
High Prevalence of Carbapenemase-Producing Acinetobacter baumannii in Wound Infections, Ghana, 2017/2018

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Clinical Diagnosis and Sample Collection
2.3. Microbiological Culture and Susceptibility Testing
2.4. Molecular Analyses
3. Results
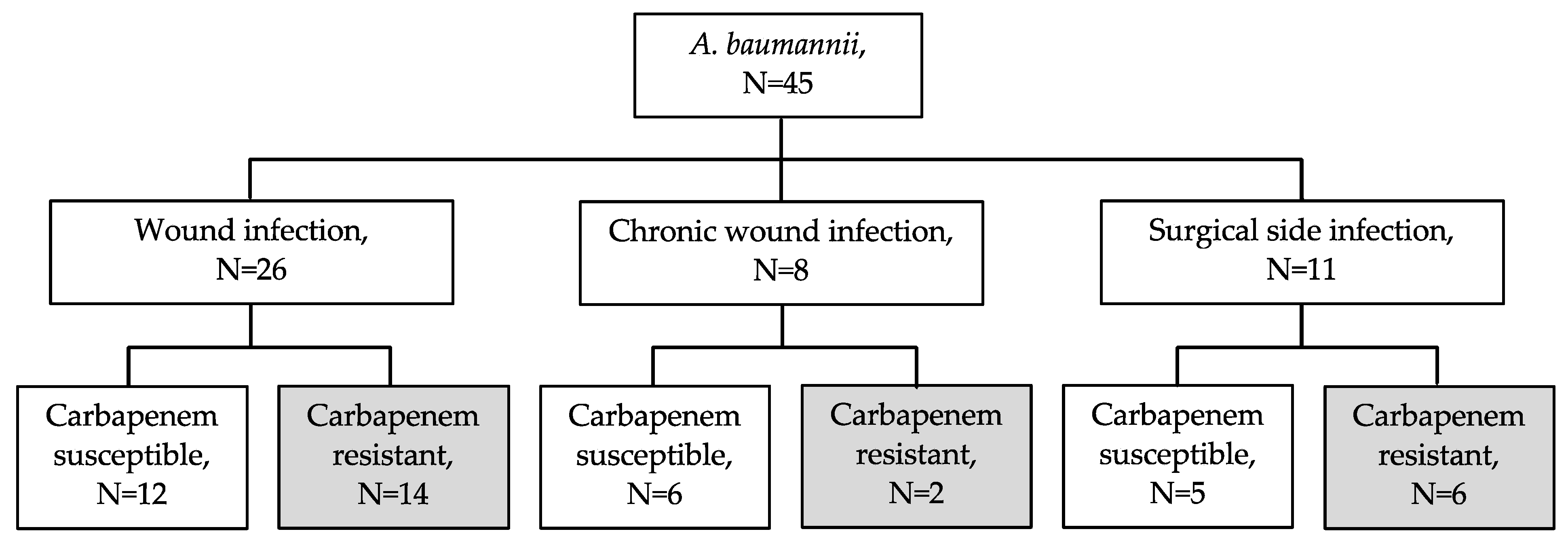
3.1. Wound Infection Classification
3.2. Identification and Susceptibility of Detected Bacterial Pathogens
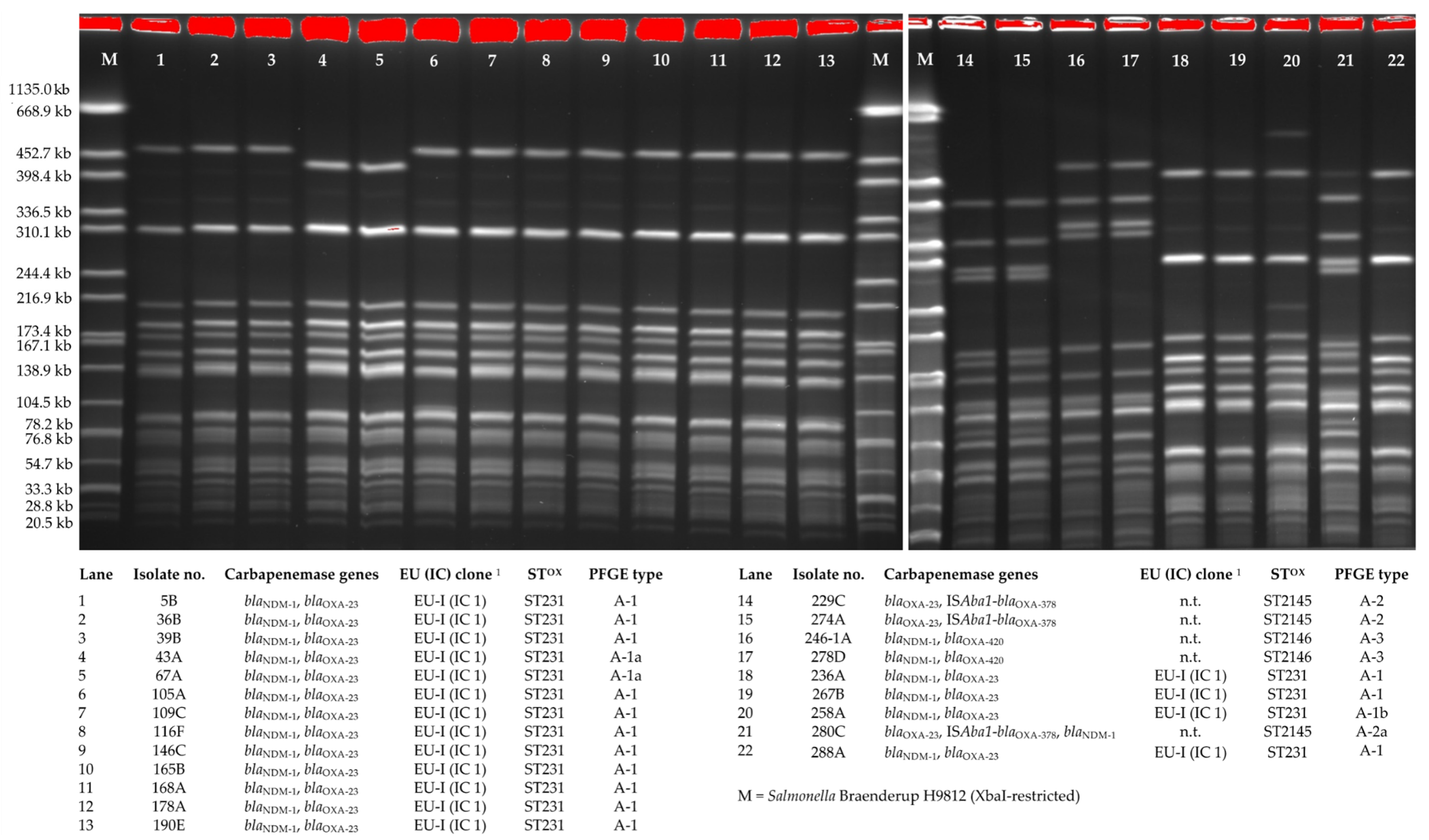
3.3. Molecular Characteristics of A. baumannii
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vrancianu, C.O.; Gheorghe, I.; Dobre, E.G.; Barbu, I.C.; Cristian, R.E.; Popa, M.; Lee, S.H.; Limban, C.; Vlad, I.M.; Chifiriuc, M.C. Emerging Strategies to Combat beta-Lactamase Producing ESKAPE Pathogens. Int. J. Mol. Sci. 2020, 21, 8527. [Google Scholar] [CrossRef] [PubMed]
- Shallcross, L.J.; Howard, S.J.; Fowler, T.; Davies, S.C. Tackling the threat of antimicrobial resistance: From policy to sustainable action. Philos. Trans. R. Soc. B 2015, 370, 20140082. [Google Scholar] [CrossRef] [PubMed]
- Hansen, G.T. Continuous Evolution: Perspective on the Epidemiology of Carbapenemase Resistance Among Enterobacterales and Other Gram-Negative Bacteria. Infect. Dis. Ther. 2021. [Google Scholar] [CrossRef]
- Halat, D.H.; Moubareck, C.A. The Current Burden of Carbapenemases: Review of Significant Properties and Dissemination among Gram-Negative Bacteria. Antibiotics 2020, 9, 186. [Google Scholar] [CrossRef]
- Livermore, D.M.; Woodford, N. The beta-lactamase threat in Enterobacteriaceae, Pseudomonas and Acinetobacter. Trends Microbiol. 2006, 14, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Livermore, D.M. Carbapenemases. J. Antimicrob. Chemother. 1992, 29, 609–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bush, K.; Bradford, P.A. Epidemiology of beta-Lactamase-Producing Pathogens. Clin. Microbiol. Rev. 2020, 33. [Google Scholar] [CrossRef] [PubMed]
- Weber, R.E.; Pietsch, M.; Fruhauf, A.; Pfeifer, Y.; Martin, M.; Luft, D.; Gatermann, S.; Pfennigwerth, N.; Kaase, M.; Werner, G.; et al. IS26-Mediated Transfer of bla NDM-1 as the Main Route of Resistance Transmission During a Polyclonal, Multispecies Outbreak in a German Hospital. Front. Microbiol. 2019, 10, 2817. [Google Scholar] [CrossRef] [PubMed]
- Labi, A.K.; Nielsen, K.L.; Marvig, R.L.; Bjerrum, S.; Enweronu-Laryea, C.; Bennedbaek, M.; Newman, M.J.; Ayibor, P.K.; Andersen, L.P.; Kurtzhals, J.A.L. Oxacillinase-181 Carbapenemase-Producing Klebsiella pneumoniae in Neonatal Intensive Care Unit, Ghana, 2017–2019. Emerg. Infect. Dis. 2020, 26, 2235–2238. [Google Scholar] [CrossRef] [PubMed]
