
Bacterial Meningitis in Children: Neurological Complications, Associated Risk Factors, and Prevention


1
Department of Pediatrics, Division of Infectious Diseases, University of British Columbia, Vancouver, BC V6t 1Z4, Canada
2
Vaccine Evaluation Center, BC Children’s Hospital, Vancouver, BC V6H 3N1, Canada
*
Author to whom correspondence should be addressed.
Microorganisms 2021, 9(3), 535; https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9030535
Submission received: 27 January 2021
/
Revised: 3 March 2021
/
Accepted: 3 March 2021
/
Published: 5 March 2021
(This article belongs to the Special Issue Bacterial Meningitis: Epidemiology and Vaccination)
Abstract
:Bacterial meningitis is a devastating infection, with a case fatality rate of up to 30% and 50% of survivors developing neurological complications. These include short-term complications such as focal neurological deficit and subdural effusion, and long-term complications such as hearing loss, seizures, cognitive impairment and hydrocephalus. Complications develop due to bacterial toxin release and the host immune response, which lead to neuronal damage. Factors associated with increased risk of developing neurological complications include young age, delayed presentation and Streptococcus pneumoniae as an etiologic agent. Vaccination is the primary method of preventing bacterial meningitis and therefore its complications. There are three vaccine preventable causes: Haemophilus influenzae type b (Hib), S. pneumoniae, and Neisseria meningitidis. Starting antibiotics without delay is also critical to reduce the risk of neurological complications. Additionally, early adjuvant corticosteroid use in Hib meningitis reduces the risk of hearing loss and severe neurological complications.
1. Introduction
Acute bacterial meningitis is the most common bacterial central nervous system (CNS) infection. It is a devastating illness, especially in neonates (age < one month) and infants (age < one year). Bacterial meningitis has a high case-fatality rate of up to 30% [1,2,3,4,5], and as many as 50% of survivors develop neurological complications [1,3,6,7,8,9,10]—with outcomes highly dependent on patient’s age and the infecting organism. This article provides an overview of the short and long-term neurological complications of bacterial meningitis, the associated risk factors, and available vaccines and therapies which may reduce the risk of complications.
2. Epidemiology and Etiology
The incidence of bacterial meningitis in children differs by age group and is highest in infants aged younger than two months [11,12]. In the United States, the incidence rate during 2006–2007 in children under two months was 81 cases per 100,000, compared with 0.4 cases per 100,000 in children aged 11–17 years. Bacterial meningitis is more common in low and middle income countries (LMICs) compared to high income countries (HICs) [13,14]. For example, the incidence rate of meningitis in 2016 in all ages in South Sudan was 270 per 100,000 whereas in Australia it was 0.5 per 100,000 [14].
The most common organisms causing bacterial meningitis vary by age group (Table 1). Introduction of vaccines against Haemophilus influenzae type b (Hib), Neisseria meningitidis and Streptococcus pneumoniae over the last three decades has led to a drastic decrease in the incidence rate of bacterial meningitis beyond the neonatal period in countries with these vaccines included as part of their routine infant and children immunization programs [15]. However, the case fatality rate has not changed significantly [16,17,18,19,20].
Hib was the leading cause of bacterial meningitis in the 1990s, but became uncommon in countries that introduced Hib immunization. However, it is still a frequent cause of bacterial meningitis in the countries were Hib vaccine is not universal or in unvaccinated children due to vaccine hesitancy [27]. In countries where Hib is now rare, S. pneumoniae has become the leading cause of bacterial meningitis outside the neonatal period, except in some European and Sub-Saharan African countries, where it is the second most common cause in this age group after N. meningitidis [26]. Group B Streptococcus (GBS) and Escherichia coli remain the leading causes of bacterial meningitis in neonates with little change in incidence rates over time [4,12]. Intrapartum antibiotic prophylaxis has reduced the risk of early onset, but not late-onset GBS meningitis [28,29]. Although, Listeria monocytogenes is an uncommon cause, it should be considered in neonates.
3. Pathophysiology of Bacterial Meningitis
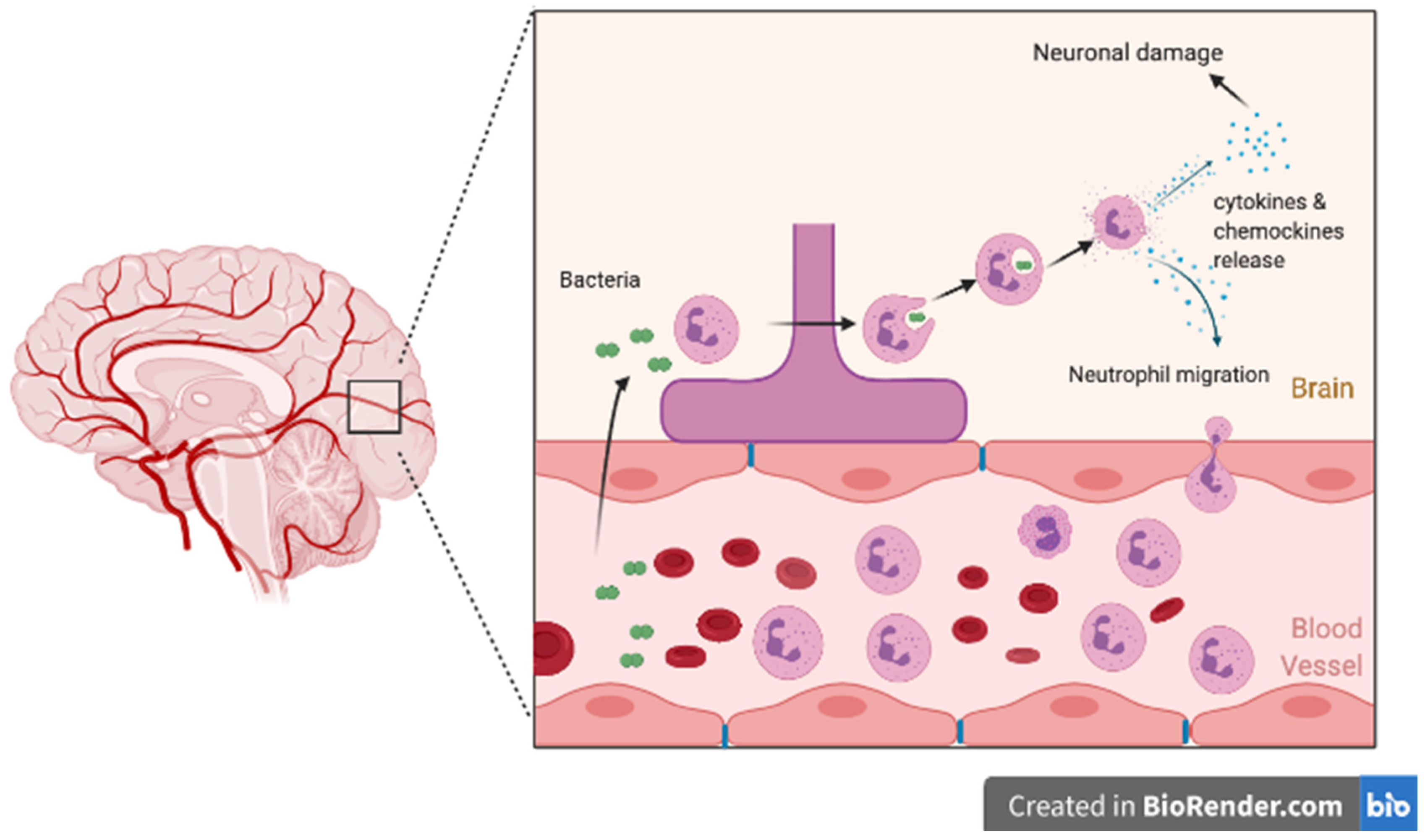
Meningitis develops after the pathogen invades the CNS either though hematogenous route (bacteremia) or by direct extension secondary to sinusitis or mastoiditis and multiplies in the subarachnoid space. The presence of bacteria in the subarachnoid space leads to activation of the immune response, resulting in bacterial lysis. The presence of bacterial particles triggers a further inflammatory response with on-going migration of neutrophils across the blood–brain barrier and continuous cytokine and chemokine release (including IL-1B or CXCL1,2,5) (Figure 1) [7,30,31,32,33,34,35]. A persistent inflammatory state subsequently leads to decreased cerebral perfusion, cerebral edema, raised intracranial pressure, metabolic disturbances, and vasculitis, all contributing to neuronal injury and ischemia [32].
