immunodeficiency virus. Vet. Rec. 2000, 146, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Foley, J.E.; Poland, A.; Carlson, J.; Pedersen, N.C. Risk factors for feline infectious peritonitis among cats in multiple-cat environments with endemic feline enteric coronavirus. J. Am. Vet. Med. Assoc. 1997, 210, 1313–1318. [Google Scholar] [PubMed]
- Pedersen, N.C.; Allen, C.E.; Lyons, L.A. Pathogenesis of feline enteric coronavirus infection. J. Feline Med. Surg. 2008, 10, 529–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, F.W. Update on FIP. In Proceedings of the 12th Annual Kal Kan Symposium for the Treatment of Small Animal Disease, Johnson, OH, USA, 16–17 October 1988; pp. 43–47. [Google Scholar]
- Cave, T.A.; Golder, M.C.; Simpson, J.; Addie, D.D. Risk factors for feline coronavirus seropositivity in cats relinquished to a UK rescue charity. J. Feline Med. Surg. 2004, 6, 53–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Addie, D.D. Clustering of feline coronaviruses in multicat households. Vet. J. 2000, 159, 8–9. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, N.C.; Sato, R.; Foley, J.E.; Poland, A.M. Common virus infections in cats, before and after being placed in shelters, with emphasis on feline enteric coronavirus. J. Feline Med. Surg. 2004, 6, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Addie, D.D.; Toth, S.; Murray, G.D.; Jarrett, O. Risk of feline infectious peritonitis in cats naturally infected with feline coronavirus. Am. J. Vet. Res. 1995, 56, 429–434. [Google Scholar]
- Poland, A.M.; Vennema, H.; Foley, J.E.; Pedersen, N.C. Two related strains of feline infectious peritonitis virus isolated from immunocompromised cats infected with a feline enteric coronavirus. J. Clin. Microbiol. 1996, 34, 3180–3184. [Google Scholar] [CrossRef]
- Vennema, H.; Poland, A.; Foley, J.; Pedersen, N.C. Feline infectious peritonitis viruses arise by mutation from endemic feline enteric coronaviruses. Virology 1998, 243, 150–157. [Google Scholar] [CrossRef] [Green Version]
- Kipar, A.; May, H.; Menger, S.; Weber, M.; Leukert, W.; Reinacher, M. Morphologic features and development of granulomatous vasculitis in feline infectious peritonitis. Vet. Pathol. 2005, 42, 321–330. [Google Scholar] [CrossRef]
- Kipar, A.; Meli, M.L.; Failing, K.; Euler, T.; Gomes-Keller, M.A.; Schwartz, D.; Lutz, H.; Reinacher, M. Natural feline coronavirus infection: Differences in cytokine patterns in association with the outcome of infection. Vet. Immunol. Immunopathol. 2006, 112, 141–155. [Google Scholar] [CrossRef] [PubMed]
- Acar, D.D.; Olyslaegers, D.A.; Dedeurwaerder, A.; Roukaerts, I.D.; Baetens, W.; Van Bockstael, S.; De Gryse, G.M.; Desmarets, L.M.; Nauwynck, H.J. Upregulation of endothelial cell adhesion molecules characterizes veins close to granulomatous infiltrates in the renal cortex of cats with feline infectious peritonitis and is indirectly triggered by feline infectious peritonitis virus-infected monocytes in vitro. J. Gen. Virol. 2016, 97, 2633–2642. [Google Scholar]
- Takano, T.; Azuma, N.; Satoh, M.; Toda, A.; Hashida, Y.; Satoh, R.; Hohdatsu, T. Neutrophil survival factors (TNF-alpha, GM-CSF, and G-CSF) produced by macrophages in cats infected with feline infectious peritonitis virus contribute to the pathogenesis of granulomatous lesions. Arch. Virol. 2009, 154, 775–781. [Google Scholar] [CrossRef]