- Strydom, K.A.; Chen, L.; Kock, M.M.; Stoltz, A.C.; Peirano, G.; Nobrega, D.B.; Lowe, M.; Ehlers, M.M.; Mbelle, N.M.; Kreiswirth, B.N.; et al. Klebsiella pneumoniae ST307 with OXA-181: Threat of a high-risk clone and promiscuous plasmid in a resource-constrained healthcare setting. J. Antimicrob. Chemother. 2020, 75, 896–902. [Google Scholar] [CrossRef]
- Leski, T.A.; Bangura, U.; Jimmy, D.H.; Ansumana, R.; Lizewski, S.E.; Li, R.W.; Stenger, D.A.; Taitt, C.R.; Vora, G.J. Identification of blaOXA-(5)(1)-like, blaOXA-(5)(8), blaDIM-(1), and blaVIM carbapenemase genes in hospital Enterobacteriaceae isolates from Sierra Leone. J. Clin. Microbiol. 2013, 51, 2435–2438. [Google Scholar] [CrossRef] [Green Version]
- Bonomo, R.A.; Burd, E.M.; Conly, J.; Limbago, B.M.; Poirel, L.; Segre, J.A.; Westblade, L.F. Carbapenemase-Producing Organisms: A Global Scourge. Clin. Infect. Dis. 2018, 66, 1290–1297. [Google Scholar] [CrossRef]
- Manenzhe, R.I.; Zar, H.J.; Nicol, M.P.; Kaba, M. The spread of carbapenemase-producing bacteria in Africa: A systematic review. J. Antimicrob. Chemother. 2015, 70, 23–40. [Google Scholar] [CrossRef] [Green Version]
- Semret, M.; Haraoui, L.P. Antimicrobial Resistance in the Tropics. Infect. Dis. Clin. N. Am. 2019, 33, 231–245. [Google Scholar] [CrossRef] [PubMed]
- Doi, Y. Treatment Options for Carbapenem-resistant Gram-negative Bacterial Infections. Clin. Infect. Dis. 2019, 69, S565–S575. [Google Scholar] [CrossRef] [Green Version]
- Laxminarayan, R.; Matsoso, P.; Pant, S.; Brower, C.; Rottingen, J.A.; Klugman, K.; Davies, S. Access to effective antimicrobials: A worldwide challenge. Lancet 2016, 387, 168–175. [Google Scholar] [CrossRef]
- Munoz-Price, L.S.; Weinstein, R.A. Acinetobacter infection. N. Engl. J. Med. 2008, 358, 1271–1281. [Google Scholar] [CrossRef]
- Sebeny, P.J.; Riddle, M.S.; Petersen, K. Acinetobacter baumannii skin and soft-tissue infection associated with war trauma. Clin. Infect. Dis. 2008, 47, 444–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, K.A.; Moran, K.A.; McAllister, C.K.; Gray, P.J. Multidrug-resistant Acinetobacter extremity infections in soldiers. Emerg. Infect. Dis. 2005, 11, 1218–1224. [Google Scholar] [CrossRef]