4. Bacterial Meningitis Complications
There are many complications that are associated with bacterial meningitis. These include short-term complications such as seizures, focal neurological deficits and subdural effusions, and long-term complications such as hearing loss, cognitive impairment, hydrocephalus, learning disability, and epilepsy [8,36,37,38]. Neurological sequelae are more likely to happen in LMICs compared with HICs [37] due to delayed presentation to medical services, lack of access to healthcare and limited resources. Additionally, complications are likely under reported in LMICs (Table 2) [7].
4.1. Short-Term Complications
4.1.1. Subdural Effusion
Subdural effusions occur in 20–39% of children with bacterial meningitis [50,51,52]. Subdural effusion is most common in infants (age < one year) compared to older children [8,51]. There is no significant difference in subdural effusions complication due to Hib meningitis compared to S. pneumoniae and N. meningitidis [51]. Most subdural effusions in the context of bacterial meningitis are asymptomatic, resolve spontaneously and rarely require intervention. Indications for drainage include an infected effusion or empyema, focal neurological signs or symptoms, or increased intracranial pressure [51].
4.1.2. Focal Neurological Deficit
Focal neurological deficit refers to a set of signs and symptoms resulting from a lesion localized to a specific anatomical site in central nervous system [53]. Examples include isolated limb weakness or hemiparesis, visual deficit or a speech impediment. They are estimated to occur in 3–14% of bacterial meningitis cases [41,42].
Acute focal neurological deficits after bacterial meningitis are usually due to ischemic stroke, but can also occur due to subdural empyema, cerebral abscess or intracranial bleeding [7]. Focal neurological deficits generally improve over months to years after the initial insult. Abscess collections can be surgically drained which usually leads to complete symptom resolution while focal deficits resulting from an ischemic event take longer to resolve. In a recent study, children with stroke following bacterial meningitis compared to children without stroke were less likely to have a normal neurological exam at discharge (21% vs. 76%) and within a seven years follow-up period (31% vs. 74%) [54]. Focal neurological deficits that persist after acute infection are not a very common complication after bacterial meningitis in childhood (Table 2); however, the incidence is highest for infections occurring in the first year of life [55].
4.2. Long-Term Complications
4.2.1. Hearing Loss
Sensorial hearing loss is the most widely reported neurological sequelae of bacterial meningitis [7,27,44,51,56,57,58,59]. Hearing loss may develop from both the direct spread of bacterial products and as a result of the host inflammatory response in the meninges and CSF. When bacteria reach the cochlea, a severe labyrinthitis results, which leads to blood-labyrinth barrier breakage, and ultimately meningitis-associated hearing loss [7]. Around 10% of children with bacterial meningitis develop unilateral or bilateral sensorineural hearing loss [37,60]; 5% of children develop bilateral severe or profound hearing loss [37]. Hearing loss is a more common complication in infections caused by S. pneumoniae (14–32%), compared with N. meningitidis (4–23%) and H. influenzae (20%) [44,60]. Children with hearing loss are at risk of further developing balance disturbances [61] and speech and language delay [62], and are therefore at higher risk of having long-term behavioral problems [63].
Reversible deafness (i.e., transient hearing loss) has been documented in long term follow up of children with pneumococcal meningitis [7,61]. For example, a study done among children with pneumococcal meningitis in Bangladesh reported that 33% of children in short-term follow-up (30–40 days) had hearing loss, but only 18% had persistent hearing loss in long-term follow-up (6–24 months) following hospital. The difference was attributed to recovery of transient hearing impairment [43].
4.2.2. Cognitive Impairment
Due to the irreversible neuronal damage that occurs during bacterial meningitis, the risk of developing long-term cognitive deficits and learning difficulties are significant [3,48]. The rates of cognitive impairment world-wide are difficult to estimate because there is no standardized method of measuring it and long-term data on meningitis survivors are rarely available.
In a Dutch study, 680 children between the age of 4 and 13 years who survived bacterial meningitis were followed up for 6 years after their meningitis episode. The study followed their educational, behavioral and general health issues. The survivors were compared to a control group of healthy school-age siblings and peers, with similar socioeconomic background. It was found that 30% of children with meningitis had problems with school achievement or concentration. Additionally, these children repeated a school year twice as often as the control group (16% vs. 8%). Moreover, the post-meningitis group were referred to special-needs school four times more frequently compared to control group [48].
In a Danish nationwide population-based cohort study, adults who had a bacterial meningitis in childhood were compared to control group that included a general population of the same age and sex, their siblings and the siblings of meningitis patients. Adults who had childhood bacterial meningitis had lower educational achievements and economic self-sufficiency compared to control group. By the age of 35 years, 11%, 10.2% and 5.5% fewer had completed high school in meningococcal pneumococcal, and Hib meningitis, respectively. Additionally, 7.9%, 8.9% and 6.5% fewer had obtained a higher education in meningococcal pneumococcal, and Hib meningitis, respectively. Additionally, 3.8%, 10.6% and 4.3% had lower economic self-sufficiency in meningococcal pneumococcal, and Hib meningitis, respectively [49]. In a study done in Bangladesh, short (30–40 days) and long-term (6–24 months) follow-up revealed that 41% in both groups had deficits in mental development and 49% and 35%, respectively, had psychomotor delay [43]. Another example, in a study that was done in Brazil, 5.88% children developed learning disabilities, and 7.35% children had developmental delay [40].
Finally, psychiatric disease including anxiety and depression is likely under-recognized and underreported in meningitis survivors and contributes to cognitive difficulties and overall quality of life [64].
4.2.3. Seizures and Epilepsy
One of the clinical presentations of bacterial meningitis is seizures [65,66]. In cases of bacterial meningitis with seizures, if seizures develop early during the illness and are easily controlled, permanent neurological complications are rarely of concern. However, if seizures are prolonged, difficult to control or develop 72 h after admission, neurological sequelae are more likely to occur and are usually suggestive of a cerebrovascular event [44,67]. In HICs, 1–5% of epilepsy cases are presumed to be due to CNS infection; including bacterial meningitis [68]. In Sub-Saharan Africa 26% of patients have epilepsy attributed to CNS infection [69].
