
Understanding the Role of Duration of Vaccine Protection with MenAfriVac: Simulating Alternative Vaccination Strategies


Abstract
:1. Introduction
2. Materials and Methods
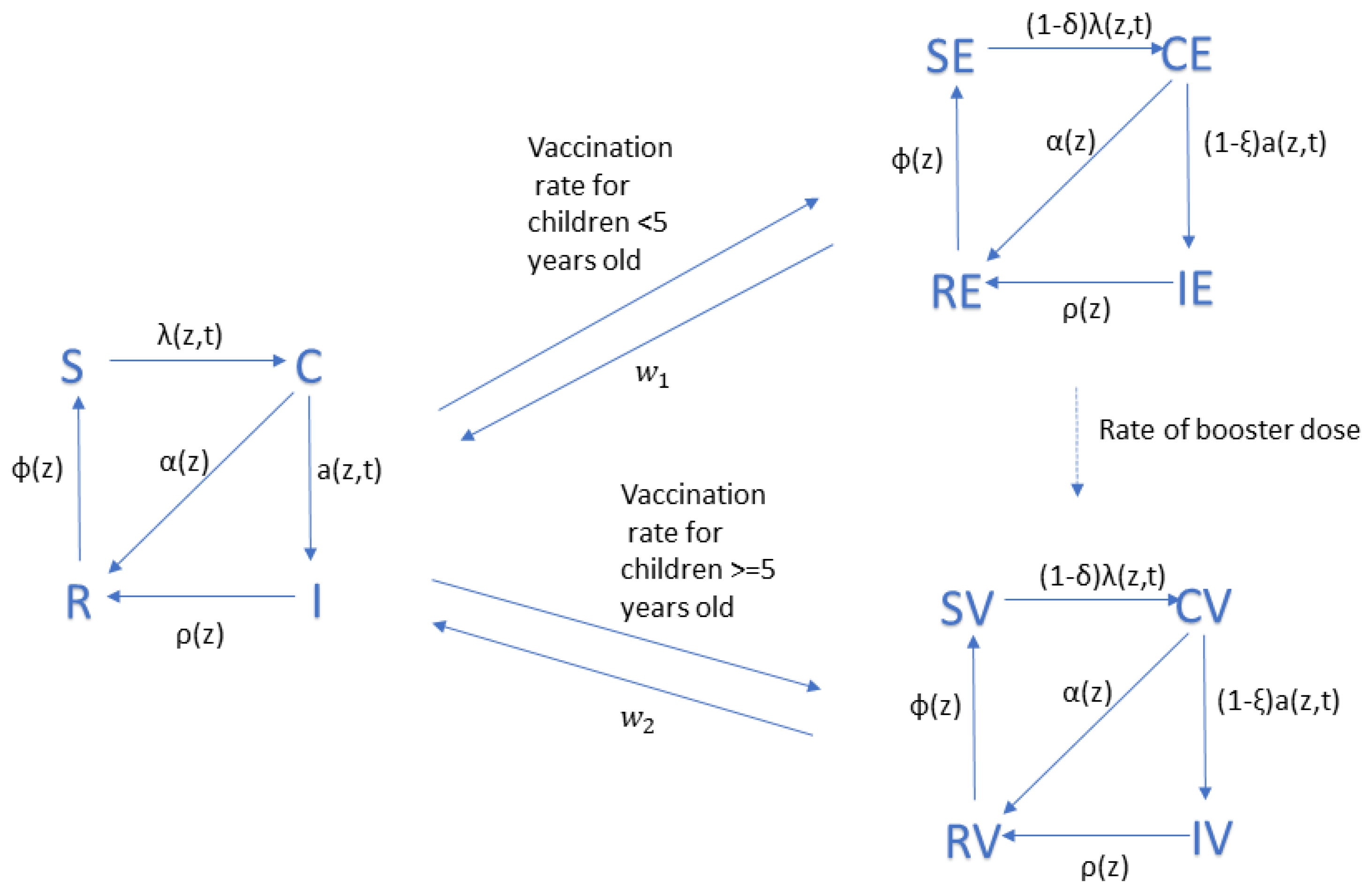
2.1. Model Structure
2.2. Model Parameters
2.3. Vaccination Strategies
2.4. Model Implementation
3. Results
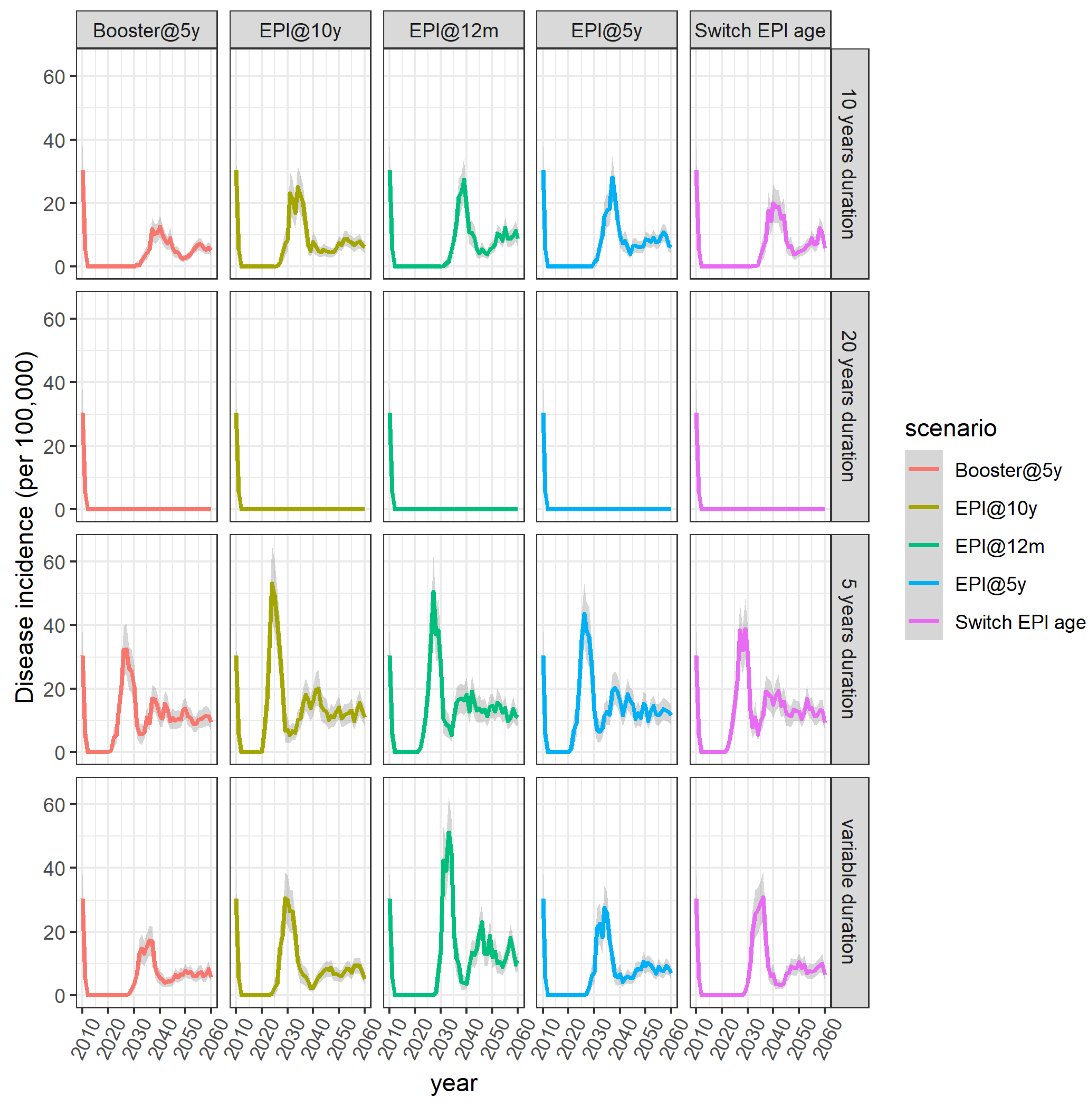
3.1. Baseline Scenario (10 Years Duration of Protection)
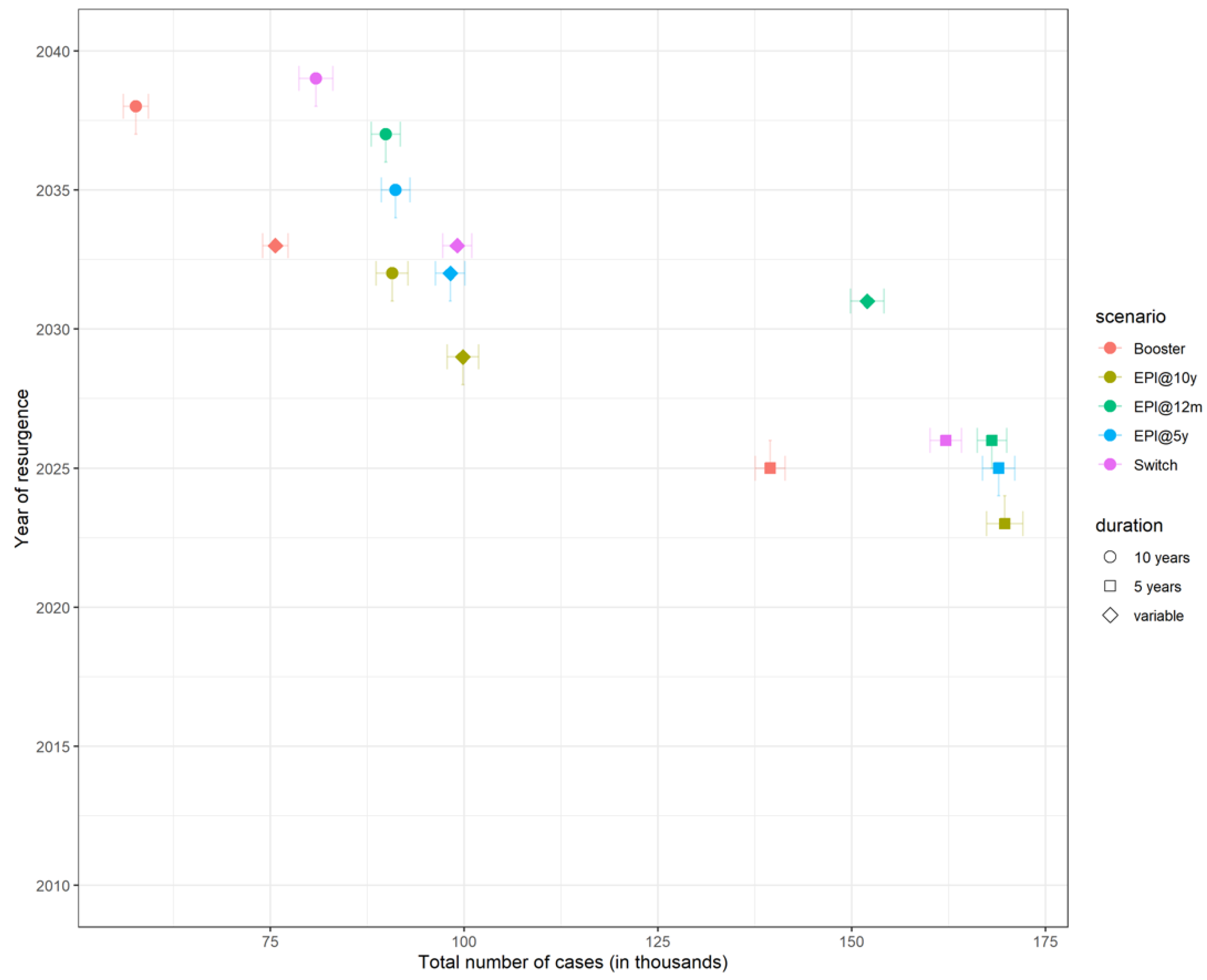
3.2. Time to Resurgence
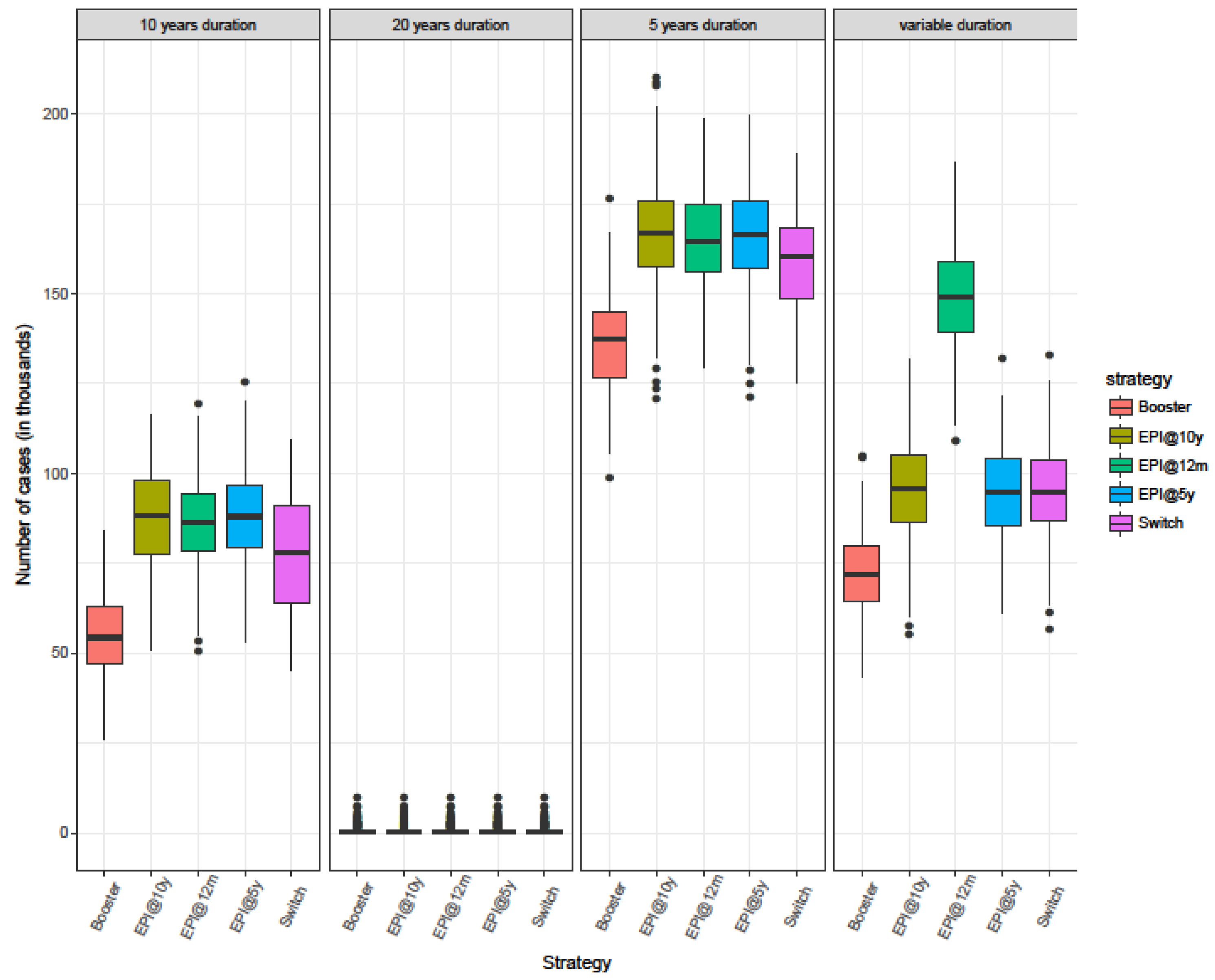
3.3. Burden of Disease
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compartment Name | Definition |
|---|---|
| S | Susceptible individuals not vaccinated |
| C | Carriers of NmA not vaccinated |
| I | Individuals with invasive disease not vaccinated |
| R | Immune after colonization or disease not vaccinated |
| SE | Susceptible individuals vaccinated before the age of 5 years |
| CE | Carriers of NmA vaccinated before the age of 5 years |
| IE | Diseased individuals vaccinated before the age of 5 years |