- Petersen, K.; Cannegieter, S.C.; van der Reijden, T.J.; van Strijen, B.; You, D.M.; Babel, B.S.; Philip, A.I.; Dijkshoorn, L. Diversity and clinical impact of Acinetobacter baumannii colonization and infection at a military medical center. J. Clin. Microbiol. 2011, 49, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Leaper, D.; Assadian, O.; Edmiston, C.E. Approach to chronic wound infections. Br. J. Dermatol. 2015, 173, 351–358. [Google Scholar] [CrossRef]
- Savage, V.J.; Chopra, I.; O’Neill, A.J. Staphylococcus aureus biofilms promote horizontal transfer of antibiotic resistance. Antimicrob. Agents Chemother. 2013, 57, 1968–1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowler, P.G. Antibiotic resistance and biofilm tolerance: A combined threat in the treatment of chronic infections. J. Wound Care 2018, 27, 273–277. [Google Scholar] [CrossRef]
- Singh, N.; Manchanda, V. Control of multidrug-resistant Gram-negative bacteria in low- and middle-income countries-high impact interventions without much resources. Clin. Microbiol. Infect. 2017, 23, 216–218. [Google Scholar] [CrossRef] [Green Version]
- Cox, J.A.; Vlieghe, E.; Mendelson, M.; Wertheim, H.; Ndegwa, L.; Villegas, M.V.; Gould, I.; Hara, G.L. Antibiotic stewardship in low- and middle-income countries: The same but different? Clin. Microbiol. Infect. 2017, 23, 812–818. [Google Scholar] [CrossRef] [Green Version]
- Nordmann, P.; Poirel, L. Epidemiology and Diagnostics of Carbapenem Resistance in Gram-negative Bacteria. Clin. Infect. Dis. 2019, 69, S521–S528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, H.; Janssen, I.; Cooper, P.; Kainyah, C.; Pellio, T.; Quintel, M.; Monnheimer, M.; Gross, U.; Schulze, M.H. Antimicrobial-Resistant Bacteria in Infected Wounds, Ghana, 2014. Emerg. Infect. Dis. 2018, 24, 916–919. [Google Scholar] [CrossRef]
- Cheesbrough, M. District Laboratory Practice in Tropical Countries, 2nd ed.; Cambridge University Press: Cambridge, UK, 2006; Volume Part 2. [Google Scholar]
- Rieber, H.; Frontzek, A.; Pfeifer, Y. Molecular Investigation of Carbapenem-Resistant Acinetobacter spp. from Hospitals in North Rhine-Westphalia, Germany. Microb. Drug Resist. 2017, 23, 25–31. [Google Scholar] [CrossRef]
- Pfeifer, Y.; Wilharm, G.; Zander, E.; Wichelhaus, T.A.; Gottig, S.; Hunfeld, K.P.; Seifert, H.; Witte, W.; Higgins, P.G. Molecular characterization of blaNDM-1 in an Acinetobacter baumannii strain isolated in Germany in 2007. J. Antimicrob. Chemother. 2011, 66, 1998–2001. [Google Scholar] [CrossRef] [Green Version]