4.2.4. Hydrocephalus
Hydrocephalus incidence is around 7% of bacterial meningitis in children [71] and it is more common in neonates and infants; 25% [72,73]. It is more common in neonatal Gram negative meningitis [57]. Hydrocephalus may develop at the beginning of the illness or weeks later after diagnosis with bacterial meningitis. The most common type of hydrocephalus after bacterial meningitis is communicating hydrocephalus; seen in up to 52% of cases with hydrocephalus [74]. In communicating hydrocephalus CSF flows freely between the ventricles but is not adequately reabsorbed back into the blood stream. Depending on the size of hydrocephalus and resulting neurologic impairment temporary or permanent ventricular shunt placement may be required [75].
5. Risk Factors
There are many risk factors associated with neurological complications in bacterial meningitis (Table 3).
In general, infants are at higher risk of developing neurological complications compared to older children [3,9,23]. 71% of infants (aged < one year) with bacterial meningitis develop neurological complications compared to 38% in children aged one to five years and 10% in those aged six to 16 years [9]. Children younger than 12 months at time of diagnosis with bacterial meningitis are at increased risk of developing hydrocephalus, subdural effusion, seizure disorder and hearing loss [76]. Altered level of consciousness is associated with poor prognosis [6,9]. 82% of children with bacterial meningitis who developed neurological complications had altered level of consciousness on presentation; where, 39% of children with bacterial meningitis who did not develop neurological complications had altered level of consciousness [9]. The longer the duration that the child was unconscious, the worst the outcome is.
In bacterial meningitis, delayed presentation to hospital increase the risk of subdural effusion, hydrocephalus, hearing impairment and seizure disorder [76]. Although delayed presentation is one of the known risk factors for developing neurological complications, there is no universal definition for the duration of the delay. In one study, children admitted with duration of illness <48 h had a lower incidence of neurological complication (40%) compared to children who were admitted after 48 h of illness [9]. Children with S. pneumoniae meningitis have a higher risk of developing neurological complication (75% of S. pneumoniae meningitis cases) compared to N. meningitidis (25%) and Hib (20%) [9]. S. pneumoniae compared to N. meningitidis and Hib is associated with higher risk of symptomatic seizures, hydrocephalus, hearing loss and mental retardation [76]. Delay in starting antibiotics beyond 24–72 h has a poor prognosis and leads to increased risk of severe neurological complication such as hydrocephalus, subdural effusion, hearing loss, and seizure disorder [76]. In summary, young age, delayed presentation and S. pneumoniae as an etiologic agent were associated with increased risk of neurological complications in both HIC and LMIC settings [11,15,54,71,76,77,78].
6. Prevention of Neurological Complication
6.1. Primary Prevention
The most effective prevention of neurological complications from bacterial meningitis is preventing the infection though infant and childhood vaccination programs. Despite the development of multiple vaccines against the organisms causing bacterial meningitis, there continue to be many meningitis outbreaks caused by vaccine-preventable organisms [79,80]. There are currently vaccines against 3 of the organisms that cause bacterial meningitis: Hib, N. meningitidis (capsular groups A, B, C, W and Y) and 23 of the >90 serotypes of S. pneumoniae [4,15]. Hib conjugate vaccine targets only type b H. influenzae, and is given as three or four doses before 18 months of age [81]. There are two types of vaccine against N. meningitidis: Conjugate vaccines against capsular groups A, C, W, and Y and protein vaccines against group B. There are two types of vaccines against S. pneumoniae: Pneumococcal conjugate vaccines (PCV 10 against 10 serotypes, PCV 13 against 13 serotypes) and polysaccharide vaccine against 23 serotypes which is not routinely used in healthy children [82].
Routine vaccination can lead to development of community protection by indirect effect prevention of transmission within a population [83]. Since the introduction of pneumococcal conjugate vaccines (PCVs), the overall incidence of invasive pneumococcal disease (IPD) has dropped significantly, including in unimmunized children, highlighting these indirect effects [84,85]. For example, in South Africa, Morocco, Gambia, Mozambique, Kenya and Burkina Faso, 32–81% reduction in IPD has been reported after PCV introduction, with highest reduction in children aged under 24 months (55–89%) [86]. However, infections caused by non-vaccine serotypes infections have increased in some countries. In the United States, the proportion of IPD caused by non-vaccine serotype increased from 6% to 38% after the introduction of PCV7 vaccine; sometimes referred to as serotype replacement [85,87,88]. Overall, IPD incidence dropped.
The highest rate of meningococcal disease worldwide is in the Sub-Saharan Africa, specifically in the “meningitis belt” region where major epidemics occur every 5–12 years [89]. After the introduction of MenA vaccine to the Sub-Saharan Africa in 2010, there has been a 99% reduction in group A meningitis in this region [90] and capsular group W is the currently the commonest [91]. Rate of meningococcal meningitis are much lower in other parts of Sub-Saharan Africa, although longitudinal surveillance outside of the meningitis belt is limited [92]. Following wide-spread introduction of Hib vaccine, S. pneumoniae accounted for 65% of acute bacterial meningitis cases in Malawi, while the rates of N. meningitidis have remained constant at <5% [90].
6.2. Secondary Prevention of Complications
6.2.1. Antibiotic Therapy
It is important to have a high clinical suspicion of bacterial meningitis and start appropriate treatment without delay [93,94]. The empiric antibiotic choice should be based on the most likely causative agent for patient’s age [73,95,96]. In children, third-generation cephalosporins, such as cefotaxime or ceftriaxone, are the usual empirical choice to cover the most common organisms—S. pneumoniae and N. meningitidis. Ampicillin should be added to cover L. monocytogenes in very young children; some guidelines recommended for younger than 3 months, others recommended this for those younger than 1 month [95,96].
6.2.2. Corticosteroids
Neuronal damage due to acute bacterial meningitis is not only due to bacterial invasion to the subarachnoid space, but also due to the host’s inflammatory response to this invasion [36]. The only widely researched agent that can limit subarachnoid inflammation is dexamethasone. The recommendation for the use of dexamethasone in bacterial meningitis unfortunately cannot be generalized and depends on the causative organism and the ability to administer dexamethasone within 1–12 h of administration of antibiotics [27,40,44,97].
In infant and children with Hib meningitis, administration of dexamethasone with antibiotics has shown a significant reduction in neurological sequelae rate (17%) compared to antibiotic only (23.4%) [27,59]. Additionally, rates of hearing loss were lower with dexamethasone use (12.9%) compared to antibiotics only (17.4%) [59,96,98,99]. In a large study done in Malawi, children with H. influenzae meningitis who received dexamethasone were less likely to have neurological sequelae compared to a placebo group (27% vs. 40%) [13]. Therefore, it is generally recommended that dexamethasone be administered before or with the first dose of antibiotics [1,13,96] when H. influenzae is confirmed or strongly suspected.
On the other hand, the use of dexamethasone in infants and children with pneumococcal meningitis is controversial as it has not been clearly proven to change the outcome [1,13,36,98,99]. Additionally, the use of dexamethasone for meningococcal meningitis was not proven to be effective in reduce neurological sequelae [96].