| RE | Immune after colonization or disease vaccinated before the age of 5 years |
| SV | Susceptible individuals vaccinated after the age of 5 years |
| CV | Carriers of NmA vaccinated after the age of 5 years |
| IV | Diseased individuals vaccinated after the age of 5 years |
| RV | Immune after colonization or disease vaccinated after the age of 5 years |

Appendix B
| Outcome | No Vaccination | EPI@12m | EPI@5y | EPI@10y | Switch | Booster |
|---|---|---|---|---|---|---|
| Total number of cases (in thousands) | 260.7 (258–263.4) | 86.3 (84.6–88.1) | 87.6 (85.8–89.3) | 87.1 (85.1–89.2) | 77.3 (75.1–79.5) | 54.1 (52.5–55.6) |
| Cases averted (in thousands) | - | 174.4 (171.8–176.9) | 173.1 (170.7–175.5) | 173.5 (171.1–176) | 183.4 (181–185.8) | 206.6 (204.3–209) |
| % of cases averted | - | 66.8 (66.2–67.4) | 66.4 (65.8–67) | 66.6 (65.9–67.2) | 70.4 (69.7–71.1) | 79.3 (78.7–79.8) |
| Year of resurgence | - | 2032 | 2030 | 2027 | 2034 | 2031 |
| Total number of doses given (in millions) | - | 42.03 | 33.87 | 30.02 | 39.96 | 63.88 |
| NNV | - | 241 | 196 | 173 | 218 | 309 |