- Turton, J.F.; Ward, M.E.; Woodford, N.; Kaufmann, M.E.; Pike, R.; Livermore, D.M.; Pitt, T.L. The role of ISAba1 in expression of OXA carbapenemase genes in Acinetobacter baumannii. FEMS Microbiol. Lett. 2006, 258, 72–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turton, J.F.; Gabriel, S.N.; Valderrey, C.; Kaufmann, M.E.; Pitt, T.L. Use of sequence-based typing and multiplex PCR to identify clonal lineages of outbreak strains of Acinetobacter baumannii. Clin. Microbiol. Infect. 2007, 13, 807–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tenover, F.C.; Arbeit, R.D.; Goering, R.V.; Mickelsen, P.A.; Murray, B.E.; Persing, D.H.; Swaminathan, B. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: Criteria for bacterial strain typing. J. Clin. Microbiol. 1995, 33, 2233–2239. [Google Scholar] [CrossRef] [Green Version]
- Wilharm, G.; Skiebe, E.; Higgins, P.G.; Poppel, M.T.; Blaschke, U.; Leser, S.; Heider, C.; Heindorf, M.; Brauner, P.; Jackel, U.; et al. Relatedness of wildlife and livestock avian isolates of the nosocomial pathogen Acinetobacter baumannii to lineages spread in hospitals worldwide. Environ. Microbiol. 2017, 19, 4349–4364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrestha, S.; Tada, T.; Miyoshi-Akiyama, T.; Ohara, H.; Shimada, K.; Satou, K.; Teruya, K.; Nakano, K.; Shiroma, A.; Sherchand, J.B.; et al. Molecular epidemiology of multidrug-resistant Acinetobacter baumannii isolates in a university hospital in Nepal reveals the emergence of a novel epidemic clonal lineage. Int. J. Antimicrob. Agents 2015, 46, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Ayibieke, A.; Kobayashi, A.; Suzuki, M.; Sato, W.; Mahazu, S.; Prah, I.; Mizoguchi, M.; Moriya, K.; Hayashi, T.; Suzuki, T.; et al. Prevalence and Characterization of Carbapenem-Hydrolyzing Class D beta-Lactamase-Producing Acinetobacter Isolates From Ghana. Front. Microbiol. 2020, 11, 587398. [Google Scholar] [CrossRef]
- Krumkamp, R.; Oppong, K.; Hogan, B.; Strauss, R.; Frickmann, H.; Wiafe-Akenten, C.; Boahen, K.G.; Rickerts, V.; McCormick Smith, I.; Gross, U.; et al. Spectrum of antibiotic resistant bacteria and fungi isolated from chronically infected wounds in a rural district hospital in Ghana. PLoS ONE 2020, 15, e0237263. [Google Scholar] [CrossRef]
- Ingelbeen, B.; Koirala, K.D.; Verdonck, K.; Barbe, B.; Mukendi, D.; Thong, P.; El Safi, S.; Van Duffel, L.; Bottieau, E.; van der Sande, M.A.B.; et al. Antibiotic use prior to seeking medical care in patients with persistent fever: A cross-sectional study in four low- and middle-income countries. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef]