- Takano, T.; Hohdatsu, T.; Hashida, Y.; Kaneko, Y.; Tanabe, M.; Koyama, H. A “possible” involvement of TNF-alpha in apoptosis induction in peripheral blood lymphocytes of cats with feline infectious peritonitis. Vet. Microbiol. 2007, 119, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Takano, T.; Hohdatsu, T.; Toda, A.; Tanabe, M.; Koyama, H. TNF-alpha, produced by feline infectious peritonitis virus (FIPV)-infected macrophages, upregulates expression of type II FIPV receptor feline aminopeptidase N in feline macrophages. Virology 2007, 364, 64–72. [Google Scholar] [CrossRef] [Green Version]
- Addie, D.D.; Toth, S.; Herrewegh, A.A.; Jarrett, O. Feline coronavirus in the intestinal contents of cats with feline infectious peritonitis. Vet. Rec. 1996, 139, 522–523. [Google Scholar] [CrossRef]
- Meli, M.; Kipar, A.; Muller, C.; Jenal, K.; Gonczi, E.; Borel, N.; Gunn-Moore, D.; Chalmers, S.; Lin, F.; Reinacher, M.; et al. High viral loads despite absence of clinical and pathological findings in cats experimentally infected with feline coronavirus (FCoV) type I and in naturally FCoV-infected cats. J. Feline Med. Surg. 2004, 6, 69–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, E.N.; Stranieri, A.; Helps, C.R.; Porter, E.L.; Davidson, A.D.; Day, M.J.; Knowles, T.; Kipar, A.; Tasker, S. Limitations of using feline coronavirus spike protein gene mutations to diagnose feline infectious peritonitis. Vet. Res. 2017, 48, 60. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, N.C.; Liu, H.; Scarlett, J.; Leutenegger, C.M.; Golovko, L.; Kennedy, H.; Kamal, F.M. Feline infectious peritonitis: Role of the feline coronavirus 3c gene in intestinal tropism and pathogenicity based upon isolates from resident and adopted shelter cats. Virus Res. 2012, 165, 17–28. [Google Scholar] [CrossRef]
- Desmarets, L.M.; Vermeulen, B.L.; Theuns, S.; Conceicao-Neto, N.; Zeller, M.; Roukaerts, I.D.; Acar, D.D.; Olyslaegers, D.A.; Van Ranst, M.; Matthijnssens, J.; et al. Experimental feline enteric coronavirus infection reveals an aberrant infection pattern and shedding of mutants with impaired infectivity in enterocyte cultures. Sci. Rep. 2016, 6, 20022. [Google Scholar] [CrossRef]
- Addie, D.D.; Schaap, I.A.; Nicolson, L.; Jarrett, O. Persistence and transmission of natural type I feline coronavirus infection. J. Gen. Virol. 2003, 84, 2735–2744. [Google Scholar] [CrossRef] [PubMed]
- Vogel, L.; Van der Lubben, M.; Te Lintelo, E.G.; Bekker, C.P.; Geerts, T.; Schuijff, L.S.; Grinwis, G.C.; Egberink, H.F.; Rottier, P.J. Pathogenic characteristics of persistent feline enteric coronavirus infection in cats. Vet. Res. 2010, 41, 71–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, N.C.; Eckstrand, C.; Liu, H.; Leutenegger, C.; Murphy, B. Levels of feline infectious peritonitis virus in blood, effusions, and various tissues and the role of lymphopenia in disease outcome following experimental infection. Vet. Microbiol. 2015, 175, 157–166. [Google Scholar] [CrossRef]
- Vennema, H.; de Groot, R.J.; Harbour, D.A.; Dalderup, M.; Gruffydd-Jones, T.; Horzinek, M.C.; Spaan, W.J. Early death after feline infectious peritonitis virus challenge due to recombinant vaccinia virus immunization. J. Virol. 1990, 64, 1407–1409. [Google Scholar] [CrossRef] [Green Version]
- Takano, T.; Kawakami, C.; Yamada, S.; Satoh, R.; Hohdatsu, T. Antibody-dependent enhancement occurs upon re-infection with the identical serotype virus in feline infectious peritonitis virus infection. J. Vet. Med. Sci. 2008, 70, 1315–1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, R.C.; Scott, F.W. Antibody-mediated enhancement of disease in feline infectious peritonitis: Comparisons with dengue hemorrhagic fever. Comp. Immunol. Microbiol. Infect. Dis. 1981, 4, 175–189. [Google Scholar] [CrossRef]