Better understanding of specific microbial and host factors contributing to CNS infection and inflammatory response may help in identification of new therapeutic targets and specific immunomodulatory regimens.
7. Long-Term Follow Up
All children who are diagnosed with meningitis should have a hearing assessment done before discharge or 1 month within discharge; even if hearing loss is not clinically suspected [13,61]. It is critical to perform audiology assessment month after diagnosis or earlier if possible, as up to 90% of children’s cochlea with hearing loss due to meningitis can ossify, preventing appropriate treatment with cochlear implants [100,101].
Children with seizure disorders require antiepileptic medication and should ideally have long-term follow up by a neurologist [7,8,67,70]. Children with hearing loss and/ or intellectual disability will need neurodevelopmental follow up and support for speech, language and social development. Mental health concerns and psychiatric problems are likely underreported in children who were diagnosed with meningitis and periodic mental health assessments by an appropriate specialist should be included into their long-term care [64].
8. Conclusions
Children with bacterial meningitis are at risk of developing neurological complications that include focal neurological deficits, subdural effusion, hearing loss, cognitive impairment, seizure disorder, and hydrocephalus. There is a need to optimize utilization of available vaccines and to develop vaccines for pathogens implicated in neonatal meningitis (GBS and E. coli). For children diagnosed with bacterial meningitis, starting antibiotic therapy without delay is critical for a good prognosis and to reduce the risk of developing neurological complications. So far, steroids are the only drug that can control inflammatory response, but effectiveness is limited to specific situations.
Author Contributions
A.Z., H.M., and M.S. conceived and designed the structure of the manuscript. A.Z. drafted the original version of the manuscript. All authors edited and approved the final version. All authors have read and agreed to the published version of the manuscript.
Funding
None.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
MS is supported via salary awards from the BC Children’s Hospital Foundation, the Canadian Child Health Clinician Scientist Program and the Michael Smith Foundation for Health Research.
Conflicts of Interest
MS has been an investigator on projects funded by GlaxoSmithKline, Merck, Pfizer, Sanofi-Pasteur, Seqirus, Symvivo and VBI Vaccines. All funds have been paid to his institute, and he has not received any personal payments.
References
- Grandgirard, D.; Leib, S.L. Strategies to prevent neuronal damage in paediatric bacterial meningitis. Curr. Opin. Pediatr. 2006, 18, 112–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonko, A.M.; Dube, F.S.; Okoi, C.B.; Diop, A.; Thiongane, A.; Senghore, M.; Ndow, P.; Worwui, A.; Faye, P.M.; Dieye, B.; et al. Changes in the Molecular Epidemiology of Pediatric Bacterial Meningitis in Senegal after Pneumococcal Conjugate Vaccine Introduction. Clin. Infect. Dis. 2019, 69, S156–S163. [Google Scholar] [CrossRef] [PubMed]
- Shieh, H.H.; Ragazzi, S.L.B.; Gilio, A.E. Risk factors for neurological complications and sequelae in childhood acute bacterial meningitis. J. Pediatr. 2012, 88, 184. [Google Scholar] [CrossRef] [Green Version]
- Thigpen, M.C.; Whitney, C.G.; Messonnier, N.E.; Zell, E.R.; Lynfield, R.; Hadler, J.L.; Harrison, L.H.; Farley, M.M.; Reingold, A.; Bennett, N.M.; et al. Bacterial Meningitis in the United States, 1998–2007. N. Engl. J. Med. 2011, 364, 2016–2025. [Google Scholar] [CrossRef]
- Yogev, R.; A Guzmancottrill, J. Bacterial Meningitis in Children. Drugs 2005, 65, 1097–1112. [Google Scholar] [CrossRef]
- Pelkonen, T.; Roine, I.; Monteiro, L.; Correia, M.; Pitkäranta, A.; Bernardino, L.; Peltola, H. Risk Factors for Death and Severe Neurological Sequelae in Childhood Bacterial Meningitis in Sub-Saharan Africa. Clin. Infect. Dis. 2009, 48, 1107–1110. [Google Scholar] [CrossRef] [Green Version]
- Lucas, M.J.; Brouwer, M.C.; van de Beek, D. Neurological sequelae of bacterial meningitis. J. Infect. 2016, 73, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Namani, S.A.; Koci, B.M.; Milenković, Z.; Koci, R.; Qehaja-Buçaj, E.; Ajazaj, L.; Mehmeti, M.; Ismaili-Jaha, V. Early neurologic complications and long-term sequelae of childhood bacterial meningitis in a limited-resource country (Kosovo). Child’s Nerv. Syst. 2012, 29, 275–280. [Google Scholar] [CrossRef]
- Namani, S.; Milenković, Z.; Koci, B. A prospective study of risk factors for neurological complications in childhood bacterial meningitis. J. Pediatr. 2013, 89, 256–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ispahani, P.; Slack, R.C.B.; Donald, E.F.; Weston, V.C.; Rutter, N. Twenty year surveillance of invasive pneumococcal disease in Nottingham: Serogroups responsible and implications for immunisation. Arch. Dis. Child. 2004, 89, 757–762. [Google Scholar] [CrossRef]
- Softić, I.; Tahirović, H.; Hasanhodžić, M. Neonatal bacterial meningitis: Results from a cross-sectional hospital based study. Acta Med. Acad. 2015, 44, 117–123. [Google Scholar]
- Baud, O.; Aujard, Y. Neonatal Bacterial Meningitis; Elsevier: Amsterdam, The Netherlands, 2013; Volume 112, pp. 1109–1113. [Google Scholar]