- Peirano, G.; Ahmed-Bentley, J.; Fuller, J.; Rubin, J.E.; Pitout, J.D. Travel-related carbapenemase-producing Gram-negative bacteria in Alberta, Canada: The first 3 years. J. Clin. Microbiol. 2014, 52, 1575–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Bij, A.K.; Pitout, J.D. The role of international travel in the worldwide spread of multiresistant Enterobacteriaceae. J. Antimicrob. Chemother. 2012, 67, 2090–2100. [Google Scholar] [CrossRef] [Green Version]
- Rogers, B.A.; Aminzadeh, Z.; Hayashi, Y.; Paterson, D.L. Country-to-country transfer of patients and the risk of multi-resistant bacterial infection. Clin. Infect. Dis. 2011, 53, 49–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kallberg, C.; Ardal, C.; Blix, H.S.; Klein, E.; Martinez, E.; Lindbaek, M.; Outterson, K.; Rottingen, J.A.; Laxminarayan, R. Introduction and geographic availability of new antibiotics approved between 1999 and 2014. PLoS ONE 2018, 13, e0205166. [Google Scholar] [CrossRef]
- Gould, D.J.; Moralejo, D.; Drey, N.; Chudleigh, J.H.; Taljaard, M. Interventions to improve hand hygiene compliance in patient care. Cochrane Database Syst. Rev. 2017, 9, CD005186. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Co-Detected Bacterial Species in Wound Infections (n = Number of Wound Infections) | |
|---|---|
| Gram-Positive Pathogens | Gram-Negative Pathogens |
| Staphylococcus aureus, n = 6 | Proteus mirabilis, n = 6 |
| Corynebacterium striatum, n = 3 | Escherichia coli, n = 4 |
| Bacillus cereus, n = 2 | Stenotrophomonas maltophilia, n = 3 |
| Corynebacterium amycolatum, n = 1 | Enterobacter cloacae, n = 2 |
| Enterococcus avium, n = 1 | Klebsiella pneumoniae, n = 2 |
| Enterococcus casseliflavus, n = 1 | Pseudomonas aeruginosa, n = 2 |
| Enterococcus faecalis, n = 1 | Achromobacter spanius, n = 1 |
| Providencia stuartii, n = 1 | |
| Isolate No. | Sampling Date | Species | A. baumannii Specific blaOXA-51-like1 | Carbapenemase Genes | A. baumannii Typing PCR (clones EI-III) 2 | PFGE-Type | Sequence Type (ST)OX | Resistances 3 |
|---|---|---|---|---|---|---|---|---|
| 5B | 21.08.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 36B | 22.09.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 39B | 26.09.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 43A | 27.09.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1a | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 67A | 12.10.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1a | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 105A | 06.11.