- Hohdatsu, T.; Yamada, M.; Tominaga, R.; Makino, K.; Kida, K.; Koyama, H. Antibody-dependent enhancement of feline infectious peritonitis virus infection in feline alveolar macrophages and human monocyte cell line U937 by serum of cats experimentally or naturally infected with feline coronavirus. J. Vet. Med Sci. 1998, 60, 49–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornelissen, E.; Dewerchin, H.L.; Van Hamme, E.; Nauwynck, H.J. Absence of surface expression of feline infectious peritonitis virus (FIPV) antigens on infected cells isolated from cats with FIP. Vet. Microbiol. 2007, 121, 131–137. [Google Scholar] [CrossRef]
- Addie, D.D.; Jarrett, O. A study of naturally occurring feline coronavirus infections in kittens. Vet. Rec. 1992, 130, 133–137. [Google Scholar] [CrossRef]
- Addie, D.D.; Jarrett, O. Use of a reverse-transcriptase polymerase chain reaction for monitoring the shedding of feline coronavirus by healthy cats. Vet. Rec. 2001, 148, 649–653. [Google Scholar] [CrossRef]
- Foley, J.E.; Poland, A.; Carlson, J.; Pedersen, N.C. Patterns of feline coronavirus infection and fecal shedding from cats in multiple-cat environments. J. Am. Vet. Med. Assoc. 1997, 210, 1307–1312. [Google Scholar] [PubMed]
- Addie, D.; Jarrett, O. Control of feline coronavirus infections in breeding catteries by serotesting, isolation, and early weaning. Feline Pract. 1995, 23, 92–95. [Google Scholar]
- Harpold, L.M.; Legendre, A.M.; Kennedy, M.A.; Plummer, P.J.; Millsaps, K.; Rohrbach, B. Fecal shedding of feline coronavirus in adult cats and kittens in an Abyssinian cattery. J. Am. Vet. Med. Assoc. 1999, 215, 948–951. [Google Scholar] [PubMed]
- Addie, D.D.; Jarrett, O. Feline coronavirus antibodies in cats. Vet. Rec. 1992, 131, 202–203. [Google Scholar] [CrossRef] [PubMed]
- Rohner-Mächler, M. Bestimmung der Ausscheidungskinetik von Felinen Coronaviren unter Feldbedingungen. In Inaugural-Dissertation; University of Zurich: Zurich, Switzerland, 1999. [Google Scholar]
- Murphy, B.G.; Perron, M.; Murakami, E.; Bauer, K.; Park, Y.; Eckstrand, C.; Liepnieks, M.; Pedersen, N.C. The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies. Vet. Microbiol. 2018, 219, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, N.C.; Perron, M.; Bannasch, M.; Montgomery, E.; Murakami, E.; Liepnieks, M.; Liu, H. Efficacy and safety of the nucleoside analog GS-441524 for treatment of cats with naturally occurring feline infectious peritonitis. J. Feline Med. Surg. 2019, 21, 271–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Addie, D.D.; Curran, S.; Bellini, F.; Crowe, B.; Sheehan, E.; Ukrainchuk, L.; Decaro, N. Oral Mutian®X stopped faecal feline coronavirus shedding by naturally infected cats. Res. Vet. Sci. 2020, 130, 222–229. [Google Scholar] [CrossRef]
- Dickinson, P.J.; Bannasch, M.; Thomasy, S.M.; Murthy, V.D.; Vernau, K.M.; Liepnieks, M.; Montgomery, E.; Knickelbein, K.E.; Murphy, B.; Pedersen, N.C. Antiviral treatment using the adenosine nucleoside analogue GS-441524 in cats with clinically diagnosed neurological feline infectious peritonitis. J. Vet. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Addie, D.D.; Belák, S.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; Hartmann, K.; Hofmann-Lehmann, R.; Hosie, M.J.; Lloret, A.; et al. Feline Infectious Peritonitis. Available online: http://www.abcdcatsvets.org/feline-infectious-peritonitis/ (accessed on 26 March 2020).