- Molyneux, E.M.; Walsh, A.L.; Forsyth, H.; Tembo, M.; Mwenechanya, J.; Kayira, K.; Bwanaisa, L.; Njobvu, A.; Rogerson, S.; Malenga, G. Dexamethasone treatment in childhood bacterial meningitis in Malawi: A randomised controlled trial. Lancet 2002, 360, 211–218. [Google Scholar] [CrossRef]
- Zunt, J.R.; Kassebaum, N.J.; Blake, N.; Glennie, L.; Wright, C.; Nichols, E.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; A Adamu, A.; et al. Global, regional, and national burden of meningitis, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 1061–1082. [Google Scholar] [CrossRef] [Green Version]
- McIntyre, P.B.; O’Brien, K.L.; Greenwood, B.; van de Beek, D. Effect of vaccines on bacterial meningitis worldwide. Lancet 2012, 380, 1703–1711. [Google Scholar] [CrossRef]
- McAlpine, A.; Sadarangani, M. Meningitis vaccines in children. Curr. Opin. Infect. Dis. 2019, 32, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Mwenda, J.M.; Soda, E.; Weldegebriel, G.; Katsande, R.; Biey, J.N.-M.; Traore, T.; De Gouveia, L.; Du Plessis, M.; Von Gottberg, A.; Antonio, M.; et al. Pediatric Bacterial Meningitis Surveillance in the World Health Organization African Region Using the Invasive Bacterial Vaccine-Preventable Disease Surveillance Network, 2011–2016. Clin. Infect. Dis. 2019, 69, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Bettinger, J.A.; Scheifele, D.W.; Kellner, J.D.; Halperin, S.A.; Vaudry, W.; Law, B.; Tyrrell, G. The effect of routine vaccination on invasive pneumococcal infections in Canadian children, Immunization Monitoring Program, Active 2000–2007. Vaccine 2010, 28, 2130–2136. [Google Scholar] [CrossRef] [PubMed]
- Bettinger, J.A.; Scheifele, D.W.; Halperin, S.A.; Kellner, J.D.; Vanderkooi, O.G.; Schryvers, A.; De Serres, G.; Alcantara, J. Evaluation of meningococcal serogroup C conjugate vaccine programs in Canadian children: Interim analysis. Vaccine 2012, 30, 4023–4027. [Google Scholar] [CrossRef] [PubMed]
- Leal, J.; Vanderkooi, O.G.; Church, D.L.; MacDonald, J.; Tyrrell, G.J.; Kellner, J.D. Eradication of Invasive Pneumococcal Disease due to the Seven-valent Pneumococcal Conjugate Vaccine Serotypes in Calgary, Alberta. Pediatr. Infect. Dis. J. 2012, 31, e169–e175. [Google Scholar] [CrossRef] [PubMed]
- Gaschignard, J.; Levy, C.; Romain, O.; Cohen, R.; Bingen, E.; Aujard, Y.; Boileau, P. Neonatal Bacterial Meningitis. Pediatr. Infect. Dis. J. 2011, 30, 212–217. [Google Scholar] [CrossRef]
- Smith, P.B.; Garges, H.P.; Cotton, C.M.; Walsh, T.J.; Clark, R.H.; Benjamin, D.K.; Cotten, C.M. Meningitis in Preterm Neonates: Importance of Cerebrospinal Fluid Parameters. Am. J. Perinatol. 2008, 25, 421–426. [Google Scholar] [CrossRef] [Green Version]
- McCormick, D.W.; Wilson, M.L.; Mankhambo, L.; Phiri, A.; Chimalizeni, Y.; Kawaza, K.; Denis, B.; Carrol, E.D.; Molyneux, E.M. Risk Factors for Death and Severe Sequelae in Malawian Children with Bacterial Meningitis, 1997–2010. Pediatr. Infect. Dis. J. 2013, 32, e54–e61. [Google Scholar] [CrossRef] [Green Version]
- Schuchat, A.; Robinson, K.; Wenger, J.D.; Harrison, L.H.; Farley, M.; Reingold, A.L.; Lefkowitz, L.; Perkins, B.A. Bacterial Meningitis in the United States in 1995. N. Engl. J. Med. 1997, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Cockcroft, D.W.; Nair, P. Methacholine test and the diagnosis of asthma. J. Allergy Clin. Immunol. 2012, 130, 556–557. [Google Scholar] [CrossRef]
- Ceyhan, M.; Gürler, N.; Ozsurekci, Y.; Keser, M.; Aycan, A.E.; Gurbuz, V.; Salman, N.; Camcioglu, Y.; Dinleyici, E.C.; Ozkan, S.; et al. Meningitis caused by Neisseria Meningitidis, Hemophilus Influenzae Type B and Streptococcus Pneumoniae during 2005–2012 in Turkey. Hum. Vaccines Immunother. 2014, 10, 2706–2712. [Google Scholar] [CrossRef] [Green Version]
- Duke, T.; Curtis, N.; Fuller, D.G. The management of bacterial meningitis in children. Expert Opin. Pharmacother. 2003, 4, 1227–1240. [Google Scholar] [CrossRef] [PubMed]
- Phares, C.R.; Lynfield, R.; Farley, M.M.; Mohle-Boetani, J.; Harrison, L.H.; Petit, S.; Craig, A.S.; Schaffner, W.; Zansky, S.M.; Gershman, K.; et al. Epidemiology of Invasive Group B Streptococcal Disease in the United States, 1999–2005. JAMA 2008, 299, 2056–2065. [Google Scholar] [CrossRef]
- Edmond, K.M.; Kortsalioudaki, C.; Scott, S.; Schrag, S.J.; Zaidi, A.K.; Cousens, S.; Heath, P.T. Group B streptococcal disease in infants aged younger than 3 months: Systematic review and meta-analysis. Lancet 2012, 379, 547–556. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.S. Pathogenesis of bacterial meningitis: From bacteraemia to neuronal injury. Nat. Rev. Neurosci. 2003, 4, 376–385. [Google Scholar] [CrossRef]
- Koedel, U.; Klein, M.; Pfister, H.-W. New understandings on the pathophysiology of bacterial meningitis. Curr. Opin. Infect. Dis. 2010, 23, 217–223. [Google Scholar] [CrossRef]
- Scheld, W.M.; Koedel, U.; Nathan, B.; Pfister, H. Pathophysiology of Bacterial Meningitis: Mechanism (s) of Neuronal Injury. J. Infect. Dis. 2002, 186, 225–233. [Google Scholar] [CrossRef]
- Barichello, T.; Generoso, J.S.; Simões, L.R.; Goularte, J.A.; Petronilho, F.; Saigal, P.; Badawy, M.; Quevedo, J. Role of Microglial Activation in the Pathophysiology of Bacterial Meningitis. Mol. Neurobiol. 2016, 53, 1770–1781. [Google Scholar] [CrossRef]
- Hoffman, O.; Weber, J.R. Review: Pathophysiology and treatment of bacterial meningitis. Ther. Adv. Neurol. Disord. 2009, 2, 401–412. [Google Scholar] [CrossRef] [Green Version]