| Duration of Protection | 11 Years | 12 Years | 13 Years | 14 Years | 15 Years | 16 Years | 17 Years | 18 Years * |
|---|---|---|---|---|---|---|---|---|
| Minimum | 2033 | 2035 | 2037 | 2040 | 2044 | 2047 | 2056 | - |
| 1st Quartile | 2038 | 2041 | 2044 | 2048 | 2053 | 2053 | 2057 | - |
| Median | 2040 | 2043 | 2047 | 2051 | 2056 | 2057 | 2058 | - |
| Mean | 2040 | 2043 | 2047 | 2051 | 2055 | 2056 | 2058 | - |
| 3rd Quartile | 2042 | 2045 | 2049 | 2054 | 2058 | 2059 | 2058 | - |
| Maximum | 2049 | 2054 | 2059 | 2060 | 2060 | 2060 | 2060 | - |
| # of runs leading to elimination | 0 | 0 | 0 | 3 | 58 | 139 | 195 | 200 |
| % of runs leading to elimination | 0 | 0 | 0 | 1.5 | 29 | 69.5 | 97.5 | 100 |
References
- Greenwood, B. Meningococcal meningitis in Africa. Trans. R. Soc. Trop. Med. Hyg. 1999, 93, 341–353. [Google Scholar] [CrossRef]
- Lingani, C.; Bergeron-Caron, C.; Stuart, J.M.; Fernandez, K.; Djingarey, M.H.; Ronveaux, O.; Schnitzler, J.C.; Perea, W.A. Meningococcal Meningitis Surveillance in the African Meningitis Belt, 2004–2013. Clin. Infect. Dis. 2015, 