- Hickman, M.A.; Morris, J.G.; Rogers, Q.R.; Pedersen, N.C. Elimination of feline coronavirus infection from a large experimental specific pathogen-free cat breeding colony by serologic testing and isolation. Feline Pract. 1995, 23, 96–102. [Google Scholar]
- Addie, D.D.; McDonald, M.; Audhuy, S.; Burr, P.; Hollins, J.; Kovacic, R.; Lutz, H.; Luxton, Z.; Mazar, S.; Meli, M.L. Quarantine protects Falkland Islands (Malvinas) cats from feline coronavirus infection. J. Feline Med. Surg. 2012, 14, 171–176. [Google Scholar] [CrossRef] [Green Version]
- Kass, P.H.; Dent, T.H. The epidemiology of feline infectious peritonitis in catteries. Feline Pract. 1995, 23, 27–32. [Google Scholar]
- Addie, D.D.; Jarrett, O. Control of feline coronavirus infection in kittens. Vet. Rec. 1990, 126, 164. [Google Scholar] [PubMed]
- Addie, D.D.; Paltrinieri, S.; Pedersen, N.C. Recommendations from workshops of the second international feline coronavirus/feline infectious peritonitis symposium. J. Feline Med. Surg. 2004, 6, 125–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrewegh, A.A.; Mahler, M.; Hedrich, H.J.; Haagmans, B.L.; Egberink, H.F.; Horzinek, M.C.; Rottier, P.J.; de Groot, R.J. Persistence and evolution of feline coronavirus in a closed cat-breeding colony. Virology 1997, 234, 349–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gut, M.; Leutenegger, C.M.; Huder, J.B.; Pedersen, N.C.; Lutz, H. One-tube fluorogenic reverse transcription-polymerase chain reaction for the quantitation of feline coronaviruses. J. Virol. Methods 1999, 77, 37–46. [Google Scholar] [CrossRef]
- Lutz, H.; Hauser, B.; Horzinek, M. On the serological diagnosis of feline infectious peritonitis. Prakt. Tierarzt 1984, 65, 406–408. [Google Scholar]
- Osterhaus, A.D.M.E.; Horzinek, M.C.; Reynolds, D.J. Seroepidemiology of feline infectious peritonitis virus-infections using transmissible gastroenteritis virus as antigen. Zent. Vet. Reihe B 1977, 24, 835–841. [Google Scholar] [CrossRef]
- Brunner, C.; Kanellos, T.; Meli, M.L.; Sutton, D.J.; Gisler, R.; Gomes-Keller, M.A.; Hofmann-Lehmann, R.; Lutz, H. Antibody induction after combined application of an adjuvanted recombinant FeLV vaccine and a multivalent modified live virus vaccine with a chlamydial component. Vaccine 2006, 24, 1838–1846. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Antibody Titer | Number of Cats | Fecal FCoV Load |
|---|---|---|
| Negative | 8 | 2.2 × 106–5.0 × 1011 (median 2.6 × 109) |
| 1:25 | 20 | 6.4 × 106–8.0 × 1011 (median 1.3 × 1010) |
| 1:100 | 21 | 7.4 × 108–1.3 × 1012 (median 1.2 × 1010) |
| 1:400 | 8 | 3.4 × 108–2.9 × 1011 (median 2.0 × 1010) |
| 1:1600 | 0 | n. a. |
| Shedding Frequency | Number of Cats | Fecal FCoV Load |
|---|---|---|
| One sample RT-qPCR-positive | 9 | 2.2 × 106–3.1 × 1011 (median 5.2 × 109) |
| Two samples RT-qPCR-positive | 6 | 5.1 × 108–4.9 × 1011 (median 3.7 × 109) |
| Three samples RT-qPCR-positive | 5 | 2.5 × 109–5.5 × 1011 (median 1.1 × 1010) |
| Four samples RT-qPCR-positive | 37 | 3.4 × 108–1.3 × 1012 (median 2.5 × 1010) |
| Antibody Titer | Continuous Shedders (% of total) | Non-Continuous Shedders (% of total) | Total Shedding Cats |
|---|---|---|---|
| Negative | 2 (22%) | 7 (78%) | 9 |
| 1:25 | 12 (63%) | 7 (37%) | 19 |
| 1:100 | 15 (68%) | 7 (32%) | 22 |
| 1:400 | 8 (100%) | 0 (0%) | 8 |
| Total | 37 (64%) | 21 (36%) | 58 |
| Ct Value | Result |
| <40 | Positive |
| >40 | Weak positive (RT-qPCR had to be repeated in duplicate) |
| No Ct | Negative |
| Ct Value in Duplicate Repetitive Analysis | Result |
| 1× < 40 and 1× > 40 | Positive |
| 2× > 40 | Weak positive 1 |
| 1× < 40 and 1× no Ct | Questionable positive |
| 1× > 40 and 1× no Ct | Below the limit of quantification |
| 2× no Ct | Negative |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Felten, S.; Klein-Richers, U.; Hofmann-Lehmann, R.; Bergmann, M.; Unterer, S.; Leutenegger, C.M.; Hartmann, K. Correlation of Feline Coronavirus Shedding in Feces with Coronavirus Antibody Titer. Pathogens 2020, 9, 598. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9080598
Felten S, Klein-Richers U, Hofmann-Lehmann R, Bergmann M, Unterer S, Leutenegger CM, Hartmann K. Correlation of Feline Coronavirus Shedding in Feces with Coronavirus Antibody Titer. Pathogens. 2020; 9(8):598. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9080598
Chicago/Turabian StyleFelten, Sandra, Ute Klein-Richers, Regina Hofmann-Lehmann, Michèle Bergmann, Stefan Unterer, Christian M. Leutenegger, and Katrin Hartmann. 2020. "Correlation of Feline Coronavirus Shedding in Feces with Coronavirus Antibody Titer" Pathogens 9, no. 8: 598. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9080598