- Mook-Kanamori, B.B.; Geldhoff, M.; Van Der Poll, T.; Van De Beek, D. Pathogenesis and Pathophysiology of Pneumococcal Meningitis. Clin. Microbiol. Rev. 2011, 24, 557–591. [Google Scholar] [CrossRef] [Green Version]
- Chaudhuri, A. Adjunctive dexamethasone treatment in acute bacterial meningitis. Lancet Neurol. 2004, 3, 54–62. [Google Scholar] [CrossRef]
- Baraff, L.J.; Lee, S.I.; Schriger, D.L. Outcome of Bacterial Meningitis in Children a Meta-Analysis. Pediatr. Infect. Dis. J. 1993, 12, 389–394. [Google Scholar] [CrossRef]
- Mahmoudi, S.; Zandi, H.; Pourakbari, B.; Ashtiani, M.T.H.; Mamishi, S. Acute Bacterial Meningitis among Children Admitted into an Iranian Referral Children’s Hospital. Jpn. J. Infect. Dis. 2013, 66, 503–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, A.; Bradley, A.; Wall, R.; McPherson, B.; Secka, A.; Dunn, D.; Greenwood, B. Sequelae of epidemic meningococcal meningitis in Africa. Trans. R. Soc. Trop. Med. Hyg. 1988, 82, 312–320. [Google Scholar] [CrossRef]
- Casella, E.B.; Cypel, S.; Osmo, A.A.; Okay, Y.; Lefèvre, B.H.; Lichtig, I.; Marques-Dias, M.J. Sequelae from meningococcal meningitis in children: A critical analysis of dexamethasone therapy. Arq. Neuro-Psiquiatr. 2004, 62, 421–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Østergaard, C.; Konradsen, H.B.; Samuelsson, S. Clinical presentation and prognostic factors of Streptococcus pneumoniae meningitis according to the focus of infection. BMC Infect. Dis. 2005, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klobassa, D.S.; Zoehrer, B.; Paulke-Korinek, M.; Gruber-Sedlmayr, U.; Pfurtscheller, K.; Strenger, V.; Sonnleitner, A.; Kerbl, R.; Ausserer, B.; Arocker, W.; et al. The burden of pneumococcal meningitis in Austrian children between 2001 and 2008. Eur. J. Nucl. Med. Mol. Imaging 2014, 173, 871–878. [Google Scholar] [CrossRef]
- Saha, S.K.; Khan, N.Z.; Ahmed, A.S.M.N.U.; Amin, M.R.; Hanif, M.; Mahbub, M.; Anwar, K.S.; Qazi, S.A.; Kilgore, P.; Baqui, A.H.; et al. Neurodevelopmental Sequelae in Pneumococcal Meningitis Cases in Bangladesh: A Comprehensive Follow-up Study. Clin. Infect. Dis. 2009, 48, 90–96. [Google Scholar] [CrossRef]
- Arditi, M.; Mason, E.O.; Bradley, J.S.; Tan, T.Q.; Barson, W.J.; Schutze, G.E.; Wald, E.R.; Givner, L.B.; Kim, K.S.; Yogev, R.; et al. Three-Year Multicenter Surveillance of Pneumococcal Meningitis in Children: Clinical Characteristics, and Outcome Related to Penicillin Susceptibility and Dexamethasone Use. Pediatrics 1998, 102, 1087–1097. [Google Scholar] [CrossRef] [PubMed]
- Karppinen, M.; Pelkonen, T.; Roine, I.; Cruzeiro, M.L.; Peltola, H.; Pitkäranta, A. Hearing impairment after childhood bacterial meningitis dependent on etiology in Luanda, Angola. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1820–1826. [Google Scholar] [CrossRef] [PubMed]
- King, B.; Richmond, P. Pneumococcal meningitis in Western Australian children: Epidemiology, microbiology and outcome. J. Paediatr. Child Health 2004, 40, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Osuorah, D.; Shah, B.; Manjang, A.; Secka, E.; Ekwochi, U.; Ebenebe, J. Outbreak of serotype W135 Neisseria meningitidis in central river region of the Gambia between February and June 2012: A hospital-based review of paediatric cases. Niger. J. Clin. Pr. 2014, 18, 41–47. [Google Scholar]
- Koomen, I.; Grobbee, D.; Jennekens-Schinkel, A.; Roord, J.; Furth, A. Parental perception of educational, behavioural and general health problems in school-age survivors of bacterial meningitis. Acta Paediatr. 2007, 92, 177–185. [Google Scholar] [CrossRef]
- Roed, C.; Omland, L.H.; Skinhoj, P.; Rothman, K.J.; Sorensen, H.T.; Obel, N. Educational Achievement and Economic Self-sufficiency in Adults after Childhood Bacterial Meningitis. JAMA 2013, 309, 1714–1721. [Google Scholar] [CrossRef] [Green Version]
- Taylor, H.G.; Schatschneider, C.; Minich, N.M. Longitudinal outcomes of Haemophilus influenzae meningitis in school-age children. Neuropsychology 2000, 14, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Snedeker, J.D.; Kaplan, S.L.; Dodge, P.R.; Holmes, S.J.; Feigin, R.D. Subdural effusion and its relationship with neurologic sequelae of bacterial meningitis in infancy: A prospective study. Pediatrics 1990, 86, 163–170. [Google Scholar]
- Olarte, L.; Barson, W.J.; Barson, R.M.; Lin, P.L.; Romero, J.R.; Tan, T.Q.; Givner, L.B.; Bradley, J.S.; Hoffman, J.A.; Hultén, K.G.; et al. Impact of the 13-Valent Pneumococcal Conjugate Vaccine on Pneumococcal Meningitis in US Children. Clin. Infect. Dis. 2015, 61, 767–775. [Google Scholar] [CrossRef] [Green Version]
- Wippold, F.J. Focal neurologic deficit. Am. J. Neuroradiol. 2008, 29, 1998–2000. [Google Scholar] [PubMed]
- Dunbar, M.; Shah, H.; Shinde, S.; Vayalumkal, J.; Vanderkooi, O.G.; Wei, X.-C.; Kirton, A. Stroke in Pediatric Bacterial Meningitis: Population-Based Epidemiology. Pediatr. Neurol. 2018, 89, 11–18. [Google Scholar] [CrossRef]
- Tibussek, D.; Sinclair, A.; Yau, I.; Teatero, S.; Fittipaldi, N.; Richardson, S.E.; Mayatepek, E.; Jahn, P.; Askalan, R. Late-Onset Group B Streptococcal Meningitis Has Cerebrovascular Complications. J. Pediatr. 2015, 166, 1187–1192. [Google Scholar] [CrossRef] [PubMed]
- Masri, A.; Alassaf, A.; Khuri-Bulos, N.; Zaq, I.; Hadidy, A.; Bakri, F.G. Recurrent meningitis in children: Etiologies, outcome, and lessons to learn. Child’s Nerv. Syst. 2018, 34, 1541–1547. [Google Scholar] [CrossRef]
- Unhanand, M.; Mustafa, M.M.; McCracken, G.H.; Nelson, J.D. Gram-negative enteric bacillary meningitis: A twenty-one-year experience. J. Pediatr. 1993, 122, 15–21. [Google Scholar] [CrossRef]