61, S410–S415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trotter, C.L.; Lingani, C.; Fernandez, K.; Cooper, L.V.; Bita, A.; Tevi-Benissan, C.; Ronveaux, O.; Marie-Pierre, P.; Stuart, J.M. Impact of MenAfriVac in nine countries of the African meningitis belt, 2010–2015: An analysis of surveillance data. Lancet Infect. Dis. 2017, 17, 867–872. [Google Scholar] [CrossRef] [Green Version]
- Karachaliou, A.; Conlan, A.J.K.; Preziosi, M.-P.; Trotter, C.L. Modeling Long-term Vaccination Strategies with MenAfriVac in the African Meningitis Belt. Clin. Infect. Dis. 2015, 61 (Suppl. 5), S594–S600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Meningococcal A conjugate vaccine: Updated guidance, February 2015. Wkly. Epidemiol. Rec. 2015, 90, 57–62. [Google Scholar]
- Frasch, C.E.; Borrow, R.; Donnelly, J. Bactericidal antibody is the immunologic surrogate of protection against meningococcal disease. Vaccine 2009, 27, B112–B116. [Google Scholar] [CrossRef] [PubMed]
- White, M.; Idoko, O.; Sow, S.; Diallo, A.; Kampmann, B.; Borrow, R.; Trotter, C. Antibody kinetics following vaccination with MenAfriVac: An analysis of serological data from randomised trials. Lancet Infect. Dis. 2019, 19, 327–336. [Google Scholar] [CrossRef] [Green Version]
- Yaro, S.; Njanpop Lafourcade, B.-M.; Ouangraoua, S.; Ouoba, A.; Kpoda, H.; Findlow, H.; Tall, H.; Seanehia, J.; Martin, C.; Ouedraogo, J.-B.; et al. Antibody Persistence at the Population Level 5 Years after Mass Vaccination with Meningococcal Serogroup A Conjugate Vaccine (PsA-TT) in Burkina Faso: Need for a Booster Campaign? Clin. Infect. Dis. 2019, 68, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Daugla, D.M.; Gami, J.P.; Gamougam, K.; Naibei, N.; Mbainadji, L.; Narbé, M.; Toralta, J.; Kodbesse, B.; Ngadoua, C.; Coldiron, M.E.; et al. Effect of a serogroup A meningococcal conjugate vaccine (PsA–TT) on serogroup A meningococcal meningitis and carriage in Chad: A community study. Lancet 2014, 383, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Meningitis Vaccine Project: Timeline. Available online: https://www.meningvax.org/timeline.html (accessed on 30 December 2020).