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 109C | 08.11.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 116F | 10.11.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 146C | 27.11.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 165B | 06.12.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 168A | 11.12.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 178A | 15.12.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 190E | 22.12.2017 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 229C | 15.01.2018 | A. baumannii | blaOXA-378 | blaOXA-23, ISAba1-blaOXA-378 | n.t. | A-2 | ST2145 | IPM, MEM, GEN, CIP, SXT |
| 236A | 17.01.2018 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 246-1A | 24.01.2018 | A. baumannii | blaOXA-378 | blaNDM-1, blaOXA-420 | n.t. | A-3 | ST2146 | IPM, MEM, GEN, AMK, CIP, SXT |
| 258A | 05.02.2018 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1b | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 267B | 06.02.2018 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
| 274A | 14.02.2018 | A. baumannii | blaOXA-378 | blaOXA-23, ISAba1-blaOXA-378 | n.t. | A-2 | ST2145 | IPM, MEM, GEN, CIP, SXT |
| 278D | 19.02.2018 | A. baumannii | blaOXA-378 | blaNDM-1, blaOXA-420 | n.t. | A-3 | ST2146 | IPM, MEM, GEN, AMK, CIP, SXT |
| 280C | 19.02.2018 | A. baumannii | blaOXA-378 | blaOXA-23, ISAba1-blaOXA-378, blaNDM-1 | n.t. | A-2a | ST2145 | IPM, MEM, GEN, AMK, CIP, SXT |
| 288A | 24.02.2018 | A. baumannii | blaOXA-69 | blaNDM-1, blaOXA-23 | EU-I (IC 1) | A-1 | ST231 | IPM, MEM, GEN, AMK, CIP, SXT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monnheimer, M.; Cooper, P.; Amegbletor, H.K.; Pellio, T.; Groß, U.; Pfeifer, Y.; Schulze, M.H. High Prevalence of Carbapenemase-Producing Acinetobacter baumannii in Wound Infections, Ghana, 2017/2018. Microorganisms 2021, 9, 537. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9030537
Monnheimer M, Cooper P, Amegbletor HK, Pellio T, Groß U, Pfeifer Y, Schulze MH. High Prevalence of Carbapenemase-Producing Acinetobacter baumannii in Wound Infections, Ghana, 2017/2018. Microorganisms. 2021; 9(3):537. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9030537
Chicago/Turabian StyleMonnheimer, Mathieu, Paul Cooper, Harold K. Amegbletor, Theresia Pellio, Uwe Groß, Yvonne Pfeifer, and Marco H. Schulze. 2021. "High Prevalence of Carbapenemase-Producing Acinetobacter baumannii in Wound Infections, Ghana, 2017/2018" Microorganisms 9, no. 3: 537. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9030537