- Brouwer, M.C.; Wijdicks, E.F.M.; Van De Beek, D. What’s new in bacterial meningitis. Intensiv. Care Med. 2016, 42, 415–417. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Liu, X.; Wang, Y.; Liu, Q.; Kong, C.; Xu, G. Meta-analysis of adjunctive dexamethasone to improve clinical outcome of bacterial meningitis in children. Child’s Nerv. Syst. 2017, 34, 217–223. [Google Scholar] [CrossRef]
- Dodge, P.R.; Davis, H.; Feigin, R.D.; Holmes, S.J.; Kaplan, S.L.; Jubelirer, D.P.; Stechenberg, B.W.; Hirsh, S.K. Prospective Evaluation of Hearing Impairment as a Sequela of Acute Bacterial Meningitis. N. Engl. J. Med. 1984, 311, 869–874. [Google Scholar] [CrossRef]
- Sáez-Llorens, X.; McCracken, G.H. Acute Bacterial Meningitis beyond the Neonatal Period; Elsevier: Amsterdam, The Netherlands, 2008; pp. 284–291. [Google Scholar]
- Yoshinaga-Itano, C.; Sedey, A.L.; Coulter, D.K.; Mehl, A.L. Language of Early- and Later-identified Children with Hearing Loss. Pediatrics 1998, 102, 1161–1171. [Google Scholar] [CrossRef] [Green Version]
- Hall, W.C.; Li, N.; Dye, T.D.V. Influence of Hearing Loss on Child Behavioral and Home Experiences. Am. J. Public Health 2018, 108, 1079–1081. [Google Scholar] [CrossRef] [PubMed]
- Kostenniemi, U.J.; Bazan, A.; Karlsson, L.; Silfverdal, S.-A. Psychiatric Disabilities and Other Long-term Consequences of Childhood Bacterial Meningitis. Pediatr. Infect. Dis. J. 2020, 40, 26–31. [Google Scholar] [CrossRef]
- Kostenniemi, U.J.; Norman, D.; Borgström, M.; Silfverdal, S.A. The clinical presentation of acute bacterial meningitis varies with age, sex and duration of illness. Acta Paediatr. 2015, 104, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Curtis, S.; Stobart, K.; VanderMeer, B.; Simel, D.L.; Klassen, T. Clinical Features Suggestive of Meningitis in Children: A Systematic Review of Prospective Data. Pediatrics 2010, 126, 952–960. [Google Scholar] [CrossRef]
- Namani, S.A.; Kuchar, E.; Koci, R.; Mehmeti, M.; Dedushi, K. Early symptomatic and late seizures in Kosovar children with bacterial meningitis. Child’s Nerv. Syst. 2011, 27, 1967–1971. [Google Scholar] [CrossRef] [PubMed]
- Murthy, J.M.K.; Prabhakar, S. Bacterial meningitis and epilepsy. Epilepsia 2008, 49, 8–12. [Google Scholar] [CrossRef]
- Preux, P.-M.; Druet-Cabanac, M. Epidemiology and aetiology of epilepsy in sub-Saharan Africa. Lancet Neurol. 2005, 4, 21–31. [Google Scholar] [CrossRef]
- Pomeroy, S.L.; Holmes, S.J.; Dodge, P.R.; Feigin, R.D. Seizures and Other Neurologic Sequelae of Bacterial Meningitis in Children. N. Engl. J. Med. 1990, 323, 1651–1657. [Google Scholar] [CrossRef]
- De Jonge, R.C.; Van Furth, A.M.; Wassenaar, M.; Gemke, R.J.; Terwee, C.B. Predicting sequelae and death after bacterial meningitis in childhood: A systematic review of prognostic studies. BMC Infect. Dis. 2010, 10, 232. [Google Scholar] [CrossRef] [Green Version]
- Pong, A.; Bradley, J.S. Bacterial Meningitis and the Newborn Infant. Infect. Dis. Clin. N. Am. 1999, 13, 711–733. [Google Scholar] [CrossRef]
- Ouchenir, L.; Renaud, C.; Khan, S.; Bitnun, A.; Boisvert, A.-A.; McDonald, J.; Bowes, J.; Brophy, J.; Barton, M.; Ting, J.; et al. The Epidemiology, Management, and Outcomes of Bacterial Meningitis in Infants. Pediatrics 2017, 140, e20170476. [Google Scholar] [CrossRef] [Green Version]
- Huo, L.; Fan, Y.; Jiang, C.; Gao, J.; Yin, M.; Wang, H.; Yang, F.; Cao, Q. Clinical Features of and Risk Factors for Hydrocephalus in Childhood Bacterial Meningitis. J. Child Neurol. 2018, 34, 11–16. [Google Scholar] [CrossRef]
- Tamber, M.S.; Klimo, P.; Mazzola, C.A.; Flannery, A.M. Pediatric hydrocephalus: Systematic literature review and evidence-based guidelines. Part 8: Management of cerebrospinal fluid shunt infection. J. Neurosurg. Pediatr. 2014, 14, 60–71. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, D.C.; Diniz, L.M.O.; Guimarães, N.S.; Moreira, H.M.D.A.S.; Teixeira, C.C.; Romanelli, R.M.D.C. Risk factors associated with the outcomes of pediatric bacterial meningitis: A systematic review. J. Pediatr. 2020, 96, 159–167. [Google Scholar] [CrossRef]
- Feavers, I.; Pollard, A.J.; Sadarangani, M. Handbook of Meningococcal Disease Management; Springer International Publishing: Berlin/Heidelberg, Germany, 2016. [Google Scholar] [CrossRef]
- Pace, D.; Pollard, A.J. Meningococcal disease: Clinical presentation and sequelae. Vaccine 2012, 30, B3–B9. [Google Scholar] [CrossRef]
- Aku, F.Y.; Lessa, F.C.; Asiedu-Bekoe, F.; Balagumyetime, P.; Ofosu, W.; Farrar, J.; Ouattara, M.; Vuong, J.T.; Issah, K.; Opare, J.; et al. Meningitis Outbreak Caused by Vaccine-Preventable Bacterial Pathogens—Northern Ghana, 2016. Morb. Mortal. Wkly. Rep. 2017, 66, 806–810. [Google Scholar] [CrossRef] [Green Version]
- Greenwood, B. Editorial: 100 years of epidemic meningitis in West Africa—Has anything changed? Trop. Med. Int. Health 2006, 11, 773–780. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services Center for Disease Control and Prevention. Haemophilus Influenzae Type b (Hib) Vaccine: What You Need to Know Hib Vaccine. 2019. Available online: https://www.cdc.gov/vaccines/hcp/vis/vis-statements/hib.html (accessed on 2 January 2021).
- US Department of Health and Human Services Center for Disease Control and Prevention. Pneumococcal Polysaccharide Vaccine (PPSV23): What You Need to Know. 2019. Available online: https://www.cdc.gov/vaccines/hcp/vis/vis-statements/ppv.html (accessed on 2 January 2021).