- t.test Function | R Documentation. Available online: https://www.rdocumentation.org/packages/stats/versions/3.6.2/topics/t.test (accessed on 30 December 2020).
- Hashim, A.; Dang, V.; Bolotin, S.; Crowcroft, N.S. How and why researchers use the number needed to vaccinate to inform decision making—A systematic review. Vaccine 2015, 33, 753–758. [Google Scholar] [CrossRef] [Green Version]
- Soeters, H.M.; Diallo, A.O.; Bicaba, B.W.; Kadadé, G.; Dembélé, A.Y.; Acyl, M.A.; Nikiema, C.; Sadji, A.Y.; Poy, A.N.; Lingani, C.; et al. Bacterial Meningitis Epidemiology in Five Countries in the Meningitis Belt of Sub-Saharan Africa, 2015–2017. J. Infect. Dis. 2019, 220, S165–S174. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.V.; Kristiansen, P.A.; Christensen, H.; Karachaliou, A.; Trotter, C.L. Meningococcal carriage by age in the African meningitis belt: A systematic review and meta-analysis. Epidemiol. Infect. 2019, 147. [Google Scholar] [CrossRef] [PubMed]
- Edmond, K.; Clark, A.; Korczak, V.S.; Sanderson, C.; Griffiths, U.K.; Rudan, I. Global and regional risk of disabling sequelae from bacterial meningitis: A systematic review and meta-analysis. Lancet Infect. Dis. 2010, 10, 317–328. [Google Scholar] [CrossRef] [Green Version]
- Trotter, C.L.; Cibrelus, L.; Fernandez, K.; Lingani, C.; Ronveaux, O.; Stuart, J.M. Response thresholds for epidemic meningitis in sub-Saharan Africa following the introduction of MenAfriVac®. Vaccine 2015, 33, 6212–6217. [Google Scholar] [CrossRef] [PubMed]
- le Polain de Waroux, O.; Cohuet, S.; Ndazima, D.; Kucharski, A.J.; Juan-Giner, A.; Flasche, S.; Tumwesigye, E.; Arinaitwe, R.; Mwanga-Amumpaire, J.; Boum, Y., II; et al. Characteristics of human encounters and social mixing patterns relevant to infectious diseases spread by close contact: A survey in Southwest Uganda. BMC Infect. Dis. 2018, 18, 172. [Google Scholar] [CrossRef]
- Jackson, M.L.; Diallo, A.O.; Médah, I.; Bicaba, B.W.; Yaméogo, I.; Koussoubé, D.; Ouédraogo, R.; Sangaré, L.; Mbaeyi, S.A. Initial validation of a simulation model for estimating the impact of serogroup A Neisseria meningitidis vaccination in the African meningitis belt. PLoS ONE 2018, 13, e0206117. [Google Scholar] [CrossRef]
- Tartof, S.; Cohn, A.; Tarbangdo, F.; Djingarey, M.H.; Messonnier, N.; Clark, T.A.; Kambou, J.L.; Novak, R.T.; Diomande, F.; Medah, I.; et al. Identifying Optimal Vaccination Strategies for Serogroup A Neisseria meningitidis Conjugate Vaccine in the African Meningitis Belt. PLoS ONE 2013, 8, e63605. [Google Scholar] [CrossRef] [Green Version]
- Borrow, R.; Caugant, D.A.; Ceyhan, M.; Christensen, H.; Dinleyici, E.C.; Findlow, J.; Glennie, L.; von Gottberg, A.; Kechrid, A.; Moreno, J.V.; et al. Meningococcal disease in the Middle East and Africa: Findings and updates from the Global Meningococcal Initiative. J. Infect. 2017, 75, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaesoubi, R.; Trotter, C.; Colijn, C.; Yaesoubi, M.; Colombini, A.; Resch, S.; Kristiansen, P.A.; LaForce, F.M.; Cohen, T. The cost-effectiveness of alternative vaccination strategies for polyvalent meningococcal vaccines in Burkina Faso: A transmission dynamic modeling study. PLoS Med. 2018, 15, e1002495. [Google Scholar] [CrossRef] [PubMed]




| Strategy | Introduction | Catch-Up Campaign | Routine Immunisation | Assumed Coverage for EPI |
|---|---|---|---|---|
| EPI@12m (Current strategy) | 2011–2012: 1–29 years old | 2017: 1–6 years old | 2017–2060: at 12 months | 75% in 2017 and annual increments of 1% until it reaches 90% |
| EPI@5y | 2011–2012: 1–29 years old | None | 2017–2060: at 5 years | 80% |
| EPI@10y | 2011–2012: 1–29 years old | None | 2022–2060: at 10 years | 80% |
| Booster | 2011–2012: 1–29 years old | None | 2017–2060: at 12 months and 5 years |
|
| Switch | 2011–2012: 1–29 years old | 2017: 1–6 years old | 2017–2021: at 12 months 2022–2026: at 12 months and 5 years 2027–2060: at 5 years |
|
| Strategy | Duration of Protection | # of Doses | Cases | Cases Prevented | NNV |
|---|---|---|---|---|---|
| EPI@12m | 10 years | 42,034 | 86.36 | 174.39 | 241 |
| EPI@5y | 10 years | 33,878 | 87.62 | 173.13 | 196 |
| EPI@10y | 10 years | 30,024 | 87.17 | 173.58 | 173 |
| Switch | 10 years | 39,961 | 77.34 | 183.41 | 218 |
| Booster | 10 years | 63,882 | 54.09 | 206.66 | 309 |
| EPI@12m | 20 years | 42,034 | 0.65 | 260 | 162 |
| EPI@5y | 20 years | 33,878 | 0.65 | 260 | 130 |
| EPI@10y | 20 years | 30,024 | 0.71 | 260 | 115 |
| Switch | 20 years | 39,961 | 0.65 | 260 | 154 |
| Booster | 20 years | 63,882 | 0.65 | 260 | 246 |
| EPI@12m | 5 years | 42,034 | 164.53 | 96.22 | 437 |
| EPI@5y | 5 years | 33,878 | 165.41 | 95.34 | 355 |
| EPI@10y | 5 years | 30,024 | 166.19 | 94.56 | 317 |
| Switch | 5 years | 39,961 | 158.59 | 102.16 | 391 |
| Booster | 5 years | 63,882 | 135.92 | 124.83 | 512 |
| EPI@12m | Age-specific | 42,034 | 148.6 | 112.3 | 374 |
| EPI@5y | Age-specific | 33,878 | 94.66 | 166.1 | 204 |
| EPI@10y | Age-specific | 30,024 | 96.28 | 164.47 | 183 |
| Switch | Age-specific | 39,961 | 95.56 | 165.19 | 242 |
| Booster | Age-specific | 63,882 | 72.09 | 188.66 | 339 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karachaliou Prasinou, A.; Conlan, A.J.K.; Trotter, C.L. Understanding the Role of Duration of Vaccine Protection with MenAfriVac: Simulating Alternative Vaccination Strategies. Microorganisms 2021, 9, 461. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9020461
Karachaliou Prasinou A, Conlan AJK, Trotter CL. Understanding the Role of Duration of Vaccine Protection with MenAfriVac: Simulating Alternative Vaccination Strategies. Microorganisms. 2021; 9(2):461. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9020461
Chicago/Turabian StyleKarachaliou Prasinou, Andromachi, Andrew J. K. Conlan, and Caroline L. Trotter. 2021. "Understanding the Role of Duration of Vaccine Protection with MenAfriVac: Simulating Alternative Vaccination Strategies" Microorganisms 9, no. 2: 461. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9020461