- Bijlsma, M.W.; Brouwer, M.C.; Spanjaard, L.; Van De Beek, D.; Van Der Ende, A. A Decade of Herd Protection after Introduction of Meningococcal Serogroup C Conjugate Vaccination. Clin. Infect. Dis. 2014, 59, 1216–1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitney, C.G.; Farley, M.M.; Hadler, J.; Harrison, L.H.; Bennett, N.M.; Lynfield, R.; Reingold, A.; Cieslak, P.R.; Pilishvili, T.; Jackson, D.; et al. Decline in Invasive Pneumococcal Disease after the Introduction of Protein–Polysaccharide Conjugate Vaccine. N. Engl. J. Med. 2003, 348, 1737–1746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nigrovic, L.E.; Kuppermann, N.; Malley, R. For the Bacterial Meningitis Study Group of the Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics Children with Bacterial Meningitis Presenting to the Emergency Department during the Pneumococcal Conjugate Vaccine Era. Acad. Emerg. Med. 2008, 15, 522–528. [Google Scholar] [CrossRef]
- Ngocho, J.S.; Magoma, B.; Olomi, G.A.; Mahande, M.J.; Msuya, S.E.; De Jonge, M.I.; Mmbaga, B.T. Effectiveness of pneumococcal conjugate vaccines against invasive pneumococcal disease among children under five years of age in Africa: A systematic review. PLoS ONE 2019, 14, e0212295. [Google Scholar] [CrossRef]
- Kaplan, S.L.; O Mason, E.; Wald, E.R.; Schutze, G.E.; Bradley, J.S.; Tan, T.Q.; Hoffman, J.A.; Givner, L.B.; Yogev, R.; Barson, W.J. Decrease of invasive pneumococcal infections in children among 8 children’s hospitals in the United States after the introduction of the 7-valent pneumococcal conjugate vaccine. Pediatrics 2004, 113, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Singleton, R.J.; Hennessy, T.W.; Bulkow, L.R.; Hammitt, L.L.; Zulz, T.; Hurlburt, D.A.; Butler, J.C.; Rudolph, K.; Parkinson, A. Invasive Pneumococcal Disease Caused by Nonvaccine Serotypes among Alaska Native Children with High Levels of 7-Valent Pneumococcal Conjugate Vaccine Coverage. JAMA 2007, 297, 1784–1792. [Google Scholar] [CrossRef] [PubMed]
- Bozio, C.H.; Vuong, J.; Dokubo, E.K.; Fallah, M.P.; A McNamara, L.; Potts, C.C.; Doedeh, J.; Gbanya, M.; Retchless, A.C.; Patel, J.C.; et al. Outbreak of Neisseria meningitidis serogroup C outside the meningitis belt—Liberia, 2017: An epidemiological and laboratory investigation. Lancet Infect. Dis. 2018, 18, 1360–1367. [Google Scholar] [CrossRef]
- Wall, E.C.; Everett, D.B.; Mukaka, M.; Bar-Zeev, N.; Feasey, N.; Jahn, A.; Moore, M.; Van Oosterhout, J.J.; Pensalo, P.; Baguimira, K.; et al. Bacterial Meningitis in Malawian Adults, Adolescents, and Children during the Era of Antiretroviral Scale-up and Haemophilus influenzae Type b Vaccination, 2000–2012. Clin. Infect. Dis. 2014, 58, e137–e145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, E.M.; Li, Y.; Bita, A.; Moureau, A.; Nair, H.; Kyaw, M.H.; Abad, R.; Bailey, F.; Garcia, I.D.L.F.; Decheva, A.; et al. Meningococcal serogroups and surveillance: A systematic review and survey. J. Glob. Health 2018, 9, 010409. [Google Scholar] [CrossRef]
- Mustapha, M.M.; Harrison, L.H. Vaccine prevention of meningococcal disease in Africa: Major advances, remaining challenges. Hum. Vaccines Immunother. 2018, 14, 1107–1115. [Google Scholar] [CrossRef] [Green Version]
- Le Saux, N. Guidelines for the management of suspected and confirmed bacterial meningitis in Canadian children older than one month of age. Paediatr. Child Health 2014, 19, 141–146. [Google Scholar] [CrossRef] [Green Version]
- NICE UK. Meningitis (Bacterial) and Meningococcal Septicaemia in under 16s: Recognition, Diagnosis and Management. 2010. Available online: https://www.nice.org.uk/guidance/CG102/chapter/1-Guidance#pre-hospital-management-of-suspected-bacterial-meningitis-and-meningococcal-septicaemia (accessed on 14 January 2021).
- Agrawal, S.; Nadel, S. Acute bacterial meningitis in infants and children: Epidemiology and management. Pediatr. Drugs. 2011, 13, 385–400. Available online: http://0-ovidsp-ovid-com.brum.beds.ac.uk/ovidweb.cgi?T=JS&PAGE=reference&D=emed10&NEWS=N&AN=2011577682 (accessed on 16 December 2020). [CrossRef]
- Nudelman, Y.; Tunkel, A.R. Bacterial Meningitis. Drugs 2009, 69, 2577–2596. [Google Scholar] [CrossRef]
- Chaudhuri, A.; Martinez-Martin, P.; Kennedy, P.G.E.; Seaton, R.A.; Portegies, P.; Bojar, M.; Steiner, I.; EFNS Task Force. EFNS guideline on the management of community-acquired bacterial meningitis: Report of an EFNS Task Force on acute bacterial meningitis in older children and adults. Eur. J. Neurol. 2008, 15, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, M.C.; McIntyre, P.; Prasad, K.; Van De Beek, D. Corticosteroids for acute bacterial meningitis. Cochrane Database Syst. Rev. 2015, 2015, e004405. [Google Scholar] [CrossRef] [PubMed]
- Schaad, U.B.; Kaplan, S.L.; McCracken, J.G.H. Steroid Therapy for Bacterial Meningitis. Clin. Infect. Dis. 1995, 20, 685–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, K.; Nichani, J.; Hans, P.; Bruce, I.; Henderson, L.; Ramsden, R. C096 Cochlear implantation in profound hearing loss following bacterial meningitis in children. Int. J. Pediatr. Otorhinolaryngol. 2011, 75, 50. [Google Scholar] [CrossRef]
- Bille, J.; Ovesen, T. Cochlear implant after bacterial meningitis. Pediatr. Int. 2014, 56, 400–405. [Google Scholar] [CrossRef]
Figure 1.
Pathophysiology of Neuronal Damage due to Bacterial Meningitis.


{kind=link}
Table 1.
Most common organism for different Age Groups.
| Age Group | Most Common Organisms | References |
|---|---|---|
| Pre-term neonate | Escherichia coli, GBS * | [12,21,22] |
| Term neonate and infants < three months | GBS *, E. coli, Streptococcus pneumoniae, Listeria monocytogenes | [12] |
| Children ≥ three months to ten years | S. pneumoniae, Neisseria meningitidis, Haemophilus influenzae type b | [3,13,23,24] |
| Adolescent until 19 years old | N. meningitidis, S. pneumoniae | [4,25,26] |
* GBS: Group B Streptococcus.
Table 2.
Long and Short-term Neurological Complications following pneumococcal and meningococcal meningitis in Low and Middle Income Countries (LMICs) and High Income Countries (HICs).
Table 2.
Long and Short-term Neurological Complications following pneumococcal and meningococcal meningitis in Low and Middle Income Countries (LMICs) and High Income Countries (HICs).
| Pneumococcal Meningitis | Meningococcal Meningitis | References | |||
|---|---|---|---|---|---|
| LMICs | HICs | LMICs | HICs | ||
| Focal deficits | 12% | 3–14% | 2–4% | 3% | [13,39,40,41,42] |
| Hearing loss | 25% | 14–32% | 19–23% | 4% | [10,13,43,44,45] |
| Seizures | 45–63% | 15–48% | 17–33% | 2% | [40,45,46,47] |
| Cognitive impairment | 4–41% | N/A * | 4% | 12–19% | [10,13,43,48,49] |
*: Not avilable.
Table 3.
Risk factors for developing neurological complication in Bacterial Meningitis.
| Risk Factor | % with Neurological Complications | References |
|---|---|---|
| Young Age (infants < 12 months) | 71% | [9] |
| Etiology: S. pneumoniae | 75% | [9] |
| Altered Level of Consciousness on Presentation | 82% | [9] |
| Delayed Presentation | N/A * | [6,9] |
| Delayed initiation of antibiotics | N/A * | [76] |
* N/A: Not available.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zainel, A.; Mitchell, H.; Sadarangani, M. Bacterial Meningitis in Children: Neurological Complications, Associated Risk Factors, and Prevention. Microorganisms 2021, 9, 535. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9030535
AMA Style
Zainel A, Mitchell H, Sadarangani M. Bacterial Meningitis in Children: Neurological Complications, Associated Risk Factors, and Prevention. Microorganisms. 2021; 9(3):535. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9030535
Chicago/Turabian StyleZainel, Abdulwahed, Hana Mitchell, and Manish Sadarangani. 2021. "Bacterial Meningitis in Children: Neurological Complications, Associated Risk Factors, and Prevention" Microorganisms 9, no. 3: 535. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9030535
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.